Introduction
The inflammatory myofibroblastic tumor (IMT) of the
urinary bladder is a rare benign lesion, particularly for the aged.
To the best of our knowledge, there is no study about inflammatory
myofibroblastic tumor of the urinary bladder in a patient with
unilateral renal cell carcinoma. The bladder lesion may be easily
masqueraded as metastasis from the left renal cell carcinoma due to
its hypervascularity. First, we performed radical operation of the
left kidney cancer with laparoscope, then after 3 weeks, according
to the intraoperative frozen section examinations, partial
cystectomy was performed. Thus avoiding radical resection of the
bladder and corresponding complications.
Case report
A 73-year-old male with hypertension, mild diabetes
and benign prostatic hyperplasia was admitted to The Second Xiangya
Hospital (Changsha, China). The patient complained of a one-year
history of dysuria and presented with frequent and urgent
urination, which was exacerbated by urodynia without hematuria for
the prior three months.
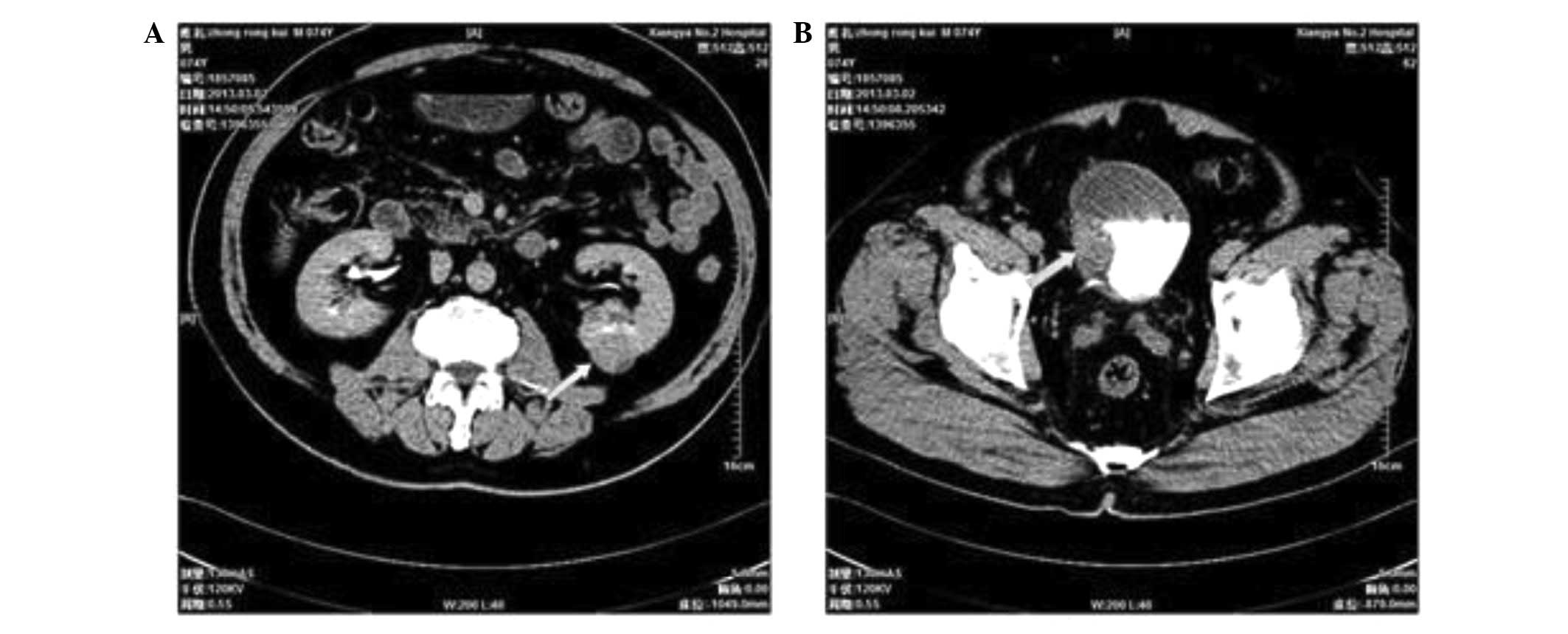
A computerised tomography (CT) scan of the patient
was performed and reviewed. A 2.5-cm slightly enhancing mass was
observed in the interpolar region of the left kidney and a 3×2-cm
enhancing mass was observed in the right and front walls of the
bladder (Fig. 1). A biopsy was not
obtained prior to surgery. A positron emission tomography (PET)-CT
scan was subsequently conducted and it revealed a 2.5×3.5-cm
slightly enhancing mass, with partially abnormal PET detection in
the interpolar region of the left kidney [maximum standardized
uptake value (SUV), 2.5] and in the right and front wall of the
bladder (maximum SUV, 3.5).
