Introduction
Although giant cell tumors (GCT) of the bones are
relatively common primary bone tumors, it is rare for a GCT to
occur in the sacrum and spine (1–3). The
symptoms are not specific, and the tumors are difficult to diagnose
at the early stage. The tumors may attain a large size and
neurological deficits may be experienced secondary to compression
of the spinal cord or nerve roots (4–6). Large
spinal GCTs are difficult to manage. Although the optimal treatment
of GCTs in the sacrum and spine remains controversial, surgery is
the main treatment; complete excision is recommended for the
treatment of spinal GCTs.
Compared with the normal spine, GCT is a
hypervascular lesion (1,7). Massive blood loss during surgery is a
severe complication (3,8,9), which
may be life-threatening and make the surgery impossible to complete
(10). Therefore, pre-operative
embolization of spinal tumors is recommended to reduce
intraoperative bleeding and make an unresectable tumor resectable.
Several studies have reported results for the pre-operative
embolization of hypervascular spinal tumors and clearly showed that
the technique is safe and effective at reducing intraoperative
blood loss (11–13). However, only a few studies have
examined the effect of pre-operative embolization for GCTs of the
spine and the majority are case reports (14).
The purpose of the present retrospective study was
to investigate the value of surgical excision with pre-operative
transarterial embolization for GCTs of the sacrum and spine, and
evaluate the follow-up outcomes.
Materials and methods
Patient data
A total of 28 consecutive patients (16 females and
12 males) with GCTs of the sacrum and spine, who underwent surgical
excision combined with pre-operative transarterial embolization
between June 1995 and August 2011, were retrospectively reviewed.
The average age at the first diagnosis was 29.6 years (range, 11–58
years). All medical charts were reviewed, including the clinical
records, operative notes and radiological and histological
findings. All 28 patients were verified to have GCT by histological
examination following surgery. Of the 28 cases, 13 were located in
the mobile spine, with 8 thoracic and 5 lumbar GCTs, and 15 cases
were located in the sacrum. The majority of patients presented with
pain or a neurological deficit at the site of tumor involvement,
such as paresthesia, weakness and bowel and/or bladder dysfunction.
The duration of the pre-operative symptoms ranged between 0.5 and
