Introduction
Orthodontic tooth movement is based on the response
of biological tissue towards a mechanical force. The movement
occurs as a result of alveolar bone remodeling through the
prolonged application of a controlled force. The applied force
induces bone resorption and bone formation on the pressure and
tension zones, respectively. In order to move a tooth in the
intended direction, bone resorption on the pressure side of the
socket wall creates space for the advancing tooth, while bone
deposition on the tension side maintains a progressively advancing
socket wall behind the moving tooth (1,2).
Bone remodeling involves the resorption of bone tissue with the
simultaneous formation of new bone tissue; the two processes are in
dynamic equilibrium in normal bone (3). During orthodontic tooth movement,
alveolar bone resorption at the area of compression occurs through
osteoclastic activities by osteoclasts, consequently creating
lacunae which are later occupied by osteoblasts to cover the
cavity. There are two processes in bone resorption, the
solubilization of minerals and the degradation of the organ matrix,
largely consisting of type I collagen. These processes are mediated
by proteolytic enzymes, including matrix metalloproteinases and
lysosomal cysteine proteinases (4). In the tension region, new bone is
formed as a result of mechanical force during orthodontic treatment
and osteoblasts differentiate from the local precursor cells. Then
osteoid is formed by mature osteoblasts and is further mineralized
with the secretion of calcium ion (5).
Root resorption is a common feature during
orthodontic tooth movement. Histological studies have reported that
root resorption occurs in 90% of teeth that have been moved
orthodontically (6,7). Root resorption, is an unavoidable
pathological outcome of orthodontic tooth movement. It is
considered to be the result of an inflammatory reaction; thus,
certain researchers call this process ‘orthodontically-induced
inflammatory root resorption’ (8).
The fundamental component behind the root resorption
process is local inflammation induced by mechanical forces which is
essential for tooth movement during orthodontic treatment (9). Studies have confirmed that
orthodontically-induced root resorption is a part of the hyaline
(sterile necrosis) zone elimination process. The first cells to be
involved in the removal of necrotic tissue are macrophage-like
cells, which may be activated by signals from sterile necrotic
tissue, as a result of orthodontic force application (10,11).
Osteoclasts and odontoclasts are implicated in the root resorption
process (10). In experimental
rats, the extent of root resorption is reported to increase only
when force reactivation is performed at the peak count of
osteoclasts in the involved region (12,13).
Several studies have reported the involvement of multinucleated
tartrate-resistant acid phosphatase-positive giant cells without
ruffled borders in the removal of hyaline tissue. These cells may
be early osteoclasts or odontoclasts (preosteoclasts) that become
involved in the elimination of necrotic tissue. The cells
differentiate into fully developed osteoclasts or odontoclasts
within hours following the introduction of a new mechanical
stimulus (14–16).
Under normal health conditions, bone tissue
undergoes a continuous process of balanced remodeling, regulated by
a number of systemic and local factors (17). Wnt ligands are among the local
signaling factors implicated in the process of bone remodeling.
Therefore, pharmacological modulation of this pathway may affect
bone mass. Activation of the canonical Wnt signaling pathway ex
vitro and in vivo may be achieved with lithium chloride
(LiCl) (18–20).
Lithium enhances bone formation and improves bone
mass in mice, and may do so via the activation of the canonical Wnt
pathway (21). The Wnt coreceptor
low-density lipoprotein receptor-related protein 5, interacts with
the Wnt ligand and members of the Frizzled co-receptor family at
the cell surface, transducing the Wnt signal via the canonical
pathway and ultimately leading to the nuclear accumulation of
β-catenin (22). β-catenin
enhances bone formation, through a canonical Wnt signaling cascade.
Previous studies have shown tissue cell-specific osteoblast
production failure in mice with β-catenin inactivation (23–25),
while mice with high levels of β-catenin in their osteoblasts,
undergo excessive bone formation with limited levels of osteoclasts
(23,26).
