Introduction
Meningioma is the second most common primary brain
tumor, which accounts for 13–15% of all intracranial neoplasms
(1,2). Traditionally, it is classified by the
combination of two properties: The site of the tumor (for example,
convex meningioma, sphenoid crest meningioma or cerebellar
meningioma) and the pathological nature of the tumor (benign or
malignant meningioma). This classification provides accurate
localization of the tumor and enables the selection of the
appropriate surgical approach, in addition to allowing the
multidisciplinary management plan and the patient's prognosis to be
determined (3,4). In general, the pathological nature of
meningioma determines its association with the brain parenchyma,
which is that benign meningioma is usually compressive to the brain
parenchyma due to its expansive growth, and malignant meningioma is
invasive into the neighboring brain parenchyma due to its intrusive
growth (5,6). However, clinical observations have
indicated that there is a sub-group of benign meningioma displaying
a malignant growth pattern, that is, invasion into the neighboring
brain tissue (7–11). This sub-type of meningioma is usually
unnoticed prior to surgical resection by the neurosurgeon, which
can often result in damage of the neighboring brain tissue. To
improve our knowledge about this unique type of meningioma and
facilitate the preservation of the neighboring brain parenchyma, a
retrospective review of all the cases of invasive benign meningioma
in a single hospital during the past 6 years was conducted. This
review presents their clinical characteristics, the evolving
treatment strategies and the post-operative outcomes.
Materials and methods
From August 2005 to August 2010, there were 254
patients with meningioma who were treated surgically in Xuanwu
Hospital affiliated with Capital Medical University (Beijing,
China). Among these, there were 19 cases (7.4%) of invasive benign
meningioma. The clinical characteristics, magnetic resonance
imaging (MRI) findings, refined surgical strategies and outcomes
were summarized and analyzed. This retrospective study was approved
by the Ethics Committee of Xuanwu Hospital affiliated with Capital
Medical University. Written informed consent was obtained from each
patient.
The clinical characteristics, magnetic resonance
imaging (MRI) results, refined surgical strategies and outcomes
were summarized and analyzed. MRI data were acquired using a 1.5 T
Siemens Sonata scanner (Siemens Medical Solutions USA, Inc.,
Malvern, PA, USA). Standard neurological physical examination was
conducted to evaluate the overall function of the central nerve
system of the patients.
Results
Clinical and MRI characteristics
The mean age of the 19 patients with invasive benign
meningioma was 53 years (range, 40–72 years). This cohort consisted
