Introduction
Diabetes is a serious global health issue and has
become one of the most common epidemics worldwide. The
International Diabetes Federation estimated that ~7% of the world's
population aged between 25 and 79 years of age had diabetes in
2010; by 2030 the figure will rise to 8% (1). Non-insulin dependent diabetes mellitus
is a leading cause of morbidity worldwide and contributes
significantly to premature mortality (2). Early-onset type 2 diabetes (EOD) has
emerged as an increasing public health problem, particularly in
developing areas such as Asia, which are undergoing rapid
socio-economic changes (3,4). A recent national investigation
completed in China showed that the prevalence of diabetes and
pre-diabetes in individuals aged 18–39 years was ~45% (5).
It is established insulin resistance and reduced
β-cell glucose sensitivity are present in patients with type 2
diabetes (6). Previously, the
concept that insulin resistance was the primary genetic component
of type 2 diabetes became widely believed (7); however, previous studies have indicated
that the first-phase insulin secretion is the earliest detectable
defect in β-cell function, and impaired β-cell function precedes
insulin resistance in the pathogenesis of type 2 diabetes (8,9).
Impaired β-cell function is regarded as a key factor in the
progression from glucose intolerance to overt type 2 diabetes, and
it could be the result of the loss of β-cell mass and/or functional
defects (10). Moreover, the
relative β-cell volume was decreased from ~20 to 50% in autopsy
specimens of patients with type 2 diabetes (11). These results suggested that diabetes
is associated with impaired β-cell function; however, the
development of β-cell hypofunction is poorly understood with
regards to type 2 diabetes.
In the present study, we evaluated the function and
deterioration of the islet β-cell in patients with type 2 diabetes
by using a 3-year follow-up and compared the difference between
late-onset diabetes (LOD) and EOD with the use of contrastive
analysis.
Materials and methods
Sample
Patients with type 2 diabetes were recruited from
the Department of Endocrinology of Huashan Hospital affiliated to
Fudan University (Shanghai, China) between 2003 and 2009. A total
of 48 patients (36 men and 12 women) with EOD (age at diagnosis,
<40 years) and 55 patients (27 men and 28 women) with LOD (age
at diagnosis, ≥40 years) were selected for the present study.
Plasma glucose concentrations were measured using an Abbott
Bichromatic Analyzer (Abbott Laboratories, Lake Bluff, IL, USA),
and diabetes was diagnosed according to the World Health
Organization plasma glucose criteria (fasting plasma glucose, ≥126
mg/dl; or 2-h plasma glucose, ≥200 mg/dl (12). In addition, anti-insular cellular
antibody (anti-ICA; cat. no. 02068), anti-glutamate decarboxylase
antibody (anti-GAD; cat. no. 020107) and anti-insulin antibody
(anti-IAA; cat. no. 02114A) all are negative. Patients were
excluded if they had type 1 diabetes as defined by acute
presentation with diabetic ketoacidosis, heavy ketonuria or
continuous requirement of insulin within half a year of diagnosis,
or unknown diabetes type. Disease course was no more than 5 years
in all subjects and all patients received oral blood glucose
lowering drugs based on alimentary control.
Ethical approval was obtained from Huashan Hospital
Clinical Research Ethics Committee. All patients provided written
informed consent for data analysis and research purpose at the time
of assessment.
Clinical studies
Participants underwent routine physical examinations
including the following measurements: Height, weight, waist
circumference, hip circumference and resting blood pressure. Height
was measured in meters (without shoes), and weight in kilograms
(without heavy clothing). Body mass index (BMI) was calculated in
kg/m2. Waist circumference was measured using a tape
measure while subjects were standing, at the midpoint between the
bottom of rip cage and the top of lateral border of iliac crests
during minimal respiration. Hip circumference was measured around
the maximal circumference of the buttocks, at approximately the
level of the pubic symphysis. Waist-hip ratio (WHR) was determined
by dividing the mean waist circumference by the mean hip
circumference. Systolic blood pressure (SBP) was measured with the
subject in the supine position following a 5-min rest.
After an overnight fast, venous blood was sampled
for measurement of plasma glucose, glycated hemoglobin A1c (HbA1c),
total cholesterol (TC), high-density lipoprotein cholesterol
(HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride
(TG), anti-ICA, anti-GAD and anti-IAA. All kits were purchased from
Youbo Biotechnoglgy Co., Ltd. (Shanghai, China).
