Introduction
While a partial resection without lymph node
dissection may be used as a curative treatment for gastric
gastrointestinal stromal tumors (GISTs), laparoscopic surgery is a
less invasive option when performed by experienced laparoscopic
surgeons. In recent years, more and more studies have demonstrated
that laparoscopic surgery is safe and effective in the treatment of
gastric GISTs, irrespective of tumor size (1–7).
Meta-analyses have also demonstrated that laparoscopic surgery for
gastric GISTs is associated with a decreased blood loss volume,
earlier return of bowel function, earlier resumption of diet, a
shorter length of hospital stay and similar oncological results
when compared with open surgery (8–10).
However, laparoscopic resection for large gastric GISTs remains
under debate in terms of the high risk of intraoperative tumor
rupture. Guidelines from the European Society for Medical Oncology
(ESMO) discouraged the use of a laparoscopic approach in with large
tumors due to the risk of tumor rupture, which was associated with
a high risk of relapse (11). The
National Comprehensive Cancer Network (NCCN) guidelines considered
laparoscopic surgery only when the GISTs were in favorable
locations, such as the greater curvature or anterior wall of the
stomach (12). In 2012, 38 GIST
experts from the Chinese Society of Clinical Oncology discussed the
treatment of GIST in Beijing and released an expert consensus
(13). This consensus did not
recommend a laparoscopic approach when the tumor size was >5 cm.
Recently, retrospective studies from Asian countries demonstrated
that laparoscopic surgery is feasible, safe and oncologically
acceptable in the treatment of large gastric GISTs (14,15).
However, evidence from a prospective study was lacking. The current
study therefore presents the initial experience from a prospective
trial.
Patients and methods
Patients
Following approval by the Ethics Committee of Xuanwu
Hospital, Capital Medical University (Beijing, China), a
prospective study was performed in the Department of General
Surgery to evaluate the feasibility and safety of laparoscopic
surgery in the treatment of 16 patients with large (>5 cm)
primary gastric GISTs between March 2011 and March 2014. Written
informed consent was obtained from each patient. Patients receiving
any additional procedures at the time of the laparoscopic partial
gastric resection that were not conducive to the recovery of bowel
function, such as enterolysis, plus those with severe chronic
medical issues (American Society of Anesthesiologists class IV or
higher) (16) or any
contraindications to laparoscopic surgery were excluded from the
study. Continuous variables are presented as the mean ± standard
deviation, however, statistical analysis of the data was not
performed due to the small sample size.
Surgical procedure
Generally, a laparoscopic sleeve, wedge or distal
gastric resection without regional lymph node dissection was
applied to all the included patients. As described in previous
studies (17,18), the location and growth pattern of the
tumor, in addition to the tumor size, were the important factors in
determining resectability through minimally invasive techniques.
Exophytic masses located in the greater curvature, fundus and
anterior wall of the stomach were easily amenable to partial
resection, and one or two laparoscopic Endo-GIA™ (Medtronic, North
Haven, CT, USA) staplers were used to remove the tumor. Exophytic
tumors located in the posterior gastric wall were turned over
towards the abdominal cavity after cutting the blood vessel around
the greater curvature, then resected directly or by Endo-GIA
stapler. Intraluminal tumors were directly resected using Endo-GIA
staplers, with a wider extent of resection or an anterior
gastrotomy to access and resect the tumor. Masses near the pylorus
were removed by laparoscopic distal gastric resection.
Intraoperative endoscopy was used to aid in tumor localization and
avoid stricture of the cardia and pylorus. A closed suction drain
placed around the surgical site was not used routinely. The
specimen was retrieved in a plastic bag through a muscle-splitting
incision in the left or right flank.
Post-operatively, nasogastric tubes were used
routinely and removed at 12 h post-surgery. On the first
post-operative day, the patients were encouraged to walk around the
bed and drink water if there were no complaints associated with
postoperative complications. Patients were discharged once they
were able to tolerate a regular diet.
Primary and secondary outcomes
Intraoperative tumor rupture was studied as the
primary outcome. Secondary outcomes were the conversion rate,
surgical duration, estimated blood loss, time to tolerate fluid and
solid diets, length of post-operative hospital stay and recurrence
rate at the end of the follow-up.
Risk stratification following
resection of the primary tumor
Risk stratification following resection of the
primary GIST was performed according to the National Institutes of
Health (NIH) risk stratification system (19).
Follow-up
According to the recommendations of the NCCN,
patients who received a laparoscopic resection for GIST were
followed up every 6 months by enhanced abdominal and pelvic
computed tomography (CT) examinations for a 2-year period, then
yearly thereafter (12).
