Introduction
The incidence and mortality of colorectal cancer
(CRC) have been increasing in Japan (1). Therefore, screening is crucial for the
early detection of CRC. The faecal occult blood test (FOBT) is a
simple, low-cost, non-invasive screening method. Although annual or
biennial guaiac-based FOBT screening reduces the incidence of CRC
by 17–20% (2) and CRC mortality by
16–33% (3–5), this screening method has been criticised
due to its poor sensitivity (6,7).
Immunochemical FOBT (iFOBT) exhibits improved sensitivity and
specificity and involves no dietary restrictions, resulting in
fewer abnormalities due to interfering substances (8). Therefore, iFOBT has been recommended as
a population-based CRC screening test in Japan since 1992 (9). Colonoscopy (CS) is the most accurate
test for detecting early cancer and for detecting and removing
advanced adenomas (10–17). However, due to its potential
limitations, low availability of qualified endoscopists and high
cost, CS is considered an opportunistic screening or detailed
examination method for patients with positive FOBT results in
population-based screening. Therefore, the characteristics of
FOBT-negative colorectal tumours may not be evident, as patients do
not generally undergo CS when their FOBT results are negative.
The aim of this study was to elucidate the
characteristics of iFOBT-negative colorectal tumours in
asymptomatic patients who underwent opportunistic screening in our
hospital.
Materials and methods
Patients
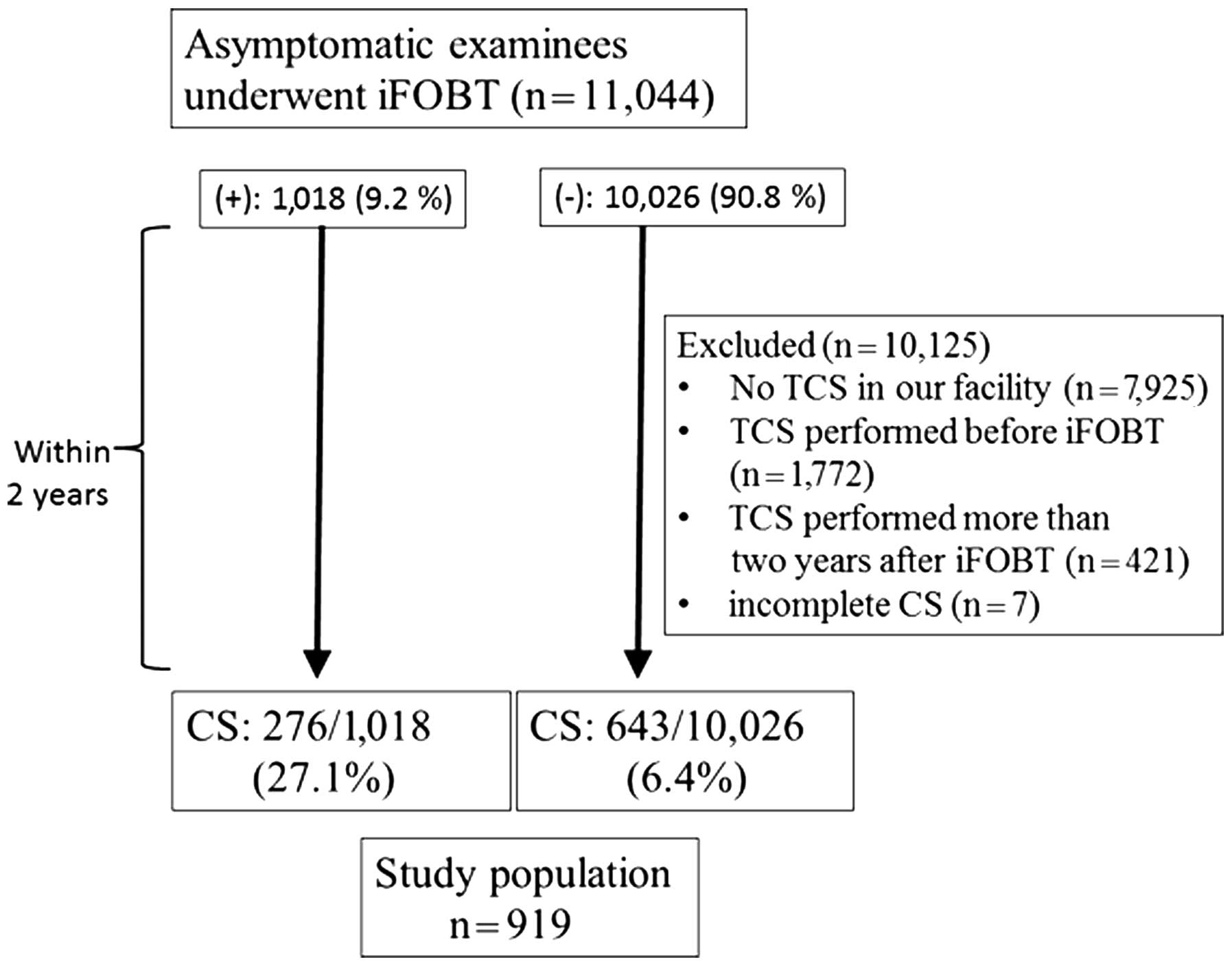
Between December, 2001 and August, 2012, iFOBT was
performed in 11,044 subclinical patients in the health screening
program of Showa University Northern Yokohama Hospital (Yokohama,
Japan). The study protocol from iFOBT to CS is outlined in Fig. 1. Total colonoscopy (TCS) involved CS
from the caecum to the rectum. A total of 7,801 patients did not
undergo TCS or underwent TCS in other facilities, 2,317 underwent
TCS prior to iFOBT, 421 underwent TCS >2 years after iFOBT and 7
underwent incomplete CS. For these reasons, 10,125 patients were
excluded from this study. A total of 919 patients (27.1%
iFOBT-positive and 6.4% iFOBT-negative) underwent TCS in our
facility within 2 years after iFOBT, regardless of the test
results. All the eligible patients were asymptomatic. The patients
were divided into iFOBT-positive and -negative groups and the
characteristics of TCS were compared between the two groups within
2 years after iFOBT.
This study's protocol was approved by the Clinical
Research Ethics Committee of Showa University Northern Yokohama
Hospital. The study was performed in accordance with the principles
of the Declaration of Helsinki. This study is registered in the
University Hospital Medical Network Clinical Trials Registry
(UMIN000012116). We used individual and endoscopic data from the
database of Showa University Northern Yokohama Hospital and written
informed consent for TCS was obtained from all the examinees prior
to conducting the original procedures.
iFOBT
We performed 1-day iFOBT. The patients were asked to
prepare a faecal sample from a specimen using an iFOBT kit. The
