Introduction
Chronic osteomyelitis (COM) is characterized by a
prolonged inflammatory process and is defined as an osseous
infection, with or without involvement of the surrounding soft
tissues. The etiology of COM is complex, often stemming from a
contiguous focus, hematogenous spread, or vascular insufficiency
(1). Despite significant
advancements in medical technology, the incidence of COM continues
to increase, even in developed countries (2). Despite various treatment strategies,
reported rates of reinfection have been as high as 20-30% (3).
The persistent infection and high incidence of
infection relapse notably increase the risk of malignant
transformation, particularly in patients presenting with sinus
tracts and skin ulcers. Hawkins first described such a malignant
transformation among patients with COM in 1835(4). However, due to its lower prevalence,
this disorder still requires comprehensive understanding. The lower
prevalence of this disorder underscores the importance of
addressing its adverse consequences. According to a previous
synthesis analysis, the overall incidences of local recurrence,
distal metastasis and tumor-related death in COM-related squamous
cell carcinoma (SCC) were over 10%, with all-cause death exceeding
30% (5). This highlights the
necessity for a reevaluation of the significance of this disease.
In the present study, a case report of SCC arising from COM of the
femur was presented.
Case report
A 65-year-old woman arrived to the Southern Medical
University Nanfang Hospital (Guangzhou, China) in November 2020,
with a chief complaint of recurring pain and pus discharge in her
left thigh for the past 50 years, following an open pierce injury
caused by an ox horn. She did not receive immediate or standard
therapy directly after the injury, leading to an infection. Over
the past 5 decades, the 65-year-old female patient sporadically
received antibiotics, resulting in fluctuating wound conditions. A
total of 5 years prior to her visit to the Southern Medical
University Nanfang Hospital (Guangzhou, China), the female patient
was diagnosed with femoral COM at the Maoming Dianbai Hospital
(Maoming, China) and underwent debridement. Unfortunately, the
infection recurred 6 months after the surgery, leading to worsening
local pain, increased pus discharge and development of wound
ulcers.
Upon initial examination, multiple sinus tracts were
observed near local tissue breakdown in the distal medial part of
the left thigh, with a cauliflower-like skin ulcer at the mouth of
the sinus tracts (Fig. 1A).
Additionally, X-rays (Fig. 1B and
C) and magnetic resonance imaging
(Fig. 1D) findings were consistent
with signs of COM. Due to suspicion of malignant transformation of
the skin ulcer, a biopsy was performed. The histopathological
outcomes revealed that some nests of mild to moderate heterotypic
squamous cells, microvascular hyperplasia, and moderate
inflammatory cells and eosinophils infiltrations were discovered in
the fibrous tissue, indicating well-differentiated SCC (Fig. 1E). Subsequently, the multiple
discipline treatment (MDT) team, comprising specialists from
oncology, imaging, infectious disease and pharmacy, recommended
limb amputation based on comprehensive assessment of the
65-year-old female patient's condition. However, the female patient
strongly insisted for a surgery with limb preservation.
Consequently, the female patient underwent radical debridement with
wide resection of the tumor, followed by placement of calcium
sulfate (CS) beads with vancomycin and gentamycin. Given the
potential risk of fracture post-resection, a rail fixator was also
implanted. Histological analysis confirmed the diagnosis of COM,
and intraoperative specimen culture indicated infection related to
Pseudomonas aeruginosa.