Results
Patients
A total of 16 patients with a tumor diameter of
>5 cm, underwent a laparoscopic resection for a gastric GIST in
the Department of General Surgery between March 2011 and March
2014. The characteristics of these patients are shown in Table I. The mean age of the patients was
63.1 years (range, 46–71 years), and 10 of the patients were male.
The most common signs or symptoms were anemia and gastrointestinal
bleeding. All patients received abdominal and pelvic CT evaluation
for primary and potential metastatic lesions. A total of 5 cases
obtained a pre-operative definitive diagnosis of a GIST through
endoscopic ultrasound-guided fine-needle biopsy, and 1 patient
received pre-operative imatinib mesylate (400 mg/day) treatment for
six months due to an excessive tumor size and multiple synchronous
liver metastases.
 | Table I.Characteristics of patients with large
gastric GIST tumors (>5 cm) who received laparoscopic
resection. |
Table I.
Characteristics of patients with large
gastric GIST tumors (>5 cm) who received laparoscopic
resection.
| Characteristic | Value |
|---|
| Mean age (range),
years | 63.1±4.2 (46–71) |
| Gender (male/female),
n | 10/6 |
| BMI | 24.5±2.1a |
| Presenting symptoms,
n (%) |
|
|
Anemia | 6 (37.5) |
|
Gastrointestinal bleeding | 4 (25.0) |
| Abdominal
pain | 3 (18.8) |
|
Incidental finding | 3 (18.8) |
| Preoperative GIST
diagnosis, n(%) | 5 (31.3) |
| Tumor size (range),
cm | 7.04±1.53
(5.2–10.8) |
| Tumor location, n
(%) |
|
| GEJ | 2 (12.5) |
|
Fundus | 3 (18.8) |
| Great
curve | 6 (37.5) |
| Body | 5 (31.3) |
| Growth pattern, n
(%) |
|
|
Exogenous | 12 (75.0) |
|
Intraluminal | 4 (25.0) |
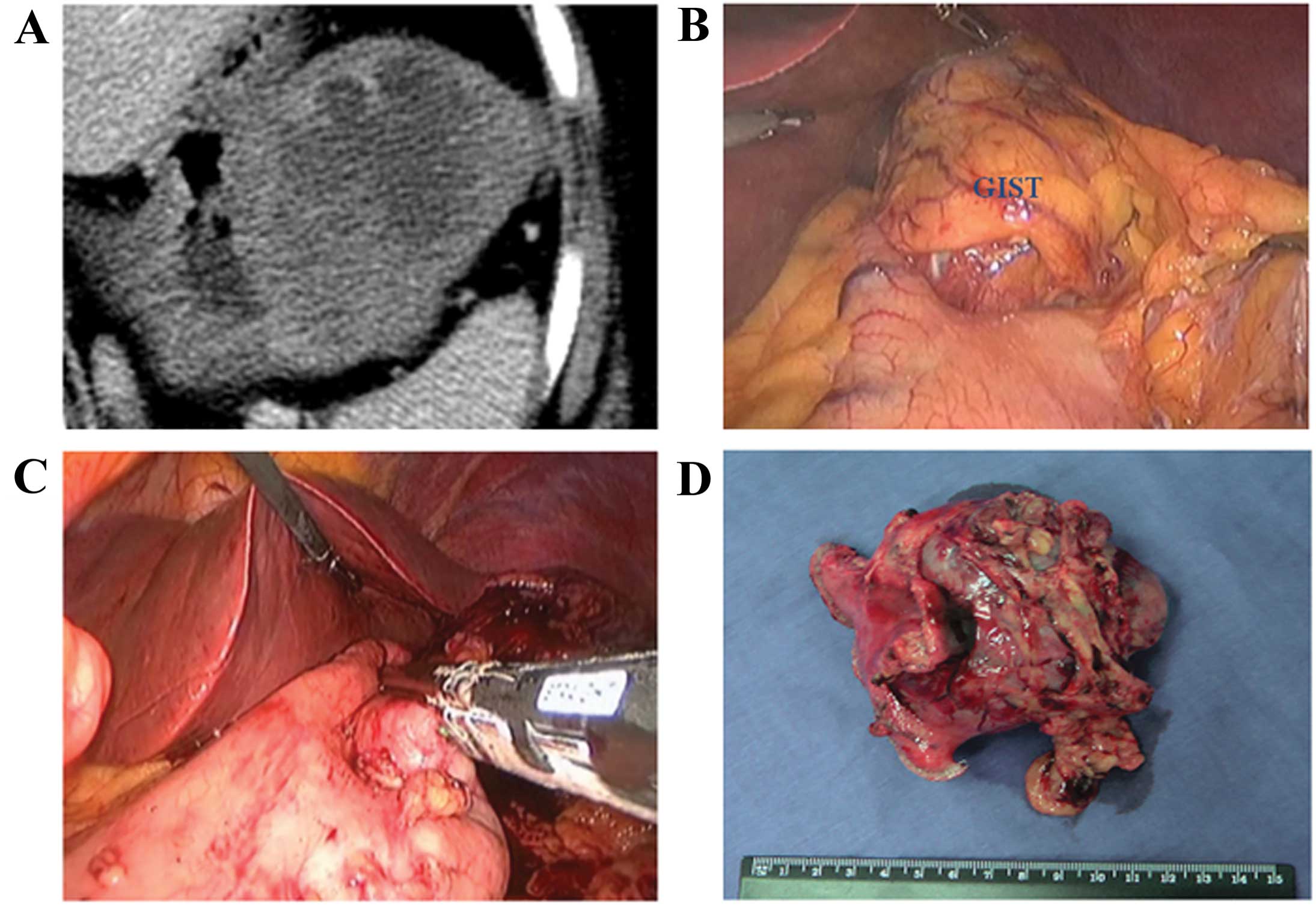
Surgical procedure
All patients successfully underwent a laparoscopic
gastric resection without conversion to an open procedure. In
total, 9 tumors located in the greater curvature, fundus or
anterior wall of the stomach with an exogenous growth pattern
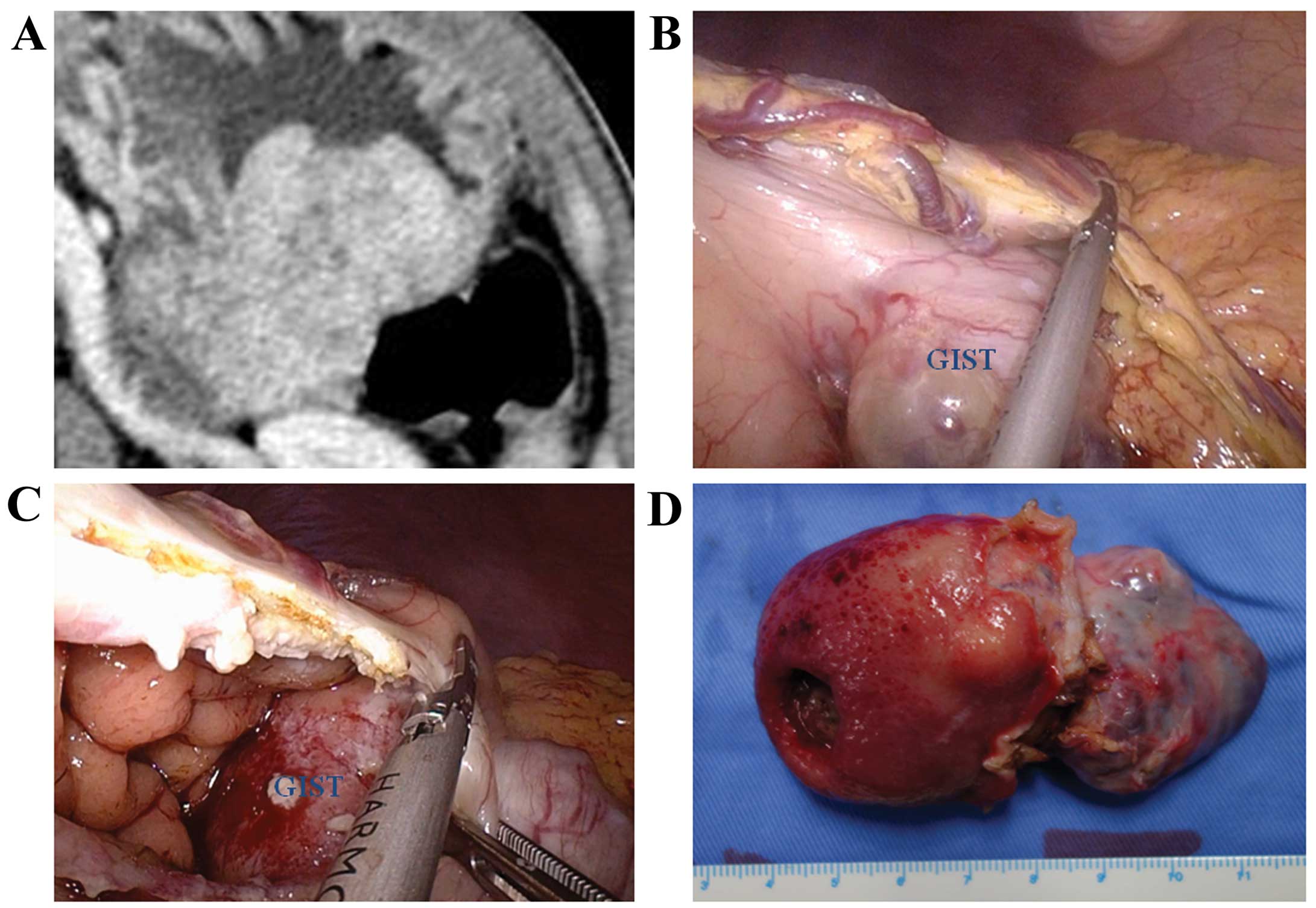
received laparoscopic sleeve or wedge resections (Fig. 1). Another 3 cases with exophytic
tumors located in the posterior wall of the stomach were turned
over toward the abdominal cavity and resected directly or by