OC-Hemodia was used between December, 2001 and March, 2008 and the
OC-Hemocatch S between April, 2008 and August, 2012 (both from
Eiken Chemical Co., Ltd., Tokyo, Japan). The faecal sample was
delivered to the hospital within 3 days and tested immediately.
CS examination and pathological
findings
All the patients underwent bowel preparation with
2–3 l polyethylene glycol solution prior to CS. Diazepam and
butylscopolamine were intravenously administered for sedation and
prevention of peristalsis. All the detected lesions were
endoscopically examined at ~80- to 100-fold magnification
(CF-240ZI, CF-H260AZI, or PCF-240ZI; Olympus, Tokyo, Japan).
Following conventional examination, the shape of each lesion was
classified according to the Paris classification system (18). For colour staining, 0.2% indigo
carmine dye and 0.05% crystal violet were applied directly through
the endoscope channel and the pit pattern was determined according
to the Kudo's pit pattern classification with the magnifying view
(19–22). The Kudo's classification system
involves morphological analysis of the colorectal crypts for
diagnosis. The pattern is classified as one of five typesas
follows: type I, round pits; type II, stellar pits; type III,
tubular or small, roundish pits; type IV, branch-like or gyrus-like
pits; and type V, irregular or non-structural pits (19,21–23).
Lesions with type I or II patterns are defined as non-neoplastic.
Type III, IV, or VI low-grade patterns are defined as
adenoma (including high-grade dysplasia) or slightly invasive
cancer that may be completely resected with endoscopy. Type
VI high-grade and type VN patterns are
defined as massively invasive cancer. The degree of submucosal
invasion was classified into two groups: Slightly invasive
submucosal cancer (SMs; invasion depth <1,000 µm) and massively
invasive submucosal cancer (SMm; invasion depth ≥1,000 µm)
(23,24). SMs does not metastasise as readily as
adenomas, making it a good indication for endoscopic resection,
whereas SMm exhibits nodal metastasis (~10%), thus requiring
surgical resection. All the observed lesions with data on the pit
pattern findings, location, shape and diameter were documented in
the electronic medical charts. The CS findings were classified
according to the most advanced histological lesion found and the
results were expressed in terms of number of patients and number of
polyps. When neither polyps (adenomatous, hyperplastic, juvenile or
inflammatory) nor cancer was detected, the CS findings were
classified as normal. If possible, all the observed neoplastic
lesions were removed endoscopically or surgically and other lesions
were biopsied if necessary. If histopathological evaluation was not
possible (e.g., the specimen could not be collected, the patient
was on oral anticoagulants, or numerous lesions were present), the
pit pattern diagnosis was substituted for the pathological
diagnosis. When the location of the lesions was analysed, the
distal colon was defined as the rectum plus the sigmoid and
descending colon, whereas the proximal colon was defined as the
transverse and ascending colon plus the caecum.