40 months (median, 4 months). Patients were followed up via
clinical examination and using imaging studies at the outpatient
clinic every three months for two years and then every six months
thereafter. The intraoperative level of blood loss, transfusion,
duration of surgery, treatment, complications, local recurrence,
follow-up status and functional outcome were reviewed. Patient
demographics are shown in Table I.
This study was approved by the ethics committee of Soochow
University. Written informed consent was obtained from all
patients.
 | Table I.Patient demographics. |
Table I.
Patient demographics.
| Demographic | Data |
|---|
| Gender, n | |
| Male | 12 |
| Female | 16 |
| Age (years), n | |
| <20 | 3 |
| 20–40 | 19 |
| >40 | 6 |
| Mean | 29.6 |
| Site, n | |
| Sacrum | 15 |
| Lumbar spine | 5 |
| Thoracic spine | 8 |
| Pre-operative
neurological function, n | |
| Normal | 11 |
| Partial loss | 17 |
| Complete loss | 0 |
| Surgical approach,
n | |
| A | 8 |
| P | 18 |
| A+P | 2 |
| Reconstruction,
n | |
| Yes | 14 |
| No | 14 |
| Nerve root
sacrificed, n | |
| Yes | 13 |
| No | 15 |
| Local recurrence,
n | |
| Yes | 8 |
| No | 20 |
| Neurological function
at six months, n | |
| Normal | 24 |
| Partial loss | 4 |
| Complete loss | 0 |
| Last status, n | |
| NED | 25 |
| STU | 2 |
| AWD | 1 |
Pre-operative arterial embolization
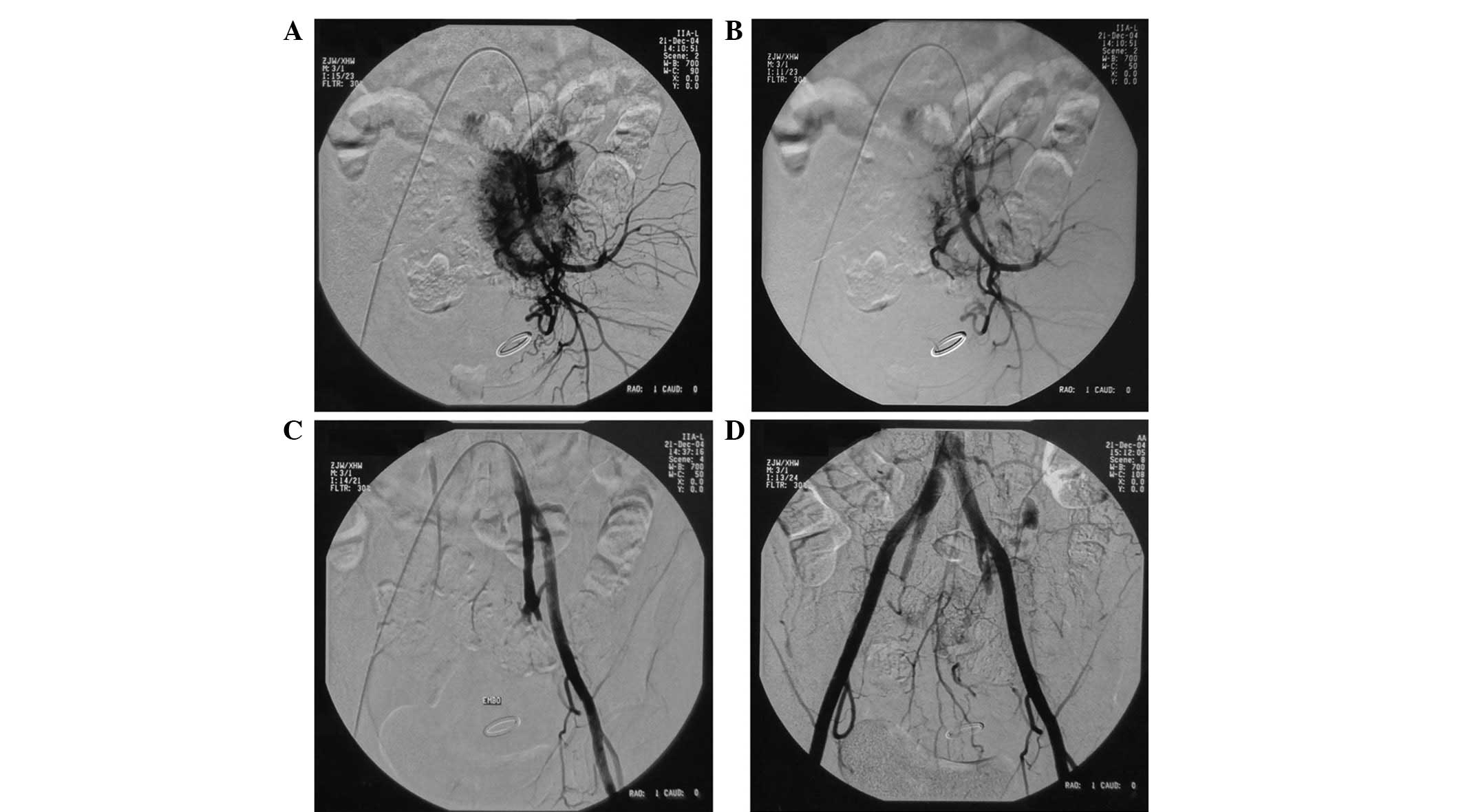
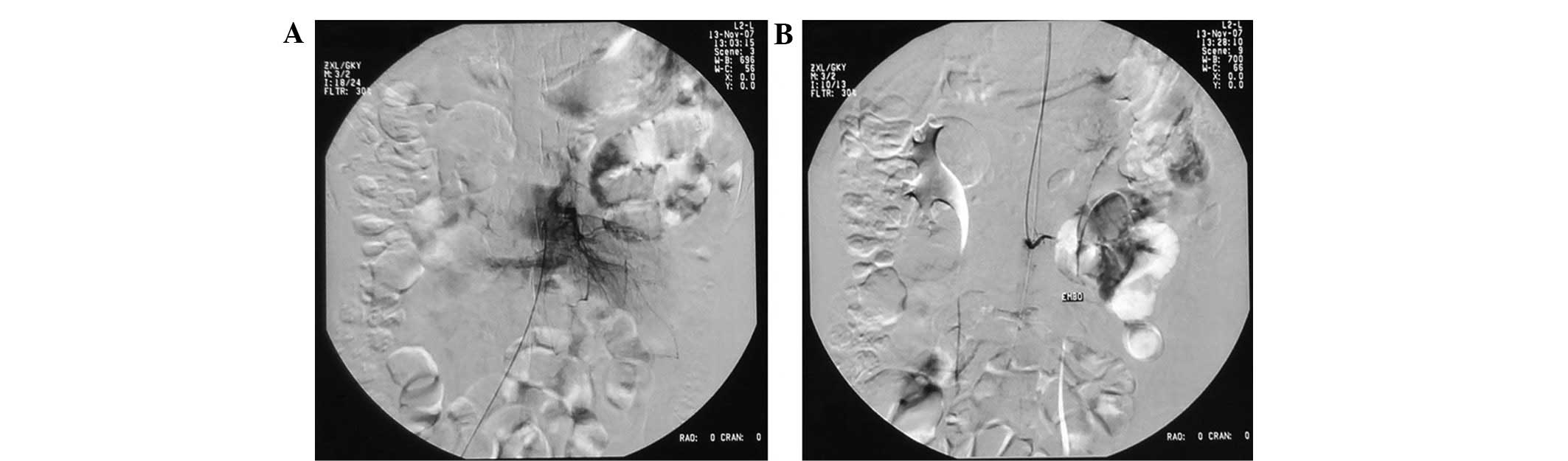
All patients underwent pre-operative angiography and
embolization using the reformed Seldinger methods following femoral
artery insertion under local anesthesia. The tumor-feeding vessels
and the size and location of the tumor, as well as the association
between the blood supply arteries and surrounding tissues, were
determined by digital subtraction angiography. Particular attention
was paid to the visualization of the radiculomedullary branches to
the anterior spinal artery (artery of Adamkiewicz). If the artery
of Adamkiewicz was visualized in the pre-embolization digital view,
embolization of this segmental vessel was not performed.
In the mobile spine, devascularization of the
segmental vessels was attempted bilaterally at the level of the
lesion, as well as at the cephalic and caudal levels, while in the
sacrum, the arteries embolized included the bilateral internal
iliac, middle sacral and bilateral L4 transverse arteries.
Gelfoam particles were used to embolize the small
intratumoral arteries, and the stems of the tumor-feeding arteries
were embolized with a gelfoam strip. The angiograph was performed