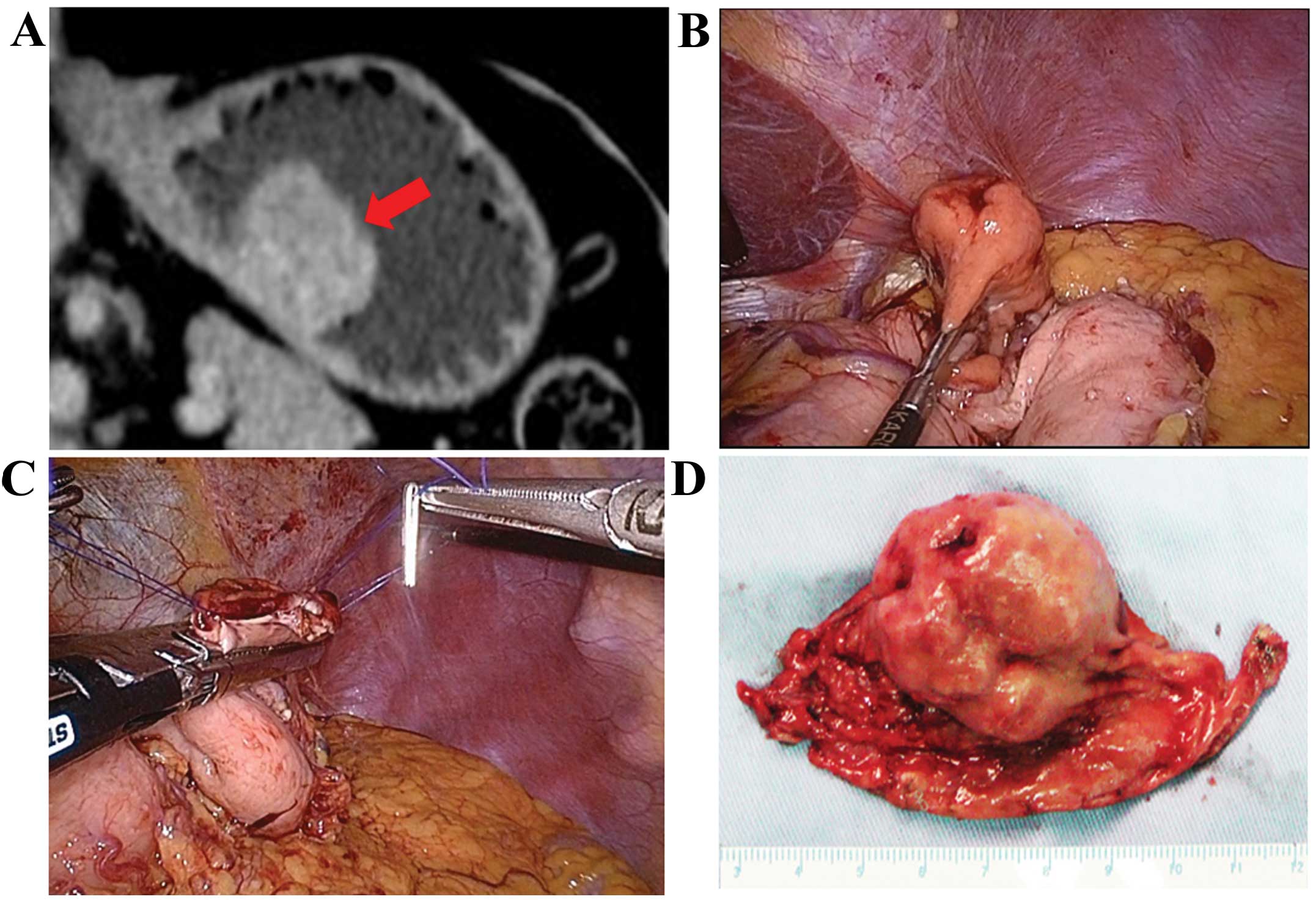
Endo-GIA (Fig. 2). Direct sleeve or
wedge resections with a wider extent were applied to 2 patients
with intraluminal tumors located in the anterior wall of the
stomach body, and two tumors that were located in the posterior
wall of the stomach with an intraluminal growth pattern were
resected though an anterior gastrotomy (Fig. 3). The characteristics of the different
surgical procedures are presented in Table II. When using the Endo-GIA resection
of the tumors, 3 patients underwent an intraoperative endoscopy to
avoid cardia stricture. A one-stage laparoscopic resection was
performed in 1 patient for the gastric GIST and synchronous liver
metastases. In total, 4 liver metastases were enucleated after 6
months pre-operative treatment. Incisional margin hemorrhage
occurred in 4 patients and subsequent hemostasis was performed with
clipping. Delayed gastric emptying occurred in 1 patient, which was
resolved at post-operative day 27. All tumors were retrieved in a
plastic bag though a muscle-splitting incision without rupture.