Under the diagnosis of left renal cell carcinoma
with possible metastasis to the urinary bladder, surgery was
performed. Laparoscopic exploration and radical resection of the
left kidney were performed, while attempting to resect as much of
the left ureter as possible. After the resection of the left
kidney, the left renal tissue was transported to The Department of
Pathology. The tissue was embedded in paraffin and sectioned by the
doctors of The Department of Pathology in The Second Xiangya
Hospital of Central South University (Changsha, China). The
pathological results were published by the professors of The
Department of Pathology in The Second Xiangya Hospital of Central
South University. The resected left renal material was paraffin
embedded and sectioned, and showed clear renal cell carcinoma
(Fig. 2). Exploration of the
bladder was performed three weeks later and a hard tumor of ~3×2 cm
was identified. The tumor was festering partially, penetrating the
serosa of the bladder and adhering to the surrounding tissues, and
was palpable where the right side and front walls of the bladder
merge. The mass was infiltrating the fat around the bladder, and
the internal orifice of urethra was clearly constrictive. In our
opinion, severe hyperplasia of the prostate gland and the severe
inflammation of the bladder may have contributed to the stricture.
The festering sections of the tumor were sent for rapid
cross-section frozen section examination and the presence of
cystitis glandularis was reported. Subsequently, under the
impression that the bladder tumor was maligant, the entire tumor
and the thickened parts of the bladder were sent to The Department
of Pathology in The Second Xiangya Hospital of Central South
University for rapid frozen cross-section examination and they
indicated a low-grade malignant mesenchymal tumor. Ultimately,
partial cystectomy was performed.
Discussion
An IMT was first reported by Bahadori and Liebow in
a lung lesion in 1973 (1). Tumor
invasion sites were reported to be mainly in the lung and
relatively rare in the urinary system. The tumor was subsequently
termed a plasma cell granuloma of the lung and Yamamoto et
al (2) reported that the
occurrence of IMTs was associated with the expression levels of the
genes p53 and murine double minute 2. In 2002, the World Health
Organization (3) officially
declared that IMTs were a type of mesenchymal tumor, few of which
relapse or transfer.
IMTs develop at any age, but commonly arise in
children and young adults, particularly in female individuals. The
occurrence of IMTs in elderly patients (>70 years old) and a
previous study (4) associated with
IMTs combined with the unilateral renal clear cell carcinoma are
extremely rare. In patients with an IMT of the urinary bladder with
renal cell carcinoma, it may be difficult to differentiate the
bladder lesion caused by the bladder cell metastasis from the renal
cell carcinoma (4). The
pathogenesis of IMTs is not clear and they present inflammatory
cell infiltration in histopathological analysis. Chronic infection
has been regarded as an important factor in the pathogenesis of
IMTs, and the microorganisms that have been isolated from IMT
lesions include mycobacteria, corynebacterium, Epstein-Barr virus
and human papilloma virus (5). In
the present case, the presence of diabetes and incomplete
obstruction of the bladder outlet may have induced a chronic
infection of the bladder of the patient.