Although cementoblasts share certain phenotypical
features with osteoblasts, the canonical Wnt pathway inhibits
differentiation and promotes the proliferation of cells responsible
for laying down cementum on root surface (27). LiCl enhances bone formation by
inhibiting glycogen synthase kinase-3 (GSK-3), an enzyme that
phosphorylates β-catenin in the cytoplasm, targeting it for
ubiquitination and degradation. The process increases the
concentration of β-catenin and augments bone formation through the
activation of the canonical Wnt signaling pathway (18–20).
Little is known of the consequences of LiCl on
dental tissue (15,16,27),
therefore the aim of the current study was to uncover the effect of
LiCl on root resorption during orthodontic tooth movement in
rats.
Materials and methods
Animals
Ethical approval for this study was obtained from
the Institutional Animal Welfare Committee of the Chaoyang district
and the Jilin University Animal Care Commissioner (Changchun,
China). In total, 10 Sprague Dawley rats were purchased from the
Animal Laboratory of Jilin University. The study involved healthy
8-week-old male rats, weighing 200±10 g at the start of experiment.
The rats were randomly allocated into an experimental group (EG) or
control group (CG). There were 5 rats in each group.
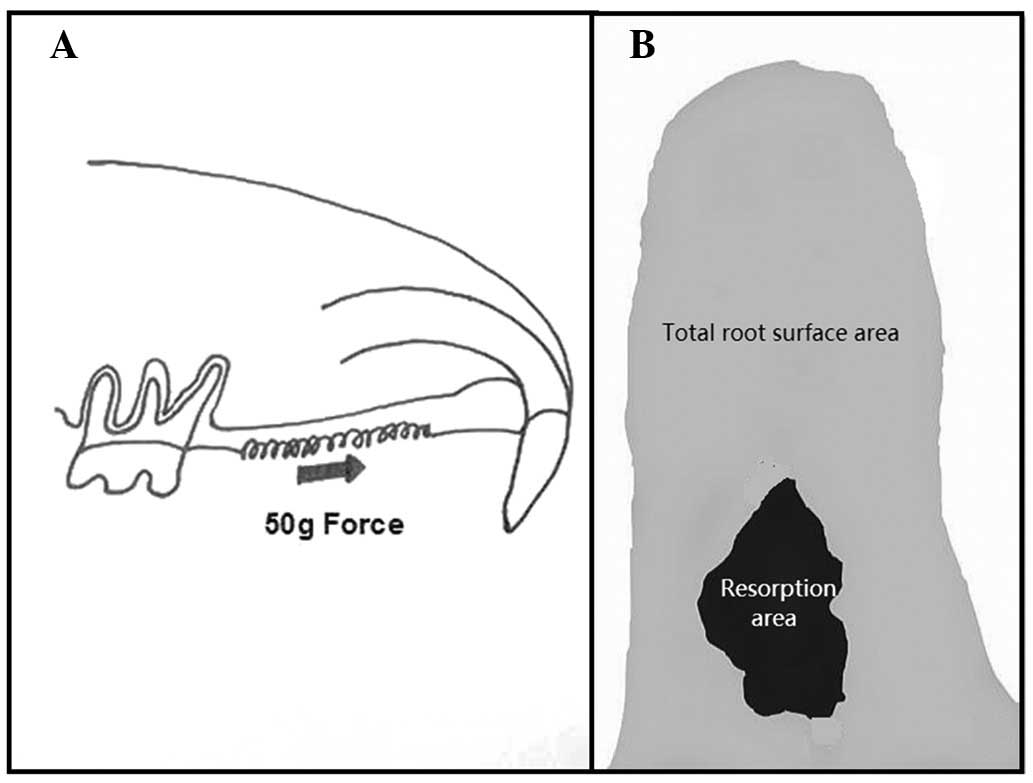
With the use of closed nickel-titanium (NiTi) coil
springs (Shengmate Technology Co. Ltd. Beijing, China), a 50-g
force was applied between the upper incisor and the first molars in
order to mimic orthodontic biomechanics in the experimental and
control groups. The appliances, consisting of a NiTi coil spring
tied with stainless steel wires between the maxillary incisors and
right first molar, were placed in all subjects under general
anesthesia (Fig. 1). A tension
gauge (Tianmei New Environmental Material Co. Ltd., Nanchang City,
China) was used to measure the force of the springs prior to
inserting them into the mouth of the rat. The ends of the ligature
wires were covered with composite resin to prevent the appliances
from loosening.