again to ensure that all tumor-supplying vessels were embolized.
(Figs. 1 and 2).
Operative technique
Surgery was performed within one to two days after
the arterial embolization. For the mobile spine, the surgical
approach was decided based on the position of the tumor. If the
stabilization of the spine was disrupted following the removal the
tumor, instrumentation was required. For the GCTs of the sacrum, a
single posterior approach was used for 14 patients, while a
one-stage anterior and posterior combined approach was used for one
patient who presented with a larger tumor. The mechanical stability
was often insufficient if the S1 and total sacrum or substantial
portions of the two iliac wings were excised; consequently, a
spinal instrumentation system was required to support the spine.
All the tumor excisions were defined as intralesional. Subsequent
to exposure, the tumor perimeter was packed with gauze to prevent
spillage of the tumor tissue during curettage. The nerve roots were
protected and preserved whenever possible. If the nerve roots or
spinal dura mater were contaminated with the tumor cell during
surgery, the membrane was dissected carefully. The surgical field
was covered thoroughly with 95% ethyl alcohol gauze, then cleaned
with warm normal saline. Sterilized distilled water was used to
lyse the residual microscopic tumor debris. Routinely, effective
suction drainage was placed post-operatively to promote primary
healing.
Statistical analysis
Data were analyzed with SAS version 8.1 (SAS
Institute, Cary, NC, USA). For comparisons of the quantitative data
of the two groups, the independent samples t-test was used;
continuous data are expressed in terms of the mean and standard
deviation. P<0.05 was considered to indicate a statistically
significant difference.
Results
No symptomatic complications were observed to be
associated with embolization, and all the tumor masses were removed
completely without any intraoperative shock or fatalities. The
average intraoperative level of blood loss was 1,528.6 ml (range,
400–5,800 ml), the average transfusion volume was 1,514.3 ml
(range, 400–6,000 ml) and the average duration of surgery was 225.4
min (range, 120–470 min). The sites of the tumors and the lengths
of time between embolization and tumor resection were compared in
terms of average intraoperative level of blood loss, average
transfusion volume and average duration of surgery (Table II).
| Table II.Blood loss, transfusion and duration
of surgery. |
Table II.