The pathological findings were evaluated by
experienced pathologists in our facility. Patients with
intramucosal carcinoma or carcinoma in situ were considered
to have high-grade dysplasia. CRC was defined as invasion of the
malignant cells beyond the muscularis mucosae. Advanced neoplasia
(AN), which was considered to require intensive therapy, was
defined as a CRC or advanced adenoma (adenoma ≥10 mm in size, ≥20%
villous component, or high-grade dysplasia). Non-AN was defined as
an adenoma of <10 mm, without a villous component. Neoplasia was
defined as CRC, advanced adenoma, or non-AN.
Outcome measures and statistical
analysis
SPSS for Windows version 20.0 statistical software
(IBM Corp., Chicago, IL, USA) was used for data analysis. For
descriptive findings, quantitative data are presented as means and
standard deviations (SDs) and categorical variables are presented
as percentages. Differences in demographic characteristics between
participants with positive and negative faecal test results were
determined using the Student's t-test, χ2 test, or
Fisher's exact test. A two-tailed P-value of <0.05 indicated
statistical significance.
Results
Patient characteristics
Of the 11,044 patients, 926 underwent CS within 2
years after iFOBT. The remaining 919 patients (564 men and 355
women) were included in the study. Of the 919 patients, 721
underwent TCS for the first time in our facility; the remaining
patients had a history of previous TCS in our facility.
The demographic characteristics of the included
patients are summarised in Table I.
The mean age of the patients was 58.0 years (SD, 11.7 years). The
average inspection interval between iFOBT and CS was 365.2 days
(SD, 214.71 days). Of the 919 patients, 276 were included in the
iFOBT-positive and 643 in the iFOBT-negative group. No significant
differences in age were present between the two groups. However,
the male-to-female ratio was significantly higher in the
iFOBT-negative compared with that in the iFOBT-positive group
(P<0.05). Additionally, the inspection interval between iFOBT
and CS was significantly longer in the iFOBT-negative group
