Introduction
Lung cancer remains the leading cause of
cancer-associated mortality in developed countries, although
certain clinically-relevant advances have been achieved (1,2). The
majority of patients with lung cancer present with an advanced
progression of the disease at the time of diagnosis and mortality
is usually attributed to distant multiorgan metastases (3). Metastasis is a multistep process and
~90% of patients with cancer of any organ succumb due to metastases
(4). Consequently, developing
novel therapeutic strategies for the treatment of these patients
presents a great challenge. However, there may be marked
differences between the primary lung tumors and their metastases
with respect to morphology and biomarker expression. A critical
issue in the treatment of metastatic non-small cell lung cancer
(NSCLC) is the genetic variability and differences between the
primary tumors and their corresponding metastases.
The release of tumor cells from the primary tumor is
the primary step of metastasis. Changes to cell adhesion molecules
(CAMs) promote metastasis, which results in a deterioration of the
disease prognosis. β-catenin, a multifunctional protein encoded in
chromosome 3p21, is a crucial component of CAMs and is critical in
cell-cell adhesion and tissue remodeling processes (5). In cell-cell adhesion, β-catenin binds
to the intracellular domain of E-cadherin (6,7).
E-cadherin is a well-characterized cell-cell adhesion molecule that
connects neighboring epithelial cells in a specialized structure
termed the adherens junction (8).
It is an invasion suppressor gene that is frequently inhibited or
undergoes mutation in invasive tumors (9). E-cadherin also mediates adhesive
interactions between epithelial cells and exerts an effect on the
organization of the actin cytoskeleton through binding to
β-catenin.
β-catenin plays an important role in the
Wnt/β-catenin signaling pathway by activating the transcription of
target genes and leading to cell proliferation, invasion and
metastasis (10). Wnt signaling is
transduced through β-catenin, which is regulated by the adenomatous
polyposis coli (APC)/axin/glycogen synthase kinase (GSK) 3β
complex. In the presence of Wnt stimulation, the dishevelled
segment polarity protein 1 (DVL1) gene is activated, at least in
part by phosphorylation, which in turn recruits the GSK-3β complex
away from the degradation complex (11–13).
This allows the stabilization of β-catenin, resulting in the
accumulation of free cytosolic β-catenin. β-catenin is able to
translocate to the nucleus where it complexes with T cell factor
(TCF)/lymphoid enhancer binding factor (LEF) to stimulate the
expression of Wnt-target molecules (11,14).
Thus, the protein β-catenin exhibits a combined
function in cells as a major structural component of cell-cell
adherens junctions and as a central signaling molecule in the Wnt
signaling pathway. However, few studies have analyzed the functions
of β-catenin in patient-matched lung primary lesions and
patient-matched distant metastases regarding either the
cadherin-catenin system or the Wnt signaling pathway. In order to
evaluate the dual role of β-catenin and to determine its importance
as a predictor of metastasis and disease progression, the present
study investigated the expression levels of Wnt1, β-catenin and
E-cadherin in lung adenocarcinoma (ADC) and squamous cell
carcinomas (SqCC) sections.
Materials and methods
Clinical data acquisition
The present study cohort comprised 460 patients with
NSCLC who underwent surgical resection at Seoul National University
Bundang Hospital (Seoul, Korea) from May 2003 to April 2008. Of the
460 patients included, 112 patients had recurrence and from these,
41 specimens of the primary tumors and their corresponding
metastatic lesions were available for study. The current study
procedures were approved by the Institutional Review Board (IRB) at
Seoul National University Bundang Hospital (B1008-109-301).
Immunohistochemical assays
Sections (4 μm thick) from formalin-fixed,
paraffin-embedded tissue were deparaffinized in xylene and
rehydrated in graded ethanol. The succeeding steps were performed
automatically at 37°C using the Benchmark® XT Slide
Staining System Specifications (Ventana Medical Systems, Tucson,
AZ, USA). Antigen retrieval was performed by immersing the slides
in citrate buffer (pH 6.0) for 15 min and endogenous peroxidases
were blocked with 1% H2O2 for 10 min.
The sections were incubated with rabbit polyclonal
antibody for Wnt1 (H-89; Santa Cruz Biotechnology, Inc., Santa
Cruz, CA, USA; dilution 1:100), mouse monoclonal antibody for
β-catenin (5H10; Zymed Laboratories, Invitrogen Life Technologies,
Carlsbad, CA, USA; dilution 1:1,000) and mouse monoclonal antibody
for E-cadherin (SPM471; Thermo Fisher Scientific, Waltham, MA, USA;
dilution 1:150) at 4°C overnight. The sections were subsequently
washed with tris-buffered saline (pH 7.4).