Blood loss, transfusion and duration
of surgery.
| Variable | Patient no. | Blood loss (ml)
| Transfusion (ml)
| Surgery duration
(min)
|
|---|
| Mean | SD | P-value (t-test) | Mean | SD | P-value (t-test) | Mean | SD | P-value (t-test) |
|---|
| Site | | | | 0.611 | | | 0.641 | | | 0.266 |
| Sacrum | 15 | 1640.0 | 1455.4 | | 1620.0 | 1472.7 | | 204.7 | 104.2 | |
| Mobile Spine | 13 | 1400.0 | 899.1 | | 1392.3 | 986.1 | | 249.2 | 102.7 | |
| Time between
embolization and surgery (days) | | | | 0.372 | | | 0.302 | | | 0.140 |
| 1 | 23 | 1626.1 | 1257.8 | | 1630.4 | 1308.9 | | 245.0 | 110.0 | |
| 2 | 5 | 1080.0 | 965.4 | | 980.0 | 861.4 | | 167.0 | 60.2 | |
All the patients were treated with intralesional
surgical resection combined with pre-operative transarterial
embolization. A total of 14 patients underwent reconstruction. Six
patients were treated post-operatively with adjuvant radiation
therapy and no radiation myelopathy or sarcomatous transformation
was observed in the study. Of the 28 patients, eight (28.6%)
experienced complications perioperatively or during the follow-up.
Six (21.4%) patients had wound complications; three experienced
skin necrosis, two had wound infections and one patient had a sinus
tract infection. Five of these patients were healed following
dressing changes, debridement or systemic antibiotics, although the
remaining patient still suffered from wound exudation at the final
follow-up, which required dressing changes every day. One patient