(P<0.001). Neoplastic lesions were observed in 318 of the 643
iFOBT-negative patients (49.3%) and in 213 of the 276
iFOBT-positive patients (77.2%). The average tumour size (including
adenomas <10 mm) was significantly smaller in the iFOBT-negative
compared with that in the iFOBT-positive group (4.36±3.96 vs.
5.81±6.54 mm, respectively; P<0.001) (Table II). AN was observed in 40 of the 643
iFOBT-negative patients (6.2%) and in 52 of the 276 iFOBT-positive
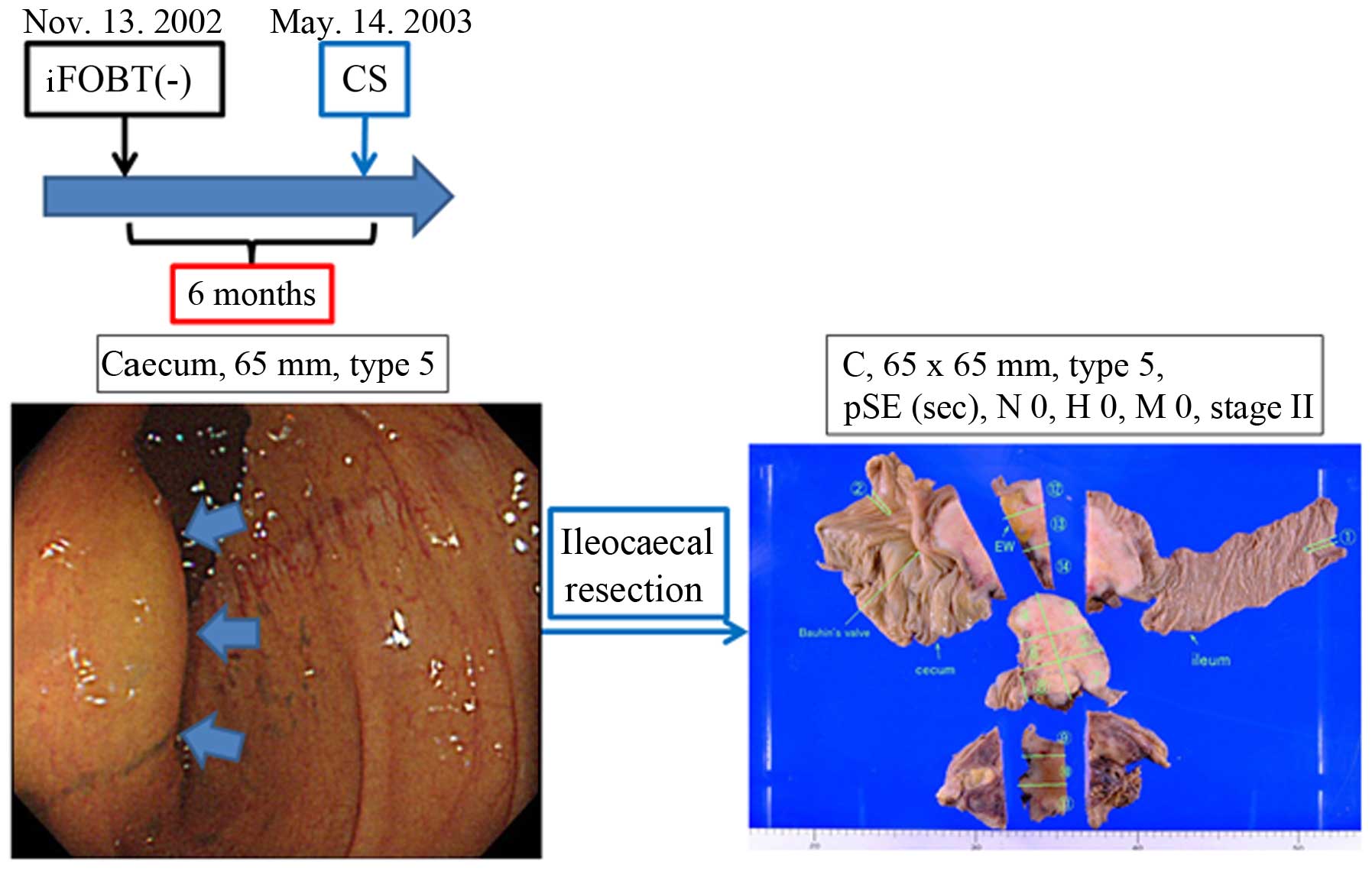
patients (18.8%). CRC was observed in 1 of the 643 iFOBT-negative
patients (0.16%) (Fig. 2) and in 10
of the 276 iFOBT-positive patients (3.62%). The detection rates of
neoplasia, AN and CRC were significantly lower in the
iFOBT-negative compared with that in the iFOBT-positive group
(P<0.001). The number of non-AN lesions was 470 in the
iFOBT-negative group and 338 in the iFOBT-positive group. The ratio
of non-AN lesions was significantly higher in the iFOBT-negative
compared with the iFOBT-positive group (91.6 vs. 82.4%,
respectively; P<0.001).
 | Table I.Demographic characteristics of
patients according to iFOBT results. |
Table I.
Demographic characteristics of
patients according to iFOBT results.
| Variables | iFOBT-negative
(n=643) | iFOBT-positive
(n=276) | P-value |
|---|
| Gender,
male/female | 409/234 | 155/121 | <0.05 |
| Age, years (mean ±
SD) | 57.7±11.2 | 58.5±12.7 | 0.3431 |
| iFOBT to CS interval,
days (mean ± SD) | 379±200 | 131±131 | <0.001 |
| Neoplasia |
|
|
|
|
Cases/total (%) | 318/643 (49.3) | 213/276 (77.2) | <0.001 |
| Total
lesions | 513 | 410 |
|
| Non-advanced
neoplasia |
|
|
|
|
Cases/total (%) | 260/643 (40.4) | 181/276 (65.6) | <0.001 |
| Total
lesions | 470 | 338 |
|
| Advanced
neoplasia |
|
|
|
|
Cases/total (%) | 40/643 (6.2) | 52/276 (18.8) | <0.001 |
| Total
lesions | 43 | 72 |
|
| Advanced
adenoma |
|
|
|
|
Cases/total (%) | 39/643 (6.1) | 43/276 | <0.001 |
| Total
lesions | 42 | 61 (15.6) |
|
| Colorectal
cancer |
|
|
|
|
Cases/total (%) | 1/643 (0.16) | 10/276 (3.62) | <0.001 |
| Total
lesions | 1 | 11 |
|
| Table I.Comparison of neoplasm
characteristics between the two groups. |
Table I.
