Introduction
Lung cancer is one of the most common cancers
worldwide. In the USA, an estimated 226,160 new cases were
diagnosed in 2012, accounting for 14% of cancer diagnoses. In
addition, lung cancer accounts for more mortalities than any other
type of cancer; an estimated 160,340 mortalities were reported in
2012, accounting for 28% of all cancer-related mortalities
(1). In China, lung cancer replaced
liver cancer as the leading cause of mortality in patients with
malignant tumors in 2008, and the mortality rate has increased by
464.84% in the past three decades (2). Lung cancer has two major forms, namely
small cell lung cancer (SCLC) and non-small cell lung cancer
(NSCLC); the latter of these accounts for 85–90% of lung cancer
cases (3). As early detection
methods are lacking, the majority of NSCLC patients are diagnosed
at an advanced stage of disease (4).
At present, the most common treatment approaches for advanced NSCLC
in clinical practice include surgery, chemotherapy and radiation
therapy; however, the prognosis of surgery is poor due to the high
incidence of recurrence. The effects of chemotherapy and radiation
therapy are also limited, associated with drug resistance and
adverse reactions (5). Therefore,
novel and effective therapeutic strategies are urgently required
for advanced NSCLC in clinical therapy.
With the rapid development of cellular and molecular
immunology, the pathogenesis of cancer has been closely linked to
the host immune system (6). A number
of researchers and doctors have recognized immunological therapy as
a promising therapeutic approach in the treatment of cancer when
following surgery, chemotherapy and radiation therapy (7,8). One
type of immunological therapy uses cytokine-induced killer (CIK)
cells, which are peripheral blood mononuclear cells (PBMCs) that
have been stimulated by various cytokines [interferon (IFN)-γ,
anti-cluster of differentiation (CD)3 antibodies, interleukin
(IL)-1 and/or IL-2]. This allows for the proliferation of effector
cells, which include non-specific T cells and natural killer (NK)
cells, with lymphokine-activated killer (LAK) activity. These
proliferative CIK cells simultaneously express the T-cell marker
CD3 and the NK cell marker CD56, which provide cytotoxic effects in
order to kill tumor cells. The CIK cells combine the marked
anticancer activity of T cells with the non-major
histocompatibility complex (MHC)-restricted anticancer activity of
NK cells (9). Compared with
conventional therapeutic approaches, CIK therapy has several
advantages, such as increased anticancer activity, a broader
anticancer spectrum, the ability to prevent tumor recurrence, and
fewer adverse reactions (10). CIK
cells have been evaluated as an adoptive immunotherapy by a number
of clinical trials investigating their clinical applicability in
the treatment of various kinds of cancers, including liver cancer
(11), lung cancer (12), melanoma (13), gastrointestinal cancer (14) and renal cell carcinoma (15,16).
The efficacy and safety of chemotherapy and CIK
immunotherapy co-treatment and chemotherapy alone for advanced
NSCLC have been evaluated in previous studies; however, these have
mainly focused on short-time overall survival (OS; <2 years),
progression free survival (PFS) and response rate (12,17–19). In
addition, few studies on factors predictive of clinical outcome in
immune therapy have been performed (20–23).
Therefore, an effective prognostic factor is urgently required to
improve the effectiveness of CIK therapy in advanced NSCLC
patients. The aim of the present study was to evaluate 29 whole
blood or serum indicators to identify factors that are predictive
of clinical outcome following CIK cell therapy combined with
chemotherapy, and to evaluate the 5-year prognosis of patients with
advanced NSCLC.
Materials and methods
Patient characteristics
The present study was approved by the Ethics
Committee of Chinese PLA General Hospital (Beijing, China). Written
informed consent was obtained from all patients. All the procedures
in this study were conducted in accordance with the Declaration of
Helsinki. From March 2008 to October 2013, 42 patients with
advanced NSCLC (stages III and IV) were enrolled at the
Biotherapeutic Department of the Chinese PLA General Hospital. All
of the patients with NSCLC were administered 4–6 cycles of
cisplatin- or carboplatin-based chemotherapy regimens, including
gemcitabine, pemetrexed or docetaxel. All patients were treated
with CIK cell therapy 7–10 days following chemotherapy. CIK cell
treatment was administered at 1-month intervals. All 42 patients
were eligible for CIK maintenance treatment until they no longer
agreed to continue maintenance treatment or until disease
progression occurred. For each therapy cycle, patients were given
an infusion of 2–10×109 CIK cells. Data concerning age,
gender, tumor stage, surgery resection status, CIK therapy cycle
and tumor subtype were also collected. Patient characteristics are
shown in Table I.
 | Table I.Characteristics of the 42 patients
enrolled in the study. |
Table I.
Characteristics of the 42 patients
enrolled in the study.
| Characteristic | Number |
|---|
| Age |
|
| ≥60
years | 21 |
| <60
years | 21 |
| Gender |
|
|
Male | 25 |
|
Female | 17 |
| Stage |
|
|
III | 11 |
| IV | 31 |
| Surgery
resection |
|
|
Yes | 8 |
| No | 34 |
| Therapy cycles |
|
| ≥4 | 22 |
|
<4 | 20 |
| Type |
|
|
Squamous | 30 |
|
Adenocarcinoma | 6 |
|
Others | 6 |
Preparation of CIK cells
All procedures used in CIK cell preparation were
performed within a sterile environment. Expansion and culture of
the CIK cells was performed in accordance with a previous method
(24). Peripheral blood (50 ml) was
collected, and PBMCs were extracted by Ficoll-Paque
density-gradient centrifugation (GE Healthcare Life Sciences,
Chalfont, UK). PBMCs were then washed three times in PBS, and
suspended in GT-T551 medium (2×106 cells/ml; Takara Bio,
Inc., Otsu, Japan), seeded into a 75-cm2 culture flask,
and then placed into a 5% CO2 incubator at 37°C. After 6
h, the liquid was transferred into a new 75-cm2 culture
flask, which had been pretreated with phosphate-buffered saline
containing 5 µg/ml mouse anti-CD3 monoclonal antibody (cat. no.