experienced cerebrospinal fluid leakage that was treated by a
conservative method. The dural tears were repaired with a 4-0 or
5-0 silk suture and then covered with a gelatin sponge. The patient
was positioned with their head down, in the Trendelenburg position.
One thoracic patient developed kyphosis, which was also treated
conservatively as there was no pain and the patient was able to
tolerate the condition. No patients experienced deep-vein
thrombosis, pulmonary embolism or hardware failure requiring
surgical revision.
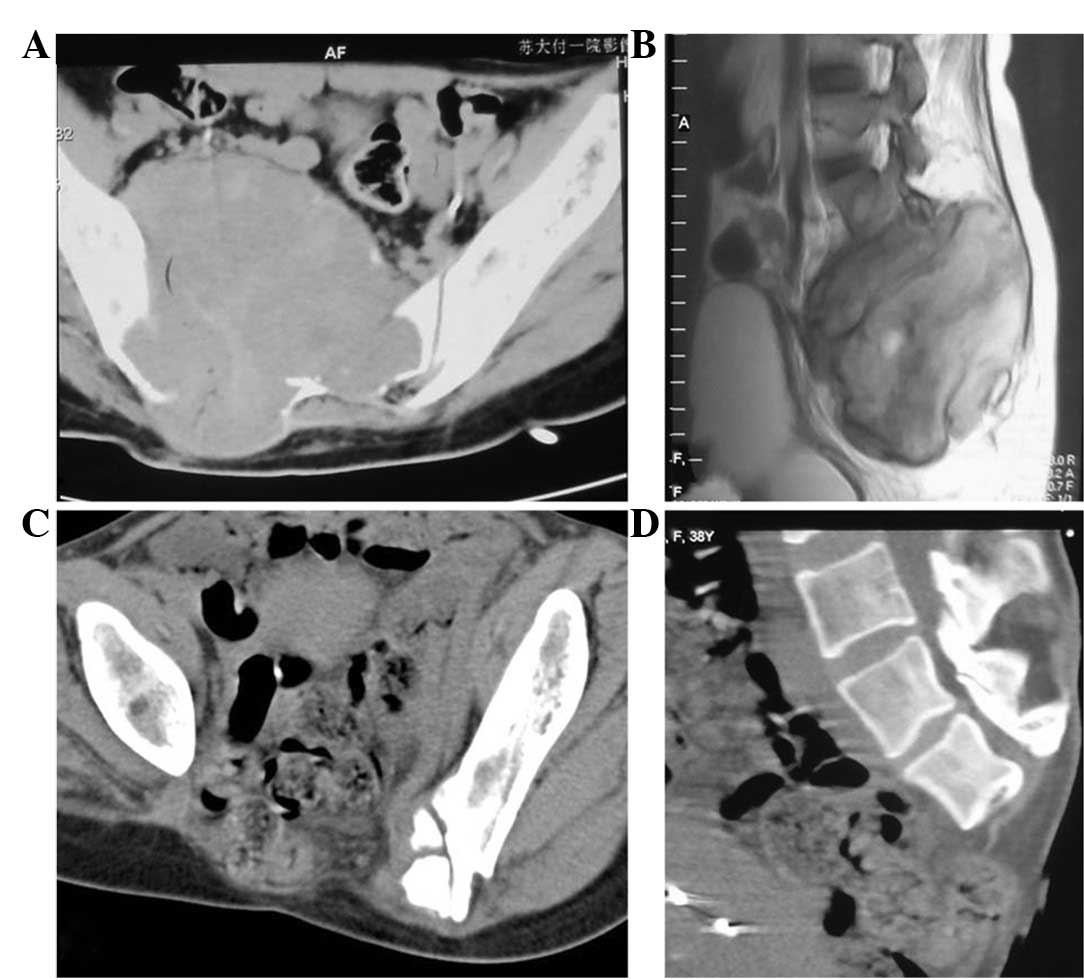
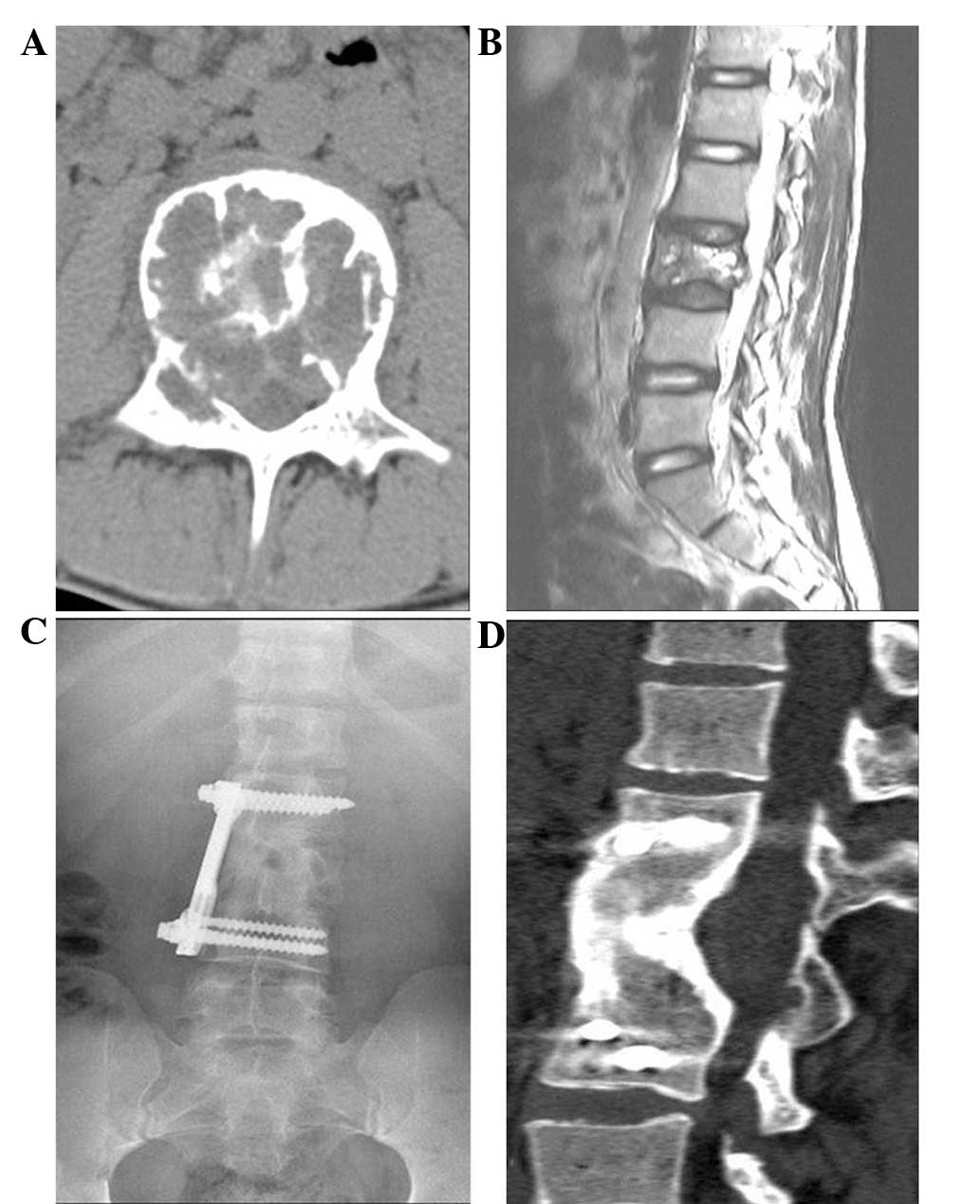
All the cases were followed up for an average of
86.3 months (range, 12–193 months). A total of eight patients
developed recurrence (28.6%) and the average time was 35.6 months
(range, 5–79 months). Of the eight patients, seven received
surgical revision with no repeated recurrence observed. The
remaining patient received no treatment and remained alive with the
disease. At the final follow-up, 25 patients showed no evidence of
disease, one patient was alive with the disease and two patients
had succumbed. No patients had metastases in the lungs. In total,
11 sacral GCT patients (Fig. 3) and
all the spinal GCT patients (13 cases; Fig. 4) had normal neurological function,
whereas the function of the sphincter muscles was impaired in four
sacral GCT patients. Two patients were able to walk with an
assistive device and the other 26 patients were able to ambulate
without any support.
