Introduction
Cervical cancer is the most common carcinoma of the
genital tract in women, with an age-standardized incidence of 8.9
cases per 100,000 women/year (1),
and an estimated 150,000 new cases per year in China (2), particularly in young women.
The diagnosis of cervical cancer now relies on
specialized clinical examinations, computed tomography (CT),
magnetic resonance imaging (MRI) and ultrasound. Compared with CT,
which has a low contrast resolution of soft tissue, MRI is the
ideal modality for visualization of the cervix (3). However, it is not usually possible to
perform MRI immediately due to inconvenience and the limitations of
contraceptive devices. By contrast, ultrasound is gaining clinical
interest since it is less time consuming, cheaper, noninvasive and
safe, particularly for patients undergoing repeated
examination.
Acoustic radiation force impulse (ARFI) ultrasound
imaging, as a new technique of elastography, works on the principle
that different tissues have different coefficients of elasticity
and therefore are under different levels of strain. Color coding
and relative shear wave velocity (SWV) have been demonstrated with
ARFI ultrasound imaging. According to the elasticity of
pathological tissues, it is possible to conclude qualitatively and
quantitatively the benign or malignant pathological tissue
(4–8). However, ARFI ultrasound imaging uses
a short-duration acoustic push pulse technique and is a non-manual
technique, other elastic techniques require manual vibration.
(9–11).
ARFI, a new technique of ultrasonic elastography, as
a recent development of imaging technology, is able to obtain
qualitative and quantitative information of the elasticity
distribution within tissues and has the advantages of being
noninvasive, painless and convenient. Hence, it has significant
clinical value and wide application prospects. Currently ARFI
ultrasound imaging is used for evaluation of tissue elasticity in
the liver, pancreas, breast, thyroid and prostate (12–19).
However, there are few reports concerning its use in cervical
cancer (20). It is reported that
ARFI has been used in transvaginal ultrasound imaging (21). However, although transvaginal
ultrasound has numerous advantages, it is not applied to women that
have not had sexual intercourse, it may cause bleeding and
infection and a number of women will not accept this examination
method (22). Transvaginal
ultrasound does not reveal the field in which cervical cancer
occurs, including metastases to the pelvic cavity, the larger lymph
nodes and violation of bladder and rectum. Therefore we suggest the
use of transabdominal ultrasound with ARFI ultrasound imaging for
the evaluation of cervical cancer. ARFI ultrasound imaging may be
applied to all women, is safe, painless, convenient and likely to
be accepted by patients. In addition, it is possible to identify
more information about cervical cancer and the surrounding tissues,
particularly distant metastases. This is important for the
physician when determining the area of infiltration and planning
treatment. The current study was designed to investigate the
clinical value of ARFI ultrasound imaging in the prediction of
cervical malignancies by detecting changes in tissue stiffness.
Materials and methods
General information
Fifty-eight consecutive patients were selected from
the Department of Obstetrics and Gynecology of the Shanghai First
People’s Hospital, School of Medicine, Shanghai Jiaotong University
between March 2012 and October 2012. The inclusion criterion was
the presence of lesions in the uterine cervix with definite
pathological results. The exclusion criteria were a lesion diameter
of <5 mm and a depth between the lesion and skin of >80 mm.
To avoid infection and vaginal bleeding, and to enable the
examination of women that have not had sexual intercourse, we used
a transabdominal rather than transvaginal sonographic probe. A
total of 58 women were enrolled (mean age 53.6±18.9 years, range
22–78 years) in the study. This study was conducted in accordance
with the Declaration of Helsinki and with approval from the Ethics
Committee of Shanghai Jiaotong University (Shanghai, China).
Written informed consent was obtained from all participants.
Acquisition of the ARFI data
Real-time ARFI ultrasound imaging was performed
using an Acuson S2000 diagnostic ultrasound system (Siemens
Healthcare, Erlangen, Germany) equipped with a 3.5 MHz abdominal
probe. All examinations were performed in succession by two
independent sonographers. The sonographers had >10 years
experience in ultrasonic scanning. They were blinded to the
colposcopy findings and physical examination results when
performing the examinations.