The biotinylated secondary antibody was incubated
with the sections for 20 min. The slides were then stained using a
diaminobenzidine detection kit and counterstained with hematoxylin.
The EnVision™ detection system (K5007, Dako, Glostrup,
Denmark) was used which included a peroxidase-conjugated polymer
backbone and secondary antibody molecules directed against rabbit
and mouse immunoglobulins.
Evaluation of the staining
Two pathologists (X.X and J.H.C.) independently
performed blinded semiquantitative evaluations of the staining
under a light microscope (BX51; Olympus Corporation, Tokyo, Japan),
without prior knowledge of the patient data. To calculate the
expression levels of Wnt1, the scoring criteria used were based on
a semiquantitative approach, in which the percentage of positive
tumor cells (0–100%) was determined and multiplied by the staining
intensity (0, negative; 1, weak; 2, moderate; 3, strong). A total
score within the range of 0–300 was generated for each sample,
where 0–100 was classified as negative and 101–300 was classified
as positive for Wnt1 expression.
For the expression of E-cadherin, a positive
expression of <30% in the membrane was considered as reduced
membranous expression. When evaluating the expression of β-catenin,
a classification of staining patterns was used as follows: i)
membranous pattern, the immunoreactivity was present solely in the
cell membranes; ii) membranous-cytoplasmic pattern, the
immunoreactivity was also present in the cytoplasm; iii)
cytoplasmic pattern, the immunoreactivity was predominantly in the
cytoplasm and in <20% of the nucleus; and iv)
cytoplasmic-nuclear pattern, the immunoreactivity was present in
the cytoplasm and concomitantly in >20% of the nucleus (15,16).
Strong positively stained specimens of the cytoplasmic-nuclear,
membranous-cytoplasmic and cytoplasmic patterns (≥10%) were
considered positive (17).
Specimens with membranous patterns <70% were considered to have
reduced β-catenin expression (18).
Statistical analysis
The analyses were performed using the SPSS 17.0
software (SPSS, Inc., Chicago, IL, USA). The χ2 test was
used to evaluate the comparison of β-catenin, E-cadherin and Wnt1
expression between primary and metastatic tumors. P<0.05 was
considered to indicate a medically statistically significant
difference.
Results
Patient characteristics
Of the 460 patients, 112 patients (112/460, 24.3%)
had recurrence and from these, 41 pairs of specimens of the primary
tumors and the corresponding metastatic lesions were available for
study. The origins of the 41 paired specimens used for analysis
were the lungs (n=26), brain (n=6), bone (n=1), liver (n=1), pleura
(n=3), spine (n=1), kidneys (n=2) and soft tissue (n=1; Table I). The patients consisted of 27
(65.9%) males and 14 (34.1%) females with ages ranging from 20 to
80 years (mean, 60.3 years). In terms of smoking status, the
patients were divided into 19 (46.3%) non-smokers and 22 (53.7%)
smokers. The hematoxylin and eosin-stained slides were reviewed
independently by two pathologists (X.X. and J.H.C.) to confirm the
original diagnoses, based on the World Health Organization criteria
(19). There were 31 ADCs and 10
SqCCs, with the tumor diameters ranging from 1.5 to 8.0 cm (mean,
4.0 cm). The 41 patients were classified at the time of initial
surgical removal using the 7th Edition of the International Union
Against Cancer and American Joint Committee on Cancer (AJCC) TNM
classification of Malignant Tumors from the International
Association for the Study of Lung Cancer (IASLC) (20) as follows: pathological stage
(P-stage) I, 9 (22.0%) patients; P-stage II, 14 (34.1%) patients
and; P-stage III, 18 (43.9%) patients. The detailed
clinicopathological characteristics of the patients in the present
study are summarized in Table
II.
 | Table IStatus of recurrence. |
Table I
Status of recurrence.
| Metastatic site | Total (n) | Available tissues
(n) |
|---|
| Lung | 53 | 26 |
| Brain | 15 | 6 |
| Bone | 12 | 1 |
| Liver | 6 | 1 |
| Pleura | 12 | 3 |
| Adrenal gland | 3 | 0 |
| Spine | 3 | 1 |
| Pancreas | 2 | 0 |
| Kidney | 2 | 2 |
| Soft tissue | 2 | 1 |
| Skin | 1 | 0 |
| Heart | 1 | 0 |
| Total | 112 | 41 |
| Table IIClinicopathologic characteristics. |
Table II
Clinicopathologic characteristics.
