Introduction
Chronic obstructive pulmonary disease (COPD) is one
of the leading causes of morbidity and mortality worldwide, which
is characterized by irreversible or partly reversible progressive
limitation of the airflow (1,
2). Cigarette smoking is the major
risk factor, but only 10–15% of long-term smokers develop
symptomatic airflow obstruction (3,
4). This indicates that the genetic
factors may contribute to the individual susceptibility for the
development of COPD. Numerous studies have shown that genetic
factors are likely to have a role in determining the susceptibility
of an individual to COPD (1,
2, 5–8), and
genetic variants in the vitamin D-binding protein (VDBP)
gene have also been linked to COPD risk (7, 9,
10).
VDBP (also known as Gc-globulin) is expressed in a
number of tissues, such as liver, kidney, gonads and fat (11). Notably, VDBP is also expressed by
human neutrophils (12),
contributes to macrophage activation (13), augments monocyte and neutrophil
chemotaxis to C5-derived peptides and acts as a scavenger protein
to clear extracellular G-actin released from necrotic cells
(14, 15). Additionally, VDBP is the major
plasma carrier protein of vitamin D, deficiency of which may also
be linked to COPD (7, 16, 17).
The human VDBP gene (GC) has been localized to chromosome
4q11-q13 and is highly polymorphic, with three commonly recognized
variants (GC*1F, GC*1S and GC*2) caused by non-synonymous
single-nucleotide polymorphisms (SNPs; rs7041 and rs4588) and
>120 rarer variants (18).
GC*1F, GC*1S and GC*2 are not alleles as such, but haplotypes
composed of combinations of the SNPs at these loci, so an
individual may be homozygous or heterozygous for each variant,
depending on the two haplotypes present. The role of GC
polymorphisms in COPD has been explored in a number of studies by
investigating the association of GC variants and susceptibility of
COPD (9, 10, 19–25).
However, the results of these studies were inconclusive and may not
be powerful enough due to the limited sample size. To evaluate the
overall effect of the haplotypic association between the GC
polymorphisms (rs7041 and rs4588) and COPD risk, a meta-analysis
was conducted in the present study by pooling all the available
data together.
Materials and methods
Identification of eligible
studies
To identify all the eligible studies that
investigated the haplotypic association of the GC rs7041 and rs4588
polymorphisms with COPD risk, a comprehensive electronic search of
Web of Science, PubMed, Google Scholar, Embase, Cochrane Library,
China National Knowledge Infrastructure and Wanfang Database was
performed until June 1, 2014. Various combinations of the following
medical subject headings and key words were applied in order to
include the maximum number of studies associated as possible:
Vitamin D-binding protein, VDBP, GC or Gc-globulin; rs7041 or
rs4588; and chronic obstructive pulmonary disease, COPD;
polymorphisms, variants or haplotypes. Furthermore, the reference
lists of the reviews and retrieved studies were manually screened
for additional studies. There were no restrictions for language and
only published studies with full-text studies were included.
Inclusion and exclusion criteria
The studies identified from the above-mentioned
databases were screened by two independent investigators according
to the following predesigned inclusion criteria: i) Case-control
design; ii) evaluating the correlation of GC haplotypes (at
position rs7041 and rs4588) with COPD risk; and iii) providing
sufficient data to calculate the odds ratio (OR) and its
corresponding 95% confidence interval (CI). When several studies
with overlapping data were eligible, those with smaller sample size
or less reliability were excluded. In addition, the studies without
detailed information were excluded, following the efforts to
extract data from the original study or failure of contact with the
corresponding authors.
Data extraction
Data from the eligible studies were extracted by two
investigators independently and in duplicate according to the
predesigned data-collection form. The following information was
extracted: Last name of the first author, publication year, country
of origin, ethnicity, source of controls, number of the two COPD
cases, control subjects and phenotypic distribution in the two
groups. Different ethnicities were categorized as Asian and
Caucasian. Discrepancies occurring during the process of study
inclusion and data extraction were resolved by discussion with a
third investigator and consensus on each item was achieved
eventually.