The patients were asked to lie in a supine position
with a half-full bladder. Conventional sonography was used to
observe the shape, size, boundary and echoes of each lesion. Color
Doppler was used to access the blood supply of the lesions. The
highest sensitivity for detection of color Doppler signals was
used, allowing for the detection of blood flow velocities ≥2
cm/sec. Using the ARFI elasticity model, elastography imaging (EI),
Virtual Touch tissue imaging (VTI) and Virtual Touch tissue
quantification (VTQ) were used to measure the elasticity of the
lesions and surrounding tissues in turn.
eSie Touch EI
The eSie Touch EI method generates grayscale and
color scale elastograms. On the grayscale image, with increasing
stiffness of the tissue, the images gradually change from white to
black. White depicts the softest tissue and black, the hardest
tissue. On the color scale, with increasing stiffness of the
tissue, the image gradually changes from red to blue. Red
represents the softest tissue and blue the hardest tissue (23).
According to Thomas et al(24), analysis of hardness classification
of EI was as follows: 1st grade: definitely normal: 2/3 area was
green, 1/3 was red, blue was negligible; 2nd grade: approximately
normal, 2/3 area was green, 1/3 area was red and blue; 3rd grade:
between normal and abnormal, 2/3 area was green, 1/3 area was red
and blue; 4th grade: abnormal, blue area in the cervix was more
extensive than red area, and blue area may extend beyond the
cervix; 5th grade: definitely abnormal, blue area more extensive
than red area, blue area markedly extends beyond the cervix.
Virtual Touch tissue imaging
In the VTI model, the region of interest (ROI)
should encircle the lesion. To obtain appropriate images, the probe
was applied with light pressure to make complete contact with the
abdomen. The VTI button was then pressed, a short (∼100
μsec) acoustic push pulse was transmitted through tissue,
and a black-and-white VTI image was obtained. A very stiff tissue
may displace little or not at all. On the VTI elastic image, the
softness or hardness of lesions and peripheral cervical tissue may
be observed (25).
On the basis of the VTI classification method of
Shuang-Ming et al(26) and
research on thyroid nodule imaging, the images were divided into 4
types: ‘softer’, with the nodule whiter than the surrounding
thyroid tissue; ‘equal stiffness’, with similar image colors of the
nodule and the peripheral thyroid tissue; ‘stiffer’, with the
nodule appearing blacker (>50%) than the surrounding thyroid
tissue; and ‘cellular sample’, with the nodule showing an
alternating black and white honeycomb-like distribution.
Virtual Touch tissue quantification
In the VTQ model, the ROI (6×10 mm) was placed
inside the lesion and the depth of the ROI was <80 mm. For more
accurate and objectively derived elastic parameters, the ROI was
placed inside lesions whose smallest diameters were >5 mm; it
was continuously measured three times randomly, and the average
value was calculated as the VTQ value (m/sec). The measurements of
the surrounding tissues were performed with the ROI placed at the
same level as the lesion and within 5–10 mm from the lesion,
avoiding vascular structures; three consecutive elastic parameters
were obtained and the average value was calculated as the VTQ value
of the surrounding tissues.
Statistical analysis
All statistical analysis used SPSS version 17.0
software (SPSS Inc, Chicago, IL, USA). All measured data were
presented as the mean ± standard deviation. The EI and VTI image
analysis used the non-parametric Mann-Whitney U test. Groups of
lesions and peripheral normal tissue were compared using the
Student U test. The χ2 test was used to calculate the
sensitivity, specificity, positive predictive value, negative
predictive value and diagnostic accordance rate.
Results
Lesion properties
From the 58 malignant lesions, 47 (81.03%) were
squamous and 11 (18.97%) were adenocarcinoma. The lesion sizes
ranged from 10×10 mm to 24×33 mm, with an average of 18.6×15.4
mm.
Conventional sonography
The 58 malignant lesions all appeared solid on
B-mode sonography, and all were hypoechoic. According to their
morphologic characteristics, boundary, echoes on gray scale
sonography and color Doppler flow imaging, the sensitivity,
specificity and diagnostic accuracy were 78.95, 77.97 and 78.45%,
respectively (Table I).
 | Table IDiagnosis of cervical cancer and
surrounding normal tissue by conventional sonography. |
Table I
Diagnosis of cervical cancer and
surrounding normal tissue by conventional sonography.