| Table II.Characteristics of different
laparoscopic approaches in treatment of large (>5 cm) gastric
gastrointestinal stromal tumors. |
Table II.
Characteristics of different
laparoscopic approaches in treatment of large (>5 cm) gastric
gastrointestinal stromal tumors.
| Group | Tumor size, cm | Growth pattern | Surgical duration,
min) | Estimated blood loss,
ml | Time to tolerate
solid diet, days | Length of
post-operative hospital stay, days | Follow-up time,
months |
|---|
| 1 (n=9) | 7.5±1.8 | Exogenous | 73.2±25.9 | 28.6±9.2 | 2.1±0.3 | 3.6±0.5 | 20.9±11.6 |
| 2 (n=3) | 6.4±1.4 | Exogenous | 110.7±12.6 | 65.3±9.5 | 2.7±0.6 | 4.0±0.4 | 11.7±12.7 |
| 3 (n=2) | 6.5±0.1 | Intraluminal | 69.6±0.7 | 17.5±10.6 | 2.0±0.0 | 15.0±16.9 | 18.0±4.2 |
| 4 (n=2) | 6.3±0.7 | Intraluminal | 140.0±2.8 | 52.5±3.5 | 4.5±0.7 | 6.0±0.0 | 6.0±2.8 |
Primary and secondary outcomes
With regard to the primary outcome, no
intraoperative tumor ruptures occurred. As for secondary outcomes,
the median duration of surgery was 88.1±31.9 min, with an estimated
blood loss volume of 37.1±18.7 ml. No patient required a blood
transfusion. The mean time until the start of oral intake for fluid
and solid diets was 1.1±0.6 and 2.5±0.9 days, respectively. The
median length of post-operative hospital stay was 5.4±5.8 days
(Table III).
| Table III.Operative and post-operative
characteristics. |
Table III.
Operative and post-operative
characteristics.
| Characteristic | Value |
|---|
| Intraoperative tumor
rupture, n (%) | 0 (0.0) |
| Conversion to open
surgery, n (%) | 0 (0.0) |
| Median surgical
duration (range), mina | 88.1±31.9
(45–142) |
| Estimated blood loss
(range), mla | 37.1±18.7
(10–75) |
| Mean time to tolerate
a fluid diet (range), daysa | 1.1±0.6
(0.5–3.0) |
| Mean time to
tolerate a solid diet (range), daysa | 2.5±0.9 (2–5) |
| Median length of
post-operative hospital stay (range), daysa | 5.4±5.8 (3–27) |
| Complications, n
(%) | 5 (31.3) |
| Anastamotic
bleeding, n (%) | 4 (25.0) |
| Delayed gastric
emptying, n (%) | 1 (6.3) |
Pathological finding and risk
stratification following resection of the primary tumor
The mean tumor size for all patients was 7.04±1.53
cm (range, 5.2–10.8 cm). Positively staining for cluster of
differentiation (CD)117, discovered on GIST-1, CD34 and S-100 was
found in 15 (93.8%), 13 (81.3%), 10 (62.5%) and 2 (12.5%) patients,
respectively. Since all gastric tumor sizes were >5 cm, risk
stratification was only dependent on mitotic rate. According to the
NIH risk stratification, 11 patients with tumors exhibiting a
mitotic rate of <5/50 high-power fields were classified as the
moderate-risk group. While the other 5 patients belonged to the
high-risk group. All patients were administered imatinib (400
mg/day) therapy post-operatively for at least 1 year (Table IV).
| Table IV.Pathological finding and risk
stratification. |
Table IV.