| Characteristics | No. of patients | Percentage (%) |
|---|
| Total | 41 | 100.0 |
| Gender |
| Male | 27 | 65.9 |
| Female | 14 | 34.1 |
| Age |
| ≤65 | 24 | 58.5 |
| >65 | 17 | 41.5 |
| Smoking |
| Non-smoker | 19 | 46.3 |
| Smoker | 22 | 53.7 |
| Histological
type |
| Adenocarcinoma | 31 | 75.6 |
| Squamous cell
carcinoma | 10 | 24.4 |
| Tumor size |
| ≤3 cm | 13 | 31.7 |
| >3 cm | 28 | 68.3 |
| Pleural invasion |
| Absent | 25 | 61.0 |
| Present | 16 | 39.0 |
| Venous
invasion |
| Absent | 31 | 75.6 |
| Present | 10 | 24.4 |
| Lymphatic
invasion |
| Absent | 15 | 36.6 |
| Present | 26 | 63.4 |
| Perineural
invasion |
| Absent | 37 | 90.2 |
| Present | 4 | 9.8 |
| Necrosis |
| <10% | 22 | 53.7 |
| ≥10% | 19 | 46.3 |
| Tumor status |
| T1 | 10 | 24.4 |
| T2 | 24 | 58.5 |
| T3 | 7 | 17.1 |
| Nodal status |
| N0 | 16 | 39.0 |
| N1 | 8 | 19.5 |
| N2 | 16 | 39.0 |
| N3 | 1 | 2.4 |
| P-stage |
| stage I | 9 | 22.0 |
| stage II | 14 | 34.1 |
| stage III | 18 | 43.9 |
| Survival |
| Alive | 25 | 61.0 |
| Succumbed | 16 | 39.0 |
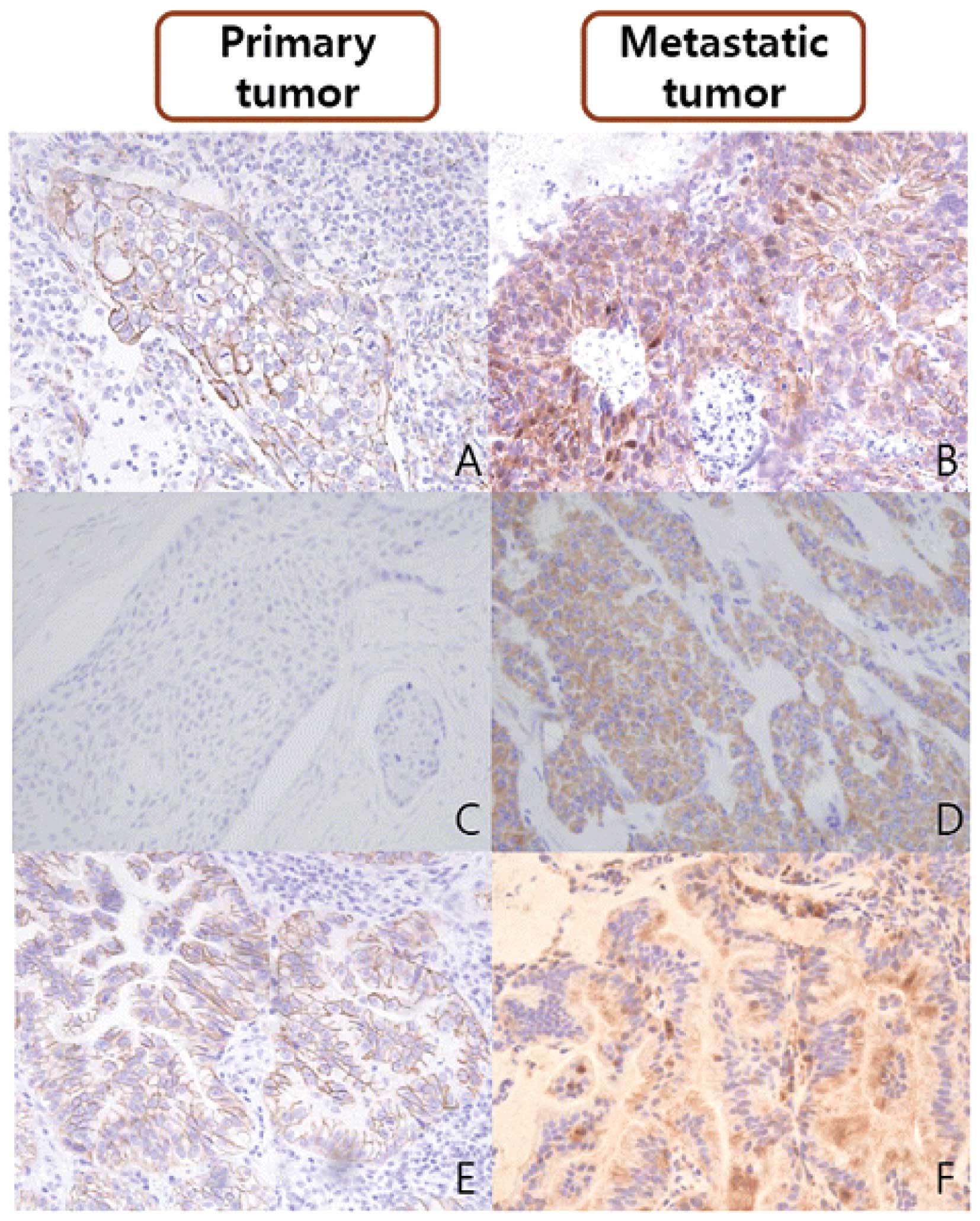
Expression of β-catenin by the primary
tumors and the corresponding metastases
β-catenin expression was normally localized to the
cell membrane of the respiratory epithelium; however, reduced
expression in the cell membrane, cytoplasm and/or nuclear
translocation was considered an indication of its aberrant
expression. Altered expression of β-catenin was more frequent in
the metastatic tumors (34/41, 82.9%) than in their corresponding
primary tumors (24/41, 58.5%; P<0.05). In the 12 discordant
cases of β-catenin expression, where the β-catenin expression
status differed between the primary tumor and the metastasis, 11
cases revealed acquired β-catenin alterations in the metastatic