Data analysis
The statistical analysis was conducted using STATA
software (version 12.0; Stata Corporation, College Station, TX,
USA). The ORs of COPD were recalculated and compared between
GC*1F-1F and non GC*1F-1F, GC*1F-1S and non GC*1F-1S, GC*1S-1S and
non GC*1S-1S, GC*2-1S and non GC*2-1S, GC*2-1F and non GC*2-1F, and
GC*2–2 and non GC*2–2. Heterogeneity among studies was examined
with the χ2-based Q testing and I2 statistics
(26). When there was a significant
heterogeneity (P<0.10), a random-effects model (the DerSimonian
and Laird method) was selected to pool the data (27). Otherwise, a fixed-effects model (the
Mantel-Haenszel method) was selected to pool the data (28). Publication bias was examined with
funnel plots Begg and Egger tests (29, 30).
When no publication bias existed, the funnel plot was considered as
symmetrical. The statistical significance of the pooled OR was
assessed with the Z test and P<0.05 was considered to indicate a
statistically significant difference. For the Egger's tests, the
significance level was also set at 0.05. Subgroup analyses were
also conducted to assess any moderating effects of ethnicity
(Caucasian and Asian) on ORs derived from each study.
Results
Characteristics of the eligible
studies
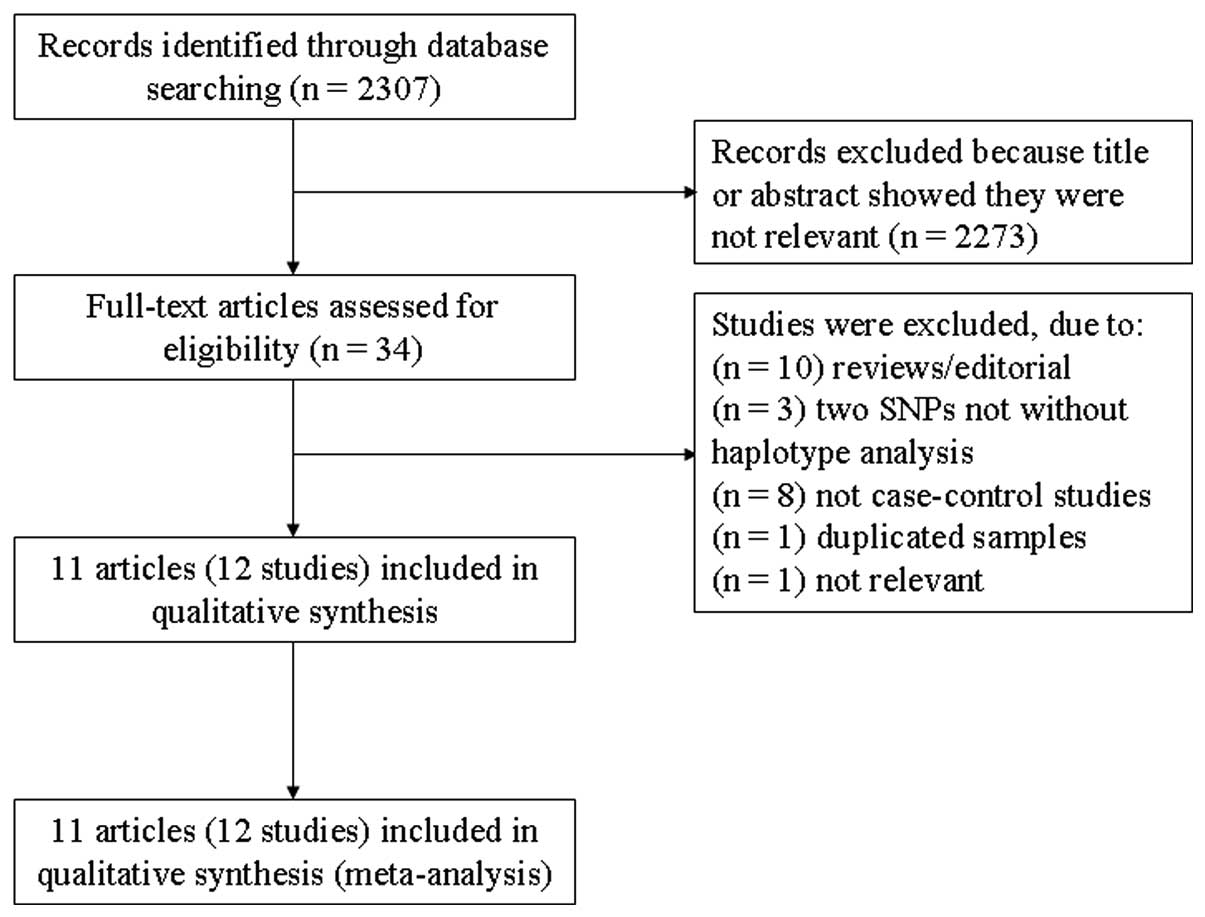
A total of 2,307 studies were obtained with the
initial search of databases. Following screening, 12 case-control
studies in 11 eligible studies with a total of 2,937 participants
(1,190 cases and 1,747 controls) fulfilled the inclusion criteria
(9, 10, 19–25,
31, 32), from which genotype data of the GC
polymorphisms (rs7041 and rs4588) were obtained (shown in Table I). The flowchart of reviews
demonstrates the detailed process of selection (Fig. 1). As for ethnicity, seven studies
investigated the Caucasian population (21, 23–25,
31, 32) and five studies investigated the
Asian population (9, 10, 19,
20, 22). The qualities of these studies were
considered accessible for the meta-analysis.