Islet β-cell secretory activity was measured by
means of glucagon stimulation test (Express Technology Co., Ltd.,
Beijing, China). C-peptide (CPR0) levels were measured at fasting
state. Glucagon stimulation test was performed by intravenous
loading of 1 mg glucagon. The acute response to glucagon was
measured by the C-peptide levels 6 min after glucagon challenge
(CPR6).
BMI, HbA1c, CPR0 and CPR6 were measured at the
beginning of the experiment, and thereafter, these indexes were
examined once every year.
Biochemical assays and laboratory
analyses
Blood glucose and lipid levels were analyzed using
an automatic biochemical analyzer (AU5800; Beckman Coulter, Inc.,
Brea, CA, USA) according to the manufacturer's instructions. HbA1c
was determined using high-performance liquid chromatography
(Shimadzu Corporation, Kyoto, Japan). Blood glucose was measured by
a glucose oxidase method using a kit (DiaSys Diagnostic Systems
GmbH, Holzheim, Germany). HDL-C was measured by a direct method of
immunosuppression using a kit (DiaSys Diagnostic Systems GmbH).
LDL-C was measured by a direct measuring method using the a kit
(Sekisui Chemical, Co., Ltd., Osaka, Japan). TG and TC measurements
were performed using an enzymic kit (Beckman Coulter, Inc.).
C-peptide was assayed using a radio-immuno method (Shangsha Yike
Biotech Co., Ltd., Changsha, China).
Statistical analysis
Measurement data and non-normally distributed data
are expressed as the mean ± standard deviation and interquartile
range, respectively. All data were analyzed by use of
Kolmogorov-Smirnov normality test and if the data were not normally
distributed, a log transformation was performed on these data.
χ2 test and two sided t-tests were used for
comparison of enumeration and measurement data, respectively. The
correlation between islet β-cell function and various indexes were
analyzed using Pearson correlation analysis. All statistical
analyses were performed using SPSS software, version 17.0 (SPSS,
Inc., Chicago, IL, USA).
Results
Baseline general characteristics in
the EOD and LOD groups
At the baseline, subjects with EOD had lower levels
of SBP, DBP, BMI, CPR0, CPR6 and greater levels of HbA1c and TG
compared to subjects with LOD (all P<0.01) (Table I). Compared with the baseline, CPR0,
CPR6 and TG were decreased in the EOD and LOD groups at 12, 24 and
36 months (Table II).
 | Table I.Baseline general characteristics of
study participants. |
Table I.
Baseline general characteristics of
study participants.
| Characteristic | EOD | LOD |
|---|
| Gender
(male/female) |
36/12 |
27/28 |
| Age (years) | 35.44±5.11 |
59.96±8.50a |
| SBP (mmHg) | 118.35±15.44 |
136.18±21.21a |
| DBP (mmHg) | 78.33±9.65 |
84.47±10.42a |
| BMI
(kg/m2) | 23.31±2.93 |
25.17±2.99a |
| FBS (mmol/l) |
9.63±3.26 | 10.09±1.58 |
| HbA1c (%) | 10.88±2.32 |
9.83±1.46a |
| CPR0
(nmol/l)b |
1.1–2.10 |
1.98–3.46a |
| CPR6
(nmol/l)b |
2.00–4.20 |
5.29–7.48a |
| TC (mmol/l) |
4.53±0.99 |
5.15±1.15 |
| TG
(mmol/l)b |
1.31–3.57 |
1.00–2.30a |
| HDL
(mmol/l)b |
0.96–1.21 |
1.00–1.24 |
| LDL
(mmol/l)b |
1.83–3.46 |
2.22–3.71 |
| Table II.Clinical data of study participants
during the 3-year follow-up. |
Table II.
