Introduction
Neck mass can develop due to infectious,
inflammatory, congenital, traumatic, benign, or malignant causes
(1). Exclusion of other diseases
is essential for the accurate diagnosis of neck mass (1-4).
Lymphoma accounts for 12% of all malignant tumors
occurring in the head and neck region and is the third most common
malignant tumor after squamous cell carcinoma and thyroid cancer
(5). Lymphomas are generally
classified into Hodgkin lymphoma and non-Hodgkin lymphoma (1,3,5).
Hodgkin lymphoma typically occurs in the lymph nodes of the neck,
while non-Hodgkin lymphoma can spread to extranodal sites,
including the major salivary glands, paranasal sinuses and Waldeyer
ring (1). Non-Hodgkin lymphoma
accounts for ~90% of all lymphoma (5). Treatment of malignant lymphoma is
very diverse and treatment is only possible with an accurate
diagnosis (5,6). Treatment of malignant lymphoma is
very diverse and treatment is only possible with an accurate
diagnosis (6). The prognosis of
patients with early-stage disease was improved compared with that
of patients with late-stage disease (5).
In malignant lymphoma, multiple neck masses are one
of the most common manifestations (1,4).
However, there have been recent cases where a solitary large neck
mass was diagnosed as malignant lymphoma on definitive biopsy.
Therefore, the present study examined the clinical characteristics
of patients with a final diagnosis of solitary large malignant
lymphoma in the head and neck region following surgery at a
hospital.
Patients and methods
The present study received approval from the
Institutional Review Board of Chonnam National University Hwasun
Hospital (approval no. CNUHH-2023-021). Patients with a final
diagnosis of solitary large malignant lymphoma in the head and neck
region after surgery between January 2015 and December 2022 were
enrolled. All cases that did not meet this criteria were
excluded.
Clinical data obtained from the patients were
reviewed, including sex, age, past medical history, symptoms,
duration of symptoms, site, number and size of malignant lymphoma,
preoperative fine-needle aspiration cytology (FNAC), preoperative
diagnosis, final histopathologic results after surgery,
postoperative treatment, postoperative complications, current
status and follow-up.
One or more radiological examinations, including
computed tomography, magnetic resonance imaging and ultrasound,
were conducted for all patients before surgery to assess the extent
of the lesion and assist with treatment planning. All surgical
specimens were confirmed by histopathological examination with
immunophenotyping.
Results
The clinical findings of 13 patients with solitary
large malignant lymphoma of the head and neck are summarized in w
I. Of the 13 patients with solitary large malignant lymphoma, eight
were male and five female. The mean age of the patients was
50.7±23.2 years (range; 15-80 years). Examination of past medical
history identified three patients with hypertension, one with
angina and one with liver cirrhosis.
The most common symptom of solitary large malignant
lymphoma was a neck mass (n=11; 84.6%). Two patients with malignant
lymphoma of the tongue complained of foreign body sensation in the
throat (n=1) and coughing (n=1). None complained of B symptoms such