The common clinical manifestations of IMTs of the
bladder in hematological analysis include gross hematuria, an
increased erythrocyte sedimentation rate, anemia and
hypergammaglobulinemia (6). A
small number of patients with an IMT present with frequent
micturition, urgency of urination, odynuria and dysuria, lower
abdominal pain or urinary tract symptoms (7) IMTs are usually reported by CT
scanning as a 2- to 11-cm tumor in the bladder or submucosa
(8), occasionally accompanied by
fat infiltration around the bladder. In the majority of cases of
IMTs, the imaging and cystoscopic findings are non-specific with
its hypervascularity and invasiveness. The imaging and cystoscopic
findings of this tumor always indicate the malignant tumors of the
urinary bladder due to its non-specificity, IMTs of the bladder are
difficult to diagnose, particularly prior to surgery. The bladder
lesions caused by an IMT (4) are
always locally aggressive and mimic those of malignancies, and it
is easy to misdiagnose an IMT as a malignant bladder tumor.
Furthermore, six months after treatment, patients with an IMT
exhibit no recurrence.
Radical resection is the preferred method of
treatment for IMTs of the bladder (9). The choice of partial resection of the
bladder or transurethral resection of a bladder tumor depends on
the depth of the tumor invasion. For large tumor masses, treatment
of the patients with celecoxib and prednisone is attempted first
(10), and then partial resection
of bladder is performed if the tumor has narrowed.
In the present case, it was difficult to distinguish
whether the two cases were due to transference as all the
iconographic data, including the PET-CT scan, indicated that the
masses in the left kidney and bladder of the patient may be
malignant. Intraoperative rapidly frozen cross-section examination
of IMT resection material is essential, particularly in the cases
when it is not possible to collect a preoperative biopsy, in order
to avoid radical resection of the bladder and the associated
complications.
References
|
1
|
Bahadori M and Liebow AA: Plasma cell
granulomas of the lung. Cancer. 31:191–208. 1973. View Article : Google Scholar
|
|
2
|
Yamamoto H, Oda Y, Saito T, Sakamoto A,
Miyajima K, Tamiya S and Tsuneyoshi M: p53 Mutation and MDM2
amplification in inflammatory myofibroblastic tumours.
Histopathology. 42:431–439. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fetcher CDM, Unni KK and Mertens F:
Pathology and Genetics of Tumors Soft Tissue and Bone. IARC press;
Lyon: 2002
|
|
4
|
Kim SH, Cho JY and Kim SH: Inflammatory
myofibroblastic pseudotumor of the urinary bladder in a patient
with bilateral renal cell carcinoma. J Ultrasound Med. 27:483–486.
2008.PubMed/NCBI
|
|
5
|
Arber DA, Weiss LM and Chang KL: Detection
of Epstein-Barr Virus in inflammatory pseudotumor. Semin Diagn
Pathol. 15:155–160. 1998.PubMed/NCBI
|
|
6
|
Tang TT, Segura AD, Oechler HW, et al:
Inflammatory myofibrohistiocytic proliferation simulating sarcoma
in children. Cancer. 65:1626–1634. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li HB, Xu YM and Yu JJ: Diagnostic puzzle
of inflammatory pseudotumor of the urinary bladder: a case report
with brief literature review. South Med J. 103:563–566. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fujiwara T, Sugimura K, Imaoka I and Igawa
M: Inflammatory pseudotumor of the bladder: MR findings. J Comput
Assist Tomogr. 23:558–561. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim HW, Choi YH, Kang SM, Ku JY, Ahn JH,
Kim JM, Chung JM, et al: Malignant inflammatory myofibroblastic
tumor of the bladder with rapid progression. Korean J Urol.
53:657–661. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Berger A, Kim C, Hagstrom N and Ferrer F:
Successful preoperative treatment of pediatric bladder inflammatory
myofibroblastic tumor with anti-inflammatory therapy. Urology.
70:372.e13–e15. 2007. View Article : Google Scholar
|
|
11
|
Fletcher CDM, Unni KK and Mertens F:
Pathology and Genetics of Tumors Soft Tissue and Bone. IARC press;
Lyon: 2002
|