lesions; the exception was one case of SqCC (case no. 39; Table III).
| Table IIIImmunohistochemical changes from
primary to metastatic tumors. |
Table III
Immunohistochemical changes from
primary to metastatic tumors.
| No. | Histology | Metastasic
site | β-catenin | E-cadherin | Wnt1 |
|---|
| 1 | ADC | Lung | ● | ● | ● |
| 2 | ADC | Spine | ● | ● | ◐ |
| 3 | ADC | Brain | ● | ● | ◑ |
| 4 | ADC | Brain | ● | ● | ◯ |
| 5 | ADC | Soft tissue | ● | ◐ | ● |
| 6 | ADC | Lung | ● | ◐ | ◑ |
| 7 | ADC | Bone | ● | ◑ | ● |
| 8 | ADC | Pleura | ● | ◑ | ● |
| 9 | ADC | Kidney | ● | ◑ | ● |
| 10 | ADC | Pleura | ● | ◑ | ◐ |
| 11 | ADC | Lung | ● | ◑ | ◐ |
| 12 | ADC | Lung | ● | ◑ | ◐ |
| 13 | ADC | Lung | ● | ◑ | ◯ |
| 14 | ADC | Lung | ● | ◯ | ● |
| 15 | ADC | Lung | ● | ◯ | ● |
| 16 | ADC | Bronchus | ● | ◯ | ◯ |
| 17 | ADC | Lung | ◑ | ◑ | ● |
| 18 | ADC | Lung | ◑ | ◑ | ● |
| 19 | ADC | Lung | ◑ | ◑ | ● |
| 20 | ADC | Lung | ◑ | ◑ | ◐ |
| 21 | ADC | Lung | ◑ | ◑ | ◯ |
| 22 | ADC | Liver | ◑ | ◑ | ◯ |
| 23 | ADC | Pleura | ◑ | ◯ | ● |
| 24 | ADC | Lung | ◑ | ◯ | ● |
| 25 | ADC | Lung | ◑ | ◯ | ◑ |
| 26 | ADC | Bronchus | ◯ | ◑ | ● |
| 27 | ADC | Lung | ◯ | ◑ | ● |
| 28 | ADC | Brain | ◯ | ◯ | ● |
| 29 | ADC | Brain | ◯ | ◯ | ● |
| 30 | ADC | Lung | ◯ | ◯ | ● |
| 31 | ADC | Lung | ◯ | ◯ | ◐ |
| 32 | SqCC | Kidney | ● | ● | ◯ |
| 33 | SqCC | Lung | ● | ◐ | ◯ |
| 34 | SqCC | Brain | ● | ◑ | ● |
| 35 | SqCC | Lung | ● | ◑ | ◐ |
| 36 | SqCC | Lung | ● | ◑ | ◐ |
| 37 | SqCC | Bronchus | ● | ◑ | ◯ |
| 38 | SqCC | Lung | ● | ◯ | ◯ |
| 39 | SqCC | Bronchus | ◐ | ◯ | ◐ |
| 40 | SqCC | Brain | ◑ | ● | ◑ |
| 41 | SqCC | Lung | ◑ | ● | ◑ |
Following subgroup analysis of the 31 cases of ADC,
discordance in β-catenin expression between the primary tumors and
the metastatic lesions was revealed in nine cases (9/31, 29.0%).