Pathological finding and risk
stratification.
| Parameter | n (%) |
|---|
| Cell type |
|
|
Spindle | 11 (68.8) |
|
Epithelioid | 2
(12.5) |
|
Mixed | 3
(18.8) |
| Mitotic rate, /50
HPF |
|
| ≤5 | 11 (68.8) |
|
5–10 | 4 (25.0) |
|
≥10 | 1 (6.3) |
| Positive for |
|
|
CD117 | 15 (93.8) |
|
DOG1 | 13 (81.3) |
|
CD34 | 10 (62.5) |
|
S-100 | 2 (12.5) |
| Ki-67 index, % |
|
|
<10 | 13 (81.3) |
|
≥10 | 3
(18.8) |
| Risk
stratification |
|
|
Moderate | 11 (68.8) |
|
High | 5
(31.3) |
Follow-up
The follow-up period for all patients ranged between
2 and 38 months (mean, 16.9±11.2 months). A total of 12 patients
received one or more enhanced CT scan. No local or distant
recurrence was observed in any of the patients and none of the
patients succumbed to the disease.
Discussion
The role of even single-port laparoscopic resection
for relatively small gastric GISTs has been established by a series
of retrospective cohort and comparative studies (1,2,6,7,17,20–24). In a
study by Sexton et al, 61 patients received laparoscopic
gastric resection for GISTs, with one conversion to an open
procedure in order to control bleeding originating from the spleen.
The mean tumor size was 3.8±1.8 cm and all but one case achieved an
R0 resection. The mean surgical duration was 151.9±67.3 min, and
the mean estimated blood loss volume was 97.4±200.7 ml (25). In a size-matched study (median size,
3.6 cm in laparoscopic group vs. 4.3 cm in open group), Karakousis
et al found that the median length of stay post-surgery in
the laparoscopic group was lower than that in the open group (4 vs.
7 days; P=0.002), as was estimated blood loss (25 vs. 100 ml;
P=0.006). Median surgical duration, operative mortality, and 30-day
morbidity and oncological outcomes were similar in the two groups
(24). A long-term survival study
also demonstrated favorable results for laparoscopic surgery, even
in patients with large GISTs (2,26,27).
As aforementioned, the current guidelines or
consensus from NCCN, ESMO and China discourage the use of
laparoscopic surgery for large gastric GISTs (11,12).
Guidelines from Japan also suggest that the laparoscopic resection
of gastric GISTs should be reserved for patients with a tumor size
of <5 cm and performed only by a skilled surgeon with complete
familiarity with the neoplastic characteristics of gastric GISTs
(28). The major concern with regard
to laparoscopic surgery in the treatment of large gastric GISTs is
the risk of tumor spillage or tumor capsule rupture, resulting in
peritoneal seeding and a worse prognosis. However, De Vogelaere
et al stated that the low morbidity rates and long-term
disease-free period of 100% observed in their study cohort
indicated laparoscopic resection to be a safe and effective method
for treating gastric GISTs, irrespective of tumor size (5). Ronellenfitsch et al also
demonstrated that the feasibility of laparoscopic wedge resection
was not determined by tumor size, and that the indication for a
laparoscopic wedge resection was not directly affected by the
location of the gastric GIST (29). A
size-matched study showed that laparoscopic resection for GISTs
>5 cm was superior to an open procedure in terms of surgical
duration, blood loss, time to ground activities, first flatus and
liquid diet, and post-operative stay (15). In the Xuanwe Hospital, Capital Medical
Hospital, laparoscopic surgery is the first choice of treatment for
gastric GISTs regardless of the tumor size or location. In the
present perspective study, laparoscopic resection for large gastric
GISTs was found to be feasible and safe, without a requirement for
conversion to open surgery. No intraoperative tumor rupture
occurred and the application of the concept of fast-track surgery
significantly accelerated patient recovery, with a post-operative
hospital stay of 5.4±5.8 days. To avoid combined organ resection
and major functional sequelae, guidelines recommend pre-operative
imatinib treatment of differing durations dependent on the mutation
type (11). In the present series, a
63-year-old female patient with a large, 15×10-cm, gastric GIST
located near the gastroesophageal junction and synchronous liver
metastases received a one-stage laparoscopic resection for the
primary and metastatic tumors after 6 months of pre-operative
therapy (30). This case was the
first to demonstrate the feasibility of one-stage surgery for a
giant gastric GIST and liver metastasis.
