Introduction
Urosepsis is a specific form of urinary tract
infection, resulting in serious systemic infection by hematogenous
spread. Specifically, 20–30% of patients with sepsis develop the
condition as a result of a urinary tract infection (1), and urinary tract infection accounts
for 5–7% of severe cases of sepsis (2,3).
Clinically, acute upper urinary tract obstruction is common and is
likely to cause septic shock (4).
Therefore, early diagnosis and effective treatment of urinary
sepsis is essential for the prevention of mortality.
Tumor necrosis factor-α (TNF-α), interleukin (IL)-6
and IL-10 are cytokines involved in the inflammatory response of
sepsis. During the inflammatory response, TNF-α is initially
released, regulating IL-6 and IL-8 levels. IL-10 is an important
anti-inflammatory and immune inhibitory cytokine secreted by
macrophages, which inhibits TNF-α and increases the IL-1 receptor
antagonist (5).
Ulinastatin (UTI) is a 143-amino acid, acidic
glycoprotein secreted by the liver. UTI inhibits trypsin and is
commonly used in the treatment of pancreatitis. In addition, UTI
stabilizes lysosomal membranes and inhibits lysosomal enzyme
release and myocardial depressant factor production. UTI also
inhibits neutrophil activation and transendothelial migration,
reduces inflammatory cell infiltration and downregulates
inflammatory cytokines and is currently used for the treatment of
acute circulatory failure. Early administration of UTI has been
demonstrated to inhibit neutrophil protease release and excessive
inflammatory responses and reduce the release of oxygen free
radicals and consumption of superoxide dismutase (6,7). UTI
effectively reduces body temperature, respiratory rate, white blood
cell count (WBC) and regulates levels of TNF-α, plasma IL-6,
C-reactive protein (CRP) and procalcitonin in patients with sepsis
(8).
In our previous study, a non-cytotoxic antitumor
reagent was demonstrated to downregulate the expression of
Survivin, Bcl-xL and Mta-1 in tumor cells (9) and upregulate expression of Smad-4
(10). In the present study,
urinary tract obstruction was performed in rats and the urinary
tract was infected with Escherichia coli endotoxin (LPS) to
establish a model of sepsis. Successfully established models were
used to determine whether UTI induces changes in IL-10 and TNF-α
expression. In addition, the efficacy and the associated molecular
mechanisms of UTI in the treatment of sepsis were investigated.
Materials and methods
Reagents
LPS (0111:B4) was purchased from Sigma-Aldrich (St.
Louis, MO, USA). UTI was purchased from Techpool Bio-Pharma Co.,
Ltd. (Guangdong, China). TNF-α and IL-10 kits were purchased from
Shanghai Shengke Co. (Shanghai, China). TNF-α and IL-10 antibodies
were purchased from Beijing Biosynthesis Biotechnology Co., Ltd.
(Beijing, China). Rabbit SP-HRP and DAB color kits were purchased
from Beijing cwbiotech Co., Ltd. (Beijing, China).
Animal models
Twenty-four rabbits (weight, 1.80–2.20 kg) were
purchased from the Department of Animal Experiments, Nanhua
University (Hengyang, China). The study was approved by the ethics
committee of the University of South China, Hengyang, Hunan, China.
Rabbits were randomly divided into 4 groups; the normal, sham,
sepsis model and UTI groups. In the normal, sham and UTI groups,
rabbits were fed normally. Rabbits were anesthetized with 10%
chloral hydrate (3 ml/kg) after being weighed, and were then fixed
to the operating table. The abdominal cavity was exposed using a
3-cm longitudinal incision and the left psoas muscle was located.
The left ureter was then separated. The abdominal cavity was closed
and the intestines were reset. In the sepsis model and sham groups,
the left ureter was found and separated using the same surgical
approach. The lower end of the ureter was ligated and 1 ml LPS (800
μg/kg) was injected. The ureter was again ligated above the
injection point. Following local irrigation, the abdominal cavity
was closed. In the UTI group, the surgical approach was identical
to that used in the sepsis model group. Following surgery,
1.5×107 units UTI were dissolved in 3 ml saline and
injected into the marginal ear vein. Following surgery, rabbits
from all groups were fed and watered normally.