 | Table I.Main characteristics of all the
eligible studies. |
Table I.
Main characteristics of all the
eligible studies.
|
Genotype
frequencies of GC haplotypes (rs7041-rs4588) |
|---|
|
|
|---|
| Cases | Control |
|---|
|
|
|
|---|
| First author | Year | Country | Ethnicity | Source of
controls | No. of
case/control | 1F-1F | 1F-1S | 1S-1S | 2-1S | 2-1F | 2–2 | 1F-1F | 1F-1S | 1S-1S | 2-1S | 2-1F | 2–2 | (Refs.) |
|---|
| Wood | 2011 | UK | Caucasian | HS | 93/351 | 0 | 2 | 39 | 41 | 1 | 10 | 0 | 0 | 145 | 150 | 0 | 56 | (24) |
| Shen | 2010 | China | Asian | HS | 100/100 | 35 | 20 | 7 | 13 | 22 | 3 | 13 | 26 | 4 | 12 | 29 | 16 | (10) |
| Huang | 2007 | China | Asian | HS | 75/69 | 24 | 21 | 2 | 8 | 18 | 2 | 8 | 18 | 3 | 7 | 20 | 13 | (19) |
| Korytina | 2006 | Rep of Bashk | Caucasian | HS | 131/106 | 8 | 26 | 30 | 29 | 25 | 13 | 12 | 39 | 14 | 25 | 9 | 7 | (21) |
| Korytina | 2006 | Russia | Caucasian | HS | 166/130 | 14 | 31 | 42 | 49 | 20 | 10 | 14 | 29 | 25 | 45 | 12 | 5 | (21) |
| Lu | 2004 | China | Asian | HS | 69/52 | 23 | 15 | 5 | 9 | 16 | 1 | 6 | 16 | 3 | 8 | 14 | 5 | (22) |