Although a laparoscopic approach for gastric GISTs
has been considered as the gold-standard surgical treatment in
recent series and reviews, laparoscopic resection for large gastric
GISTs, particularly those >5 cm, remains a challenging
technique. To avoid intraoperative tumor rupture, toothless forceps
should be used to grasp the normal stomach wall. Valle et al
demonstrated that large exophytic lesions can be protected from
lacerations of the capsule by covering them with an endobag prior
to starting the resection on disease-free tissue (5). A plastic bag should be used routinely
when removing tumors from the abdominal cavity.
There are several limitations to the present study.
Firstly, the characteristics of this cohort study meant that the
short-term results of an open approach could not be obtained for
comparison. Secondly, the limited number of cases and short
duration of follow-up may have restricted the value of the
conclusions. Thirdly, the tumors included in this study were mainly
located within the fundus and greater curvature of the stomach,
which were easy targets for laparoscopic surgery.
Irrespective of these limitations, the present
results also suggested that laparoscopic resection for large
gastric GISTs is feasible and safe. Laparoscopic surgery should be
considered as the standard approach in all cases, irrespective of
tumor size and location. Randomized controlled studies with
long-term follow-up periods should be performed to confirm these
results.
References
|
1
|
DeVogelaere K, Hoorens A, Haentjens P and
Delvaux G: Laparoscopic versus open resection of gastrointestinal
stromal tumors of the stomach. Surg Endosc. 27:1546–1554. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Honda M, Hiki N, Nunobe S, Ohashi M,
Kiyokawa T, Sano T and Yamaguchi T: Long-term and surgical outcomes
of laparoscopic surgery for gastric gastrointestinal stromal
tumors. Surg Endosc. 28:2317–2322. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tabrizian P, Sweeney RE, Uhr JH, Nguyen SQ
and Divino CM: Laparoscopic resection of gastric and small bowel
gastrointestinal stromal tumors: 10-Year experience at a single
center. J Am Coll Surg. 218:367–373. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Valle M, Federici O, Carboni F, Carpano S,
Benedetti M and Garofalo A: Gastrointestinal stromal tumors of the
stomach: The role of laparoscopic resection. Single-centre
experience of 38 cases. Surg Endosc. 28:1040–1047. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
DeVogelaere K, Van Loo I, Peters O,
Hoorens A, Haentjens P and Delvaux G: Laparoscopic resection of
gastric gastrointestinal stromal tumors (GIST) is safe and
effective, irrespective of tumor size. Surg Endosc. 26:2339–2345.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shu ZB, Sun LB, Li JP, Li YC and Ding DY:
Laparoscopic versus open resection of gastric gastrointestinal
stromal tumors. Chin J Cancer Res. 25:175–182. 2013.PubMed/NCBI
|
|
7
|
Kakeji Y, Nakanoko T, Yoshida R, Eto K,
Kumashiro R, Ikeda K, Egashira A, Saeki H, Oki E, Morita M, et al:
Laparoscopic resection for gastrointestinal stromal tumors in the
stomach. Surg Today. 42:554–558. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zheng L, Ding W, Zhou D, Lu L and Yao L:
Laparoscopic versus open resection for gastric gastrointestinal
stromal tumors: A meta-analysis. Am Surg. 80:48–56. 2014.PubMed/NCBI
|
|
9
|
Liang JW, Zheng ZC, Zhang JJ, Zhang T,
Zhao Y, Yang W and Liu YQ: Laparoscopic versus open gastric
resections for gastric gastrointestinal stromal tumors: A
meta-analysis. Surg Laparosc Endosc Percutan Tech. 23:378–387.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Koh YX, Chok AY, Zheng HL, Tan CS, Chow
PK, Wong WK and Goh BK: A systematic review and meta-analysis
comparing laparoscopic versus open gastric resections for
gastrointestinal stromal tumors of the stomach. Ann Surg Oncol.
20:3549–3560. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
The ESMO/European Sarcoma Network Working
Group, . Gastrointestinal stromal tumors: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol. 23
(Suppl 7):vii49–vii55. 2012.PubMed/NCBI
|
|
12
|
vonMehren M, Randall RL, Benjamin RS,
Boles S, Bui MM, Casper ES, Conrad EU III, Delaney TF, Ganjoo KN,
George S, Gonzalez RJ, et al: National Comprehensive Cancer
Network: Soft tissue sarcoma, version 2.2014. J Natl Compr Canc
Netw. 12:473–483. 2014.PubMed/NCBI
|
|
13
|
Chinese expert committee of
gastrointestinal stromal tumor, . Chinese expert consensus of GIST.