| Sonographic diagnosis
| |
|---|
| Parameter | Suspected
malignant | Suspected normal
tissue | Total |
|---|
| Malignant | 51 | 13 | 58 |
| Normal tissue | 12 | 49 | 58 |
| Sensitivity, % | | | 78.95 |
| Specificity, % | | | 77.97 |
| Accuracy, % | | | 78.45 |
eSie Touch elastography imaging
analysis
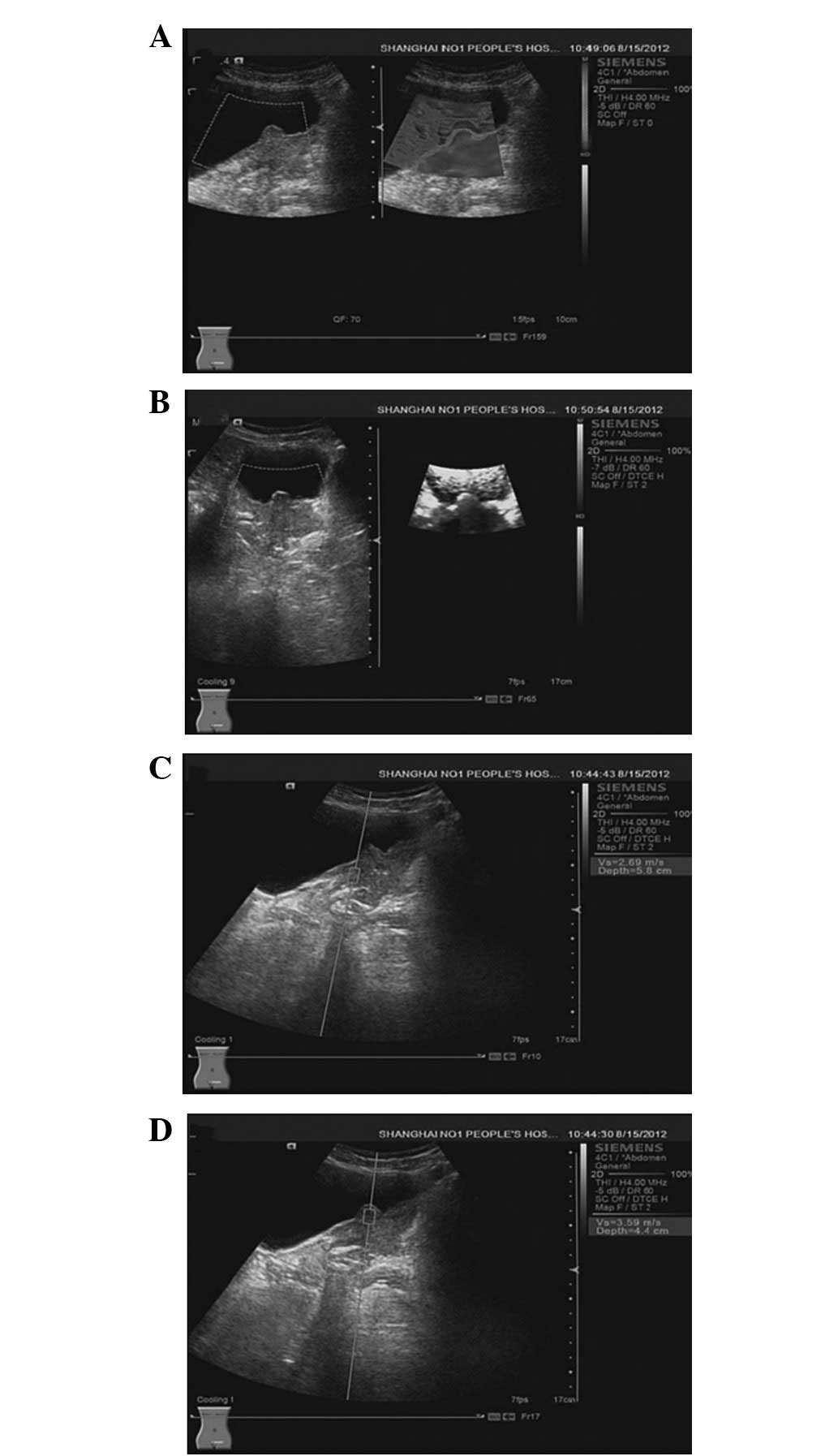
Compared with the surrounding cervical tissue,
72.41% (42 of 58) of the malignant lesions showed 4th or 5th grade
images and 27.59% (16 of 58) had 3rd grade images (Table II; Fig. 1A). The EI images showed a
significant difference between the malignant lesions and
surrounding normal tissues (P<0.001).