After 24 h, 4–5 ml blood from the marginal ear vein
of surviving rabbits in the sham and sepsis model groups was
extracted for subsequent analyses. At 36 h, 2–3 ml blood from the
left iliac vein of surviving rabbits was removed for routine blood
testing. Following centrifugation (1409 × g) of the venous blood
samples, 5–8 ml supernatant was collected and further detection of
IL-10 and TNF-α was performed. Rabbits were sacrificed following
blood sample extraction. The left kidney, the lungs and the liver
were placed in 10% neutral formalin for 24 h and embedded in
paraffin. CRP was detected using an AU800 automatic biochemical
analyzer (Olympus Optical Co., Ltd., Tokyo, Japan).
Enzyme-linked immunosorbent assay
(ELISA)
Blood was coagulated and centrifuged at room
temperature for 10–20 min. The supernatant was collected and
standards were diluted as the control. Diluted samples (50 μl) were
added to blank wells and 50 μl diluted standard was added to
standard wells. In the sample wells, 50 μl diluted standard and 10
μl sample was added. The sample was gently mixed and incubated for
30 min at 37°C. OD values at a wavelength of 450 nm were determined
by ELISA for each well.
Hematoxylin and eosin (H&E)
staining
Tissues were dried in an incubator and dewaxed for
10 min using xylene. Next, samples were dewaxed again with fresh
xylene for 5 min. Following H&E staining, samples were observed
under a light microscope and images were captured.
Immunohistochemical method
Rabbit kidney tissue specimens were embedded and
sliced in a paraffin block to a thickness of 4 mm, according to the
manufacturer’s instructions. Tissues were treated with
diethylpyrocarbonate (DEPC). The secondary antibody was
biotin-labeled goat anti-rabbit secondary antibody solution.
Western blot analysis
Total proteins were isolated from tissues, separated
on SDS-PAGE gels and transferred to membranes. Membranes were
incubated with primary antibodies against IL-10 (1:200), TNF-α
(1:200) and β-actin (1:1,000; Santa Cruz Biotechnology Inc., Santa
Cruz, CA, USA). Next, membranes were incubated with horseradish
peroxidase-conjugated secondary antibodies (sc-2030; Santa Cruz
Biotechnology Inc.), visualized using an enhanced chemiluminescence
detection kit (Pierce Biotechnology, Inc., Rockford, IL, USA) and
exposed to X-ray film. β-actin was used as a loading control.
Statistical analysis
Data were processed using SPSS 13.0 statistical
software. Data are expressed as the mean ± SD. One-way ANOVA was
applied for comparison between groups. A two-sample paired t-test
analysis method was applied for comparison at 24 and 36 h following
surgery. P<0.05 was considered to indicate a statistically
significant difference.
Results
Body temperature and respiratory rate of
rabbits following surgery
To establish the rabbit model, 24 rabbits were
randomly divided into 4 groups, the normal, sham, sepsis model and
UTI groups, each containing 6 rabbits. As demonstrated in Table I, at 24 and 36 h postoperatively,
body temperature was not found to be significantly different
compared with normal rabbits. Respiratory rates between the sham
and normal groups at 24 and 36 h following surgery were not
identified as significantly different (P=0.731 and P=0.683). The
body temperature of sepsis model rabbits began to rise 24 h after
establishment of the model. At 36 h, marked changes in body
temperature were observed, increasing from 38.6 to 41.0°C (P=0.00),
and the respiratory rate increased from 46.5 to 77.5 bpm (P=0.00).
Body temperature decreased 36 h after surgery when UTI treatment
was administered. When comparing the UTI and model groups, the
difference was found to be statistically significant (P=0.010).
Respiratory rate was also observed to be significantly different
between the treatment and model groups (P=0.034).
 | Table IComparison of body temperature and
respiratory rate in 4 groups of rabbits at 36 h postoperatively
(mean ± SD, n=6). |
Table I
Comparison of body temperature and
respiratory rate in 4 groups of rabbits at 36 h postoperatively
(mean ± SD, n=6).