Comparison of neoplasm
characteristics between the two groups.
| Variables | iFOBT-negative (513
lesions) | iFOBT-positive (410
lesions) | P-value |
|---|
| Non-advanced
neoplasia | 470 | 338 |
|
| Average
size, mm (mean ± SD) | 3.68±1.44 | 3.89±1.58 | 0.05 |
|
Location, proximal/total
(%) | 260/470 (55.3) | 191/338 (56.5) | 0.737 |
|
Shapea, protruding/total (%) | 198/470 (42.1) | 190/338 (56.2) | <0.001 |
| Advanced
neoplasia | 43 | 72 |
|
| Average
size, mm (mean ± SD) | 11.8±10.3 | 14.8±11.6 | 0.080 |
|
Location, proximal/total
(%) | 20/43 (46.5) | 28/72 (38.9) | 0.423 |
|
Shapea, protruding/total (%) | 20/42a (47.6) | 43/68a (63.2) | 0.108 |
| Advanced
adenoma | 42 | 61 |
|
| Average
size, mm (mean ± SD) | 10.5±6.24 | 12.3±7.39 | 0.197 |
|
Location, proximal/total
(%) | 19/42 (45.2) | 25/61 (41.0) | 0.668 |
| Shape,
protruding/total (%) | 20/42 (47.6) | 41/61 (68.3) | <0.05 |
| Colorectal
cancer | 1 | 11 |
|
| Average
size (mm) | 65.0 | 28.6±19.5 |
|
|
Location, proximal/total
(%) | 1/1 (100) | 3/11 (27.3) | 0.333 |
|
Shapea, protruding/total (%) | (advanced
cancer) | 2/7a (18.2) |
|
| Combined (total
neoplasia) | 513 | 410 |
|
| Average
size, mm (mean ± SD) | 4.36±3.96 | 5.8±6.54 | <0.001 |
|
Location, proximal/total
(%) | 280/513 (54.6) | 219/410 (53.4) | 0.724 |
|
Shapea, protruding/total (%) |
218/512a
(42.6) |
233/406a
(57.4) | <0.001 |
| Rate of
non-advanced neoplasia | 470/513 (91.6) | 338/410 (82.4) | <0.001 |
| Rate of
advanced neoplasia | 43/513 (8.4) | 72/410 (17.6) | <0.001 |
| Rate of
advanced adenoma | 42/513 (8.2) | 61/410 (14.9) | <0.01 |
| Rate of
colorectal cancer | 1/513 (0.19) | 11/410 (2.7) | <0.01 |
Neoplasm characteristics
The comparison of neoplasm characteristics between
the two groups is summarised in Table
II. The number of AN lesions was 43 in the iFOBT-negative group
(CRC, n=1; high-grade dysplasia, n=6; adenoma ≥10 mm, n=21; and
tubulovillous adenoma, n=15) and 72 in the iFOBT-positive group
(CRC, n=11; high-grade dysplasia, n=19; adenoma ≥10 mm, n=31; and
tubulovillous adenoma, n=11). The ratios of CRC and AN were
significantly lower in the iFOBT-negative compared with those in
the iFOBT-positive group (0.19 vs. 2.7% and 8.4 vs. 17.6%,
respectively; P<0.001). With respect to location, the rate of
proximal-sided neoplasia (neoplasia or AN or CRC) tended to be
higher in the iFOBT-negative compared with that in the
iFOBT-positive group; however, there were no significant
differences between the two groups. With respect to shape
(excluding advanced CRC), the ratio of protruding neoplasia was
significantly lower in the iFOBT-negative compared with that in the
iFOBT-positive group.
Discussion
The effect of FOBT screening on the reduction of
mortality due to CRC has been established (3–5). However,
due to the imperfect sensitivity of FOBT, a certain risk of missing
advanced lesions is always present (25,26).
Although a number of previous studies have reported the performance
of iFOBT, CS was not performed in iFOBT-negative patients (25,26).
Additionally, certain studies on iFOBT invited asymptomatic
patients with negative iFOBT results to undergo CS to validate the
test results (27–31). To date, very few studies have
investigated the characteristics of colorectal tumours in
iFOBT-negative patients. As we sought to characterise colon tumours
using our original diagnostic standard with magnifying endoscope
technology (19–21), we were specifically interested in the
characteristics of neoplastic lesions in iFOBT-negative patients
and have herein attempted to elucidate the incidence, location and
shape of these lesions. The aim of the present study was to
determine the characteristics of colonic neoplasms that tend to be
missed by iFOBT screening. The knowledge obtained herein may be
useful in cancer screening using CS, particularly for patients
without iFOBT results.