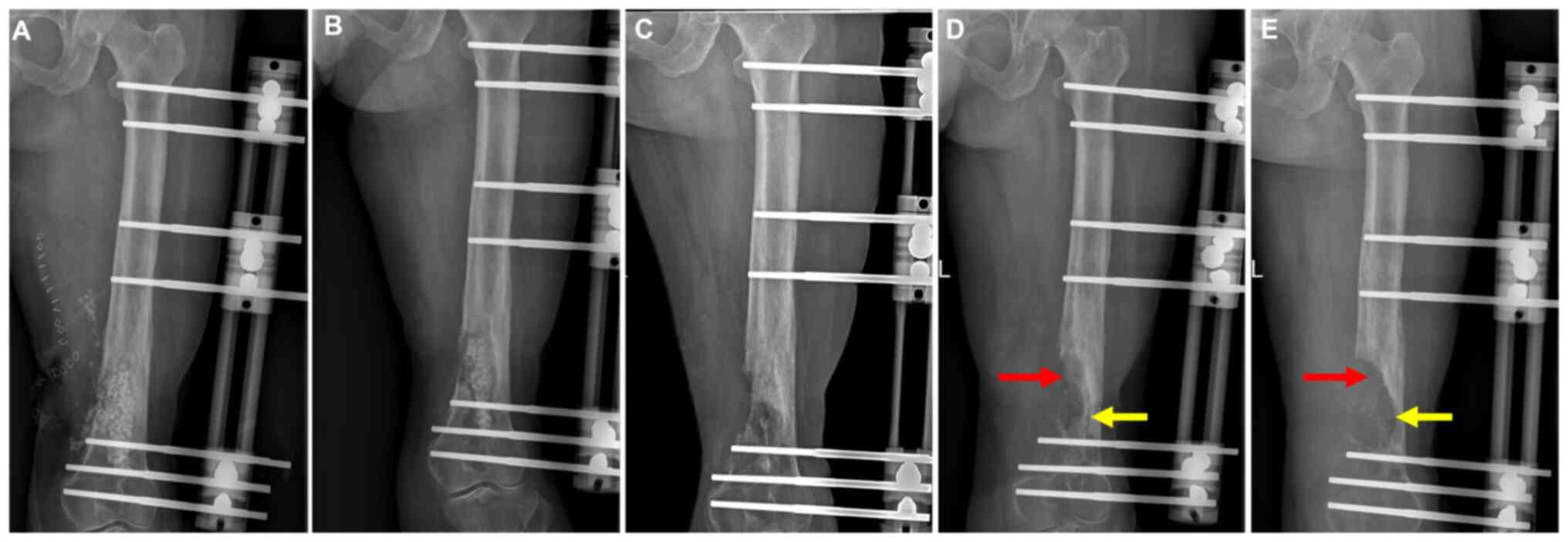
The post-operative radiograph revealed a rail
fixator with local implantation of vancomycin and gentamycin loaded
by CS beads in the distal femur (Fig.
2A). The wound exhibited satisfactory recovery before
discharge. The patient was scheduled for follow-up appointments at
intervals of 1, 2, 3, 6, 12, 18 and 24-months post-surgery.
However, the compliance of the patient was suboptimal.
A total of 1-month post-surgery, partial
biodegradation of the CS beads was observed on radiographs
(Fig. 2B). Completed biodegradation
of the beads accompanied by new bone formation occurred 4 months
post-surgery (Fig. 2C). However, a
subsequent X-ray image revealed an abnormal osteolysis signal at
the surgical site, despite normal skin appearance at the 7-month
follow-up (Fig. 2D, arrows).
Considering the potential recurrence of COM with or without SCC,
hospitalization was recommended to the female patient for further
tests, which the patient declined. A total of 10 months
post-surgery, the patient returned to the Southern Medical
University Nanfang Hospital (Guangzhou, China) with complaints of
recurrent pain accompanied by a draining sinus tract in the left
thigh. An X-ray revealed a more typical sign of osteolysis with
enlargement of the affected area (Fig.
2E, arrows). After counseling, the patient consented to undergo
surgery to prevent pathological fracture.
Following admission, the patient underwent
whole-body positron emission tomography/computed tomography
scanning, demonstrating a high possibility of SCC recurrence in the
left thigh, along with suspicious lesions indicating lymphatic
metastasis in the inguinal region (Fig.
3A and B) and a draining sinus
tract in the skin (Fig. 3C). Based
on these findings, the MDT team once again recommended amputation
due to the recurrence of SCC with a significant risk of metastasis,
to which the patient consented. During the surgery, the lesion was
identified as bean curd-like necrosis with a foul odor,
infiltrating the osseous tissue (Fig.
3D). Histological testing confirmed the presence of
well-differentiated SCC. Subsequently, the patient underwent
amputation of the middle thigh (Fig.
3E). Histological examination of the residual tissues revealed
no evidence of tumor cells (Fig.
3F). The patient recovered well after the surgery, and no signs
of recurrence were detected at the one-year follow-up
assessment.