All nine discordant cases demonstrated acquired β-catenin
alterations in the metastatic tumors (Table III).
Subgroup analysis of the 10 cases of SqCC revealed
three cases of discordance in β-catenin expression between the
primary and matched metastases. Among them, two cases (case nos. 40
and 41) demonstrated acquired β-catenin alterations in the
metastases but normal β-catenin expression in the primary tumors.
The status of β-catenin expression in the primary and metastatic
tumors is summarized in Fig. 1 and
Tables III and IV.
| Table IVComparison of β-catenin, E-cadherin
and Wnt1 expression between primary and metastatic tumors. |
Table IV
Comparison of β-catenin, E-cadherin
and Wnt1 expression between primary and metastatic tumors.
| | β-catenin
alteration | E-cadherin
loss | Wnt1
overexpression |
|---|
| |
|
|
|
|---|
| Tumor type |
Characteristics | + | − | P-value | + | − | P-value | + | − | P-value |
|---|
| Total (n=41) | Primary tumor | 24 | 17 | 0.004 | 10 | 31 | 0.001 | 27 | 14 | NS |
| Metastatic
tumor | 34 | 7 | | 26 | 15 | | 23 | 18 | |
| ADC (n=31) | Primary tumor | 16 | 15 | 0.003 | 6 | 25 | 0.002 | 23 | 8 | NS |
| Metastatic
tumor | 25 | 6 | | 19 | 12 | | 20 | 11 | |
| SqCC (n=10) | Primary tumor | 8 | 2 | NS | 4 | 6 | NS | 4 | 6 | NS |
| Metastatic
tumor | 9 | 1 | | 7 | 3 | | 3 | 7 | |
Correlation of β-catenin and E-cadherin
expression in the primary tumors and the corresponding
metastases
Immunohistochemical analysis revealed that
E-cadherin expression was uniform in the cell membranes of the
normal bronchial mucosa. E-cadherin expression was mainly observed
on the membranes of the tumor cells and in certain cases, in the
cytoplasm. Loss of E-cadherin expression had greater prevalence in
metastatic tumors (26/41, 63.4%) than in their matching primary
tumors (10/41, 24.4%; P<0.05; Fig.
1 and Table IV).
Following subgroup analysis of the 31 cases of ADC,
discordance of E-cadherin expression between the primary tumors and
metastatic lesions was observed in 17 cases (17/31, 54.8%). Among
these, 15 (88.2%) cases acquired aberrant expression of E-cadherin
in the metastases, although the expression was unaltered in the
primary tumors. Altered β-catenin expression was associated with a
decreased level of E-cadherin expression (P<0.001; Table V). Among the nine cases of ADC that
demonstrated acquired β-catenin alterations in the metastatic
lesions, six cases (6/9, 66.7%) were accompanied by E-cadherin loss
but no Wnt1 overexpression (Table
III).
| Table VComparison of β-catenin vs.
E-cadherin and Wnt1 expression in adenocarcinomas. |
Table V
Comparison of β-catenin vs.
E-cadherin and Wnt1 expression in adenocarcinomas.
| | E-cadherin
expression | | Wnt1
expression |
|---|
| |
| |
|
|---|
| Characteristic | | ◯ | ◑ | ◐ | ● | P-value | ◯ | ◑ | ◐ | ● | P-value |
|---|
| β-catenin
expression | ◯ | 4 | 2 | 0 | 0 | <0.001 | 0 | 0 | 1 | 5 | NS |
| ◑ | 3 | 6 | 0 | 0 | | 2 | 1 | 1 | 5 | |
| ◐ | 0 | 0 | 0 | 0 | | 0 | 0 | 0 | 0 | |
| ● | 3 | 7 | 2 | 4 | | 3 | 2 | 4 | 7 | |
In the subgroup analysis of the 10 cases of SqCC,
there were five cases showing discordances in E-cadherin expression
between the primary and matched metastases. Among these, four cases
(case nos. 34–37) revealed decreased E-cadherin expression in the
metastases but normal expression in the primary tumors (Table III). No significant association
was identified between the expression of β-catenin and that of
E-cadherin in the cases of SqCC.