T210; Takara Bio, Inc.) at 4°C overnight. This medium was then
supplemented with 0.6% serum from the patient. On day 0, 1,000 U/ml
recombinant human interleukin-2 (rhIL-2; Peprotech, Inc. Rocky
Hill, NJ, USA) and 10,000 U/ml recombinant IFN-γ (Peprotech Inc.)
were added to the culture medium. The cells were cultured in a
humidified 5% CO2 incubator at 37°C. Fresh GT-T551
medium with 1,000 U/ml rhIL-2 was added every 3 days. CIK cells
were harvested on day 14. The collection criteria were as follows:
i) The proportions of CD3+,
CD3+CD8+ and CD3+CD56+
cells were >95, >80 and >20%, respectively, as determined
by flow cytometry; ii) cell viability, which was measured by Trypan
blue staining, was >95%; iii) contamination, such as bacteria,
fungi, endotoxins and Mycoplasma, could not be detected (as
assessed by researchers from the Department of Microbiology,
Chinese PLA General Hospital, Beijing, China); iv) the total number
of cells was 2–10×109. The CIK cell therapy cycle is
illustrated in Fig. 1.
Flow cytometric analysis of
phenotype
The CIK cells were resuspended in 100 µl of PBS
containing 15 µl of the following monoclonal mouse antibodies:
anti-CD4-fluorescein isothiocyanate (FITC), anti-CD8-phycoerythrin
(PE), anti-CD3-chlorophyll protein complex (PerCP), included within
a Tritest kit (cat. no. 340298), in addition to 5 µl
anti-CD56-allophycocyanin (APC; cat. no. 555518) in the dark for 30
min at 4°C, and then washed twice in PBS. The antibodies and
isotype control antibodies were purchased from BD Biosciences (San
Jose, CA, USA). These were used to stain cell surface markers in
order to identify the CIK phenotype. Data acquisition was performed
using a FACSCalibur flow cytometer (BD Biosciences).
Detection of 29 whole blood or serum
indicators
A total of 8 whole blood indicators that were
tested, namely hemoglobin, white blood cell (WBC) count, red blood
cell (RBC) count, platelet count, lymphocytes, monocytes, basophils
and eosinophils. These were detected using an XE-2100 Automated
Hematology System kit (Sysmex Corporation). A total of 21 serum
indicators were tested, which were: Lactate dehydrogenase (LDH),
alkaline phosphatase (ALP), alanine aminotransferase (ALT),
aspartate aminotransferase (AST), total protein (TP), albumin
(ALB), total bilirubin (TB), direct bilirubin (DB), total bile acid
(TBA), γ-glutamyl aminotransferase (γGGT), urea (UR), creatinine
(CR), uric acid (UA), carbon dioxide (CO2),
neuron-specific enolase (NSE), carcino-embryonic antigen (CEA),
α-fetoprotein (AFP), carbohydrate antigen (CA)125, CA724, CA153 and
CA199. Detection kits for LDH, ALP, ALT, AST, TP, ALB, γGGT, UR,
CR, UA, CO2, NSE, CEA, AFP, CA125, CA724, CA153 and
CA199 were provided by Roche Diagnostics (Basel, Switzerland). DB
and TB detection kits were provided by Hitachi Chemical Diagnostics
(Mountain View, CA, USA). TBA detection kits were provided by
Strong Biotechnologies (Beijing, China). LDH, ALP, ALT, AST, TP,
ALB, γGGT, UR, CR, UA, CO2, DB, TB and TBA were detected
using a Hitachi 7600 automatic biochemical analyzer (Hitachi,
Tokyo, Japan). NSE, CEA, AFP, CA125, CA724, CA153, and CA199 were
detected using a Roche E170EE automated immunoassay analyzer (Roche
Diagnostics).
Prognosis evaluation
The median progress free survival (mPFS) was used to
evaluate the prognosis of the patients with advanced NSCLC
receiving CIK cell therapy combined with chemotherapy. Patients
without a known date of mortality were reported as indicated at the
time of the last follow-up.
Statistical analysis
All statistical analysis was performed using SPSS
software (version 13 for Windows; SPSS, Inc., Chicago, IL, USA) and
GraphPad Prism (version 6 for Windows; GraphPad Software, Inc., La
Jolla, CA, USA). All data are reported as median (25th percentile,
75th percentile). The indicators were compared between pre- and
post-therapy by paired t-test, and the indicators between different
CIK cell therapy cycles were also compared by paired t-test. The
survival curves were calculated by the Kaplan-Meier method, and
differences between survival curves were compared by the log-rank
test. Log-rank tests were also used to conduct the single factor
analysis for age, gender, tumor stage, surgery resection status,
CIK therapy cycle, tumor subtype information, and differential
whole blood or serum indicators. Multivariate analysis was
performed using the Cox's proportional hazards regression model to
evaluate the significance of prognostic factors. P-values <0.05
were considered to indicate a significant difference.
Results
Comparison of peripheral lymphocyte
subsets
The percentages of CD3+,
CD3+CD4+, CD3+CD8+,
CD3+CD56+ and
CD8+CD56+peripheral lymphocyte subsets, and
the CIK/PBMC ratio in the first and second cycles of therapy were
compared with those in PBMCs, as reported in Fig. 2. The percentage of
CD3+CD4+ lymphocytes in the CIK group were
significantly reduced when compared with the PBMC group in the
first cycle (P<0.001) and second cycle (P<0.001) of therapy
(Fig. 2A and D). The percentage of
CD3+CD8+ lymphocytes in the CIK group
revealed a significant increase when compared with the PMBC group
in the first cycle (P<0.001) and second cycle (P<0.001) of
therapy (Fig. 2B and E). The
percentage of CD3+CD56+ lymphocytes in the
CIK group was also significantly increased when compared with that
in the PBMC group in the first (P=0.001) and second cycles
(P<0.001) of therapy (Fig. 2C and
F). Furthermore, the percentage of total CD3+
lymphocytes in the CIK group was significantly increased when
compared with that in the PBMC group in the first cycle
(P<0.001) and second cycle (P<0.001) of therapy (Fig. 2G and H). The CIK/PBMC ratio in the
first and second cycles of therapy was also compared. The CIK/PBMC
ratio in the second cycle was significantly reduced when compared
with that in the first cycle of therapy (P<0.001). However, no
significant difference was observed between the percentage of total
CD8+CD56+ lymphocytes in the CIK group and
the PBMC group following the first and second cycles of therapy
(both P>0.05; data not shown).