| Laufs | 2004 | Iceland | Caucasian | HS | 102/183 | 1 | 11 | 39 | 35 | 5 | 11 | 2 | 24 | 68 | 67 | 8 | 14 | (25) |
| Ito | 2004 | Japan | Asian | HS | 103/88 | 33 | 29 | 3 | 11 | 25 | 2 | 15 | 27 | 5 | 10 | 30 | 1 | (9) |
| Ishii | 2001 | Japan | Asian | HS | 63/82 | 23 | 15 | 1 | 6 | 16 | 2 | 17 | 27 | 5 | 8 | 18 | 7 | (20) |
| Schellenberg | 1998 | UK | Caucasian | HS | 75/64 | 41 | | | 32 | | 2 | 31 | | | 24 | | 9 | (23) |
| Horne | 1990 | USA | Caucasian | HS | 104/413 | 6 | 24 | 40 | 23 | 3 | 8 | 5 | 66 | 141 | 134 | 25 | 42 | (32) |
| Kueppers | 1977 | USA | Caucasian | HS | 109/109 | 62 | | | 46 | | 1 | 57 | | | 47 | | 5 | (31) |
Meta-analysis of haplotypes and the
association with COPD
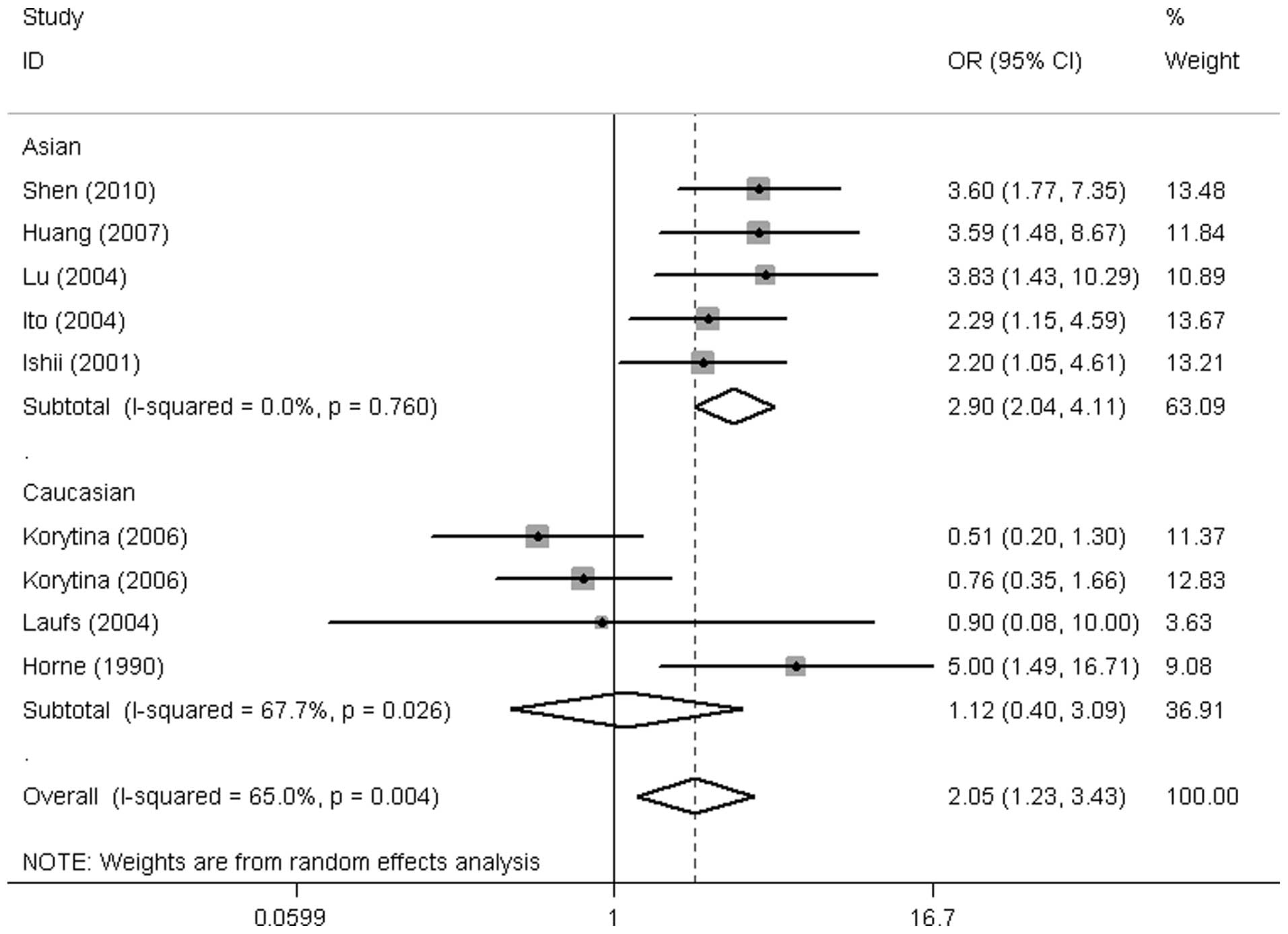
Overall, among the six haplotypes of the VDBP
gene (GC*1F-1F, GC*1F-1S, GC*1S-1S, GC*2-1S, GC*2-1F and GC*2–2), a
significantly increased risk was observed in GC*1F homozygotes
(GC*1F-1F vs. non GC*1F-1F: OR=2.02, 95% CI: 1.23-3.43, P=0.006)
and no association between other GC haplotypes and COPD risk were
detected (Fig. 2 and Table II).
| Table II.Results of the meta-analysis for
haplotypes (rs7041-rs4588). |
Table II.