of 9 male patients and 10 female patients. The initial symptoms at
diagnosis included decreased muscle power of a single extremity (7
cases), dysphasia accompanied by decreased muscle power of a single
extremity (9 cases) and decreased sensation of a single extremity
(3 cases). Notably, to some extent, there were certain common
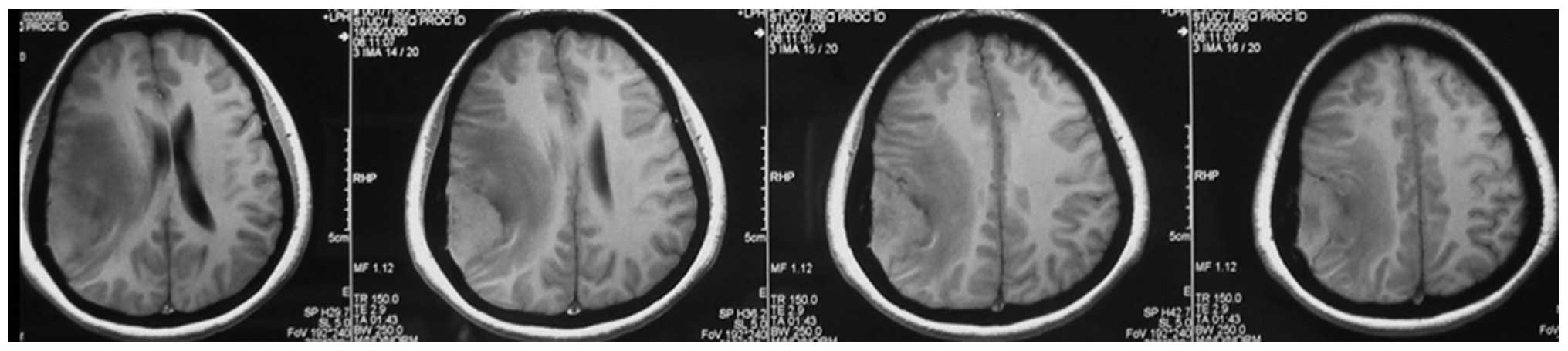
features shared by the MRI results of these patients. The
meningiomas were all located on the convexity of the cerebral
hemisphere and crossed the central lobe. On T1-weighted imaging
(Fig. 1), the meningiomas appeared
to exhibit iso- or hyperintense signals and grew along the dural
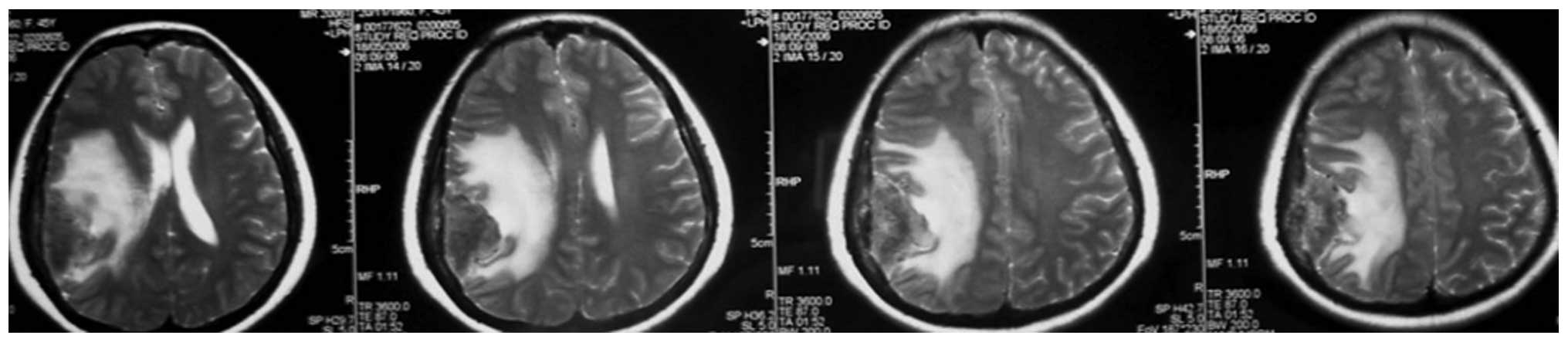
matter. On T2-weighted imaging (Fig.
2), there was absent or very narrow sub-arachnoid space between
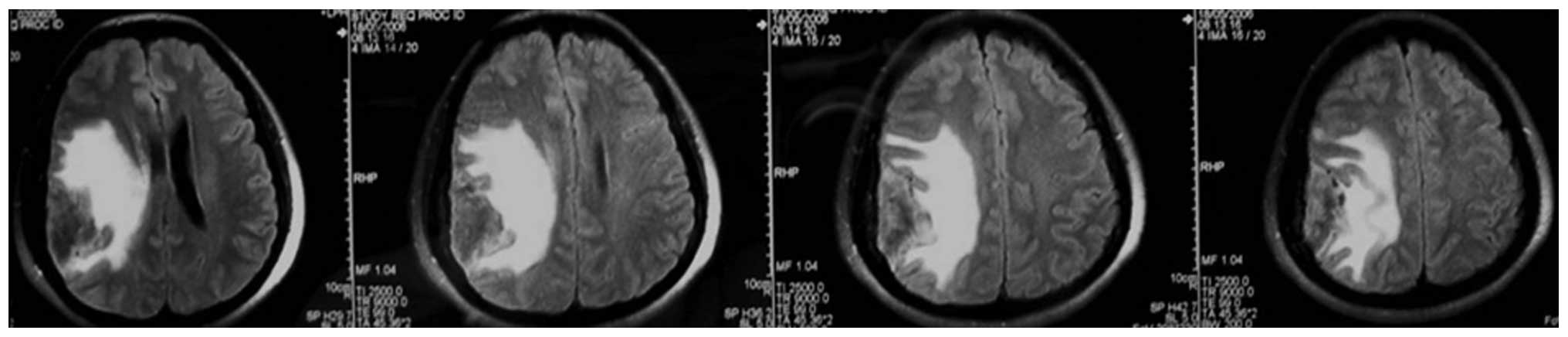
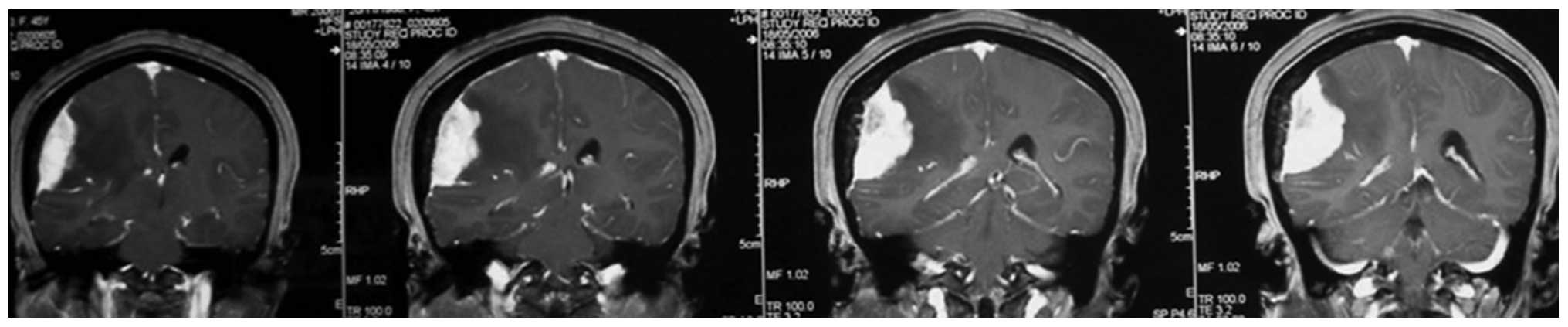
the meningioma and the adjacent brain parenchyma. Fluid-attenuated
inversion recovery imaging (Fig. 3)
confirmed the existence of severe edema surrounding the tumor. On
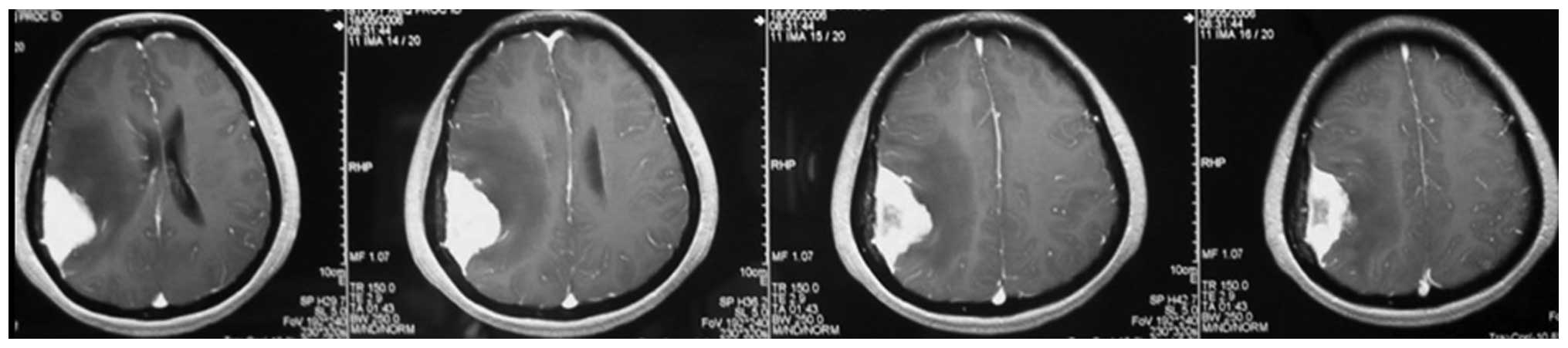
T1-weighted enhanced images (Figs. 4
and 5), firstly, these meningiomas
were flat in shape with extensive bases, accompanied by evident
‘tail signs’; secondly, at the apex of the meningiomas, the
boundary between the tumors and the adjacent brain parenchyma could
not be perceived clearly; thirdly, these meningiomas appeared to be
protruding into the neighboring brain tissue.