Correlation of β-catenin and Wnt1
expression in the primary tumors and the corresponding
metastases
Wnt1 expression appeared in the form of a
cytoplasmic staining pattern (Fig.
1). Wnt1 expression was negative in the non-neoplastic type I
or II pneumocytes, bronchiolar epithelial cells, mesenchymal cells
and inflammatory cells.
In the subgroup analysis of the 31 cases of ADC,
discordance of Wnt1 expression between the primary tumors and
metastatic lesions was observed in nine cases (9/31, 29.0%). Among
the nine cases of ADC that revealed acquired β-catenin alterations
in the metastatic lesion, only one case (1/9, 11.1%; case no. 25)
had an accompanying change in Wnt1 expression. In a further seven
cases (7/9, 77.8%) the expression levels of Wnt1 were preserved
from the primary tumor to the metastatic lesions. The remaining
case (1/9, 11.1%; case no. 20) overexpressed Wnt1 in the primary
tumor but revealed no expression of Wnt1 in the metastatic tumor
(Table III). No correlation was
identified between the expression of Wnt1 and β-catenin in the
cases of ADC (Table V).
In the subgroup analysis of the 10 cases of SqCCs,
the expression of Wnt1 was preserved from the primary to metastatic
tumors in 50% (5/10) of cases. There were three cases revealing
discordance in β-catenin expression between the primary and matched
metastases. Among them, two cases (case nos. 40 and 41) that
demonstrated β-catenin alterations in the metastases and intact
expression in their primary tumors exhibited acquired Wnt1
overexpression in the metastases. The remaining case (case no. 39)
exhibited altered β-catenin expression in the primary tumors but
intact β-catenin expression in the metastatic lesion. In these
three cases, altered β-catenin expression was accompanied by
altered Wnt1 expression, but no change in E-cadherin expression
(Table III). However, no
significant association was identified between the expression of
β-catenin and Wnt1 in the primary and metastatic tumors due to the
small number of cases examined.
Discussion
The present study aimed to investigate whether the
distant metastases of lung cancer may have aberrant β-catenin
expression compared with the primary tumor and how such β-catenin
expression is regulated. Distant metastases are common and numerous
studies that have investigated metastatic patterns in primary lung
cancer have revealed large variations in the frequency of
metastatic involvement between organ systems (4,21,22).
The most frequently involved intrathoracic sites are the: lungs
(24–97%), mediastinal lymph nodes (46–85%) and pleura (15–45%). The
most frequently involved extrathoracic sites are the: liver
(38–58%), brain (14–45%), bone (20–40%) and adrenal glands (36–64%)
(23,24). The data from the present study are
within a similar range to those previously reported.
In the current study, aberrant expression of
β-catenin in the primary tumors was preserved in the metastatic
lesions for the majority of cases of ADC and SqCC (23/41, 56.1%),
with the exception of one case of SqCC. The acquisition of changes
in β-catenin expression during the metastatic progression of NSCLC
were observed in 26.8% (11/41) of cases. These results suggest that
the alteration of β-catenin expression is an important mechanism in
tumor progression and the metastasis of NSCLC. Previous studies
have also demonstrated that the aberrant expression of β-catenin is
an independent prognostic factor of NSCLC, regardless of tumor,
node and metastasis (TNM) stage (16,25).
The results of the present study also indicate that
the loss of E-cadherin expression was much more prevalent in the
metastatic tumors than in their matching primary tumors. Intact
complexes of β-catenin/E-cadherin are important adhesion molecules
and inhibitors of cancer invasion and metastasis. In the current
study, the results indicate that changes in the stability and
function of the β-catenin/E-cadherin complex resulted in the
development of metastasis in tumors. A number of previous studies
have also revealed a significant association between reduced
E-cadherin expression and tumor differentiation grade, lymph node
involvement, venous invasion and distant metastasis (24,26).
However, few studies have verified these results using primary
tumors and their matching metastatic tumors.
The results of the present study demonstrated that
the alteration in β-catenin expression may be affected by signaling
pathways that differ according to histological type. Alterations in
β-catenin expression were significantly associated with the loss of
E-cadherin in ADCs. Among the nine cases of ADC that acquired
β-catenin alterations in the metastatic tumors, six cases (66.7%)
were accompanied by a reduction in E-cadherin expression, and there
was only one case (11.1%) in which Wnt1 overexpression was detected
in the metastatic tumor. These results suggest that the aberration
of β-catenin expression during tumor progression and metastasis in
ADCs is more likely to be associated with the cadherin-catenin
system than with the Wnt signaling pathway. Previous studies have
also revealed that the aberration of β-catenin expression may
induce epithelial-mesenchymal transition (EMT) during the
development of cell lines and tumors (27–29).