Results of the meta-analysis for
haplotypes (rs7041-rs4588).
| Meta-analysis | Heterogeneity |
|---|
|
|
|
|---|
| Genetic model | Pooled OR (95%
CI) | POR | I2,
% | P-value | Bias P-value |
|---|
| 1F-1F vs. non
1F-1F | 2.052
(1.227–3.431)a |
0.006a |
65.0 |
0.004 |
0.883 |
| 1.115
(0.402–3.090)b |
0.834 |
67.7 |
0.026 |
0.667 |
| 2.922
(2.064–4.136)a, c |
1.47E-09a |
0.0 |
0.760 |
0.287 |
| 1F-1S vs. non
1F-1S | 0.808
(0.651–1.003) |
0.054 |
0.0 |
0.629 |
0.427 |
| 0.830
(0.617–1.117)b |
0.220 |
28.6 |
0.246 |
0.671 |
| 0.784
(0.572–1.074)c |
0.130 |
0.0 |
0.801 |
0.563 |
| 1S-1S vs. non 1S-1S | 1.174
(0.947–1.456) |
0.144 |
0.0 |
0.604 |
0.327 |
| 1.223 (0.974–1.536)b |
0.083 |
0.0 |
0.566 |
0.059 |
| 0.837 (0.434–1.615)c |
0.595 |
0.0 |
0.470 |
0.088 |
| 2-1S vs. non 2-1S | 0.864
(0.707–1.056) |
0.152 |
0.0 |
0.935 |
0.463 |
| 0.835 (0.666–1.047)b |
0.118 |
0.0 |
0.554 |
0.853 |
| 0.980 (0.633–1.515)c |
0.927 |
0.0 |
0.995 |
0.540 |
| 2-1F vs. non 2-1F | 0.937
(0.726–1.209) |
0.616 |
30.0 |
0.179 |
0.739 |
| 1.340 (0.869–2.067)b |
0.185 |
44.8 |
0.142 |
0.269 |
| 0.774 (0.563–1.062)c |
0.113 |
0.0 |
0.753 |
0.174 |
| 2–2 vs. non 2–2 | 0.610
(0.308–1.207) |
0.155 |
71.5 |
0.000 |
0.112 |
| 1.033 (0.505–2.129)b |
0.929 |
68.1 |
0.004 |
0.443 |
| 0.212 (0.105–0.428)a, c |
1.51E-05a |
3.5 |
0.387 |
0.285 |
According to ethnicity, the results demonstrated a
markedly increased risk in Asians with GC*1F homozygotes, but not
in Caucasians (GC*1F-1F vs. non GC*1F-1F; OR, 2.92; 95% CI,
2.06-4.14; P=1.47E-09; OR, 1.12; 95% CI, 0.40-3.09; P=0.834,
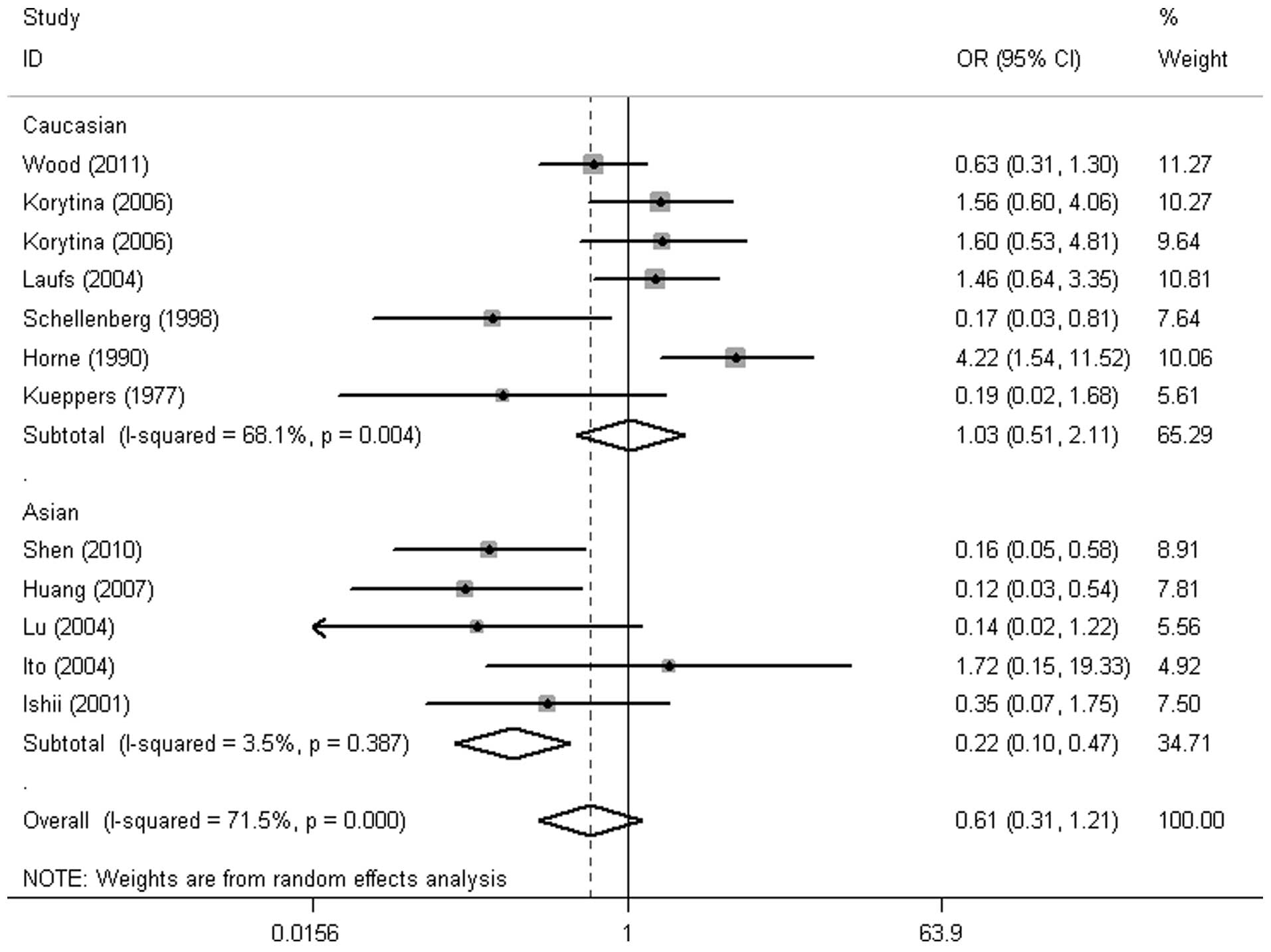
respectively) (Fig. 3 and Table II). In addition, GC*2 homozygotes
in Asians were at lower risk of COPD (GC*2–2 vs. non GC*2–2: OR,
2.21; 95% CI, 0.11-0.43; P=1.51E-05) (Fig. 4). No significant association was
observed in the other haplotypes (Table II).
Sensitivity analysis
Sensitivity analysis was also performed to explore
the potential influence of each individual study on the overall
results by deleting one single study each time from the pooled
analysis. No substantial change was demonstrated in the overall
studies, indicating that no individual study affected the pooled OR
significantly (data not shown).
Heterogeneity and publication
bias
Among the six haplotypes, significant heterogeneity
was observed in the GC*1F homozygotes and GC*2 homozygotes with