Comparison of whole blood routine and
serum biomarker tests
In addition to conducting an analysis of immune
indicators, 29 whole blood and serum biomarker indicators were
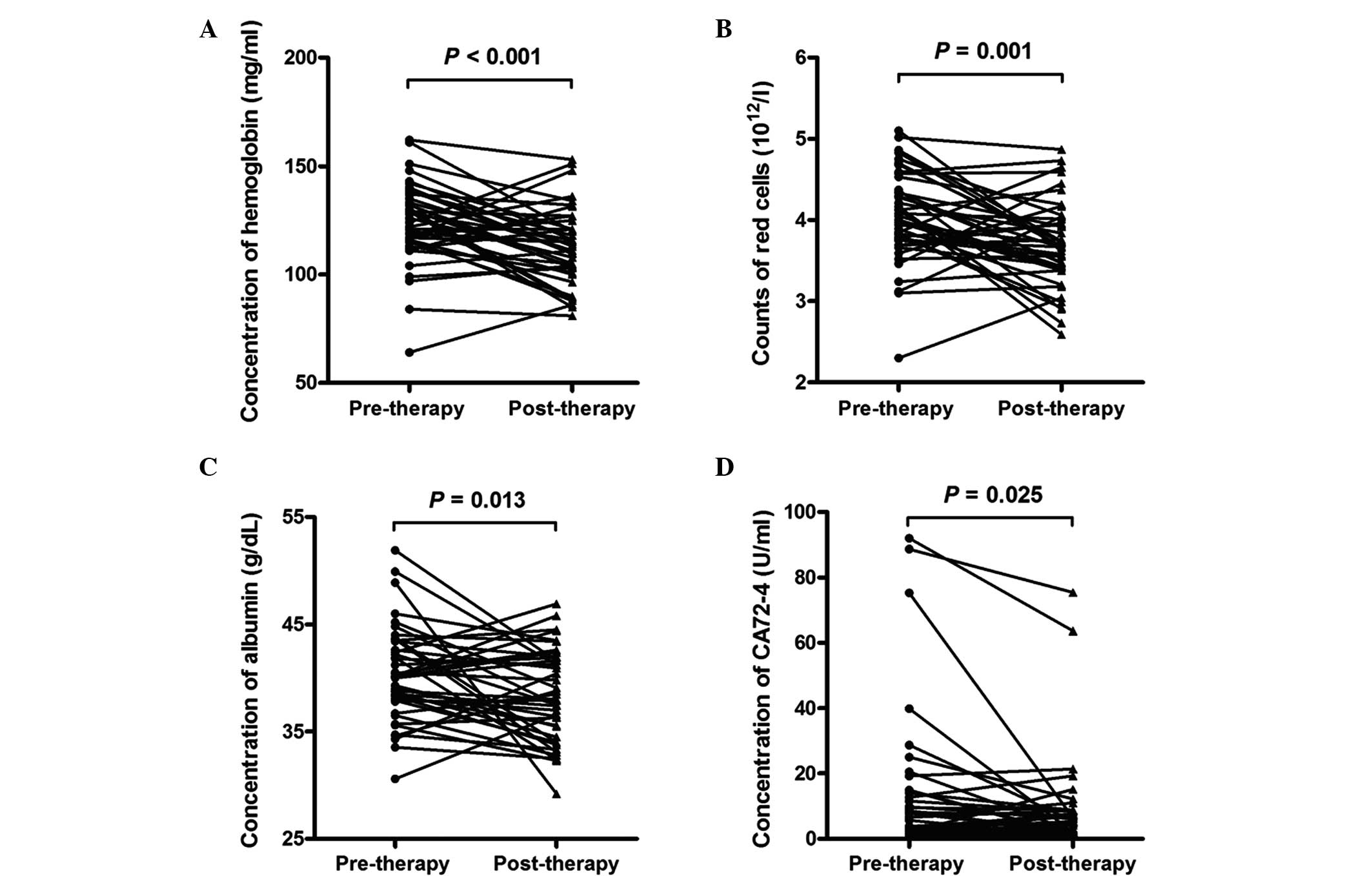
analyzed, the results of which are shown in Table II. The hemoglobin (P<0.001) and
RBC counts (P=0.001) of the whole blood analyses were significantly
reduced in the advanced lung cancer patients post-therapy when
compared with those pre-therapy (Fig. 3A
and B). The levels of hemoglobin in the pre-therapy group were
125.00 (115.75, 135.50) mg/ml, and in the post-therapy group were
112.00 (102.50, 122.00) mg/ml. The RBC count in the pre-therapy
group was 4.03 (3.74, 4.41) ×1012/l, and in the
post-therapy group was 3.67 (3.40, 4.01) ×1012/l. No
significant difference in the other indicators in the whole blood
analyses (WBC count, platelet count, lymphocytes, monocytes,
basophils and eosinophils) were observed between pre-therapy and
post-therapy in the patients with advanced lung cancer. In the
serum biomarker test, the ALB (P=0.013) and CA724 (P=0.025) levels
revealed a significant reduction in the patients with advanced lung
cancer post-therapy compared with those pre-therapy (Fig. 3C and D). The levels of ALB in the
pre-therapy group were 40.10 (37.88, 43.43) g/dl, and in the
post-therapy were 37.95 (34.38, 41.71) g/dl. The levels of CA724 in
the pre-therapy group were 6.10 (1.91, 14.20) U/ml, and in the
post-therapy group were 4.92 (2.05, 8.47) U/ml. The other
indicators in the serum biomarker test (including LDH, ALP, ALT,
AST, TP, TB, DB, TBA, γGGT, UR, CR, UA, CO2, NSE, CEA,
AFP, CA153, CA199, and CA125) revealed no observable significant
difference between pre-therapy and post-therapy in the advanced
lung cancer patients.
| Table II.Comparison of 29 whole blood routine
and serum biomarker indicators between pre-and post-therapy in 42
patients with advanced lung cancer. |
Table II.