Discussion
GCTs are hypervascular lesions (1,7) that
rarely occur in the spine (1–3). Due
to the complicated anatomical structure and hypervascularity of the
tumors, massive blood loss often occurs during the surgical
treatment procedures. Turcotte et al (3) reported that the average level of
intraoperative blood loss was 7,500 ml, while Ozaki et al
(8) reported that the level of
intraoperative blood loss ranged between 2,400 and 6,700 ml
(median, 5,250 ml). Takeda et al (9) reported the level of intraoperative
blood loss of two patients to be 4,921 ml and 20,000 ml,
respectively. Bleeding during spinal GCT surgery is a severe
complication, which may be life-threatening and make it impossible
to complete the surgical procedure (10). Therefore, pre-operative embolization
of the spinal tumors is recommended to reduce intraoperative
bleeding. Several studies have reported the results of
pre-operative embolization for hypervascular spinal tumors and have
clearly shown that the technique is safe and effective at reducing
intraoperative blood loss (11–13).
In a study on spinal metastases from renal cell carcinoma (15), the median intraoperative blood loss
was recorded as 1,500 ml (range 300–8,000 ml). Wilson et al
(16) reported that the mean
estimated level of intraoperative blood loss of the primary spine
tumors was 1,562 ml. Similarly in the present study, the estimated
mean level of blood loss was 1,528.6 ml.
In the present study, a gelatin sponge was used as
the embolic agent, which is a temporary vascular occlusive agent
that is degraded by proteolytic enzymatic pathways and resorbed
within seven to 21 days after embolization (17). The majority of authors suggest that
surgery should be performed within 24 h to prevent pre-operative
recanalization or tumor revascularization via collaterals (12). We agree that subsequent surgery
should be performed within 24 h, but the present study observed
that the level of blood loss was usually not large if embolization
occurred within two days. The average level of blood loss of
patients who underwent surgery within one day post-embolization was
1,626.1 ml and the average level of blood loss of patients who
underwent surgery within two days was 1,080 ml; no significant
difference was observed (P>0.05). In the present study, gelfoam
particles were used to embolize the small intratumoral arteries and
then gelfoam strips were used to embolize the stem of the
tumor-feeding artery. With this method, all tumor-feeding arteries
may be embolized completely and the risk of hemorrhage from
anastomoses of the lateral branches may be decreased.
Pre-operative transarterial embolization for tumors
of the spine is a relatively safe procedure, but it does carry
certain risks. The most catastrophic complication is spinal cord
ischemia associated with the embolization of unrecognized
radiculomedullary arteries. Finstein et al (18) reported a case of post-embolization
paralysis and paresthesia in a patient with a thoracolumbar GCT.
Although, this complication is extremely rare, careful analysis of
the pre-embolization angiograms is essential to identify and
protect the radiculomedullary and spinal arteries. Angiography
should be performed prior to embolization to define the vascular
anatomy. The presence of a radiculomedullary artery supplying the
spinal cord and a dangerous intersegmental anastomosis should not
be missed.
Although histologically benign, GCTs are locally
aggressive and the local recurrence rate is significantly higher in
the spine compared with the extremities. Sanjay et al
(4) reported a recurrence rate of
42% from 24 patients with GCTs of the spine at the Mayo Clinic.