Surgical strategies and outcomes
Microsurgeries were performed to remove the
meningioma for all 19 cases. For all cases, the originating site of
the meningioma was coagulated and divided first. Following this,
for the earliest 4 cases, a traditional extra-capsular approach was
used, which involved separating the tumor from the brain parenchyma
along the arachnoid membrane. In two of these 4 cases, it was
observed that there were ‘cauliflower-like’ nodules on the surfaces
of the meningiomas, which enwrapped the normal brain tissues and
vessels. This surgical challenge was sometimes not possible to
overcome and the total removal of the meningioma could only be
achieved at the cost of the enwrapped normal brain tissue and
associated vessels. To improve the surgical removal, the strategy
was modified for the following 15 cases. Initially, the
intra-capsular extirpation of the central part of the meningioma
was conducted carefully, until the capsule wall of the tumor was
reached. Then, dissection of the tumor was continued according to
the classic extra-capsular method, which was along the interface
between the tumor and the brain parenchyma. In 11 of these 15
cases, the ‘cauliflower-like’ tumor nodules enwrapping the
neighboring normal cortex and associated vessels were also
encountered. These enwrapped brain structures could be much more
easily separated and spared by gentle dissection, which was greatly
facilitated by the removal of the bulk of the tumor. For all 19
cases, total removals were achieved and the pathologic results were
benign meningioma [World Health Organization (WHO) grade 1–2]. The
follow-up period was >6 months. For the earliest 4 cases, mild
but permanent neurological impairments were observed, which
included mild dysphasia (1 case), decreased muscle power of the
contralateral fingers (2 cases) and decreased sensation of the
contralateral palms (1 case). By contrast, for the other 15 cases,
there was only 1 case with permanent neurological impairment
(decreased sensation and muscle power of the contralateral
fingers).
Discussion
The traditional pathological classification of
meningioma consists of benign (WHO 1), atypical (WHO 2) and
anaplastic types (WHO 3) (12). In
general, benign meningioma grows expansively and compresses the
neighboring brain parenchyma while aggressive meningioma is
invasive. However, clinical practice has revealed that there is a
sub-group of meningioma with intermediate characteristics. These
meningiomas are benign in histology, but malignant in their growth
(13). This introduces the challenge
of total removal while ensuring the protection of neurological
functions. Previous studies have demonstrated the MRI features and
potential molecular biomarker for this sub-group of meningiomas
(13,14). However, there are no prior studies
describing the overall clinical features for these patients and
surgical strategy for the removal of these tumors.
According to the experience gained in these 19
cases, it was observed that there were certain features shared by
these invasive benign meningiomas. The peak age of onset was ~50
years; the main manifestation was mild focal neurological deficits,
which included dysphasia, and decreased sensation and muscle power
of the contralateral limb. The MRI findings usually had the
following characteristics: The lesions were located at the
convexity of the cerebral hemisphere involving the central lobe,
with an extensive base at the dural matter and evident ‘tail sign’;
there was a minimal boundary between the tumor and the neighboring
brain cortex; finally, and probably most importantly, the apex of
tumor often enwrapped the normal brain tissue and associated
vessels.