Comparison of 29 whole blood routine
and serum biomarker indicators between pre-and post-therapy in 42
patients with advanced lung cancer.
| Indicator | Pre-therapy | Post-therapy | P-value |
|---|
| Hemoglobin,
mg/ml | 125.00 (115.75,
135.50) | 112.00
(102.50,122.00) |
<0.001a |
| WBC count,
×109/l | 5.36 (4.66,
7.04) | 5.17 (4.28,
6.98) | 0.795 |
| RBC count,
×1012/l | 4.03 (3.74,
4.41) | 3.67 (3.40,
4.01) | 0.001a |
| Platelet count,
×109/l | 246 (184.50,
297.50) | 255.5 (185.50,
310.00) | 0.163 |
| Lymphocytes, % | 0.27 (0.21,
0.31) | 0.313 (0.210,
0.37) | 0.400 |
| Monocytes, % | 0.72 (0.61,
0.90) | 0.076 (0.063,
0.093) | 0.575 |
| Basophils,% | 0.003 (0.002,
0.006) | 0.004 (0.002,
0.007) | 0.918 |
| Eosinophils, % | 0.014 (0.09,
0.028) | 0.02 (0.010,
0.037) | 0.058 |
| LDH, U/l | 173.6 (138.6,
244.9) | 182.075 (138.75,
246.48) | 0.772 |
| ALP, U/l | 78.25 (61.20,
99.15) | 71.3 (60.50,
96.48) | 0.992 |
| ALT, U/l | 17.05 (13.88,
26.60) | 17.7 (14.04,
26.60) | 0.341 |
| AST, U/l | 19.35 (15.30,
23.55) | 18.6 (16.05,
26.80) | 0.971 |
| TP, g/l | 64.70 (60.60,
72.20) | 64.6 (62.55,
68.00) | 0.147 |
| ALB, g/dl | 40.10 (37.88,
43.43) | 37.95 (34.38,
41.71) | 0.013a |
| TB, µmol/l | 9.85 (7.83,
11.95) | 8.65 (6.38,
11.20) | 0.190 |
| DB, µmol/l | 2.85 (2.08,
4.23) | 2.5 (1.79,
4.35) | 0.902 |
| TBA, µmol/l | 3.75 (2.95,
6.78) | 3.2 (2.55,
4.25) | 0.119 |
| γGGT, U/l | 33.33 (21.50,
56.98) | 33.25 (23.15,
61.33) | 0.668 |
| UR, mmol/l | 4.78 (3.79,
5.70) | 4.26 (3.40,
5.52) | 0.470 |
| CR, µmol/l | 66 (56.20,
73.10) | 61.73 (52.04,
79.96) | 0.425 |
| UA, µmol/l | 286.6 (248.53,
324.65) | 274.45 (230.23,
353.80) | 0.830 |
| CO2,
mmol/l | 27 (25.68,
28.73) | 27.33 (26.05,
28.48) | 0.389 |
| NSE, ng/ml | 11.55 (9.75,
16.69) | 12.55 (10.07,
19.13) | 0.338 |
| CEA, ng/ml | 5.24 (1.81,
19.04) | 6.25 (2.91,
56.10) | 0.489 |
| AFP, U/l | 2.84 (2.13,
3.92) | 3.02 (2.37,
3.96) | 0.552 |
| CA724, U/ml | 6.1 (1.91,
14.20) | 4.92 (2.05,
8.47) | 0.025a |
| CA153, U/ml | 20.01 (13.62,
32.60) | 27.43 (16.57,
51.93) | 0.237 |
| CA199, U/ml | 12.04 (6.14,
20.03) | 12.8 (8.34,
38.64) | 0.134 |
| CA125, U/ml | 53.38 (19.75,
110.40) | 30.34 (17.69,
124.60) | 0.462 |
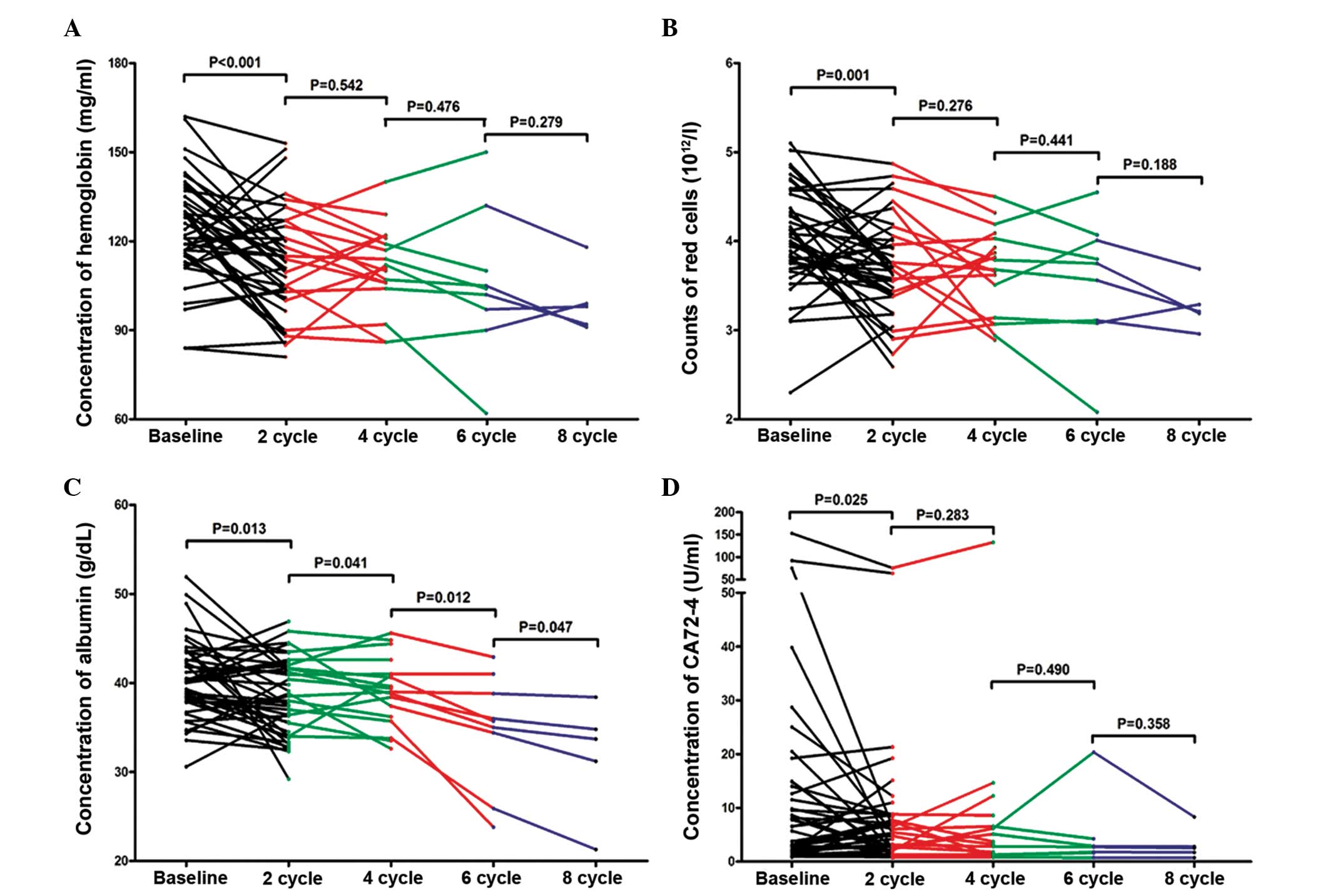
Differential indicators in continuous
therapy cycles
Following analysis of the differential indicators
between pre- and post-therapy in the advanced lung cancer patients,
the differential indicators hemoglobin, RBC, ALB, and CA724 were
compared between different numbers of continuous therapy cycles. No
significant difference in concentration of hemoglobin was observed
between 2 vs 4 cycles (P=0.542), 4 vs. 6 cycles (P=0.476) or 6 vs.
