Introduction
Nocardiosis is a rare but severe pyogenic infection
that is most commonly found in patients who are immunocompromised
(1). Pulmonary disease is the most
common presentation in patients with nocardiosis and approximately
one-third of such patients have a disseminated disease (2). Common predisposing factors for
nocardial infection include corticosteroid therapy, chemotherapy
for neoplasms and acquired immune deficiency syndrome. Patients
with nephrotic syndrome also have high morbidity of nocardial
infection due to immunosuppressive regimens. Hwang et al
(3) previously described a patient
with nephrotic syndrome, accompanied by pulmonary nocardiosis, but
negative for human immunodeficiency virus (HIV); however, to the
best of our knowledge, a patient with nephrotic syndrome with
nocardiosis who is also HIV-positive has yet to be reported. In the
present study, an unusual case of a patient with nephrotic syndrome
who developed disseminated nocardiosis following immunocompromised
therapy and HIV infection is described.
Case report
During the autumn of 2010, a 55-year-old male
developed edema in his lower legs and foamy urine. The patient was
admitted to the Changde Hospital, (Changde, China) and was
diagnosed with nephrotic syndrome. A test for antibodies against
HIV was found to be negative. The patient was treated with
prednisone therapy (60 mg/day) for 3 months, and the dosage was
then reduced to 5 mg/month. However, the patient failed to improve
after 10 months and was transferred to the Second Xiangya Hospital
(Changsha, China) for further investigation and treatment. On
admission, bilateral lower extremity edema was observed. Laboratory
studies identified a persistent albuminuria with an initial total
24 h urinary protein loss of 9.6 g and a serum albumin level of
13.4 g/l. The creatinine clearance rate was 58 ml/min. The blood
urea nitrogen level was normal; however, the serum cholesterol
level was grossly elevated (7.32 mmol/l). The patient tested
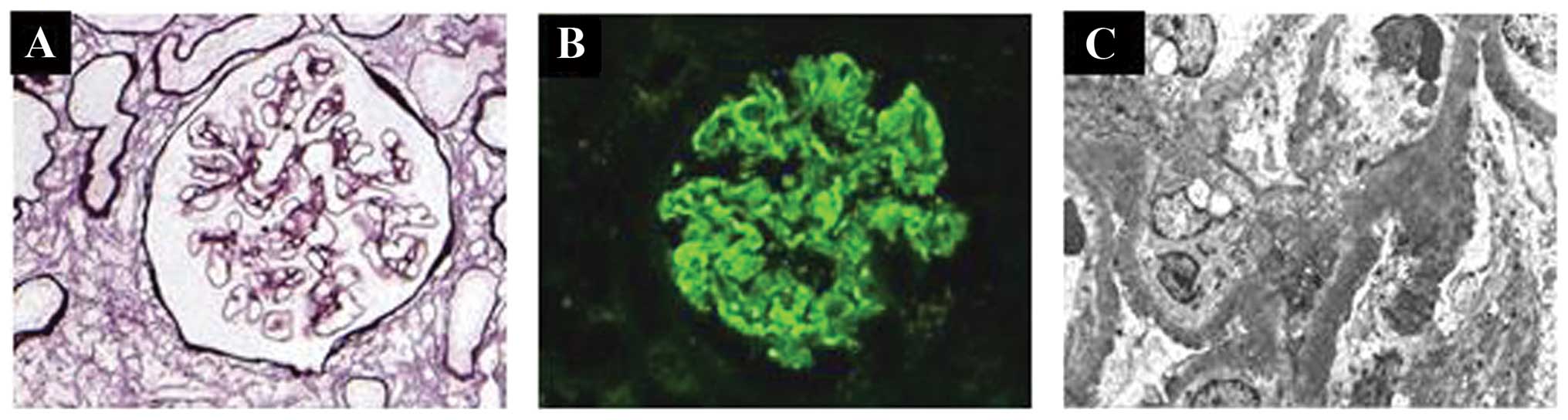
negative for antibodies against HIV. Renal biopsy showed membranous
nephropathy (Fig. 1) and the
patient was administered 30 mg prednisone daily and 1 mg tacrolimus
daily.