P<0.10; subsequent to stratifying for populations, no
significant heterogeneity was observed in Asians, but the
heterogeneity remained significant in Caucasians. For publication
bias, no significant results were observed with all P>0.05 of
Egger's test. Additionally, funnel plots of haplotypes did not show
significant publication bias either. Results of heterogeneity and
publication bias are shown in Table
II.
Discussion
In the present study, the results indicated that the
GC*1F-1F homozygote carriers have an increased risk of COPD.
However, following subgroup analysis by ethnicity, a significant
increased risk of COPD was found in Asians, but not in Caucasians.
The GC*2–2 homozygote carriers in Asians may have a decreased risk
of COPD.
To the best of our knowledge, this is the first
meta-analysis of the VBDP gene polymorphsims and COPD
susceptibility. In the present meta-analysis, 12 eligible studies
were combined with 1,190 cases and 1,747 controls to yield summary
statistics, indicating that the GC*1F-1F homozygotes of the
VDBP gene were associated with the COPD risk among the
overall population (Table II).
According to ethnicity, the GC*1F homozygotes were considered as a
risk factor for COPD in Asian populations, while the presence of
the GC*2 homozygotes may be one of the protective factors against
COPD in Asians (Table II). These
findings on the correlation between GC polymorphisms and COPD were
indirectly supported by the evidence that the VDBP gene
influenced vitamin D concentrations and was associated to forced
expiratory volume in one second (7,
24). However, the results from the
present analyses failed to reveal the significant association
between the GC polymorphisms and COPD susceptibility among
Caucasians, this was extremely different from the findings by Horne
et al (32) and Schellenberg
et al (23), but consistent
with the findings by other studies (21, 25,
31, 33). This may be due to the fact that
other factors, such as the differences in age, gender, lifestyle
factors, clinical characteristics or the analysis method of the
VDBP genotype may have influenced the results. The frequency
difference between Caucasians and Asians may be a cause of variable
association with COPD between these two ethnic groups and studies
based on larger well-designed populations are required to clarify
the associations between the VDBP gene polymorphism and COPD
susceptibility.