As expected, the incidence and average size of
neoplasia, non-AN, AN and CRC were lower in iFOBT-negative compared
with that in iFOBT-positive patients. Unfortunately, we identified
no characteristic findings that were significantly specific to
iFOBT-negative patients. However, there were certain potentially
informative findings that provided clues to determining the weak
points of iFOBT. First, although there were no differences in
tumour location between the two groups, AN in iFOBT-negative
patients tended to be located in the proximal colon more often
compared with AN in iFOBT-positive patients. Additionally, CRC in
iFOBT-negative patients, which only involved one lesion in this
study, was also found in the proximal colon; this case of an
iFOBT-negative CRC, which infiltrated the serosa, is shown in
Fig. 2. These findings suggest that
patients with tumours in the proximal colon may have negative iFOBT
results, even when the tumours have malignant potential. Second,
the rate of protruding non-AN (small lesions) was significantly
lower in iFOBT-negative compared with iFOBT-positive patients. This
tendency was not significantly evident for AN, suggesting that
lesion size more significantly affected the sensitivity of iFOBT
rather than lesion shape. However, the rate of protruding total
neoplasia (non-AN and AN) was significantly lower in iFOBT-negative
compared with that in iFOBT-positive patients. These results
suggest that proximal and/or non-protruding (particularly small)
tumours may be iFOBT-negative.
Sessile serrated adenoma/polyps (SSA/P), which were
recently recognised as precancerous lesions of CRC, also tend to be
proximally located and of the flat-elevated type (i.e., 0-IIa or
0-IIb in the Paris classification) (32,33). This
characteristic feature corresponds with their tendency to be missed
by iFOBT in the present study. In fact, we observed three cases of
histologically proven SSA/P (average diameter ± SD of 16.0±4.62
mm), but all three were iFOBT-negative. This finding indicates that
SSA/P may be missed during CRC surveillance using iFOBT.
The iFOBT was confirmed as an excellent method of
CRC screening, as the detection rate of CRC was significantly
higher in iFOBT-positive compared with that in iFOBT-negative
patients (3.62 vs. 0.16%, respectively). Moreover, the detection
rate of AN was lower in iFOBT-negative compared with that in
iFOBT-positive patients (8.4 vs. 17.6%, respectively). However, it
should be emphasised that neoplasia was found in almost half
(49.3%) of the iFOBT-negative patients, suggesting that iFOBT
screening is insufficient for targeting neoplasia, irrespective of
the malignant potential of the neoplasia. In particular, 6.3% of
the iFOBT-negative patients had AN, including 1 patient with CRC
who required therapeutic intervention. We consider that this number
is not insignificant and requires clinical attention. Park et
al (26) also reported that the
sensitivity for AN was markedly lower compared with that for CRC.
As advanced adenoma is considered to be a precancerous lesion
(31), endoscopic treatment for these
lesions may reduce the incidence and mortality of CRC. Therefore,
regularly conducting iFOBT alone for cancer screening is
insufficient for detecting all CRC lesions; it is necessary to
occasionally complement iFOBT with CS to compensate for the
inaccuracy of iFOBT.
Our study had several limitations. First, we used
the 1-day iFOBT, despite an earlier study recommending 2-day iFOBT,
which is more cost-effective compared with the 1-day iFOBT
(27). However, the compliance
associated with the 2-day method is lower, as it involves more
complicated procedures. The 1-day method was used in our study to
allow for simpler data analysis. In fact, CRC screening programs
vary among countries. For example, Australia uses the annual 2-day
iFOBT, most European countries use the annual 1-day iFOBT and Italy
uses the biennial 1-day iFOBT (27–30,34,35).
The second limitation is that this study focused on patients
undergoing CS within 2 years after iFOBT. The interval of 2 years
may be relatively long, since, with the exception of Italy, CRC
screening in several countries is performed annualy. The third
limitation is that the population of the present study did not
comprise the participants of a population-based screening program,
but rather the participants of an opportunistic screening program.
According to a 2009 national survey by the Japanese Society of
Gastrointestinal Cancer Screening, the CRC detection rate was
0.051% (1,617/3,195,750) in opportunistic screening and 0.21%
(5,309/2,508,0197) in population-based screening (http://www.jsgcs.or.jp/files/uploads/iinkai_h21.pdf).
Moreover, the patients in the population-based screening program
tended to be older compared with those in the opportunistic
screening program. The survey also reported that the adenoma and
CRC detection rates increased with age. We therefore expect the CRC
and adenoma detection rates to be higher in population-based
screening compared with those in the present study. The fourth
limitation is that this was a retrospective study that may contain
selection bias, compromising the ability to generalize the study
results. Several patients were excluded from this study (n=10,125).
However, the majority of the excluded patients were iFOBT-negative
patients who did not undergo TCS in the population-based screening.
In fact, 9,383 of the 10,125 excluded patients were iFOBT-negative.
Therefore, a prospective follow-up study in which iFOBT-negative
patients undergo TCS is desired.