| Table IIElastography imaging analysis of
malignant and normal tissues. |
Table II
Elastography imaging analysis of
malignant and normal tissues.
| Lesion type
| |
|---|
| Grade | Malignant (n=58) | Normal tissue
(n=58) | Total |
|---|
| 1 | 0 | 28 | 28 |
| 2 | 0 | 20 | 20 |
| 3 | 3 | 7 | 10 |
| 4 | 19 | 3 | 22 |
| 5 | 36 | 0 | 36 |
Virtual Touch tissue imaging
analysis
Compared with the surrounding cervical tissue,
84.48% (49 of 58) of the malignant lesions showed stiffer images
and 15.52% (9 of 58) had black and white honeycomb-like images
(Table III; Fig. 1B). The VTI images showed a
significant difference between malignant lesions and normal
cervical tissues (P<0.001).
| Table IIIVirtual Touch tissue imaging analysis
of malignant and normal tissues. |
Table III
Virtual Touch tissue imaging analysis
of malignant and normal tissues.
| Lesion type
| |
|---|
| Characteristic | Malignant (n=58) | Normal tissue
(n=58) | Total |
|---|
| Softer | 4 | 25 | 29 |
| Equal | 18 | 21 | 39 |
| Stiffer | 32 | 4 | 36 |
| Honeycomb | 4 | 8 | 12 |
Virtual Touch tissue quantification
analysis
All the lesions were assessed at least three times
by two independent observers based on various static images and the
average value was recorded as the final result. The observers were
blinded to the physical and pathological results. The assessments
of the two observers had high consistency (κ=0.71).
Surrounding normal tissues had lower VTQ values
(Table IV; Fig. 1C), with a mean of 2.11±1.19 m/sec,
while the VTQ values in malignant lesions were higher than the
surrounding normal tissues (3.41±1.59 m/sec, P<0.001; Fig. 1D).
| Table IVVirtual Touch tissue quantification
(VTQ) imaging analysis of malignant and normal tissues. |
Table IV
Virtual Touch tissue quantification
(VTQ) imaging analysis of malignant and normal tissues.
| Tissue type | n | VTQ value, m/s | P-value |
|---|
| Malignant | 58 | 3.41±1.59 | <0.001 |
| Normal tissue | 58 | 2.11±1.19 | |
Discussion
Sonoelastography remains a primary method for the
diagnosis of cervical cancer. Compared with cervical biopsy, which
is the gold standard, women are more likely to accept noninvasive
examination. A previous study has shown that there is a statistical
difference of elasticity between malignant and normal cervical
tissue. The stiffer the object, the larger the elastic modulus.
Malignant tissues are stiffer than benign tissues. Therefore the
elastic modulus of the former is greater than that of the latter.
Cervical tissues mainly comprise collagen fiber and a few muscle
fibers. Although cervical tissues may undergo changes to elasticity
under different physiological conditions, for example, the
elasticity may be affected by pregnancy or the menstrual cycle, the
normal elasticity of cervical tissues does not change with age
(24).
ARFI ultrasound imaging is a convenient examination
method. We used eSie Touch EI utilizing ARFI ultrasound technology
to qualitatively diagnose cervical cancer. eSie Touch imaging forms
the elastogram by computing relative tissue deformation globally
and displaying the information within a user-defined ROI. This
method uses grayscale and color coding to show the relative
stiffness of the tissues. The more black or blue a tissue appears,
the stiffer the tissue is. Our study showed that the malignant
tissues were stiffer than the surrounding tissues using EI.
In the current study, VTI utilizing ARFI ultrasound
technology was used to qualitatively diagnose cervical cancer. A
Virtual Touch software image is a qualitative grayscale map of
relative tissue stiffness (elastogram) for a user-defined ROI. This
method uses a grayscale to demonstrate the relative stiffness of
the tissues. The blacker a tissue appears, the stiffer the tissue
is. Our study showed that the malignant tissues were stiffer than
the surrounding tissues using VTI.
VTQ utilizing ARFI ultrasound technology was used to
quantitatively diagnose cervical cancer. In VTQ, an acoustic push
pulse is applied to the ROI to induce a shear-wave. The time
between the generation of the shear-wave and detection of the peak
is utilized to compute the SWV. Multiple measurements were taken
throughout the chosen location and the mean was calculated. This
numerical value was correlated with the stiffness of tissue within
the ROI. We used ARFI ultrasound imaging to obtain the SWV between
the malignant and normal tissues. The stiffer a tissue, the greater
its SWV (27,28). The present study showed that the
malignant tissue was stiffer than the surrounding tissues using
VTQ.