8 cycles (P=0.279; Fig. 4A). No
observably significant difference in RBC counts was detected
between 2 vs. 4 cycles (P=0.276), 4 vs. 6 cycles (P=0.441) and 6
vs. 8 cycles (P=0.188; Fig. 4B).
However, the data report in Fig. 4C
reveal that the concentration of albumin was significantly reduced
as the number of therapy cycles increased; 2 vs. 4 cycles
(P=0.041), 4 vs. 6 cycles (P=0.012), 6 vs. 8 cycles (P=0.047). The
concentration of albumin at 4, 6 and 8 cycles of therapy was 36.64
(36.08, 41.40), 35.70 (30.15, 39.90) and 33.70 (26.25, 36.60) g/dl,
respectively. No significant difference was observed in
concentration of CA724 between 2 vs. 4 cycles (P=0.283), 4 vs. 6
cycles (P=0.490) or 6 vs. 8 cycles (P=0.358; Fig. 4D).
Univariate and multivariate survival
analysis
The results of log-rank test analysis, as shown in
Table III, indicated that age,
gender, tumor stage, surgery resection status, the number of CIK
therapy cycles and tumor subtype were not significant predictors of
PFS (P>0.05). The mPFS time of the patients with high expression
levels of albumin [20.0 months, 95% confidence interval (CI):
17.4–22.6] was longer than the mPFS for patients with low
expression levels of albumin (36.0 months, 95% CI: 24.7–47.3), as
reported in Fig. 5. Following Cox
regression analysis, it was identified that the expression of
albumin had a significant effect on the prognosis of patients
following CIK cell therapy combined with chemotherapy
(P=0.034).
| Table III.Univariate analysis of factors for
prognosis analysis of patients with advanced lung cancer treated
with CIK cell therapy combined with chemotherapy. |
Table III.
Univariate analysis of factors for
prognosis analysis of patients with advanced lung cancer treated
with CIK cell therapy combined with chemotherapy.
|
|
| Kaplan-Meier single
factor analysis |
|---|
|
|
|
|
|---|
| Correlative
factor | No. | mPFS (months) | 95% CI | P-value |
|---|
| Age |
|
|
| 0.219 |
| ≥60
years | 21 | 24.0 | 17.0–36.0 |
|
| <60
years | 21 | 39.0 | 18.0–41.0 |
|
| Gender |
|
|
| 0.350 |
|
Male | 25 | 21.0 | 6.8–35.2 |
|
|
Female | 17 | 36.0 | 19.2–52.7 |
|
| Stage |
|
|
| 0.287 |
|
III | 11 | 48.0 | 32.3–63.7 |
|
| IV | 31 | 33.4 | 24.6–43.1 |
|
| Surgical
resection |
|
|
| 0.555 |
|
Yes | 8 | 31.0 | 14.7–47.3 |
|
| No | 34 | 25.0 | 6.3–43.7 |
|
| Therapy cycles |
|
|
| 0.058 |
| ≥4 | 22 | 39.0 | 22.0–55.9 |
|
|
<4 | 20 | 20.0 | 14.1–25.9 |
|
| Type |
|
|
| 0.148 |
|
Squamous | 30 | 37.7 | 28.0–47.5 |
|
|
Adenocarcinoma | 6 | 43.0 | 17.7–68.3 |
|
|
Others | 6 | 22.2 | 7.8–36.5 |
|
| Albumin |
|
|
| 0.034a |
|
Increased | 19 | 20.0 | 17.4–22.6 |
|
|
Decreased | 23 | 36.0 | 15.8–46.2 |
|
A Cox proportional hazards regression model was then
used to conduct a multivariate analysis of age, gender, tumor
stage, surgery resection status, CIK therapy cycles, tumor subtype,
and the expression of albumin, and the results are reported in
Table IV. The number of CIK therapy
cycles (P=0.041) and the concentration of albumin (P=0.038) were
demonstrated to be independent indicators in the prognosis of CIK
cell therapy combined with chemotherapy for patients with advanced
NSCLC. The risk of an adverse clinical outcome in patients
receiving ≥4 CIK therapy cycles patients was 0.38 (95% CI:
0.14–1.13)-fold that of the patients receiving <4 CIK therapy
cycles. The risk of an adverse clinical outcome in patients with
increased expression levels of albumin was 0.32 (95% CI:
0.10–1.24)-fold that of patients with lower expression levels of
albumin; patients with high expression levels of albumin and
receiving more CIK therapy cycles may therefore have a better
prognosis compared with patients with low expression levels of
albumin and receiving fewer treatment cycles. Other factors,
including age, gender, tumor stage, surgery resection status and
tumor subtype, did not appear to be independent prognostic factors
(P>0.05).
| Table IV.Multivariate analysis (Cox model) of
factors for prognosis analysis of patients with advanced lung
cancer treated with CIK cell therapy combined with
chemotherapy. |
Table IV.