Zhonghua Wei Chang Wai Ke Za Zh. 15:301–307. 2012.
|
|
14
|
Takahashi T, Nakajima K, Miyazaki Y,
Kurokawa Y, Yamasaki M, Miyata H, Takiguchi S, Nishida T, Mori M
and Doki Y: Surgical strategy for the gastric gastrointestinal
stromal tumors (GISTs) larger than 5 cm: Laparoscopic surgery is
feasible, safe and oncologically acceptable. Surg Laparosc Endosc
Percutan Tech. 25:114–118. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lin J, Huang C, Zheng C, Li P, Xie J, Wang
J and Lu J: Laparoscopic versus open gastric resection for larger
than 5 cm primary gastric gastrointestinal stromal tumors (GIST): A
size-matched comparison. Surg Endosc. 28:2577–2583. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Owens WD, Felts JA and Spitznagel EL Jr:
ASA physical status classifications: A study of consistency of
ratings. Anesthesiology. 49:239–243. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pucci MJ, Berger AC, Lim PW, Chojnacki KA,
Rosato EL and Palazzo F: Laparoscopic approaches to gastric
gastrointestinal stromal tumors: An institutional review of 57
cases. Surg Endosc. 26:3509–3514. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Privette A, McCahill L, Borrazzo E, Single
RM and Zubarik R: Laparoscopic approaches to resection of suspected
gastric gastrointestinal stromal tumors based on tumor location.
Surg Endosc. 22:487–494. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Joensuu H: Risk stratification of patients
diagnosed with gastrointestinal stromal tumor. Hum Pathol.
39:1411–1419. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sasaki A, Nitta H, Otsuka K, Fujiwara H,
Takahara T and Wakabayashi G: Single-port versus multiport
laparoscopic resection for gastric gastrointestinal stromal tumors:
A case-matched comparison. Surg Today. 44:1282–1286. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Melstrom LG, Phillips JD, Bentrem DJ and
Wayne JD: Laparoscopic versus open resection of gastric
gastrointestinal stromal tumors. Am J Clin Oncol. 35:451–454. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chen YH, Liu KH, Yeh CN, Hsu JT, Liu YY,
Tsai CY, Chiu CT, Jan YY and Yeh TS: Laparoscopic resection of
gastrointestinal stromal tumors: Safe, efficient and comparable
oncologic outcomes. J Laparoendosc Adv Surg Tech A. 22:758–763.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ma JJ, Hu WG, Zang L, Yan XW, Lu AG, Wang
ML, Li JW, Feng B, Zhong J and Zheng MH: Laparoscopic gastric
resection approaches for gastrointestinal stromal tumors of
stomach. Surg Laparosc Endosc Percutan Tech. 21:101–105. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Karakousis GC, Singer S, Zheng J, Gonen M,
Coit D, DeMatteo RP and Strong VE: Laparoscopic versus open gastric
resections for primary gastrointestinal stromal tumors (GISTs): A
size-matched comparison. Ann Surg Oncol. 18:1599–1605. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sexton JA, Pierce RA, Halpin VJ, Eagon JC,
Hawkins WG, Linehan DC, Brunt LM, Frisella MM and Matthews BD:
Laparoscopic gastric resection for gastrointestinal stromal tumors.
Surg Endosc. 22:2583–2587. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Novitsky YW, Kercher KW, Sing RF and
Heniford BT: Long-term outcomes of laparoscopic resection of
gastric gastrointestinal stromal tumors. Ann Surg. 243:738–745.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Amin AT, Kono Y, Shiraishi N, Yasuda K,
Inomata M and Kitano S: Long-term outcomes of laparoscopic wedge
resection for gastrointestinal stromal tumors of the stomach of
less than 5 cm in diameter. Surg Laparosc Endosc Percutan Tech.
21:260–263. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nishida T, Hirota S, Yanagisawa A, Sugino
Y, Minami M, Yamamura Y, Otani Y, Shimada Y, Takahashi F and Kubota
T: GIST Guideline Subcommittee: Clinical practice guidelines for
gastrointestinal stromal tumor (GIST) in Japan: English version.
Int J Clin Oncol. 13:416–430. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ronellenfitsch U, Staiger W, Kähler G,
Ströbel P, Schwarzbach M and Hohenberger P: Perioperative and
oncological outcome of laparoscopic resection of gastrointestinal
stromal tumour (GIST) of the stomach. Diagn Ther Endosc.
2009:2861382009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cao F, Li J, Li A, Fang Y and Li F:
One-stage laparoscopic resection for a large gastric
gastrointestinal stromal tumor and synchronous liver metastases
following preoperative imatinib therapy: A case report. Oncol Lett.
5:1233–1236. 2013.PubMed/NCBI
|