All subjects in the EG were gavage-fed 200-mg/kg
LiCl every 48 h during the experiment. The CG was not treated
medically. The rats were sacrificed after 14 days using an
anesthetic overdose.
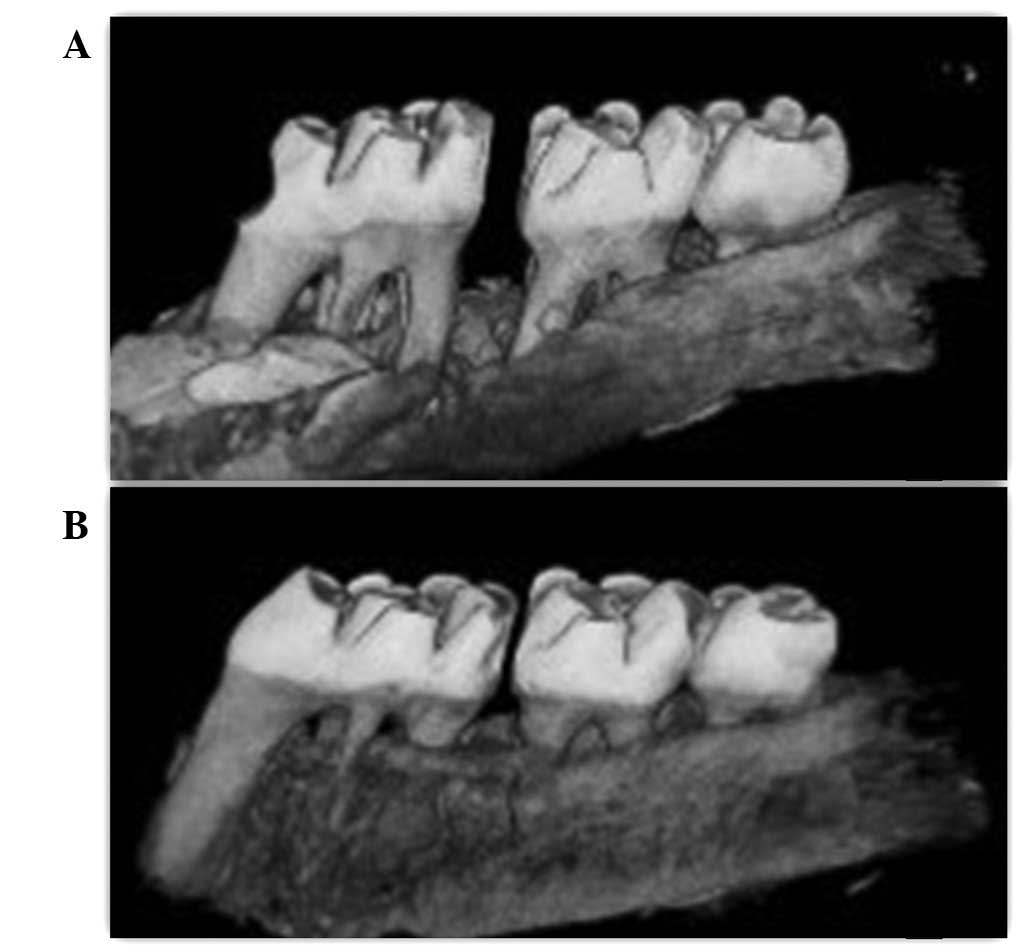
Tooth movement was assessed using ZKKS-MCT-Sharp
micro-computed tomography (Zhongke Kaisheng Medical Technology Co.