Discussion
COM is a common infectious disorder that can arise
from contiguous focus, hematogenous spread and diabetic foot
ulcers. The incidence of this disorder was even increased in
developed countries, and one possible explanation is due to the
increase in diabetes-related OM among the individuals over 60 years
(2). However, the malignant
transformation of SCC arising from COM is rare, with reported
incidences ranging from 0.2-1.7% (6-8).
Although SCC arising from COM was first documented by Hawkins in
1835(4), the mechanisms underlying
such malignant transformation from inflammation to tumor formation
remain a topic of debate. One prevailing hypothesis suggests that
COM may possess carcinogenic properties, implying that the
long-term inflammation could facilitate malignant transformation,
tumor development, invasion and metastasis. Additionally, mediators
involved in COM pathogenesis may exert pleiotropic effects on tumor
development (9), while inflammatory
cytokines might influence the expression of tumor suppression genes
(10,11). Moreover, factors such as heredity,
exposure to toxins and immunologic factors (11-14)
may also contribute to the pathogenesis of COM-related SCC.
Therefore, a number of factors are considered to contribute to the
development of SCC secondary to COM.
SCC arising from COM shares several clinical
characteristics with COM, such as a higher incidence in males and
lower limbs, with trauma-induced infection being the most common
cause (15). However, SCC also
exhibits unique features. Notably, it often manifests after a
prolonged period, with reported average durations of 27 years
(5) or 31 years (16) before onset. Nevertheless, not all
cases of malignant transformation take such a lengthy period.
Khaladj et al (17) reported
a case of SCC arising from foot osteomyelitis with a duration as
short as three months. Additionally, SCC presents clinical signs
and symptoms similar to those of COM, including sinus tracts,
redness, pain and local swelling. Presently, specific indicators to
monitor this transformation are lacking. However, patients with COM
should remain vigilant for signs such as foul odor, exophytic or
fungating masses, protracted wounds, aggravating pain and increased
drainage, as these may indicate SCC development (5). Similarly, Corrigan et al
(16) analyzed 106
literature-reported cases and suggested that SCC should be
suspected in all patients with COM with skin changes, particularly
those with sinus drainage persisting for more than three years. It
should be noted that extended disease durations and aggravating
clinical symptoms serve as clues for SCC development; however,
definitive diagnosis relies on histological tests. In the present
case report, the female patient had a notable prolonged history of
COM with sinus tracts and skin ulcers, coupled with inadequate
standard treatment, which increased the female patient's risk of
SCC development.
Based on previous systematic reviews, limb
amputation remains the primary treatment modality for COM-related
SCC (5,16), with both studies indicating that
>80% of patients with this condition undergo amputation. While
amputation is a radical approach, it serves as a comprehensive
strategy to eliminate both infection and tumor burden (18), leading to a faster and safer
recovery, particularly in advanced or complex cases (19). In addition to amputation, wide tumor
resection may be considered for patients without evidence of distal
metastasis (18). Mohs micrographic
surgery, characterized by serial sections to achieve absolute tumor
resection, has been applied in COM-related SCC cases with
satisfactory outcomes. However, due to the limited sample size of
this patient group, future studies with large cohorts are warranted
to more accurately evaluate the efficacy of Mohs micrographic
surgery. Conservative therapy is generally not recommended as a
routine management for SCC due to its malignant nature. However, it
may be considered in patients with absolute contraindications to
surgery (5). Currently,
chemotherapy and radiotherapy are primarily employed in patients
with local recurrence and distal metastasis. Nevertheless, the
limited number of studies in this area results in a scarcity of
robust evidence regarding their efficacy.
Although amputation is the primary treatment for SCC
arising from COM, its clinical efficacy remains suboptimal, with
local recurrence, distal metastasis and tumor-related death rates
exceeding 10% (5), demonstrating a
less-than-ideal prognosis. In the present reported case study,
despite recommendations from the MDT specialists for limb
amputation, the patient initially declined due to a strong
preference for limb preservation. Consequently, radical debridement
with wide tumor resection was performed. Unfortunately, the tumor
recurred shortly after surgery, ultimately leading to limb
amputation. The specific risk factors contributing to local
recurrence and distal metastasis remain unclear. However, according
to a synthesis analysis of 176 reported cases by Jiang et al
(5), patients with regional
lymphadenopathy at diagnosis and those with moderately to poorly
differentiated types of SCC may be at a higher risk of local
recurrence. In the present reported case, the female patient
experienced a satisfactory recovery one year after undergoing
amputation surgery.