Due to the malignant growth, it was challenging to
completely remove this benign meningioma while ensuring that
neurological function remained intact. Resection of the earliest 4
cases was performed according to the traditional extra-capsular
strategy, which was to coagulate and divide the tumor base first,
and then continue the dissection along the interface between the
tumor and brain parenchyma. This approach inevitably damaged the
vessels transiting from and into the tumor. The observation that
all 4 cases had permanent neurological deficits confirmed the
disadvantage associated with this surgical strategy. Following
careful analysis of the surgical outcomes, the resection method was
modified by combining intra- and extra-capsular approaches. The
first step was the same as the classical method, which was to
coagulate and divide the tumor base. Afterwards, intra-capsular
extirpation of the central part of the tumor was performed. Care
was taken not to damage the transit vessels when approaching the
tumor-brain interface. The enucleation of the central part of the
tumor created a working space, which greatly facilitated the
identification of the transit vessels. After this, the tumor was
separated from brain parenchyma along the sub-arachnoid membrane.
The use of a sponge during this dissection process was important.
Finally, it was critical to separate the enwrapped brain cortex and
associated vessels from the invading ‘cauliflower-like’ nodules of
the meningioma. It is recommended that no efforts are spared in
this process, since the enwrapped brain tissue may have retained
its ability to function. The observation that there was only 1 case
with mild neurological impairment post-operatively in the later 15
cases confirms the advantage of the modified strategy.
In summary, the present study further revealed the
clinical features of the invasive benign meningioma and indicated
the advantage of combined intra-extra capsular strategy for the
surgical resection.
References
|
1
|
Wiemels J, Wrensch M and Claus EB:
Epidemiology and etiology of meningioma. J Neurooncol. 99:307–314.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Longstreth WT Jr, Dennis LK, McGuire VM,
Drangsholt MT and Koepsell TD: Epidemiology of intracranial
meningioma. Cancer. 72:639–648. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mawrin C and Perry A: Pathological
classification and molecular genetics of meningiomas. J Neurooncol.
99:379–391. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Scheithauer BW: Tumors of the meninges:
Proposed modifications of the World Health Organization
classification. Acta Neuropathol. 80:343–354. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Riemenschneider MJ, Perry A and
Reifenberger G: Histological classification and molecular genetics
of meningiomas. Lancet Neurol. 5:1045–1054. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Modha A and Gutin PH: Diagnosis and
treatment of atypical and anaplastic meningiomas: A review.
Neurosurgery. 57:538–550. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Trembath D, Miller CR and Perry A: Gray
zones in brain tumor classification: Evolving concepts. Adv Anat
Pathol. 15:287–297. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gay E, Lages E, Ramus C, Guttin A, El
Atifi M, Dupré I, Bouamrani A, Salon C, Ratel D, Wion D, et al: The
heterogeneity of meningioma revealed by multiparameter analysis:
Infiltrative and non-infiltrative clinical phenotypes. Int J Oncol.
38:1287–1297. 2011.PubMed/NCBI
|
|
9
|
Fritz J, Roser F, Tatagiba M and Bornemann
A: The basement membrane at the tumour-brain interface of
brain-invasive grade I meningiomas. Neuropathol Appl Neurobiol.
31:339–342. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Utsuki S, Oka H, Sato Y, Kawano N,
Tsuchiya B, Kobayashi I and Fujii K: Invasive meningioma is
associated with a low expression of E-cadherin and beta-catenin.
Clin Neuropathol. 24:8–12. 2005.PubMed/NCBI
|
|
11
|
Suwa T, Kawano N, Oka H, Ito H and Kameya
T: Invasive meningioma: A tumour with high proliferating and
‘recurrence’ potential. Acta Neurochir (Wien). 136:127–131. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Commins DL, Atkinson RD and Burnett ME:
Review of meningioma histopathology. Neurosurg Focus. 23:E32007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rempel SA, Ge S and Gutiérrez JA: SPARC: A
potential diagnostic marker of invasive meningiomas. Clin Cancer
Res. 5:237–241. 1999.PubMed/NCBI
|
|
14
|
Nakano T, Asano K, Miura H, Itoh S and
Suzuki S: Meningiomas with brain edema: Radiological
characteristics on MRI and review of the literature. Clin Imaging.
26:243–249. 2002. View Article : Google Scholar : PubMed/NCBI
|