as fever, chill and weight loss. The duration of symptoms was
2.4±3.4 months (range; 0.2-12 months). Overall, 6 patients (46.2%)
had right-sided malignant lymphoma and seven patients (53.8%) had
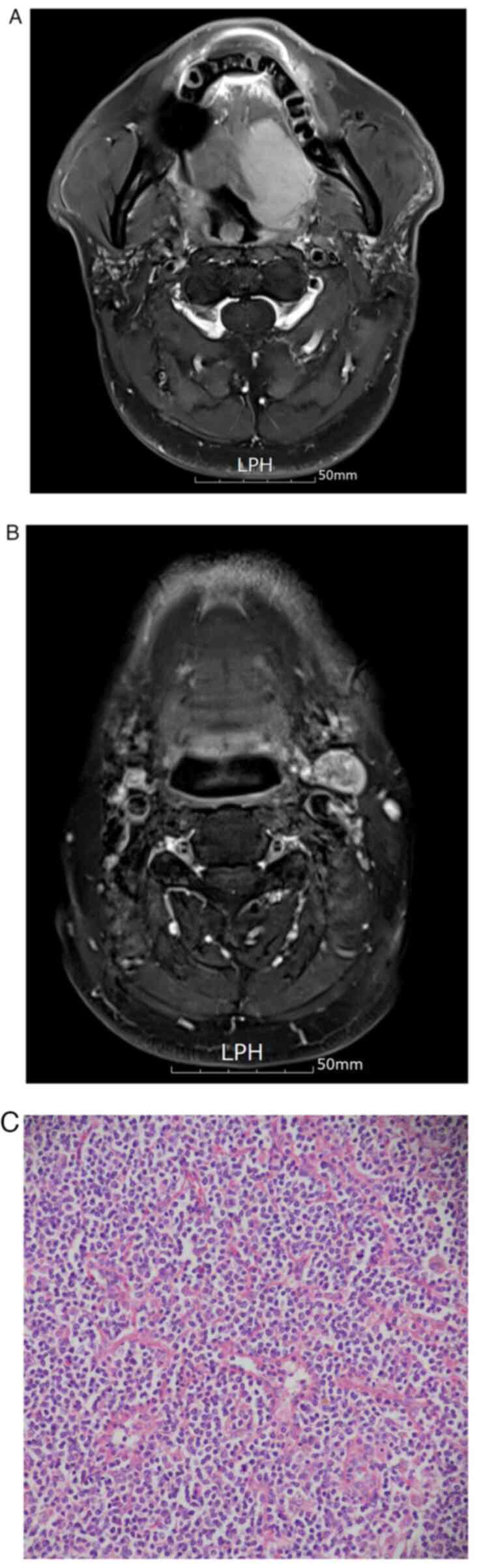
left-sided malignant lymphoma. The most common sites of solitary
large malignant lymphoma in the head and neck region were neck
level II in eight patients, neck level IV in two patients, parotid
glands in two patients and the tongue in two patients. One patient
had masses both on the tongue and at neck level II (Fig. 1).
The number of malignant lymphomas was as follows: 11
patients had one large tumor and two patients had two large tumors.
The mean tumor size was 4.0±1.3 cm (range; 2.7-6.8 cm). Among the
two patients with two lymphomas, the size of the second neck mass
was 3.2 cm in one patient and 2.7 cm in the other. Preoperative
FNAC was performed on 11 patients (84.6%). FNAC results identified
four patients with reactive lymphadenitis, three patients with
atypical lymphoid lesion, three patients with non-diagnostic
results and one patient with poorly differential malignancy. The
preoperative diagnosis (based on imaging tests, physical
examination and FNAC results) was benign neck mass in seven cases,
malignant lymphoma in three cases, parotid tumors in two cases and
metastatic carcinoma in one case.
All patients underwent surgical resection under
general anesthesia and were diagnosed with malignant lymphoma based
on the final histopathologic biopsy. There were no major
complications after surgery. The most common type of solitary large
malignant lymphoma was diffuse large B-cell lymphoma (n=6; 46.2%),
followed by follicular lymphoma (n=3), classic Hodgkin lymphoma
(n=2), angioimmunoblastic T-cell lymphoma (n=1) and marginal zone
B-cell lymphoma (n=1).
A total of 11 patients (84.6%) received
postoperative treatment, including chemotherapy (n=8), radiation
therapy (n=2), or both (n =1). The remaining two patients underwent
periodic follow-up without any treatment. A total of 12 patients
are currently under follow-up without disease recurrence after the
completion of treatment and one patient diagnosed 1 month ago is
currently undergoing radiation therapy. The follow-up period was
47.3±19.0 months (range; 1-62 months).
Discussion
In the present study, analysis of solitary large
malignant lymphoma in the head and neck region demonstrated that
neck mass was the most common symptom and mainly occurred at neck
level II. Of the 13 patients with malignant lymphoma, 11 of them
had a single large neck mass with a mean size of 4.0 cm. The
remaining two patients had two neck masses and all four neck masses
were larger than 2.7 cm. The most common type of solitary large
malignant lymphoma was diffuse large B-cell lymphoma (46.2%).
Although various tests such as FNAC, imaging tests
and blood tests were performed, only three patients (23.1%) were
diagnosed as having malignant lymphoma before surgery. FNAC is a
highly accurate, safe and cost-effective method, which is widely
used in initial tests for the histopathological evaluation of neck
masses (1). However, it is not
recommended for the diagnosis of malignant lymphoma because the
tumor tissue architecture cannot be obtained (1,6).