In the current study, a transabdominal scan probe
was used to avoid infection and vaginal bleeding, particularly in
women that have not had sexual intercourse. This method is able to
scan the tissues surrounding the cervix, and examine the lymph
nodes and violation of the bladder and rectum. It was important in
determining the stage of cervical cancer and is the subject of our
next study. However, the transabdominal probe has certain
limitations, such as when examining deeper tissues or when used on
patients with high adiposity.
In conclusion, ARFI ultrasound imaging is a superior
method for the examination of cervical cancer. ARFI ultra-sound
imaging of the uterine cervix may be an objective method for the
assessment of soft tissue. ARFI ultrasound imaging has a high
sensitivity and specificity in the evaluation of cervical cancer
and therefore has a good diagnostic value in clinical
applications.
Acknowledgements
This study was supported by the
Departments of Ultrasound, Obstetrics and Gynecology and Pathology
of Shanghai First People’s Hospital (Shanghai, China). This work
was also supported by grant 10411951800 from the Scientific
Research Project of the Shanghai Science and Technology Commission
and grant SHDC 12010221 from the Joint Development and Application
Project of Appropriate Technology of Shanghai Municipal
Hospital.
References
|
1.
|
Testa AC, Ludovisi M, Manfredi R, et al:
Transvaginal ultra-sonography and magnetic resonance imaging for
assessment of presence, size and extent of invasive cervical
cancer. Ultrasound Obstet Gynecol. 34:335–344. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Zhang XJP and Zheng J: Revised FIGO
staging of cervical cancer and treatments. Journal of International
Reproductive Health/Family Planning. 30:153–154. 2011.
|
|
3.
|
Fischerova D, Cibula D, Stenhova H, et al:
Transrectal ultrasound and magnetic resonance imaging in staging of
early cervical cancer. Int J Gynecol Cancer. 18:766–772. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Lees WR: Acoustic radiation force imaging:
a new method for quantifying hepatic fibrosis. Eur Radiol.
19:s3082009.
|
|
5.
|
Son CY, Kim SU, Han WK, et al: Normal
liver elasticity values using acoustic radiation force impulse
imaging: a prospective study in healthy living liver and kidney
donors. J Gastroenterol Hepatol. 27:130–136. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Fahey BJ, Nightingale KR, Nelson RC,
Palmeri ML and Trahey GE: Acoustic radiation force impulse imaging
of the abdomen: demonstration of feasibility and utility.
Ultrasound Med Biol. 31:1185–1198. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Yorifuji T, Tanaka T, Makino S, Koshiishi
T, Sugimura M and Takeda S: Balloon tamponade in atonic bleeding
induces uterine contraction: attempt to quantify uterine stiffness
using acoustic radiation force impulse elastography before and
after balloon tamponade. Acta Obstet Gynecol Scand. 90:1171–1172.
2011. View Article : Google Scholar
|
|
8.
|
Boursier J, Isselin G, Fouchard-Hubert I,
et al: Acoustic radiation force impulse: a new ultrasonographic
technology for the widespread noninvasive diagnosis of liver
fibrosis. Eur J Gastroenterol Hepatol. 22:1074–1084. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Sporea I, Sirli R, Bota S, Popescu A,
Sendroiu M and Jurchis A: Comparative study concerning the value of
acoustic radiation force impulse elastography (ARFI) in comparison
with transient elastography (TE) for the assessment of liver
fibrosis in patients with chronic hepatitis B and C. Ultrasound Med
Biol. 38:1310–1316. 2012. View Article : Google Scholar
|
|
10.
|
Colombo S, Buonocore M, Del Poggio A, et
al: Head-to-head comparison of transient elastography (TE),
real-time tissue elastography (RTE), and acoustic radiation force
impulse (ARFI) imaging in the diagnosis of liver fibrosis. J
Gastroenterol. 47:461–469. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Sporea I, Sirli R, Popescu A, et al: Is it
better to use together transient elastography (TE) and acoustic
radiation force impulse elastography (ARFI) for fibrosis evaluation
in patients with chronic HCV hepatitis? Gastroenterology.