Despite these limitations, our study demonstrated
the clinical significance of CS during CRC screening. Nishihara
et al (17) also reported that
the multivariate hazard ratio for death from CRC was 0.32 (95% CI:
0.24–0.45) after screening CS. CS may detect small, non-protruding
and proximally located colorectal tumours in iFOBT-negative
patients. In particular, as certain precancerous lesions that are
curable with endoscopic therapy are not detectable by iFOBT,
screening using CS is crucial for reducing the mortality and
incidence of CRC.
Acknowledgements
We would like to express our appreciation to Daisuke
Watanabe (Kobe University), Nobunao Ikehara (Ikehara Clinic) and
Yoko Tanaka (Showa University Northern Yokohama Hospital) for their
instructive advice regarding this article.
References
|
1
|
Wan DS: Epidemiologic trend of and
strategies for colorectal cancer. Ai Zheng. 28:897–902. 2009.(In
Chinese). PubMed/NCBI
|
|
2
|
Mandel JS, Church TR, Bond JH, Ederer F,
Geisser MS, Mongin SJ, Snover DC and Schuman LM: The effect of
fecal occult-blood screening on the incidence of colorectal cancer.
N Engl J Med. 343:1603–1607. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kronborg O, Fenger C, Olsen J, Jørgensen
OD and Søndergaard O: Randomised study of screening for colorectal
cancer with faecal-occult-blood test. Lancet. 348:1467–1471. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hardcastle JD, Chamberlain JO, Robinson
MH, Moss SM, Amar SS, Balfour TW, James PD and Mangham CM:
Randomised controlled trial of faecal-occult-blood screening for
colorectal cancer. Lancet. 348:1472–1477. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mandel JS, Bond JH, Church TR, Snover DC,
Bradley GM, Schuman LM and Ederer F: Reducing mortality from
colorectal cancer by screening for fecal occult blood. Minnesota
Colon Cancer Control Study. N Engl J Med. 328:1365–1371. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Imperiale TF, Ransohoff DF, Itzkowitz SH,
Turnbull BA and Ross MEColorectal Cancer Study Group: Fecal DNA
versus fecal occult blood for colorectal-cancer screening in an
average-risk population. N Engl J Med. 351:2704–2714. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rozen P, Levi Z, Hazazi R, Waked A, Vilkin
A, Maoz E, Birkenfeld S and Niv Y: Quantitative colonoscopic
evaluation of relative efficiencies of an immunochemical faecal
occult blood test and a sensitive guaiac test for detecting
significant colorectal neoplasms. Aliment Pharmacol Ther.
29:450–457. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Saito H, Soma Y, Nakajima M, Koeda J,
Kawaguchi H, Kakizaki R, Chiba R, Aisawa T and Munakata A: A
case-control study evaluating occult blood screening for colorectal
cancer with hemoccult test and an immunochemical hemagglutination
test. Oncol Rep. 7:815–819. 2000.PubMed/NCBI
|
|
9
|
Saito H: Screening for colorectal cancer:
Current status in Japan. Dis Colon Rectum. 43 (Suppl):S78–S84.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Imperiale TF, Glowinski EA, Lin-Cooper C,
Larkin GN, Rogge JD and Ransohoff DF: Five-year risk of colorectal
neoplasia after negative screening colonoscopy. N Engl J Med.
359:1218–1224. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Baxter NN, Goldwasser MA, Paszat LF,
Saskin R, Urbach DR and Rabeneck L: Association of colonoscopy and
death from colorectal cancer. Ann Intern Med. 150:1–8. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kahi CJ, Imperiale TF, Juliar BE and Rex
DK: Effect of screening colonoscopy on colorectal cancer incidence
and mortality. Clin Gastroenterol Hepatol. 7:770–775; quiz.
7112009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brenner H, Haug U, Arndt V, Stegmaier C,
Altenhofen L and Hoffmeister M: Low risk of colorectal cancer and
advanced adenomas more than 10 years after negative colonoscopy.
Gastroenterology. 138:870–876. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Brenner H, Chang-Claude J, Seiler CM and
Hoffmeister M: Long-term risk of colorectal cancer after negative
colonoscopy. J Clin Oncol. 29:3761–3767. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Brenner H, Chang-Claude J, Seiler CM,
Rickert A and Hoffmeister M: Protection from colorectal cancer
after colonoscopy: A population-based, case-control study. Ann
Intern Med. 154:22–30. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Quintero E, Castells A, Bujanda L,
Cubiella J, Salas D, Lanas Á, Andreu M, Carballo F, Morillas JD,
Hernández C, et al: Role: COLONPREV Study InvestigatorsColonoscopy
versus fecal immunochemical testing in colorectal-cancer screening.