Ltd. Guangzhou, China). The rats were scanned at the same distance
and orientation in order to obtain the lateral cephalographs of the
maxillary molars with the surrounding alveolar bone (Fig. 2).
Measurement
The distance between the nearest points of the first
and second molars was measured on the digital radiographs of each
subject using ImageJ software version 1.44; (National Institutes of
Health, Bethesda, MD, USA) to determine the amount of tooth
movement. After measuring tooth movement, the maxillary right first
molar and the surrounding alveolar bone were extracted in
toto for root resorption assessment. The samples were soaked in
5% sodium hypochlorite solution for 12 h. Subsequently, the
alveolar bone was removed to expose the five roots of the first
molar. In order to obtain clear root surfaces, the distobuccal and
distopalatal roots were carefully cleaned to remove the remnants of
periodontal ligaments. The teeth were dried and scanned for
resorption area examination. The resorption areas on the digital
radiographs of the mesial surfaces of the distal roots were
measured using ImageJ software. The resorption area and the entire
mesial surface area of the two distal roots were measured
separately using the same software (Fig 3).
Statistical analysis
The resorption area ratio was obtained by dividing
the resorption crater area by the total surface area. The same
researcher measured all subjects, and every measurement was
repeated three times. The mean value was used in the final
analysis. One-way analysis of variance was performed using SPSS
version 17 (SPSS Inc., Chicago, IL, USA) to compare the groups.
P<0.05 was considered to indicate a statistically significant
result.
Results
Observations
The rats survived until the end of the experiment.
Prior to the experiment, none of the rats had a space between the
first and second molar crowns. Following 14 days of experimental
force application, all subjects had spaces of varying sizes between
the first and second right maxillary molars. The space appeared in
the third day after force loading and became apparent after 7 days.
The average distance measured in the CG was slightly higher than in
the EG. However, the difference was not considered statistically
significant (P=0.224; Table
I).
 | Table ITooth movement and root resorption
following 14 days of treatment. |
Table I
Tooth movement and root resorption
following 14 days of treatment.
| Variable | Experimental
group | Control group | P-value |
|---|
| Tooth movement,
mm | 0.1120±0.061 | 0.1755±0.072 | 0.224 |
| Root resorption area
ratio | 0.0491±0.027 | 0.1535±0.106 | 0.046* |
Roots of the target molars in all subjects were
successfully separated from the alveolar bone. Root resorption
craters with different forms were observed in the two groups
following the experiment, mainly in the cervical and middle
one-third of the root. Rough cementum areas were observed on the
mesial surface of the distobuccal and distopalatal roots. The mean
root resorption area ratio of the CG was significantly greater than
that of the EG (P<0.05).
Discussion
Previous studies have demonstrated the ability of
LiCl to enhance bone formation via the canonical Wnt/β-catenin
signaling pathway. LiCl has been used for decades for the treatment
of bipolar disorder by increasing β-catenin signaling through the
inhibition of GSK-3β (18,28). The canonical Wnt/β-catenin pathway
increases bone mass in several ways, including the renewal of stem
cells, stimulation of preosteoblast replication, induction of
osteogenesis and inhibition of osteoblast and osteocyte apoptosis
(29).
Since orthodontic tooth movement involves the
repeated process of alveolar bone remodeling (30,31),
LiCl has the potential to affect tooth movement during orthodontic
treatment by affecting the process of bone formation. Osteoclasts,
are involved in resorbing the alveolar bone at pressure areas,
which appear in the direction of the applied force, while
osteoblasts are involved in new bone formation at tension areas, on
the opposite side (30,32).
Osteoclasts and odontoclasts are implicated, with
other cells, in the orthodontically-induced inflammatory root
resorption process (14–16).
LiCl enhances bone formation through the canonical
Wnt/β-catenin pathway. Studies have shown that mice with high
levels of β-catenin in osteoblasts form excessive bone substances
with limited osteoclasts (23,26).