Multivariate analysis (Cox model) of
factors for prognosis analysis of patients with advanced lung
cancer treated with CIK cell therapy combined with
chemotherapy.
|
| Cox multiple factor
analysis |
|---|
|
|
|
|---|
| Correlative
factor | P-value | Exp(B) | 95% CI |
|---|
| Age | 0.109 | 2.31 | 0.83–6.41 |
| ≥60
years |
|
|
|
| <60
years |
|
|
|
| Gender | 0.992 | 1.01 | 0.32–3.13 |
|
Male |
|
|
|
|
Female |
|
|
|
| Stage | 0.236 | 2.47 | 0.55–11.05 |
|
III |
|
|
|
| IV |
|
|
|
| Surgical
resection | 0.363 | 0.47 | 0.10–2.37 |
|
Yes |
|
|
|
| No |
|
|
|
| Therapy cycles |
0.041a | 0.38 | 0.14–1.13 |
| ≥4 |
|
|
|
|
<4 |
|
|
|
| Type | 0.166 | 1.54 | 0.84–2.82 |
|
Squamous |
|
|
|
|
Adenocarcinoma |
|
|
|
|
Others |
|
|
|
| Albumin |
0.038a | 0.32 | 0.10–1.24 |
|
Increased |
|
|
|
|
Decreased |
|
|
|
Discussion
The primary treatment approaches for cancers in
clinical practice are surgical resection, chemotherapy and
radiotherapy; however, efficacy can be poor due to high rates of
recurrence and a poor prognosis. With the development of immunology
and understanding of the etiology of cancer development,
immunological therapy has emerged as a promising treatment approach
for cancers. Previous studies have demonstrated that the adaptive
and innate cellular immunity are important for antitumor effects
(25–27). Antitumor cellular immune activity can
be markedly enhanced by increased lymphocyte number (28,29).
Immunological therapy is conducted using autologous T cells or NK
cells, which are isolated from the cancer patients, activated and
expanded in vitro; the expanded T cells or NK cells are then
re-infused in vivo into the cancer patients. These expanded
cells simultaneously express the T-cell marker CD3 and the NK cell
marker CD56, which provides the cells with cytotoxic activity,
enabling them to kill tumor cells (30). Immunotherapy is a promising therapy
in the advancement of cancer treatment; however, the efficacy of
CIK therapy in the treatment of NSCLC remains controversial
(17,31). The main reason for this controversy
is that there is no systematic, multi-center, convincing clinical
evidence to support the use of this therapy in NSCLC. Although
numerous studies have been performed to investigate CIK therapy of
NSCLC, the majority of the studies have focused mainly on
short-term survival and the adverse reactions (32–34).
Studies on the factors associated with clinical outcome of immune
therapy are lacking. In the present study, by evaluating the
predictive value of 29 whole blood or serum indicators, the aim was
to identify a predictive factor for the 5-year survival prognosis
of CIK cell therapy combined with chemotherapy in patients with
advanced NSCLC. The therapeutic effects of immunotherapy are
considered to be mainly dependent upon boosting the immune system
to exhibit anticancer activity.
In the present study, the percentage of
CD3+CD56+ lymphocytes in the CIK group
significantly increased when compared with that in the PBMC group
in the first and second cycles. This is consistent with the
findings of previous studies (35,36), and
demonstrated the expansion of CD3+CD56+
T-cells in populations of PBMCs in the present study. Albumin is
known as a negative acute-phase protein in inflammation (37). The reduction in albumin concentration
may be used as a biomarker of inflammation (38). In addition, malnutrition and cachexia
in cancer patients are current problems (39), associated with the host response to
tumor and anticancer therapies, and ultimately result in poor
survival (40). Serum albumin is a
useful indicator for estimating visceral protein function; in the
advanced stage of cancer, malnutrition and inflammation suppress
albumin synthesis (41). Lower
levels of serum albumin have been associated with poor survival
across numerous studies (42–45). In
the present study, it was revealed that the patients with high
expression levels of albumin had a relatively better prognosis when
compared with patients with low expression levels of albumin, which
is consistent with the previous studies. Serum albumin levels have
also been associated with autoimmune symptoms, and the appearance
of autoimmune symptoms may be a predictive indicator of better
survival and prognosis following cancer treatment (46). In patients with thyroid cancer, serum
thyroid auto-antibodies have been identified to be a positive
prognostic indicator (47). For
melanoma patients treated with IFN-α2b, autoimmune symptoms were
demonstrated to predict better overall survival rates (48,49).
These studies indicate that autoimmune symptoms may positively
correlate with the survival time of patients. Immune cell
infiltration by T helper 1 cells and cytotoxic T cells may also be
a promising prognostic indicator (50). MHC class I chain-related gene A
(MICA) protein was demonstrated to be a potential indicator of the
clinical outcome in patients with advanced NSCLC (20,51). In
addition, immunology score and tumor-associated antigens may
predict the outcome of immunotherapy (50,52).
Until now, the association between autoimmune symptoms and the
prognosis in patients with advanced NSCLC was unknown. The present
study revealed that albumin concentration may be an indicator of
the clinical outcome in patients with advanced NSCLC.
There are certain limitations to the present study.
First, the sample size was relatively small (the number of patients
was only 42) and following 2, 4, 6 and 8 cycles, the numbers of
matched patients were even fewer. This may create a bias in the
results, thus a greater number of patients are required in future
studies. Second, the present study was only performed in a single
center, and the results may be affected by the patients enrolled,
ages, gender, and so on. Multi-center validation should be
performed to provide more representative results. Third, the
present study is prospective; a retrospective study should be
performed to validate the results in this study. Fourth, due to
inconsistency of therapeutic standards between the present and
previous studies, standardization of the therapy process is
necessary to ensure comparability between studies. Lastly, any
other factors that may cause high expression of albumin should be
investigated. Further studies are required to evaluate the effect
of other factors on the prognosis in advanced NSCLC patients.
In conclusion, continuous evaluation of the
expression of albumin in serum in patients with advanced NSCLC may
help to predict the 5-year survival prognosis of the patients.