Based on the FNAC results of the present study, malignancy was
found in only one case and atypical lymphoid lesions were suspected
in three cases.
On imaging tests, malignant lymphoma is
characterized by a round-shaped morphology with a size of >1 cm
and multiple or conglomerate neck lymph nodes (4,7). In
the present study, the possibility of malignant lymphoma before
surgery was not considered because it mainly appeared as a solitary
large neck mass on imaging tests.
Accurate diagnosis and treatment of solitary large
malignant lymphoma requires multidisciplinary collaboration
(5,6). The histopathologic examination
through surgical excision and subtype confirmation through
immunophenotyping are essential (1-7).
Treatment for malignant lymphoma of the head and neck may include
systemic chemotherapy with or without radiation therapy.
Immunotherapy, high-dose chemotherapy and stem cell transplant are
also treatment options (1,3,5).
All patients survived without recurrence of
malignant lymphoma except for one patient who was recently
diagnosed and is receiving treatment. In addition, two patients
with pediatric-type follicular lymphoma are being followed up
without any recurrence and without additional treatment other than
surgery.
In summary, a solitary large neck mass should be
considered as a differential disease of malignant lymphoma in the
head and neck region and histopathologic results obtained through
surgical excision could accurately confirm the diagnosis.
The present study has limitations in that the
retrospective nature of the study, which may introduce bias in data
collection and analysis. Additionally, the reliance on surgical
resection for diagnosis may not be feasible in all cases and may
limit the applicability of the findings to patients who are not
surgical candidates.
The possibility of solitary large malignant lymphoma
in the head and neck region should be considered. As it is
difficult to accurately diagnose solitary large malignant lymphoma
before surgery, surgical resection is required to differentiate it
from other diseases.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
DHL and DNL conducted and designed the research. DHL
and DNL confirm the authenticity of all the raw data. DHL and SCL
performed the experiments, analyzed data and wrote the paper. DHL,
DNL and JYK provided technical support and designed the tables. All
authors contributed to the article and all authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study received approval from the
Institutional Review Board of Chonnam National University Hwasun
Hospital (Jeonnam, Republic of Korea; approval no. CNUHH-2023-021).
Informed patient consent was waived due to this being a
retrospective study of case records.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chorath K and Rajasekaran K: Evaluation
and management of a neck mass. Med Clin North Am. 105:827–837.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ammar MI, Oeppen RS, Bowles C and Brennan
PA: Hard neck lumps: A review of uncommon and sometimes overlooked
causes of these worrying presentations. Br J Oral Maxillofac Surg.
55:899–903. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cabeçadas J, Martinez D, Andreasen S,
Mikkelsen LH, Molina-Urra R, Hall D, Strojan P, Hellquist H,
Bandello F, Rinaldo A, et al: Lymphomas of the head and neck
region: An update. Virchows Arch. 474:649–665. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Venkitakrishnan R, Paul M, Sleeba T,
Abraham L, Joshi M, Augustine J, Ramachandran D, Cleetus M and
Vijay A: Expecting the unexpected-primary mediastinal large B cell
lymphoma presenting as huge lung parenchymal mass. Respir Med Case
Rep. 32(101370)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yan S, Ma J, Yang M, Liu B, Li S, Yang L,
Zhang Q and Li X: Analysis of the clinicopathologic characteristics
and prognosis of head and neck lymphoma. Anal Cell Pathol (Amst).
2022(4936099)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Gao YH, Xu Q, Wei G, Liu HS, Wu X, Liu LH,
Wu LL, Zhao GM and Diao LP: Primary giant lymphoma of the right
thigh: A case report and brief review of the literature. Oncol
Lett. 4:1023–1026. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Payabvash S, Brackett A, Forghani R and
Malhotra A: Differentiation of lymphomatous, metastatic, and
non-malignant lymphadenopathy in the neck with quantitative
diffusion-weighted imaging: Systematic review and meta-analysis.
Neuroradiology. 61:897–910. 2019.PubMed/NCBI View Article : Google Scholar
|