140(Suppl): S9682011.
|
|
12.
|
Gallotti A, D’Onofrio M, Romanini L,
Cantisani V and Pozzi Mucelli R: Acoustic Radiation Force Impulse
(ARFI) ultrasound imaging of solid focal liver lesions. Eur J
Radiol. 81:451–455. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
D’Onofrio M, Gallotti A, Salvia R, Capelli
P and Mucelli RP: Acoustic radiation force impulse (ARFI)
ultrasound imaging of pancreatic cystic lesions. Eur J Radiol.
80:241–244. 2011.PubMed/NCBI
|
|
14.
|
Meng W, Zhang G, Wu C, Wu G, Song Y and Lu
Z: Preliminary results of acoustic radiation force impulse (ARFI)
ultrasound imaging of breast lesions. Ultrasound Med Biol.
37:1436–1443. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Friedrich-Rust M, Romenski O, Meyer G, et
al: Acoustic Radiation Force Impulse-Imaging for the evaluation of
the thyroid gland: a limited patient feasibility study.
Ultrasonics. 52:69–74. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Zheng X, Ji P, Mao H and Hu J: A
comparison of virtual touch tissue quantification and digital
rectal examination for discrimination between prostate cancer and
benign prostatic hyperplasia. Radiol Oncol. 46:69–74. 2012.
View Article : Google Scholar
|
|
17.
|
Syversveen T, Midtvedt K, Berstad AE,
Brabrand K, Strøm EH and Abildgaard A: Tissue elasticity estimated
by acoustic radiation force impulse quantification depends on the
applied transducer force: an experimental study in kidney
transplant patients. Eur Radiol. 22:2130–2137. 2012. View Article : Google Scholar
|
|
18.
|
Mansour N, Stock KF, Chaker A, Bas M and
Knopf A: Evaluation of parotid gland lesions with standard
ultrasound, color duplex sonography, sonoelastography, and acoustic
radiation force impulse imaging - a pilot study. Ultraschall Med.
33:283–288. 2012. View Article : Google Scholar
|
|
19.
|
Allen JD, Ham KL, Dumont DM, Sileshi B,
Trahey GE and Dahl JJ: The development and potential of acoustic
radiation force impulse (ARFI) imaging for carotid artery plaque
characterization. Vasc Med. 16:302–311. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Feltovich H, Reusch L, Palmeri M, Carlsen
L and Hall T: Exploration of the human cervix using acoustic
radiation force impulse (ARFI) measurements. Am J Obstet Gynecol.
206(Suppl): S2182012. View Article : Google Scholar
|
|
21.
|
Sun LT, Ning CP, Liu YJ, Wang ZZ, Wang LD,
Kong XC and Tian JW: Is transvaginal elastography useful in
pre-operative diagnosis of cervical cancer? Eur J Radiol.
81:e888–e892. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Yang Z: Compare application value between
vaginal ultrasound and abdominal ultrasound in gynecology and
obstetrics. Chinese Journal of Ethnomedicine and Ethnopharmacy.
17:132–134. 2010.(In Chinese).
|
|
23.
|
Mateen MA, Muheet KA, Mohan RJ, et al:
Evaluation of ultrasound based acoustic radiation force impulse
(ARFI) and eSie touch sonoelastography for diagnosis of
inflammatory pancreatic diseases. JOP. 13:36–44. 2012.PubMed/NCBI
|
|
24.
|
Thomas A, Kümmel S, Gemeinhardt O and
Fischer T: Real-time sonoelastography of the cervix: tissue
elasticity of the normal and abnormal cervix. Acad Radiol.
14:193–200. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Krishnakumar M: Ultrasound Elastography.
Apollo Medicine. 3:224–226. 2010. View Article : Google Scholar
|
|
26.
|
Shuang-Ming T, Ping Z, Ying Q, Li-Rong C,
Ping Z and Rui-Zhen L: Usefulness of acoustic radiation force
impulse imaging in the differential diagnosis of benign and
malignant liver lesions. Acad Radiol. 18:810–815. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Osaki A, Kubota T, Suda T, et al: Shear
wave velocity is a useful marker for managing nonalcoholic
steatohepatitis. World J Gastroenterol. 21:2918–2925. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Gallotti A, D’Onofrio M and Pozzi Mucelli
R: Acoustic Radiation Force Impulse (ARFI) technique in ultrasound
with Virtual Touch tissue quantification of the upper abdomen.
Radiol Med. 115:889–897. 2010. View Article : Google Scholar : PubMed/NCBI
|