After ~3 months of treatment, the 24 h urinary
protein loss was reduced to 4.8 g/day and the level of serum
albumin rose to 20.2 g/l. However, the patient developed a fever
and started coughing up purulent sputum. The patient was diagnosed
with pneumonia in Hanshou Hospital (Hanshou, China) and was treated
with various combinations of penicillin, ceftriaxone and
itraconazole. However, the patient’s temperature continued to
increase and he was transferred again to the Second Xiangya
Hospital. On admission, the body temperature of the patient was
39.2°C. Inspiratory moist rales were audible in the right inferior
lung. A 2-cm hard subcutaneous nodule was palpable at the right
lower abdomen. The white blood cell count was 19.7×109/l
with 85% neutrophils. Tests for antibodies against tuberculosis
were negative and no Mycobacterium tuberculosis was found in
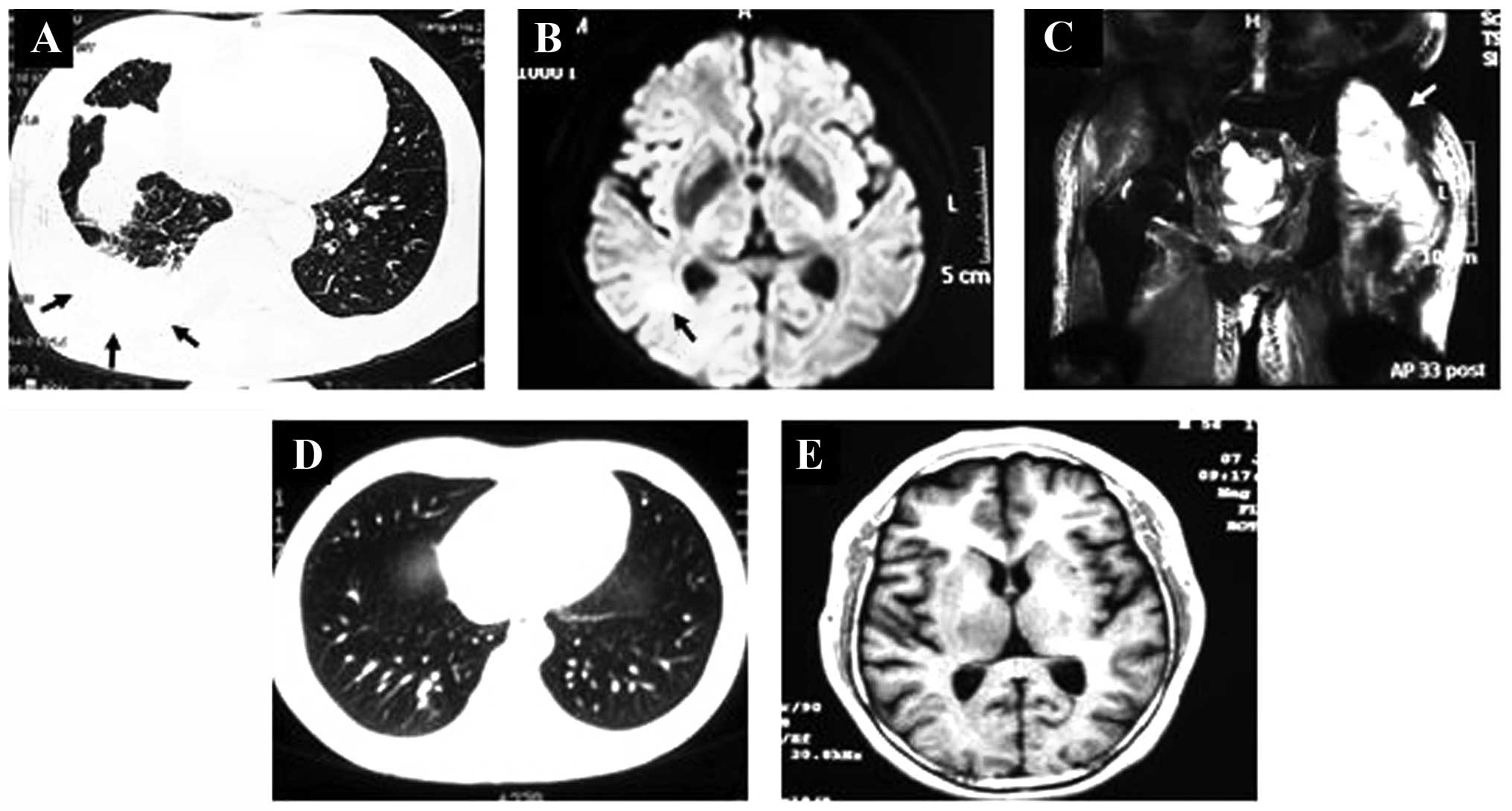
the sputum and hydrothorax. A chest computed tomography (CT) scan
revealed a nodule in the right lower lung field with pleural
effusion (Fig. 2A). After 1 week,
the patient developed left hip pain and magnetic resonance imaging
(MRI) revealed a brain abscess in the right temporal occipital
junction (Fig. 2B), as well as a
larger abscess in the left gluteal region (Fig. 2C). Pathogens isolated from sputum
and pus from the subcutaneous abdomen were identified as
Nocardia asteroides. Other pathogens, including bacteria,
mycobacteria and fungi were not isolated. The patient was therefore
diagnosed with nocardiosis. Antibodies against HIV were tested for
again and this time were found to be positive. The patient was
treated with surgical drainage of the hip abscess and the oral
administration of trimethoprim-sulfamethoxazole (0.96/4.8 g/day).