The heterogeneity is of note when interpreting the
meta-analysis results. For the significant and stable results of
the GC polymorphisms in the majority of models, there was no or
low-to moderate heterogeneity (indicated by
I2-statistics) among studies (see Table II). However, relatively clear
heterogeneity was observed in the models of GC*1F-1F and GC*2–2 in
Caucasians, which may have been responsible for the negative
results.
The current meta-analysis focused on the combined
effects of the VDBP gene rs7041 and rs4588 polymorphisms
rather than one single SNP on COPD risk (7, 34),
which may help to derive a precise estimation of the roles of
VDBP SNPs in the development of COPD episodes. However,
several limitations should be considered when interpreting the
results. First, the limited number of COPD cases and control
subjects may lead to a relatively small power. Second, the
heterogeneity was not resolved following subgroup analyses in
certain cases, indicating that other factors, such as the
differences in age, gender, lifestyle factors or clinical
characteristics, may have caused heterogeneity. Third, only
published studies with sufficient data were included, and
therefore, publication bias may have occurred even though results
of the Begg's and Egger's tests did not detect it.
In conclusion, the present meta-analysis indicated
that the GC*1F homozygotes of the VDBP gene may be a risk
factor for COPD among Asian populations, while the presence of the
GC*2 homozygotes may be one of the protective factors against COPD
in Asians. Larger and well-designed studies based on different
ethnic groups are required to confirm our results.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81070045) and the
Key Clinical Project for the Affiliated Hospital of the Ministry of
Public Health of China (grant no. 111). The authors would like to
acknowledge the reviewers for their helpful comments on the
study.
References
|
1
|
Vijayan VK: Chronic obstructive pulmonary
disease. Indian J Med Res. 137:251–269. 2013.PubMed/NCBI
|
|
2
|
Barczyk A and Pierzchala W: Diagnostic and
treatment of chronic obstructive pulmonary disease based on GOLD
statement 2011. Pol Merkur Lekarski. 33:187–192. 2012.(In Polish).
PubMed/NCBI
|
|
3
|
Fletcher C and Peto R: The natural history
of chronic airflow obstruction. Br Med J. 1:1645–1648. 1977.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Faner R, Gonzalez N, Cruz T, Kalko SG and
Agusti A: Systemic inflammatory response to smoking in chronic
obstructive pulmonary disease: evidence of a gender effect. PLoS
One. 9:e974912014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moher D, Liberati A, Tetzlaff J and Altman
DGPRISMA Group: Preferred reporting items for systematic reviews
and meta-analyses: the PRISMA statement. PLoS Med. 6:e10000972009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Issac MS, Ashur W and Mousa H: Genetic
polymorphisms of surfactant protein D rs2243639, Interleukin
(IL)-1beta rs16944 and IL-1RN rs2234663 in chronic obstructive
pulmonary disease, healthy smokers, and non-smokers. Mol Diagn
Ther. 18:343–354. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li X, Liu X, Xu Y, et al: The correlation
of vitamin D level and vitamin D-binding protein gene polymorphism
in chronic obstructive pulmonary disease. Zhonghua Nei Ke Za Zhi.
53:303–307. 2014.(In Chinese). PubMed/NCBI
|
|
8
|
Kauffmann F, Kleisbauer JP,
Cambon-De-Mouzon A, et al: Genetic markers in chronic air-flow
limitation. A genetic epidemiologic study. Am Rev Respir Dis.
127:263–269. 1983.PubMed/NCBI
|
|
9
|
Ito I, Nagai S, Hoshino Y, et al: Risk and
severity of COPD is associated with the group-specific component of
serum globulin 1F allele. Chest. 125:63–70. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shen LH, Zhang XM, Su DJ, et al:
Association of vitamin D binding protein variants with
susceptibility to chronic obstructive pulmonary disease. J Int Med
Res. 38:1093–1098. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
McLeod JF and Cooke NE: The vitamin
D-binding protein, alpha-fetoprotein, albumin multigene family:
detection of transcripts in multiple tissues. J Biol Chem.