Patients with high expression levels of albumin may have a
relatively better prognosis compared with patients with low
expression levels of albumin. However, the expression of albumin
should be detected continuously in order to eliminate any other
factors that may cause abnormal increases in albumin levels. The
present study provides a potential prognostic indicator following
CIK cell therapy combined with chemotherapy in the treatment of
advanced NSCLC, and builds a theoretical basis for the personalized
treatment for patients with advanced NSCLC.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (nos. 31270820, 81230061),
National Basic Science and Development Program of China (no.
2012CB518103).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
She J, Yang P, Hong Q and Bai C: Lung
cancer in China: Challenges and interventions. Chest.
143:1117–1126. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Molina JR, Yang P, Cassivi SD, Schild SE
and Adjei AA: Non-small cell lung cancer: Epidemiology, risk
factors, treatment and survivorship. Mayo Clin Proc. 83:584–594.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Spiro SG, Tanner NT, Silvestri GA, Janes
SM, Lim E, Vansteenkiste JF and Pirker R: Lung cancer: Progress in
diagnosis, staging and therapy. Respirology. 15:44–50. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pallis AG, Serfass L, Dziadziusko R, van
Meerbeeck JP, Fennell D, Lacombe D, Welch J and Gridelli C:
Targeted therapies in the treatment of advanced/metastatic NSCLC.
Eur J Cancer. 45:2473–2487. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fridman WH, Pagès F, Sautès-Fridman C and
Galon J: The immune contexture in human tumours: Impact on clinical
outcome. Nat Rev Cancer. 12:298–306. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fischbach MA, Bluestone JA and Lim WA:
Cell-based therapeutics: The next pillar of medicine. Sci Transl
Med. 5:179ps72013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sangiolo D: Cytokine induced killer cells
as promising immunotherapy for solid tumors. J Cancer. 2:363–368.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lu PH and Negrin RS: A novel population of
expanded human CD3+CD56+ cells derived from T
cells with potent in vivo antitumor activity in mice with severe
combined immunodeficiency. J Immunol. 153:1687–1696.
1994.PubMed/NCBI
|
|
10
|
Jiang J, Wu C and Lu B: Cytokine-induced
killer cells promote antitumor immunity. J Transl Med. 11:832013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang FS, Liu MX, Zhang B, Shi M, Lei ZY,
Sun WB, Du QY and Chen JM: Antitumor activities of human autologous
cytokine-induced killer (CIK) cells against hepatocellular
carcinoma cells in vitro and in vivo. World J Gastroenterol.
8:464–468. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang L, Ren B, Li H, Yu J, Cao S, Hao X
and Ren X: Enhanced antitumor effects of DC-activated CIKs to
chemotherapy treatment in a single cohort of advanced
non-small-cell lung cancer patients. Cancer Immunol Immunother.
62:65–73. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gammaitoni L, Giraudo L, Leuci V,
Todorovic M, Mesiano G, Picciotto F, Pisacane A, Zaccagna A, Volpe
MG, Gallo S, et al: Effective activity of cytokine-induced killer
cells against autologous metastatic melanoma including cells with
stemness features. Clin Cancer Res. 19:4347–4358. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jakel CE, Vogt A, Gonzalez-Carmona MA and
Schmidt-Wolf IG: Clinical studies applying cytokine-induced killer
cells for the treatment of gastrointestinal tumors. J Immunol Res.
2014:8972142014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang Y, Wang J, Wang Y, Lu XC, Fan H, Liu
Y, Zhang Y, Feng KC, Zhang WY, Chen MX, et al: Autologous CIK cell
immunotherapy in patients with renal cell carcinoma after radical
nephrectomy. Clin Dev Immunol. 2013:1956912013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim JS, Chung IS, Lim SH, Park Y, Park MJ,
Kim JY, Kim YG, Hong JT, Kim Y and Han SB: Preclinical and clinical
studies on cytokine-induced killer cells for the treatment of renal
cell carcinoma. Arch Pharm Res. 37:559–566. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wu C, Jiang J, Shi L and Xu N: Prospective
study of chemotherapy in combination with cytokine-induced killer
cells in patients suffering from advanced non-small cell lung
cancer. Anticancer Res. 28:3997–4002. 2008.PubMed/NCBI
|
|
18
|
Shi SB, Ma TH, Li CH and Tang XY: Effect
of maintenance therapy with dendritic cells: Cytokine-induced
killer cells in patients with advanced non-small cell lung cancer.
Tumori. 98:314–319. 2012.PubMed/NCBI
|
|
19
|
Han RX, Liu X, Pan P, Jia YJ and Yu JC:
Effectiveness and safety of chemotherapy combined with dendritic
cells co-cultured with cytokine-induced killer cells in the
treatment of advanced non-small-cell lung cancer: A systematic
review and meta-analysis. PLoS One. 9:e1089582014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen Y, Lin G, Guo ZQ, Zhou ZF, He ZY and
Ye YB: Effects of MICA expression on the prognosis of advanced
non-small cell lung cancer and the efficacy of CIK therapy. PloS
One. 8:e690442013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Herbst RS, Soria JC, Kowanetz M, Fine GD,
Hamid O, Gordon MS, Sosman JA, McDermott DF, Powderly JD, Gettinger
SN, et al: Predictive correlates of response to the anti-PD-L1
antibody MPDL3280A in cancer patients. Nature. 515:563–567. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
González-Cao M: Immunotherapy for lung
cancer. Transl Lung Cancer Res. 4:675–677. 2015.PubMed/NCBI
|
|
23
|
Mahoney KM and Atkins MB: Prognostic and
predictive markers for the new immunotherapies. Oncology 28 Suppl.
3:39–48. 2014.
|
|
24
|
Wang Y, Dai H, Li H, Lv H, Wang T, Fu X
and Han W: Growth of human colorectal cancer SW1116 cells is
inhibited by cytokine-induced killer cells. Clin Dev Immunol.
2011:6214142011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gehrmann U, Hiltbrunner S, Georgoudaki AM,
Karlsson MC, Näslund TI and Gabrielsson S: Synergistic induction of
adaptive antitumor immunity by codelivery of antigen with
α-galactosylceramide on exosomes. Cancer Res. 73:3865–3876. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Belardelli F and Ferrantini M: Cytokines
as a link between innate and adaptive antitumor immunity. Trends
Immunol. 23:201–208. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Vivier E, Raulet DH, Moretta A, Caligiuri
MA, Zitvogel L, Lanier LL, Yokoyama WM and Ugolini S: Innate or
adaptive immunity? The example of natural killer cells. Science.