N Engl J Med. 366:697–706. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nishihara R, Wu K, Lochhead P, Morikawa T,
Liao X, Qian ZR, Inamura K, Kim SA, Kuchiba A, Yamauchi M, et al:
Long-term colorectal-cancer incidence and mortality after lower
endoscopy. N Engl J Med. 369:1095–1105. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Participants in the Paris Workshop, . The
Paris endoscopic classification of superficial neoplastic lesions:
esophagus, stomach, and colon: November 30 to December 1, 2002.
Gastrointest Endosc. 58 (Suppl):S3–S43. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kudo S, Hirota S, Nakajima T, Hosobe S,
Kusaka H, Kobayashi T, Himori M and Yagyuu A: Colorectal tumours
and pit pattern. J Clin Pathol. 47:880–885. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kudo S, Rubio CA, Teixeira CR, Kashida H
and Kogure E: Pit pattern in colorectal neoplasia: Endoscopic
magnifying view. Endoscopy. 33:367–373. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kashida H and Kudo SE: Early colorectal
cancer: Concept, diagnosis, and management. Int J Clin Oncol.
11:1–8. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang Q, Fukami N, Kashida H, Takeuchi T,
Kogure E, Kurahashi T, Stahl E, Kudo Y, Kimata H and Kudo SE:
Interobserver and intra-observer consistency in the endoscopic
assessment of colonic pit patterns. Gastrointest Endosc.
60:520–526. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kudo S, Tamura S, Nakajima T, Yamano H,
Kusaka H and Watanabe H: Diagnosis of colorectal tumorous lesions
by magnifying endoscopy. Gastrointest Endosc. 44:8–14. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tsuruta O, Toyonaga A, Ikeda H, Tanikawa K
and Morimatsu M: Clinicopathological study of superficial-type
invasive carcinoma of the colorectum. Int J Oncol. 10:1003–1008.
1997.PubMed/NCBI
|
|
25
|
van Rossum LG, van Rijn AF, van Oijen MG,
Fockens P, Laheij RJ, Verbeek AL, Jansen JB and Dekker E: False
negative fecal occult blood tests due to delayed sample return in
colorectal cancer screening. Int J Cancer. 125:746–750. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Park DI, Ryu S, Kim Y-H, Lee SH, Lee CK,
Eun CS and Han DS: Comparison of guaiac-based and quantitative
immunochemical fecal occult blood testing in a population at
average risk undergoing colorectal cancer screening. Am J
Gastroenterol. 105:2017–2025. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nakama H, Zhang B and Fattah AS: A
cost-effective analysis of the optimum number of stool specimens
collected for immunochemical occult blood screening for colorectal
cancer. Eur J Cancer. 36:647–650. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bampton PA, Sandford JJ, Cole SR, Smith A,
Morcom J, Cadd B and Young GP: Interval faecal occult blood testing
in a colonoscopy based screening programme detects additional
pathology. Gut. 54:803–806. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Smith A, Young GP, Cole SR and Bampton P:
Comparison of a brush-sampling fecal immunochemical test for
hemoglobin with a sensitive guaiac-based fecal occult blood test in
detection of colorectal neoplasia. Cancer. 107:2152–2159. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
van Rossum LG, van Rijn AF, Laheij RJ, van
Oijen MG, Fockens P, van Krieken HH, Verbeek AL, Jansen JB and
Dekker E: Random comparison of guaiac and immunochemical fecal
occult blood tests for colorectal cancer in a screening population.
Gastroenterology. 135:82–90. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lieberman DA, Rex DK, Winawer SJ,
Giardiello FM, Johnson DA and Levin TRUnited States Multi-Society
Task Force on Colorectal Cancer: Guidelines for colonoscopy
surveillance after screening and polypectomy: A consensus update by
the US Multi-Society Task Force on Colorectal Cancer.
Gastroenterology. 143:844–857. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Jass JR: Hyperplastic-like polyps as
precursors of microsatellite-unstable colorectal cancer. Am J Clin
Pathol. 119:773–775. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lambert R, Kudo SE, Vieth M, Allen JI,
Fujii H, Fujii T, Kashida H, Matsuda T, Mori M, Saito H, et al:
Pragmatic classification of superficial neoplastic colorectal
lesions. Gastrointest Endosc. 70:1182–1199. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Castiglione G, Grazzini G, Miccinesi G,
Rubeca T, Sani C, Turco P and Zappa M: Basic variables at different
positivity thresholds of a quantitative immunochemical test for
faecal occult blood. J Med Screen. 9:99–103. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Morikawa T, Kato J, Yamaji Y, Wada R,
Mitsushima T, Sakaguchi K and Shiratori Y: Sensitivity of
immunochemical fecal occult blood test to small colorectal
adenomas. Am J Gastroenterol. 102:2259–2264. 2007. View Article : Google Scholar : PubMed/NCBI
|