| Group | Cases | Body temperature
(°C) | Respiratory rate
(bpm) |
|---|
| Normal | 6 | 38.6±0.4 | 46.5±4.3 |
| Sham | 6 | 38.6±0.4 | 45.5±4.2 |
| Sepsis model | 6 | 41.0±0.7a,b | 77.5±5.1a,b |
| UTI | 6 | 40.0±0.3c | 72.0±2.8c |
Peripheral blood cell count and CRP
changes
As demonstrated in Table II, at 24 and 36 h postoperatively,
when compared with normal group, WBC was slightly elevated in the
sham group but was not identified to be significantly different
(P=0.099 and P=0.062, respectively; P>0.05). WBC was observed to
increase in a time-dependent manner. At 24 and 36 h after modeling,
the WBC in the model group was 12.66×109 and
15.35×109 cells/l, respectively. In the sham group, the
WBC 36 h following surgery was identified to be significantly
higher than the normal group (P=0.00). WBC decreased in the
treatment group compared with the sepsis model group (P=0.008). No
significant difference in platelet count was identified between the
groups (P=0.686 and P=0.805, respectively). Serum CRP concentration
36 h following surgery was found to be significantly higher in the
sham group than the normal group (P=0.001). CRP levels in the model
group were observed to be significantly higher compared with the
sham and normal groups (P=0.000). CRP levels in the treatment and
sepsis model groups were identified to be significantly different,
whereby serum CRP concentration was higher in the sepsis model
group (P=0.000).
| Table IIComparison of WBC, PLTs and CRP in 4
groups of rabbits at 36 h postoperatively (mean ± SD, n=6). |
Table II
Comparison of WBC, PLTs and CRP in 4
groups of rabbits at 36 h postoperatively (mean ± SD, n=6).
| Group | Cases | WBC (109
cells/l) | PLT (109
cells/l) | CRP (mg/l) |
|---|
| Normal | 6 | 5.01±1.61 | 471.83±94.07 | 1.93±1.26 |
| Sham | 6 | 7.06±2.68 | 435.17±63.82 | 12.27±3.13a |
| Sepsis model | 6 | 15.35±1.31a,b | 451.83±51.29 | 30.03±7.65a,b |
| UTI | 6 | 12.29±1.22c | 431.50±92.31 | 19.22±3.19c |
Determination of rabbit serum IL-10 and
TNF-α concentrations
As is revealed in Table III, there was no significant
difference in serum IL-10 levels between the sham (34.543±2.820
pg/ml) and normal groups (28.751±3.608 pg/ml) at each time-point
(P=0.301 and 0.234) according to ELISA results. In the sepsis model
group, serum IL-10 levels (112.469±7.840 pg/ml) were significantly
higher than the normal and sham groups (P=0.000). Compared with the
sepsis model group, IL-10 was significantly higher in the UTI
treatment group (183.91±11.521 pg/ml) 36 h following surgery
(P=0.000).
| Table IIIComparison of IL-10 and TNF-α in 4
groups of rabbits at 36 h postoperatively (mean ± SD, n=6), as
measured by ELISA. |
Table III
Comparison of IL-10 and TNF-α in 4
groups of rabbits at 36 h postoperatively (mean ± SD, n=6), as
measured by ELISA.
| Group | Cases | IL-10 (pg/ml) | TNF-α (ng/l) |
|---|
| Normal | 6 | 28.751±3.608. | 15.074±1.413 |
| Sham | 6 | 34.543±2.820. | 18.711±1.493 |
| Sepsis model | 6 | 112.469±7.840a,b | 88.769±6.358a,b |
| UTI | 6 |
183.910±11.521c. | 31.637±2.770c |
TNF-α levels were slightly higher in the sham
(18.711±1.493 ng/l) than normal group (15.074±1.413 ng/l), but were
not found to be significantly different (P=0.466 and P=0.134).
Serum TNF-α levels in the sepsis model group (88.769±6.358 ng/l)
were significantly higher than in the normal and sham groups
(P=0.000). However, compared with the sepsis model group, serum
TNF-α concentration was observed to decrease significantly in the
UTI treatment group (31.637±2.770 ng/l; P=0.000). These results
indicate that UTI treatment increased levels of IL-10, but deceased
levels of TNF-α.