Another previous study has demonstrated that altered
E-cadherin/β-catenin complex expression is important in tumor
invasion and has an effect on the survival rate of patients with
ADCs (30). Collectively, the
results of present study revealed that the cadherin-catenin system
is an important regulator of the distant metastasis of lung
ADC.
Alterations in β-catenin expression between the
primary and metastatic tumors in the cases of SqCC were accompanied
by Wnt1 overexpression but not a loss of E-cadherin expression.
This suggests that the aberration of β-catenin in tumor progression
and metastasis in SqCCs may be associated with the Wnt signaling
pathway rather than the cadherin-catenin system. However, it
remains unclear as to whether the metastasis in SqCC is mediated by
the Wnt signaling pathway due to the small number of cases
analyzed. Therefore, further large-scaled studies are required to
evaluate the role of the Wnt signaling pathway in the metastasis of
SqCC.
The present study had certain limitations. The
sample size was relatively small, particularly that which dealt
with the Wnt-1 regulated β-catenin expression. Of the original 460
patients, 112 had recurrences but only 41 of these (31 ADCs and 10
SCCs) had tissue samples that were available for further study.
Since the majority of patients with extrathoracic metastasis did
not undergo further biopsies or surgery, the primary and
corresponding metastatic specimens were scarce and difficult to
obtain. Thus, larger studies are required to confirm the
observations made in the current study.
In conclusion, three significant results were
established in the present study. Firstly, primary lung carcinomas
that develop into distant metastases may have aberrant β-catenin
expression. Secondly, aberration of E-cadherin expression occurred
frequently during the metastatic progression of NSCLC. Finally,
changes in β-catenin expression may be regulated by the
cadherin-catenin system in ADCs, but mediated by the Wnt pathway in
SqCCs.
Acknowledgements
This study was supported by grants from the Basic
Science Research Program through the National Research Foundation
of Korea (NRF) funded by the Ministry of Education (2013-059757 to
JHC and 2011-0025344 to JEK). The authors are indebted to J.
Patrick Barron (Professor Emeritus of Tokyo Medical University and
Adjunct Professor of Seoul National University Bundang Hospital)
for his pro bono editing of the study.
References
|
1
|
Rikova K, Guo A, Zeng Q, et al: Global
survey of phosphotyrosine signaling identifies oncogenic kinases in
lung cancer. Cell. 131:1190–1203. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lee HJ, Xu X, Kim H, et al: Comparison of
direct sequencing, PNA clamping-real time polymerase chain
reaction, and pyrosequencing methods for the detection of EGFR
mutations in non-small cell lung carcinoma and the correlation with
clinical responses to EGFR tyrosine kinase inhibitor treatment.
Korean J Pathol. 47:52–60. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stenbygaard LE, Sørensen JB, Larsen H and
Dombernowsky P: Metastatic pattern in non-resectable non-small cell
lung cancer. Acta Oncol. 38:993–998. 1999. View Article : Google Scholar
|
|
5
|
Amin N and Vincan E: The Wnt signaling
pathways and cell adhesion. Front Biosci (Landmark Ed). 17:784–804.
2012. View Article : Google Scholar
|
|
6
|
Iwatsuki M, Mimori K, Yokobori T, et al:
Epithelial-mesenchymal transition in cancer development and its
clinical significance. Cancer Sci. 101:293–299. 2010. View Article : Google Scholar
|
|
7
|
Mei XD, Su H, Song J and Dong L:
Prognostic significance of β-catenin expression in patients with
non-small cell lung cancer: a meta-analysis. Biosci Trends.
7:42–49. 2013.PubMed/NCBI
|
|
8
|
Thiery JP, Acloque H, Huang RY and Nieto
MA: Epithelial-mesenchymal transitions in development and disease.
Cell. 139:871–890. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Christiansen JJ and Rajasekaran AK:
Reassessing epithelial to mesenchymal transition as a prerequisite
for carcinoma invasion and metastasis. Cancer Res. 66:8319–8326.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Polakis P: Wnt signaling and cancer. Genes
Dev. 14:1837–1851. 2000.PubMed/NCBI
|
|
11
|
Barker N and Clevers H: Catenins, Wnt
signaling and cancer. Bioessays. 22:961–965. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bienz M and Clevers H: Linking colorectal
cancer to Wnt signaling. Cell. 103:311–320. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Peifer M and Polakis P: Wnt signaling in
oncogenesis and embryogenesis - a look outside the nucleus.