Although, the optimal treatment of GCTs in the sacrum and spine
remains controversial, complete excision is recommended.
Theoretically, en bloc resection with either a marginal or wide
resection margin is able to decrease the recurrence rate, although
the duration of surgery, level of blood loss and perioperative
complication rates of this procedure are high (19,20).
In the review of Cloyd et al (21), the duration of surgery averaged 12.1
h and lasted as long as 42 h, while the mean blood loss was 3.7
liters, with one patient losing as much as 37 liters. Certain
authors (8,9,22) have
recommended conservative surgery (curettage or intralesional
excision), which has a lower morbidity and less neurological
deficits. These are accompanied by certain other advantages,
including the preservation of the stability of the spine and
pelvis, the speed and ease of the surgical procedure and the
potential for reduced blood loss. In the present study, all the
patients underwent pre-operative transarterial embolization, which
reduced the intraoperative blood loss and allowed the surgical
margin of the tumor to be identified clearly. The recurrence rate
of the present study was 28.6%, which is lower than or equal to
that reported in the literature (4,23).
The complications observed included kyphosis,
cerebrospinal fluid leakage and wound complications. Wound
complications occurred in six sacral cases and are the most
frequent complications following a posterior approach in the
sacrum, requiring long and intensive treatment (6,24). We
suggest that two effective suction drainage tubes should be placed
to aid in the prevention of hematomas developing in the large dead
spaces.
The functional outcomes of the present study were
satisfactory. In the sacrum, 13 of the 15 patients remained active
with a full range of motion in their lower extremities, while the
remaining two patients were able to walk with sticks. Of the 15
patients with sacrum GCT, four patients experienced bowel or
bladder dysfunction. When bilateral S2 nerve roots and the
unilateral S3 nerve root were preserved, 8 of 10 patients had
normal bowel and bladder function. Bilateral S2 nerve roots were
preserved in 3 patients and all of them had normal bowel and
bladder function. In the remaining 2 patients, only the unilateral
S2 nerve roots were preserved and all of them had bowel and bladder
dysfunction. This is similar to the study by Todd et al
(24), which demonstrated that the
preservation of at least the unilateral S3 nerve root is extremely
important for patients in order to sustain normal bowel and bladder
function. In the mobile spine, all 13 patients had no residual
neurological deficits at final follow-up and were able to perform
normal daily activities. However, Martin et al (23) reported that seven out of 13 spinal
GCT patients had either chronic pain or residual neurological
deficits. These may be attributed to pre-operative transarterial
embolization, which is used to reduce intraoperative hemorrhaging
and provide a clear surgical field and adequate curettage. We
suggest that if the nerve roots or spinal dura mater is
contaminated with the tumor cell during surgery, the membrane
should be dissected carefully. Following the removal of the tumor,
the surgical field was covered thoroughly with 95% ethyl alcohol
gauze, then cleaned with warm normal saline. Sterilized distilled
water was used to lyse the residual microscopic tumor debris.
Compared with techniques used in the historical
literature, pre-operative embolization significantly decreases the
level of intraoperative blood loss, makes the surgical field clear
and facilitates the maximal removal of the tumor. Pre-operative
embolization followed by intralesional resection is able to achieve
satisfactory local control and clinical outcomes. It is an
effective technique for excising GCTs of the sacrum and spine.
However, further comprehensive studies are required and a control
group would be necessary to strengthen the results.
References
|
1.
|
Luther N, Bilsky MH and Härtl R: Giant
cell tumor of the spine. Neurosurg Clin N Am. 19:49–55. 2008.
View Article : Google Scholar
|
|
2.
|
Unni KK: Giant cell tumor (Osteoclastoma).
Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases. 5th
edition. Lippincott Williams & Wilikins; Philadelphia, PA: pp.
263–283. 1996
|
|
3.
|
Turcotte RE, Sim FH and Unni KK: Giant
cell tumor of the sacrum. Clin Orthop Relat Res. 291:215–221.
1993.PubMed/NCBI
|
|
4.
|
Sanjay BK, Sim FH, Unni KK, Mcleod RA and
Klassen RA: Giant-cell tumours of the spine. J Bone Joint Surg Br.
75:148–154. 1993.PubMed/NCBI
|
|
5.
|
Hosalkar HS, Jones KJ, King JJ and Lackman
RD: Serial arterial embolization for large sacral giant-cell
tumors: mid- to long-term results. Spine (Phila Pa 1976).