H&E staining of rabbit kidney, liver
and lung tissues
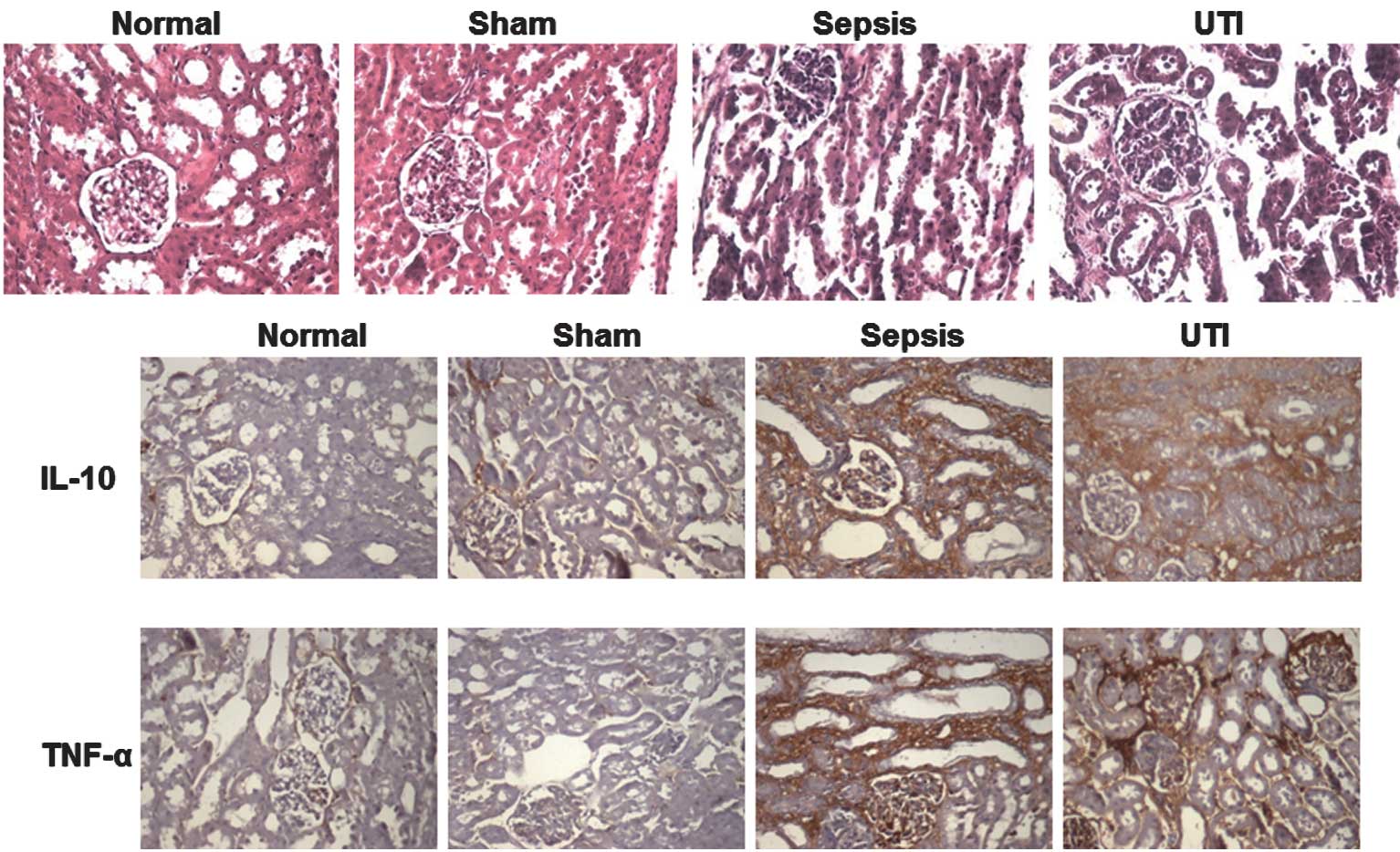
To examine the effect of UTI treatment on rabbit
tissue, H&E staining was performed in all 4 groups. As
demonstrated in Fig. 1A, kidney
tissues obtained from normal and sham groups exhibited normal
morphologies. In the sepsis model group, glomerulus deformities and
tubular lumen enlargement were observed. The renal interstitial
space was congested with edema and infiltrated with inflammatory
cells. There was slight swelling of liver cells and scattered
inflammatory cell infiltration in liver biopsies. In lung biopsies,
we observed diffuse thickening of the alveolar septa and
inflammatory cell infiltration. Pathological deformities were
attenuated in the UTI treatment group compared with the sepsis
model group. Similar results were also observed in the liver and
lung tissues (data not shown).
Immunohistochemical detection of IL-10
and TNF-α in kidney tissues of each group
To detect whether UTI induces alterations in levels
of IL-10 and TNF-α, immunohistochemical analysis of rabbit kidney
tissues was performed. Images are presented in Fig. 1B. Levels were calculated based on
immunohistochemistry detection. As demonstrated in Table IV, differences in the expression
of IL-10 and TNF-α between the normal and sham groups were not
significant. IL-10 protein levels in the UTI treatment group were
higher than in the sepsis model group. However, levels of TNF-α in
the UTI treatment group were lower than those in the sepsis model
group.