In addition to the present case, numerous previous
studies also reported clinical characteristics and treatment
efficacy of patients with SCC arising from COM. In a retrospective
study of eight cases, Li et al (20) indicated that the mean duration from
COM to SCC occurrence was 28 years, with the tibia as the most
frequent affected site. Furthermore, amputation was performed in
seven cases, with no recurrence and metastasis during the follow-up
time. Quite similar to the present case study, Luchs et al
(21) also reported a patient with
a 50-year history of femoral COM, and they used an en bloc
tumor resection combined a Van Ness rotational repair. However,
they did not track the treatment efficacy. In a recent systematic
review, Bryce-Alberti et al (22) summarized the treatment approach and
oncological outcomes of SCC arising from extremity COM. It was also
discovered that such a disorder mostly occurred following trauma,
with the tibia, foot and femur as the top sites. Meanwhile, it was
indicated that bone invasion was common (83%), and most patients
received limb amputation (90%), which appeared to be related to a
higher survival rate compared with limb salvage strategies. These
findings were supported by the present case report. In the present
study, a wide resection of the tumor together with local
antibiotics and a rail fixator as the primary limb salvage strategy
was initially utilized, but unfortunately due to its
well-differentiated type it resulted to a failure. The present case
study once again suggested that limb preservation surgery should be
conducted cautiously for patients with COM-related SCC.
There are several limitations to the present study.
First, it was presented as a single case report, leading to a
limited level of evidence. Second, the patient was only followed-up
for 1 year after the final amputation surgery, which may be
insufficient to fully evaluate the efficacy and prognosis of SCC.
Third, while limb amputation remains the primary treatment for SCC,
the attempt at limb salvage using wide tumor resection was
unsuccessful. The potential effectiveness of alternative limb
preservation strategies, such as Mohs micrographic surgery or
segmental infected bone and soft tissue resection, remains unclear
in these patients. Nonetheless, the present case study offers
valuable insights into COM-associated SCC, which may enhance
understanding of this disorder. In conclusion, while SCC arising
from COM is rare, it is crucial for patients with COM, particularly
those with prolonged disease duration, to remain vigilant for signs
of potential malignant transformation, including aggravating
symptoms, foul odor, exophytic or fungating masses, protracted
wounds, worsening pain and increasing drainage. Once the diagnosis
of SCC has been established, caution must be exercised when
considering limb preservation strategies, as the risks of local
recurrence and distal metastasis are high. Currently, limb
amputation remains the primary treatment strategy for SCC arising
from COM. It is important to note that modern prosthetics do not
notably impact the patient's quality of life. Nonetheless, ongoing
research may lead to the development of novel limb preservation
strategies in the future.
Acknowledgements
The authors would like to thank Professor Ya-ping Ye
from Department of Pathology, Nanfang Hospital, Southern Medical
University (Guangzhou, China), for his help in editing the
histopathological test figures and description of the
histopathological findings.
Funding
Funding: The present study was supported by the Clinical
Research Project of Nanfang Hospital, Southern Medical University
(grant no. 2023CR010).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YJH and BY conceptualized the present study and
confirm the authenticity of all the raw data. NJ, YSY and QRL
conducted the investigation. NJ and YSY curated the data. YSY wrote
and prepared the original draft. NJ, YJH and BY wrote, reviewed and
edited the manuscript. YJH and BY supervised the project. BY was
the project administrator. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written, retrospective informed
consent for publication following detailed explanation of the
purpose of the manuscript and understanding that no identifiable
information was going to be released.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lew DP and Waldvogel FA: Osteomyelitis.
Lancet. 364:369–379. 2004.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kremers HM, Nwojo ME, Ransom JE,
Wood-Wentz CM, Melton LJ III and Huddleston PM III: Trends in the
epidemiology of osteomyelitis: A population-based study, 1969 to
2009. J Bone Joint Surg Am. 97:837–845. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lazzarini L, Mader JT and Calhoun JH:
Osteomyelitis in long bones. J Bone Joint Surg Am. 86:2305–2318.