32:1107–1115. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Leggon RE, Zlotecki R, Reith J and
Scarborough MT: Giant cell tumor of the pelvis and sacrum: 17 cases
and analysis of the literature. Clin Orthop Relat Res. 423:196–207.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Harrop JS, Schmidt MH, Boriani S and
Shaffrey CI: Aggressive ‘benign’ primary spine neoplasms
osteoblastoma, aneurysmal bone cyst, and giant cell tumor. Spine
(Phila Pa 1976). 34(22 Suppl): S39–S47. 2009.
|
|
8.
|
Ozaki T, Liljenqvist U, Halm H, Hillmann
A, Gosheger G and Winkelmann W: Giant cell tumor of the spine. Clin
Orthop Relat Res. 401:194–201. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Takeda N, Kobayashi T, Tandai S, Matsuno
T, Shirado O, Watanabe T and Minami A: Treatment of giant cell
tumors in the sacrum and spine with curettage and argon beam
coagulator. J Orthop Sci. 14:210–214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Shimada Y, Hongo M, Miyakoshi N, Kasukawa
Y, Ando S, Itoi E and Abe E: Giant cell tumor of fifth lumbar
vertebrae: two case reports and review of the literature. Spine J.
7:499–505. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Guzman R, Dubach-Schwizer S, Heini P,
Lovblad KO, Kalbermatten D, Schroth G and Remonda L: Pre-operative
transarterial embolization of vertebral metastases. Eur Spine J.
14:263–268. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Ozkan E and Gupta S: Embolization of
spinal tumors: vascular anatomy, indications, and technique. Tech
Vasc Interv Radiol. 14:129–140. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Shi HB, Suh DC, Lee HK, et al:
Pre-operative transarterial embolization of spinal tumor:
Embolization techniques and results. AJNR Am J Neuroradiol.
20:2009–2015. 1999.PubMed/NCBI
|
|
14.
|
Rodrigues LM, Nicolau RJ, Puertas EB and
Milani C: Vertebrectomy of giant cell tumor with vertebral artery
embolization: case report. J Pediatr Orthop B. 18:99–102. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Manke C, Bretschneider T, Lenhart M,
Strotzer M, Neumann C, Gmeinwieser J and Feuerbach S: Spinal
metastases from renal cell carcinoma: effect of pre-operative
particle embolization on intraoperative blood loss. AJNR Am J
Neuroradiol. 22:997–1003. 2001.PubMed/NCBI
|
|
16.
|
Wilson MA, Cooke DL, Ghodke B and Mirza
SK: Retrospective analysis of pre-operative embolization of spinal
tumors. AJNR Am J Neuroradiol. 31:656–660. 2010. View Article : Google Scholar
|
|
17.
|
Yang HL, Chen KW, Wang GL, et al:
Pre-operative transarterial embolization for treatment of primary
sacral tumors. J Clin Neurosci. 17:1280–1285. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Finstein JL, Chin KR, Alvandi F and
Lackman RD: Postembolization paralysis in a man with a
thoracolumbar giant cell tumor. Clin Orthop Relat Res. 453:335–340.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Fidler MW: Surgical treatment of giant
cell tumours of the thoracic and lumbar spine: report of nine
patients. Eur Spine J. 10:69–77. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Wuisman P, Lieshout O, Sugihara S and van
Dijk M: Total sacrectomy and reconstruction: oncologic and
functional outcome. Clin Orthop Relat Res. 381:192–203. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Cloyd JM, Acosta FL Jr, Polley MY and Ames
CP: En bloc resection for primary and metastatic tumors of the
spine: a systematic review of the literature. Neurosurgery.
67:435–444. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Guo W, Ji T, Tang XD and Yang Y: Outcome
of conservative surgery for giant cell tumor of the sacrum. Spine
(Phila Pa 1976). 34:1025–1031. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Martin C and McCarthy EF: Giant cell tumor
of the sacrum and spine: series of 23 cases and a review of the
literature. Iowa Orthop J. 30:69–75. 2010.PubMed/NCBI
|
|
24.
|
Todd LT, Yaszemski MJ, Currier BL, Fuchs
B, Kim CW and Sim FM: Bowel and bladder function after major sacral
resection. Clin Orthop Relat Res. 397:36–39. 2002. View Article : Google Scholar : PubMed/NCBI
|