| Table IVComparison of IL-10 and TNF-α
expression in the kidneys of 4 groups of rabbits at 36 h
postoperatively (OD, mean ± SD, n=6). |
Table IV
Comparison of IL-10 and TNF-α
expression in the kidneys of 4 groups of rabbits at 36 h
postoperatively (OD, mean ± SD, n=6).
| Group | Cases | IL-10 | TNF-α |
|---|
| Normal | 6 | 0.115±0.023 | 0.141±0.022 |
| Sham | 6 | 0.111±0.022 | 0.125±0.021 |
| Sepsis model | 6 | 0.226±0.019a,b | 0.264±0.025a,b |
| UTI | 6 | 0.269±0.018c | 0.222±0.023c |
Western blot analysis of IL-10 and TNF-α
in kidney tissue of each group
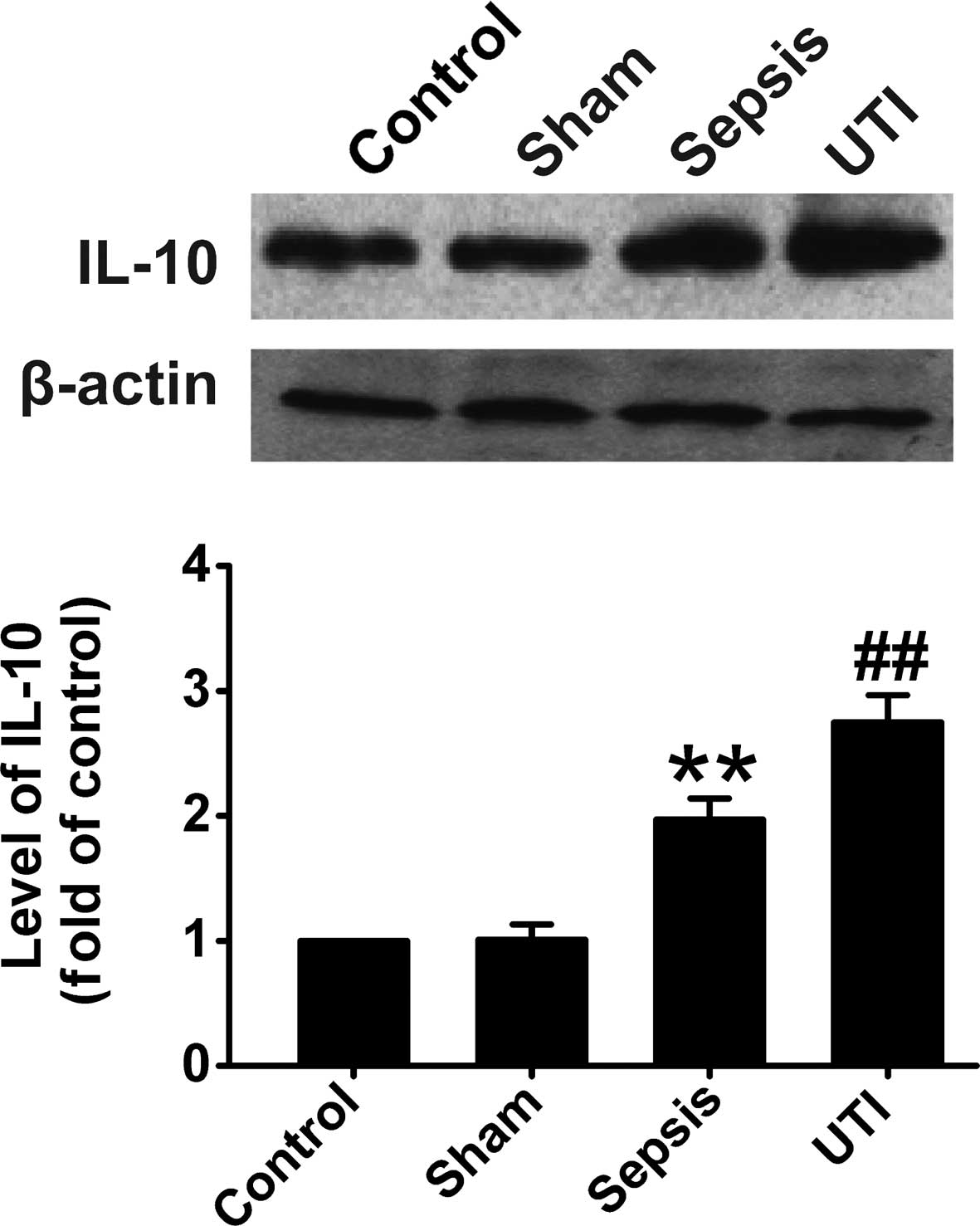
To further determine whether UTI induces alterations
in the levels of IL-10 and TNF-α, total proteins were extracted
from rabbit kidney tissues in every group and western blot analysis
was performed. As demonstrated in Fig.