2004.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Hawkins C: Cases of Warty tumours in
cicatrices. Med Chir Trans. 19:19–34. 1835.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jiang N, Li SY, Zhang P and Yu B: Clinical
characteristics, treatment, and prognosis of squamous cell
carcinoma arising from extremity chronic osteomyelitis: A synthesis
analysis of one hundred and seventy six reported cases. Int Orthop.
44:2457–2471. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Altay M, Arikan M, Yildiz Y and Saglik Y:
Squamous cell carcinoma arising in chronic osteomyelitis in foot
and ankle. Foot Ankle Int. 25:805–809. 2004.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Patel NM, Weiner SD and Senior M: Squamous
cell carcinoma arising from chronic osteomyelitis of the patella.
Orthopedics. 25:334–336. 2002.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wagner RF Jr and Grande DJ:
Pseudoepitheliomatous hyperplasia vs. squamous cell carcinoma
arising from chronic osteomyelitis of the humerus. J Dermatol Surg
Oncol. 12:632–635. 1986.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Multhoff G, Molls M and Radons J: Chronic
inflammation in cancer development. Front Immunol.
2(98)2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Sell S: Infection, stem cells and cancer
signals. Curr Pharm Biotechnol. 12:182–188. 2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Trent JT and Kirsner RS: Wounds and
malignancy. Adv Skin Wound Care. 16:31–34. 2003.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chalya PL, Mabula JB, Rambau P, Mchembe
MD, Kahima KJ, Chandika AB, Giiti G, Masalu N, Ssentongo R and
Gilyoma JM: Marjolin's ulcers at a university teaching hospital in
Northwestern Tanzania: A retrospective review of 56 cases. World J
Surg Oncol. 10(38)2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Fairbairn NG and Hamilton SA: Management
of Marjolin's ulcer in a chronic pressure sore secondary to
paraplegia: A radical surgical solution. Int Wound J. 8:533–536.
2011.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kerr-Valentic MA, Samimi K, Rohlen BH,
Agarwal JP and Rockwell WB: Marjolin's ulcer: Modern analysis of an
ancient problem. Plast Reconstr Surg. 123:184–191. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Jiang N, Ma YF, Jiang Y, Zhao XQ, Xie GP,
Hu YJ, Qin CH and Yu B: Clinical characteristics and treatment of
extremity chronic osteomyelitis in Southern China: A retrospective
analysis of 394 consecutive patients. Medicine (Baltimore).
94(e1874)2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Corrigan RA, Barlow G, Hartley C and
McNally M: Squamous cell carcinoma complicating chronic
osteomyelitis: A systematic review and case series. Surgeon.
20:e322–e337. 2022.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Khaladj M, Mbibong RM, Shah N, Mohiuddin A
and Siddiqui A: Invasive squamous cell carcinoma with osteomyelitis
of the foot a case report. J Am Podiatr Med Assoc. 105:374–376.
2015.PubMed/NCBI View
Article : Google Scholar
|
|
18
|
Panteli M, Puttaswamaiah R, Lowenberg DW
and Giannoudis PV: Malignant transformation in chronic
osteomyelitis: Recognition and principles of management. J Am Acad
Orthop Surg. 22:586–594. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Alami M, Mahfoud M, El Bardouni A, Berrada
MS and El Yaacoubi M: Squamous cell carcinoma arising from chronic
osteomyelitis. Acta Orthop Traumatol Turc. 45:144–148.
2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Li Q, Cui H, Dong J, He Y, Zhou D, Zhang P
and Liu P: Squamous cell carcinoma resulting from chronic
osteomyelitis: A retrospective study of 8 cases. Int J Clin Exp
Pathol. 8:10178–10184. 2015.PubMed/NCBI
|
|
21
|
Luchs JS, Hines J, Katz DS and Athanasian
EA: MR imaging of squamous cell carcinoma complicating chronic
osteomyelitis of the femur. AJR Am J Roentgenol. 178:512–513.
2002.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Bryce-Alberti M, Gonzalez MR,
Quevedo-Ramirez A and Pretell-Mazzini J: Squamous cell carcinoma
arising from chronic osteomyelitis in the extremities: Treatment
approach and oncological outcomes-a systematic review of the
literature. J Skin Cancer. 2022(2671420)2022.PubMed/NCBI View Article : Google Scholar
|