264:21760–21769. 1989.PubMed/NCBI
|
|
12
|
Kew RR, Sibug MA, Liuzzo JP and Webster
RO: Localization and quantitation of the vitamin D binding protein
(Gc-globulin) in human neutrophils. Blood. 82:274–283.
1993.PubMed/NCBI
|
|
13
|
Yamamoto N and Homma S: Vitamin D3 binding
protein (group-specific component) is a precursor for the
macrophage-activating signal factor from
lysophosphatidylcholine-treated lymphocytes. Proc Natl Acad Sci
USA. 88:8539–8543. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Binder R, Kress A, Kan G, Herrmann K and
Kirschfink M: Neutrophil priming by cytokines and vitamin D binding
protein (Gc-globulin): impact on C5a-mediated chemotaxis,
degranulation and respiratory burst. Mol Immunol. 36:885–892. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
McLeod JF, Kowalski MA and Haddad JG Jr:
Interactions among serum vitamin D binding protein, monomeric
actin, profilin, and profilactin. J Biol Chem. 264:1260–1267.
1989.PubMed/NCBI
|
|
16
|
Janssens W, Bouillon R, Claes B, et al:
Vitamin D deficiency is highly prevalent in COPD and correlates
with variants in the vitamin D-binding gene. Thorax. 65:215–220.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Janssens W, Lehouck A, Carremans C,
Bouillon R, Mathieu C and Decramer M: Vitamin D beyond bones in
chronic obstructive pulmonary disease: time to act. Am J Respir
Crit Care Med. 179:630–636. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cleve H and Constans J: The mutants of the
vitamin-D-binding protein: more than 120 variants of the GC/DBP
system. Vox Sang. 54:215–225. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Huang P, Ma Y, Du X, Chen J, Song B and
Hong Y: The vitamin D-binding protein gene polymorphism in chronic
obstructive pulmonary disease patients. Zhonghua Jie He He Hu Xi Za
Zhi. 30:780–781. 2007.(In Chinese).
|
|
20
|
Ishii T, Keicho N, Teramoto S, et al:
Association of Gc-globulin variation with susceptibility to COPD
and diffuse panbronchiolitis. Eur Respir J. 18:753–757. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Korytina GF, Akhmadishina LZ, Ianbaeva DG
and Viktorova TV: Genotypes of vitamin-D-binding protein (DBP) in
patients with chronic obstructive pulmonary disease and healthy
population of Republic Bashkortostan. Mol Biol (Mosk). 40:231–238.
2006.(In Russian). View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lu M, Yang B and Cai YY: The relationship
between vitamin D binding protein gene polymorphism and chronic
obstructive pulmonary disease. Zhonghua Nei Ke Za Zhi. 43:117–120.
2004.(In Chinese). PubMed/NCBI
|
|
23
|
Schellenberg D, Pare PD, Weir TD, Spinelli
JJ, Walker BA and Sandford AJ: Vitamin D binding protein variants
and the risk of COPD. Am J Respir Crit Care Med. 157:957–961. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wood AM, Bassford C, Webster D, et al:
Vitamin D-binding protein contributes to COPD by activation of
alveolar macrophages. Thorax. 66:205–210. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Laufs J, Andrason H, Sigvaldason A, et al:
Association of vitamin D binding protein variants with chronic
mucus hypersecretion in Iceland. Am J Pharmacogenomics. 4:63–68.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Der Simonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mantel N and Haenszel W: Statistical
aspects of the analysis of data from retrospective studies of
disease. J Natl Cancer Inst. 22:719–748. 1959.PubMed/NCBI
|
|
29
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kueppers F, Miller RD, Gordon H, Hepper NG
and Offord K: Familial prevalence of chronic obstructive pulmonary
disease in a matched pair study. Am J Med. 63:336–342. 1977.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Horne SL, Cockcroft DW and Dosman JA:
Possible protective effect against chronic obstructive airways
disease by the GC2 allele. Hum Hered. 40:173–176. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wood AM, Needham M, Simmonds MJ, Newby PR,
Gough SC and Stockley RA: Phenotypic differences in alpha 1
antitrypsin-deficient sibling pairs may relate to genetic
variation. COPD. 5:353–359. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bakke PS, Zhu G, Gulsvik A, et al:
Candidate genes for COPD in two large data sets. Eur Respir J.
37:255–263. 2011. View Article : Google Scholar : PubMed/NCBI
|