2, IL-10 levels in the normal and sham groups were similar. In
the sepsis group, IL-10 levels were increased. However, IL-10
levels in the UTI treatment group were found to be significantly
increased compared with the sepsis group.
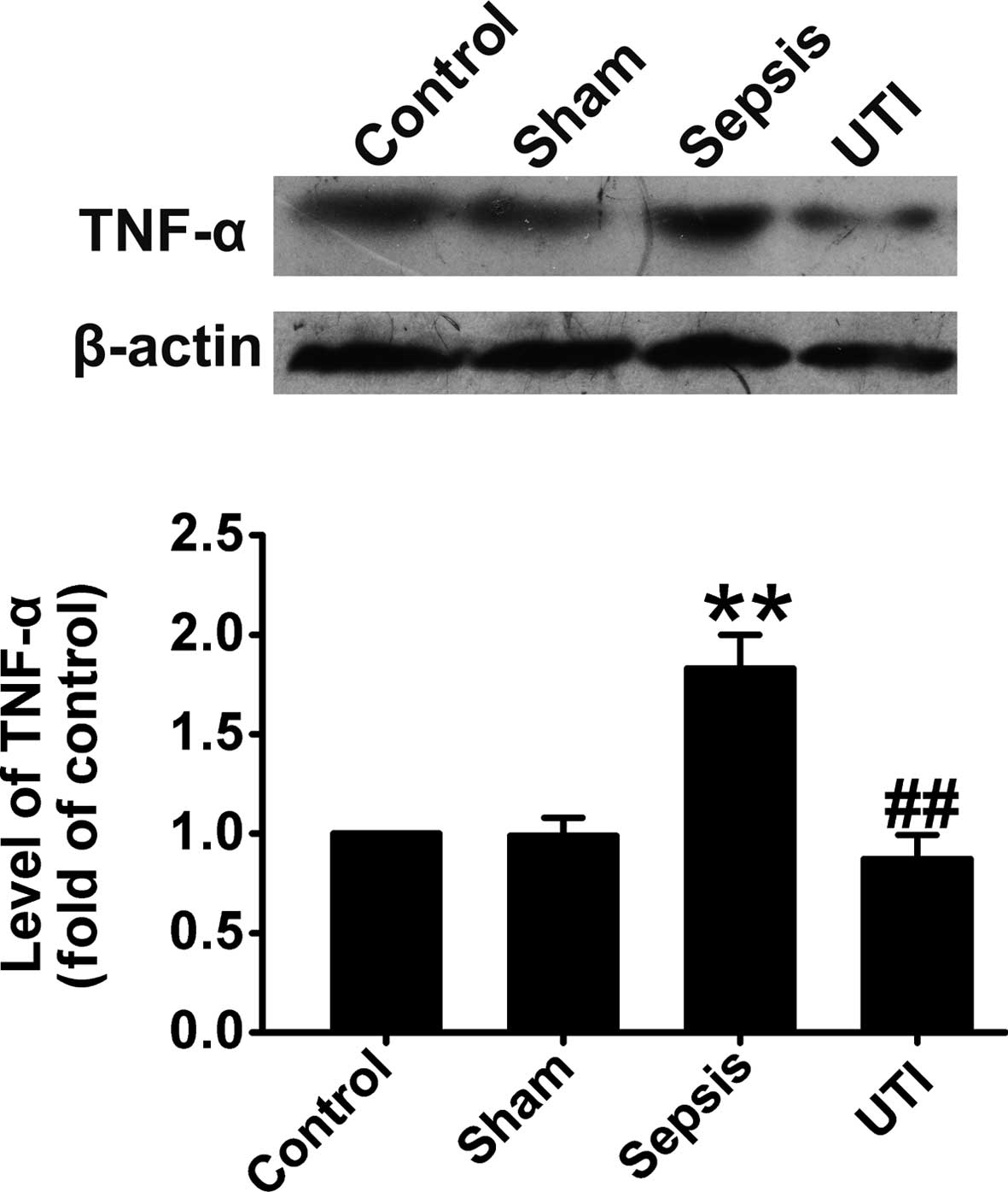
As revealed in Fig.