The patient was discharged after 50 days of hospitalization. The
trimethoprim-sulfamethoxazole therapy was continued and the patient
remained in a satisfactory condition. The results from the CT and
MIR scans showed that the size of the lung (Fig. 2D) and brain (Fig. 2E) abscesses decreased gradually
after 3 months and disappeared completely after 6 months.
Discussion
To the best of our knowledge, disseminated
nocardiosis in a patient with nephrotic syndrome and HIV infection
has not been previously reported. Nocardia species are
ubiquitous environmental microorganisms that are present worldwide
and belong to a diverse group of bacteria known as aerobic
actinomycetes. So far >50 species of the genus Nocardia
have been characterized, with ≥16 species that have been implicated
in human infection (4). The most
common of these include Nocardia asteroides, Nocardia
brasiliensis and Nocardia farcinica. In most cases,
Nocardia is an opportunistic pathogen, with the majority of
infections occurring in immunocompromised hosts, including those
with long-term corticosteroid exposure, malignancy, HIV infection
or a history of transplantation.
Peleg et al (2) previously demonstrated that treatment
with high doses of prednisone, a history of CMV infection and an
elevated mean calcineurin inhibitor level are independent risk
factors for Nocardia infection in organ transplant
recipients. Patients with nephrotic syndromes also have high
morbidity rates due to nocardial infection as a result of
immunosuppressive regimens. Particular attention should be given to
nocardial infection in immunocompromised patients if the infection
is not controlled following treatment with several antibiotics. In
the present study, the patient had two of these three risk factors:
previous treatment with prednisone and elevated levels of
calcineurin inhibitor. Tacrolimus, a calcineurin inhibitor,
inhibits T-cell activation by binding to FK-binding protein 12. T
cells are essential for an adequate host response against
Nocardia infection, primarily through the activation of
macrophages and the stimulation of a cellular immune response
(5).
In addition, in the present study the patient was
infected with HIV. Prior to the renal biopsy, the patient had
already been administered high-doses of prednisone for 10 months
without infection. However, 3 months following treatment with
prednisone and tacrolimus, the patient developed nocardiosis, an
opportunistic pathogen infection. The occurrence of an
opportunistic infection following the reduction of the steroid dose
is uncommon. Therefore, an HIV test was performed again and the
patient was found to have acquired an HIV infection during these 3
months. The HIV infection further destroyed the immune system of
the patient and induced the nocardial infection. The results from
the present study indicate that in cases of opportunistic
infections, further investigation into the risk factors of the
patient is required.
References
|
1
|
Ambrosioni J, Lew D and Garbino J:
Nocardiosis: updated clinical review and experience at a tertiary
center. 38:89–97. 2010.PubMed/NCBI
|
|
2
|
Peleg AY, Husain S, Qureshi ZA, Silveira
FP, Sarumi M, Shutt KA, Kwak EJ and Paterson DL: Risk factors,
clinical characteristics, and outcome of Nocardia infection
in organ transplant recipients: a matched case-control study. Clin
Infect Dis. 44:1307–1314. 2007.PubMed/NCBI
|
|
3
|
Hwang JH, Koh WJ, Suh GY, Chung MP, Kim H,
Kwon OJ, Lee KS, Lee NY and Han J: Pulmonary nocardiosis with
multiple cavitary nodules in a HIV-negative immunocompromised
patient. Intern Med. 43:852–854. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Brown-Elliott BA, Brown JM, Conville PS
and Wallace RJ Jr: Clinical and laboratory features of the
Nocardia spp. based on current molecular taxonomy. Clin
Microbiol Rev. 19:259–282. 2006.
|
|
5
|
Beaman BL and Beaman L: Nocardia
species: host-parasite relationships. Clin Microbiol Rev.
7:213–264. 1994.
|