Since osteoclasts and odontoclasts share a variety of common
features, it is logical that LiCl may reduce root and alveolar bone
resorption in the pressure zone. This may be achieved through the
inhibition of osteoclasts and odontoclasts, which play key roles in
resorption during orthodontic tooth movement. In addition, the
enhancement of bone formation on the pressure side may slow down
tooth movement, which requires bone resorption to give way, ahead
of the moving tooth.
The current study observed a significant reduction
in the root resorption area ratio among the EG rats compared with
the CG rats (P<0.05), indicating that LiCl is capable of
suppressing root resorption during orthodontic treatment. This may
be due to the inhibitory effects of LiCl on osteoclastic cells
which are implicated in the orthodontically-induced inflammatory
root resorption process.
A variety of drugs that have been reported to limit
the inflammation process induced by orthodontic biomechanics, tend
to suppress root resorption and hinder the movement of teeth by
interfering with the resorption process on the pressure side
(34–36). The tooth movement measured in the
current study was higher in the CG compared with the EG. However,
the difference was not statistically significant. To the best of
our knowledge, there has been no studies published on the effects
of LiCl on root resorption and tooth movement with a comparable
study design. However, other studies have investigated the effect
of several medicaments on orthodontic tooth movement (38,39).
The topical application of bisphosphonates, which
are potent bone resorption inhibitors capable of inducing
osteoclast apoptosis (40), has
been reported to suppress orthodontic tooth movement (41,42).
Non-steroidal anti-inflammatory drugs (NSAIDs) have been reported
to suppress root resorption. NSAIDs tend to limit tooth movement
through the inhibition of the periodontal inflammatory response
induced by orthodontic force (34). Histological changes were not
assessed in the current study. Histological analysis is likely to
have provided valuable information regarding the effect of LiCl on
periodontal tissue during orthodontic tooth movement and is
acknowledged to be one of the shortcomings of this study. However,
the radiological findings of the study may be used as a foundation
for further investigations on the potential benefits of LiCl in
contemporary orthodontic clinical practice.
In conclusion, LiCl attenuates
orthodontically-induced root resorption during orthodontic tooth
movement. The effect of LiCl on tooth movement is
insignificant.
Acknowledgements
This study was supported by grants from the
Specialized Research Fund for the Doctoral Program of Higher
Education (no. 20110061110072), the National Natural Science
Foundation of China (no. 81170999) and the Graduate Innovation Fund
of Jilin University (no. 20121110).
References
|
1
|
Reitan K: Biomechanical principles and
reactions. Current Orthodontic Concepts and Techniques. 4th
edition. Graber TM and Swain BF: Elsevier Inc; St Louis, MO: pp.
145–219. 2005
|
|
2
|
Diravidamani K, Sivalingam SK and Agarwal
V: Drugs influencing orthodontic tooth movement: An overall review.
J Pharm Bioallied Sci. 4:S299–S303. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tanaka Y, Nakayamada S and Okada Y:
Osteoblasts and osteoclasts in bone remodeling and inflammation.
Curr Drug Targets Inflamm Allergy. 4:325–328. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Domon S, Shimokawa H, Matsumoto Y,
Yamaguchi S and Soma K: In situ hybridization for matrix
metalloproteinase-1 and cathepsin K in rat root-resorbing tissue
induced by tooth movement. Arch Oral Biol. 44:907–915. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sprogar S, Vaupotic T, Cör A, Drevensek M
and Drevensek G: The endothelin system mediates bone modeling in
the late stage of orthodontic tooth movement in rats. Bone.