3, TNF-α levels in the normal and sham groups were similar. In
the sepsis group, TNF-α levels were increased compared with the
control group. However, TNF-α levels in the UTI treatment group
were significantly decreased compared with the sepsis group.
Results of western blot analysis were consistent with the
immunohistochemistry results, indicating that UTI upregulates IL-10
levels and downregulates TNF-α levels.
Discussion
Animal models provide a basis for pathogenesis
studies of the mechanisms of sepsis and are essential for the
development, prevention and control of this condition. Models of
sepsis simulate the etiology, pathogenesis, development and
clinical characteristics of sepsis to provide insight into methods
for its prevention and treatment. Several sepsis models have been
established and are each associated with specific characteristics
(5). In the present study, a model
of urinary tract infection and acute upper urinary tract
obstruction was established by injection of LPS and ligation of the
ureter to induce acute obstruction and a model of urinary
sepsis.
In this study, no significant differences in rabbit
rectal temperatures, respiratory rates, peripheral blood leukocytes
and serum TNF-α and IL-10 levels were identified in the sham and
normal groups at each time-point. These observations indicate that
the surgery itself did not affect organ function. In the sepsis
model group, body temperature began to rise at 24 h, respiratory
rate accelerated in a time-dependent manner, TNF-α and IL-10 levels
were observed to be significantly increased, rectal temperature
increased from 38.6 to 41.0°C and peripheral blood leukocytes
(15.35×109/l) and CRP (31.03±8.06 mg/l) increased
significantly compared with the control group. In addition, liver,
kidney and lung morphologies were altered, indicating that the
urinary sepsis model was established successfully.
Inflammatory cytokines, including TNF-α, IL-6 and
IL-10, were previously revealed to cause sepsis-related multiple
organ dysfunction syndrome (MODS) (11–14).
TNF-α is largely generated by activated monocytes/macrophages and
endothelial cells, which induce systemic inflammatory response
syndrome/MODS. IL-6 is a major cytokine that is activated by
monocytes, macrophages and endothelial cells in the acute response
phase and is induced by IL-1β and TNF-α. IL-6 is a
hepatocyte-stimulating factor that induces liver cells to produce
acute CRP and enhances the destructive inflammatory response of the
host. Continually increasing IL-6 levels indicate poor prognosis
(15). IL-10 is an important
cytokine produced by T cells, macrophages and monocytes. It
inhibits mRNA transcription for a variety of immune active
cytokines and the activation of monocytes and macrophages to
secrete other cytokines, including TNF-α and IL-1, which regulates
damage by the excessive inflammatory response triggered by
proinflammatory cytokines (16).
IL-10 is a protective and anti-inflammatory cytokine in sepsis and
MODS that reduces the systemic inflammatory response and organ
damage (17). CRP is an extremely
sensitive and nonspecific indicator of sepsis diagnosis, which is
an active protein in the acute phase of an infectious disease and
is significantly elevated in inflammation and tissue damage.
Increasing levels of CRP are closely associated with the severity
of tissue damage.
Molor-Erdene et al(18) demonstrated that UTI inhibited TNF-α
induced by LPS and significantly reduced TNF-α expression in a
dose-dependent manner in rat lung tissue. UTI reduces TNF-α and
IL-6 and improves IL-10 levels to prevent further MODS (19). In the current study, compared with
model rabbits, TNF-α levels were decreased and IL-10 levels were
increased in the control group, as demonstrated by western blot
analysis and immunohistochemistry. CRP was decreased significantly
in the treatment group, consistent with previous studies (8,19).
These observations indicate that UTI may represent an important
agent for the prevention and treatment of urinary sepsis by
inhibiting synthesis and release of TNF-α and upregulating IL-10.
UTI was found to balance the internal environmental and reduce
tissue damage.
The current study indicates that UTI may represent a
novel therapy for the prevention and treatment of urinary sepsis
and suggests that the mechanism via which UTI exerts its effects
may involve the upregulation of IL-10 and downregulation of TNF-α
levels.
References
|
1
|
Brun-Buisson C: The epidemiology of the
systemic inflammatory response. Intensive Care Med. 26(Suppl 1):
S64–S74. 2000. View Article : Google Scholar
|
|
2
|
Hotchkiss RS and Karl IE: The
pathophysiology and treatment of sepsis. N Engl J Med. 348:138–150.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Brunkhorst FM: Epidemiology, economy and
practice - results of the German study on prevalence by the
competence network sepsis (SepNet). Anasthesiol Intensivmed
Notfallmed Schmerzther. 41:43–44. 2006.(In German).
|
|
4
|
Yamamoto Y, Fujita K, Nakazawa S, et al:
Clinical characteristics and risk factors for septic shock in
patients receiving emergency drainage for acute pyelonephritis with
upper urinary tract calculi. BMC Urol. 12:42012. View Article : Google Scholar
|
|
5
|
Yao Yongming, Chai Jiake and Li Hongyuan:
Modern Sepsis Theory and Practice. Science Press; Beijing: pp.