331:44–49. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wu F, Wang ZB, Lu P, Xu ZL, Chen WZ, Zhu H
and Jin CB: Activated anti-tumor immunity in cancer patients after
high intensity focused ultrasound ablation. Ultrasound Med Biol.
30:1217–1222. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ciernik IF, Berzofsky JA and Carbone DP:
Induction of cytotoxic T lymphocytes and antitumor immunity with
DNA vaccines expressing single T cell epitopes. J Immunol.
156:2369–2375. 1996.PubMed/NCBI
|
|
30
|
Kirkwood JM, Butterfield LH, Tarhini AA,
Zarour H, Kalinski P and Ferrone S: Immunotherapy of cancer in
2012. CA Cancer J Clin. 62:309–335. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li R, Wang C, Liu L, Du C, Cao S, Yu J,
Wang SE, Hao X, Ren X and Li H: Autologous cytokine-induced killer
cell immunotherapy in lung cancer: A phase II clinical study.
Cancer Immunol Immunother. 61:2125–2133. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Li DP, Li W, Feng J, Chen K and Tao M:
Adjuvant chemotherapy with sequential cytokine-induced killer (CIK)
cells in stage IB non-small cell lung cancer. Oncol Res. 22:67–74.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhong R, Han B and Zhong H: A prospective
study of the efficacy of a combination of autologous dendritic
cells, cytokine-induced killer cells, and chemotherapy in advanced
non-small cell lung cancer patients. Tumour Biol. 35:987–994. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhong R, Teng J, Han B and Zhong H:
Dendritic cells combining with cytokine-induced killer cells
synergize chemotherapy in patients with late-stage non-small cell
lung cancer. Cancer Immunol Immunother. 60:1497–1502. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li Y, Huang SL, Wu YF, Wei J, Bao R and
Zhou DH: Expansion of CIK/NK cells from cord blood by using
different combinations of stem cell factor, FLT3 ligand and
interleukin 2, 7, 15 in vitro. Zhongguo Shi Yan Xue Ye Xue Za Zhi.
12:350–354. 2004.(In Chinese). PubMed/NCBI
|
|
36
|
Li Y, Schmidt-Wolf IG, Wu YF, Huang SL,
Wei J, Fang J, Huang K and Zhou DH: Optimized protocols for
generation of cord blood-derived cytokine-induced killer/natural
killer cells. Anticancer Res. 30:3493–3499. 2010.PubMed/NCBI
|
|
37
|
Ritchie RF, Palomaki GE, Neveux LM,
Navolotskaia O, Ledue TB and Craig WY: Reference distributions for
the negative acute-phase serum protein–s, albumin, transferrin and
transthyretin: A practical, simple and clinically relevant approach
in a large cohort. J Clin Lab Anal. 13:273–279. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Don BR and Kaysen G: Serum albumin:
Relationship to inflammation and nutrition. Semin Dial. 17:432–437.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
von Meyenfeldt M: Cancer-associated
malnutrition: An introduction. Eur J Oncol Nurs. 9(Suppl 2):
S35–S38. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Gupta D and Lis CG: Pretreatment serum
albumin as a predictor of cancer survival: A systematic review of
the epidemiological literature. Nutr J. 9:692010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yeun JY and Kaysen GA: Factors influencing
serum albumin in dialysis patients. Am J Kidney Dis. 32(Suppl 4):
S118–S125. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Siddiqui A, Heinzerling J, Livingston EH
and Huerta S: Predictors of early mortality in veteran patients
with pancreatic cancer. Am J Surg. 194:362–366. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Onate-Ocana LF, Aiello-Crocifoglio V,
Gallardo-Rincón D, Herrera-Goepfert R, Brom-Valladares R, Carrillo
JF, Cervera E and Mohar-Betancourt A: Serum albumin as a
significant prognostic factor for patients with gastric carcinoma.
Ann Surg Oncol. 14:381–389. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Lis CG, Grutsch JF, Vashi PG and
Lammersfeld CA: Is serum albumin an independent predictor of
survival in patients with breast cancer? JPEN J Parenter Enteral
Nutr. 27:10–15. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Seve P, Ray-Coquard I, Trillet-Lenoir V,
Sawyer M, Hanson J, Broussolle C, Negrier S, Dumontet C and Mackey
JR: Low serum albumin levels and liver metastasis are powerful
prognostic markers for survival in patients with carcinomas of
unknown primary site. Cancer. 107:2698–2705. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Burkholder B, Huang RY, Burgess R, Luo S,
Jones VS, Zhang W, Lv ZQ, Gao CY, Wang BL, Zhang YM and Huang RP:
Tumor-induced perturbations of cytokines and immune cell networks.
Biochim Biophys Acta. 1845:182–201. 2014.PubMed/NCBI
|
|
47
|
Souza SL, Da Montalli Assumpção LV and
Ward LS: Impact of previous thyroid autoimmune diseases on
prognosis of patients with well-differentiated thyroid cancer.
Thyroid. 13:491–495. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Krauze MT, Tarhini A, Gogas H and Kirkwood
JM: Prognostic significance of autoimmunity during treatment of
melanoma with interferon. Semin Immunopathol. 33:385–391. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Weber J: Ipilimumab: Controversies in its
development, utility and autoimmune adverse events. Cancer Immunol
Immunother. 58:823–830. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Braumuller H, Wieder T, Brenner E, Aßmann
S, Hahn M, Alkhaled M, Schilbach K, Essmann F, Kneilling M,
Griessinger C, et al: T-helper-1-cell cytokines drive cancer into
senescence. Nature. 494:361–365. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Salih HR, Rammensee HG and Steinle A:
Cutting edge: Down-regulation of MICA on human tumors by
proteolytic shedding. J Immunol. 169:4098–4102. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Ascierto PA, Capone M, Urba WJ, Bifulco
CB, Botti G, Lugli A, Marincola FM, Ciliberto G, Galon J and Fox
BA: The additional facet of immunoscore: Immunoprofiling as a
possible predictive tool for cancer treatment. J Transl Med.
11:542013. View Article : Google Scholar : PubMed/NCBI
|