43:740–747. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Harry MR and Sims MR: Root resorption in
bicuspid intrusion. A scanning electron microscope study. Angle
Orthod. 52:235–258. 1982.PubMed/NCBI
|
|
7
|
Stevnik A and Mjör IA: Pulp and dentine
reactions to experimental tooth intrusion. A histological study of
the initial changes. Am J Orthod. 57:370–385. 1970. View Article : Google Scholar
|
|
8
|
Liu Z, Xu J, EL and Wang D: Ultrasound
enhances the healing of orthodontically induced root resorption in
rats. Angle Orthod. 82:48–55. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bosshardt DD, Masseredjian V and Nanci A:
Root resorption and tissue repair in orthodontically treated human
premolars. Biological Mechanisms of Tooth Eruption, Resorption and
Replacement by Implants. Davidovitch Z and Mah J: Harvard Society
for the Advancement of Orthodontics; Boston, MA: pp. 425–437.
1998
|
|
10
|
Brudvik P and Rygh P: The initial phase of
orthodontic root resorption incident to local compression of the
periodontal ligament. Eur J Orthod. 15:249–263. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Brudvik P and Rygh P: Transition and
determinants of orthodontic root resorption-repair sequence. Eur J
Orthod. 17:177–188. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hughes B and King GJ: Effect of
orthodontic appliance reactivation during the period of peak
expansion in the osteoclast population. Anat Rec. 251:80–86. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhou D, Hughes B and King GJ:
Histomorphometric and biochemical study of osteoclasts at
orthodontic compression sites in the rat during indomethacin
inhibition. Arch Oral Biol. 42:717–726. 1997. View Article : Google Scholar
|
|
14
|
Roberts WE, Turley PK, Brezniak N and
Fiedler PJ: Bone physiology and metabolism. CDA J. 15:54–61.
1987.
|
|
15
|
Lindskog S, Blomlöf L and Hammarström L:
Dentin resorption in replanted monkey incisors. Morphology of
dentinoclast spreading in vivo. J Clin Periodontol. 15:365–370.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sismanidou C, Hilliges M and Lindskog S:
Healing of the root surface-associated periodontium: an
immunohistochemical study of orthodontic root resorption in man.
Eur J Orthod. 18:435–444. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Olsen BR, Reginato AM and Wang W: Bone
development. Annu Rev Cell Dev Biol. 16:191–220. 2000. View Article : Google Scholar
|
|
18
|
Hedgepeth CM, Conrad LJ, Zhang J, Huang
HC, Lee VM and Klein PS: Activation of the Wnt signaling pathway: a
molecular mechanism for lithium action. Dev Biol. 185:82–91. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Klein PS and Melton DA: A molecular
mechanism for the effect of lithium on development. Proc Natl Acad
Sci USA. 93:8455–8459. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
O’Brien WT, Harper AD, Jové F, Woodgett
JR, Maretto S, Piccolo S and Klein PS: Glycogen synthase
kinase-3beta haploinsufficiency mimics the behavioral and molecular
effects of lithium. J Neurosci. 24:6791–6798. 2004.PubMed/NCBI
|
|
21
|
Clément-Lacroix P, Ai M, Morvan F,
Roman-Roman S, Vayssière B, Belleville C, Estrera K, Warman ML,
Baron R and Rawadi G: Lrp5-independent activation of Wnt signaling
by lithium chloride increases bone formation and bone mass in mice.
Proc Natl Acad Sci USA. 102:17406–17411. 2005.PubMed/NCBI
|
|
22
|
Logan CY and Nusse R: The Wnt signaling
pathway in development and disease. Annu Rev Cell Dev Biol.
20:781–810. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Holmen SL, Zylstra CR, Mukherjee A, Sigler
RE, Faugere MC, Bouxsein ML, Deng L, Clemens TL and Williams BO:
Essential role of beta-catenin in postnatal bone acquisition. J
Biol Chem. 280:21162–21168. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hill TP, Später D, Taketo MM, Birchmeier W
and Hartmann C: Canonical Wnt/beta-catenin signaling prevents
osteoblasts from differentiating into chondrocytes. Dev Cell.