155–288. 2005
|
|
6
|
Saji T: Clinical utility of ulinastatin,
urinary protease inhibitor in acute Kawasaki disease. Nihon Rinsho.
66:343–348. 2008.(In Japanese).
|
|
7
|
Tani T, Aoki H, Yoshioka T, Lin KJ and
Kodama M: Treatment of septic shock with a protease inhibitor in a
canine model: a prospective, randomized, controlled trial. Crit
Care Med. 21:925–930. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shao YM, Zhang LQ, Deng LH and Yao HG:
Clinical study on effects of ulinastatin on patients with systemic
inflammatory response syndrome. Chin Wei Zhong Bing Ji Jiu Med.
17:228–230. 2005.(In Chinese).
|
|
9
|
Chen X, Wang Y, Luo H, et al: β-elemene
acts as an antitumor factor and downregulates the expression of
survivin, Bcl-xL and Mta-1. Mol Med Rep. 6:989–995. 2012.
|
|
10
|
Lu X, Wang Y, Luo H, Qiu W, Han H, Chen X
and Yang L: β-elemene inhibits the proliferation of T24 bladder
carcinoma cells through upregulation of the expression of Smad4.
Mol Med Rep. 7:513–518. 2013.
|
|
11
|
Ono S, Ichikura T and Mochizuki H: The
pathogenesis of the systemic inflammatory response syndrome and
compensatory antiinflammatory response syndrome following surgical
stress. Nihon Geka Gakkai Zasshi. 104:499–505. 2003.(In
Japanese).
|
|
12
|
Levels JH, Lemaire LC, van den Ende AE,
van Deventer SJ and van Lanschot JJ: Lipid composition and
lipopolysaccharide binding capacity of lipoproteins in plasma and
lymph of patients with systemic inflammatory response syndrome and
multiple organ failure. Crit Care Med. 31:1647–1653. 2003.
View Article : Google Scholar
|
|
13
|
Kocabaş E, Sarikçioğlu A, Aksaray N,
Seydaoğlu G, Seyhun Y and Yaman A: Role of procalcitonin,
C-reactive protein, interleukin-6, interleukin-8 and tumor necrosis
factor-alpha in the diagnosis of neonatal sepsis. Turk J Pediatr.
49:7–20. 2007.PubMed/NCBI
|
|
14
|
Ni Choileain N and Redmond HP: The
immunological consequences of injury. Surgeon. 4:23–31. 2006.
|
|
15
|
Zhang Q, Li Q, Mao BL, Qian GS, Xu JC and
Chen ZT: Studies on the expression of mRNA of anti- and
pro-inflammatory cytokines in acute lung injury induced by
lipopolysaccharide in rat. Chin Wei Zhong Bing Ji Jiu Med.
16:585–588. 2004.(In Chinese).
|
|
16
|
Moore KW, de Waal Malefyt R, Coffman RL
and O’Garra A: Interleukin-10 and the interleukin-10 receptor. Annu
Rev Immunol. 19:683–765. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sewnath ME, Olszyna DP, Birjmohun R, ten
Kate FJ, Gouma DJ and van Der Poll T: IL-10-deficient mice
demonstrate multiple organ failure and increased mortality during
Escherichia coli peritonitis despite an accelerated
bacterial clearance. J Immunol. 166:6323–6331. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Molor-Erdene P, Okajima K, Isobe H, Uchiba
M, Harada N and Okabe H: Urinary trypsin inhibitor reduces
LPS-induced hypotension by suppressing tumor necrosis factor-alpha
production through inhibition of Egr-1 expression. Am J Physiol
Heart Circ Physiol. 288:H1265–H1271. 2005. View Article : Google Scholar
|
|
19
|
Cao YZ, Tu YY, Chen X, et al: Protective
effect of ulinastatin against murine models of sepsis: inhibition
of TNF-α and IL-6 and augmentation of IL-10 and IL-13. Exp Toxicol
Pathol. 64:543–547. 2012.PubMed/NCBI
|