Science. 287:1606–1609. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
You Z, Saims D, Chen S, et al: Wnt
signaling promotes oncogenic transformation by inhibiting
c-Myc-induced apoptosis. J Cell Biol. 157:429–440. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Huang CL, Liu D, Ishikawa S, et al: Wnt1
overexpression promotes tumour progression in non-small cell lung
cancer. Eur J Cancer. 44:2680–2688. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Xu X, Sun PL, Li JZ, Jheon S, Lee CT and
Chung JH: Aberrant Wnt1/β-catenin expression is an independent poor
prognostic marker of non-small cell lung cancer after surgery. J
Thorac Oncol. 6:716–724. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu HT, Wang L, Lin D, et al: Abnormal
beta-catenin and reduced axin expression are associated with poor
differentiation and progression in non-small cell lung cancer. Am J
Clin Pathol. 125:534–541. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kase S, Sugio K, Yamazaki K, Okamoto T,
Yano T and Sugimachi K: Expression of E-cadherin and beta-catenin
in human non-small cell lung cancer and the clinical significance.
Clin Cancer Res. 6:4789–4796. 2000.
|
|
19
|
Travis WD, Brambilla E, Muller-Hermelink
HK and Harris C: Tumours of the lung, pleura, thymus and heart
Pathology and genetics. World Health Organization Classification of
Tumours. IARC Press; Lyon, France: 2004
|
|
20
|
Travis WD, Brambilla E, Noguchi M, et al:
International association for the study of lung cancer/american
thoracic society/european respiratory society international
multidisciplinary classification of lung adenocarcinoma. J Thorac
Oncol. 6:244–285. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bigin S, Yilmaz A, Ozdemir F, et al:
Extrathoracic staging of non-small cell bronchogenic carcinoma:
relationship of the clinical evaluation to organ scans.
Respirology. 7:57–61. 2002. View Article : Google Scholar
|
|
22
|
Wood SL, Pernemalm M, Crosbie PA and
Whetton AD: The role of the tumor-microenvironment in lung
cancer-metastasis and its relationship to potential therapeutic
targets. Cancer Treat Rev. 40:558–566. 2014. View Article : Google Scholar
|
|
23
|
Kremer M, Quintanilla-Martinez L, Fuchs M,
et al: Influence of tumor-associated E-cadherin mutations on
tumorigenicity and metastasis. Carcinogenesis. 24:1879–1886. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bongiorno PF, al-Kasspooles M, Lee SW, et
al: E-cadherin expression in primary and metastatic thoracic
neoplasms and in Barrett’s oesophagus. Br J Cancer. 71:166–172.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Li XQ, Yang XL, Zhang G, et al: Nuclear
β-catenin accumulation is associated with increased expression of
Nanog protein and predicts poor prognosis of non-small cell lung
cancer. J Transl Med. 11:1142013. View Article : Google Scholar
|
|
26
|
Mitselou A, Batistatou A, Nakanishi Y,
Hirohashi S, Vougiouklakis T and Charalabopoulos K: Comparison of
the dysadherin and E-cadherin expression in primary lung cancer and
metastatic sites. Histol Histopathol. 25:1257–1267. 2010.PubMed/NCBI
|
|
27
|
Ohishi Y, Oda Y, Kurihara S, et al:
Nuclear localization of E-cadherin but not beta-catenin in human
ovarian granulosa cell tumours and normal ovarian follicles and
ovarian stroma. Histopathology. 58:423–432. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang L, Cheng H, Liu Y, et al: Prognostic
value of nuclear β-catenin overexpression at invasive front in
colorectal cancer for synchronous liver metastasis. Ann Surg Oncol.
18:1553–1559. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Geyer FC, Lacroix-Triki M, Savage K, et
al: β-Catenin pathway activation in breast cancer is associated
with triple-negative phenotype but not with CTNNB1 mutation. Mod
Pathol. 24:209–231. 2011. View Article : Google Scholar
|
|
30
|
Kim H, Yoo SB, Sun P, et al: Alteration of
the E-Cadherin/β-Catenin complex is an independent poor prognostic
factor in lung adenocarcinoma. Korean J Pathol. 47:44–51. 2013.
View Article : Google Scholar : PubMed/NCBI
|