8:727–738. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Day TF, Guo X, Garrett-Beal L and Yang Y:
Wnt/beta-catenin signaling in mesenchymal progenitors controls
osteoblast and chondrocyte differentiation during vertebrate
skeletogenesis. Dev Cell. 8:739–750. 2005. View Article : Google Scholar
|
|
26
|
Glass DA II, Bialek P, Ahn JD, Starbuck M,
Patel MS, Clevers H, Taketo MM, Long F, McMahon AP, Lang RA and
Karsenty G: Canonical Wnt signaling in differentiated osteoblasts
controls osteoclast differentiation. Dev Cell. 8:751–764. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nemoto E, Koshikawa Y, Kanaya S, Tsuchiya
M, Tamura M, Somerman MJ and Shimauchi H: Wnt signaling inhibits
cementoblast differentiation and promotes proliferation. Bone.
44:805–812. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schou M: Lithium treatment at 52. J Affect
Disord. 67:21–32. 2001. View Article : Google Scholar
|
|
29
|
Krishnan V, Bryant HU and MacDougald OA:
Regulation of bone mass by Wnt signaling. J Clin Invest.
116:1202–1209. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Reitan K: Clinical and histologic
observations on tooth movement during and after orthodontic
treatment. Am J Orthod. 53:721–745. 1967. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Rygh P: Ultrastructural changes in tension
zones of rat molar periodontium incident to orthodontic tooth
movement. Am J Orthod. 70:269–281. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yoshimatsu M, Kitaura H, Fujimura Y,
Kohara H, Morita Y, Eguchi T and Yoshida N: Inhibitory effects of
IL-12 on experimental tooth movement and root resorption in mice.
Arch Oral Biol. 57:36–43. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Dolce C, Vakani A, Archer L, Morris-Wiman
JA and Holliday LS: Effects of echistatin and an RGD peptide on
orthodontic tooth movement. J Dent Res. 82:682–686. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Alakus Sabuncuoglu F and Esenlik E:
Influence of drugs on orthodontic tooth movement. Pakistan Oral
Dent J. 30:398–401. 2010.
|
|
35
|
Sandy JR and Harris M: Prostaglandins and
tooth movement. Eur J Orthod. 6:175–182. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kehoe MJ, Cohen SM, Zarrinnia K and Cowan
A: The effect of acetaminophen, ibuprofen and misoprostol on
prostaglandin E2 synthesis and the degree and rate of orthodontic
tooth movement. Angle Orthod. 66:339–349. 1996.PubMed/NCBI
|
|
37
|
Talic NF, Evans C and Zaki AM: Inhibition
of orthodontically induced root resorption with echistatin, an
RGD-containing peptide. Am J Orthod Dentofacial Orthop.
129:252–260. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Verma C, Hartig LE, Kalia S and Melsen B:
Influence of steroid drugs on orthodontically induced root
resorption. Orthod Craniofac Res. 9:57–62. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Nase JB and Suzuk JB: Osteonecrosis of the
jaw and oral bisphosphonate treatment. J Am Dent Assoc.
137:1115–1119. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Frith JC, Mönkkönen J, Auriola S,
Mönkkönen H and Rogers MJ: The molecular mechanism of action of the
antiresorptive and antiinflammatory drug clodronate: evidence for
the formation in vivo of a metabolite that inhibits bone resorption
and causes osteoclast and macrophage apoptosis. Arthritis Rheum.
44:2201–2210. 2001. View Article : Google Scholar
|
|
41
|
Adachi H, Igarashi K, Mitani H and Shinoda
H: Effects of topical administration of a bisphosphonate
(risedronate) on orthodontic tooth movements in rats. J Dent Res.
73:1478–1486. 1994.PubMed/NCBI
|
|
42
|
Igarashi K, Mitani H, Adachi H and Shinoda
H: Anchorage and retentive effects of a bisphosphonate (AHBuBP) on
tooth movements in rats. Am J Orthod. 106:279–289. 1994. View Article : Google Scholar : PubMed/NCBI
|