Clinical data of study participants
during the 3-year follow-up.
|
| EOD | LOD |
|---|
|
|
|
|
|---|
| Characteristic | Baseline | 12 month | 24 month | 36 month | Baseline | 12 month | 24 month | 36 month |
|---|
| BMI
(kg/m2) |
23.31±2.93 |
23.72±2.70 |
23.81±2.12 |
23.86±2.63 |
25.17±2.99 |
25.11±2.91 |
25.36±2.98 |
26.03±3.24 |
| HbA1c (%) |
10.88±2.32 |
9.01±2.09 |
8.49±1.67 |
8.39±1.67 |
9.83±1.46 |
8.93±1.32 |
8.38±1.37 |
8.29±1.31a |
| CPR0 (nmol/l) |
1.72±0.76 |
1.68±0.69 |
1.67±078 |
1.45±0.64 |
2.89±1.19 |
2.40±0.95 |
2.18±0.78 |
2.16±0.86a |
| CPR6 (nmol/l) |
2.96±1.67 |
2.84±1.30 |
2.71±0.93 |
2.44±0.84 |
6.66±2.43 |
5.61±1.30 |
4.85±1.22 |
5.20±1.56a |
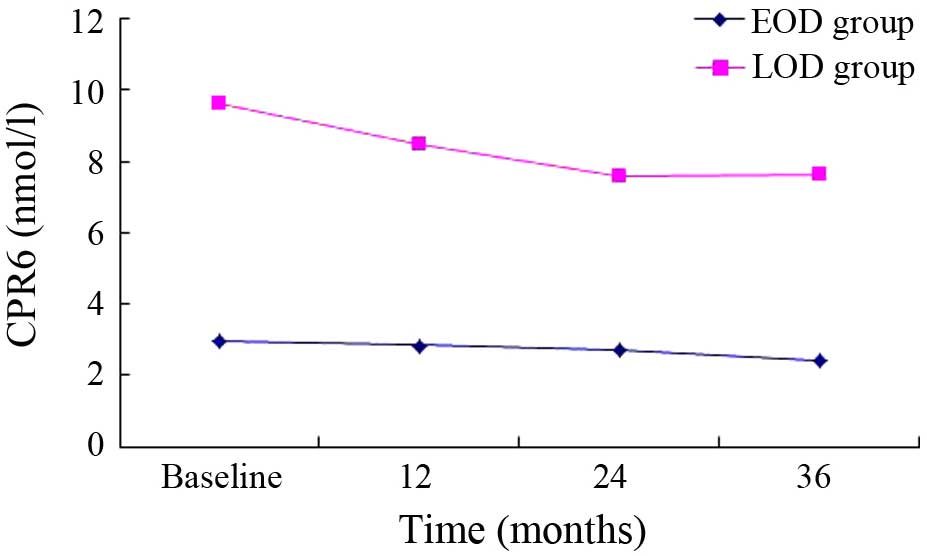
There was a decreasing trend in the EOD group
(Figs. 1–3). HbA1c, CPR0, CPR6 levels were
10.88±2.32, 1.72±0.76 and 2.96±1.67 nmol/l, respectively, when the
subjects were recruited, and these were decreased to 8.39±1.67,
1.45±0.64 and 2.44±0.84 nmol/l after 3 years. Compared with the
baseline, significant differences were detected in these indexes at
36 months (P<0.01). Furthermore, a decreasing trend was
similarly observed in the LOD group (Figs. 1–3).
At the baseline, HbA1c, CPR0 and CPR6 levels were 9.83±1.46,
2.89±1.19 and 6.66±2.43 nmol/l, respectively, which decreased to
8.29±1.31, 2.16±0.86 and 5.20±1.56 nmol/l after 3 years. Thus,
these indexes showed significant changes during the 3-year
follow-up (P<0.01).
Comparison of β-cell function failure
in the EOD and LOD groups
An >50% reduction in CPR0 or CPR6 was set as the
standard of β-cell function failure. A total of 14 subjects
(29.17%) in the EOD group and 6 subjects (10.91%) in the LOD group
were up to the >50% reduction standard 3 years later, and there
was significant difference between the two groups
(χ2=5.861, P<0.05) (Fig.
4).
Effect of WHR and BMI on CPR0 and
CPR6
Pearson correlation analysis indicated a positive
correlation between CPR0 and WHR (P<0.01), HbA1c (P<0.05) in
the EOD group after a 3-year follow-up. Furthermore, there was a
positive correlation between CPR0 and BMI (P<0.05) in the LOD
group.
Discussion
Type 2 diabetes (T2DM) is a complex population,
which possesses the characteristics of heterogeneity and
disuniformity (13). Previous
studies have suggested that following with the progressive
aggravation of insulin resistance, the islet β-cell function
declines gradually during the pathogenic course of type 2 diabetes
(14). However, numerous studies
using a variety of techniques have demonstrated that individuals
with impaired glucose tolerance or overt type 2 diabetes are
characterized by β-cell dysfunction independently of obesity and
insulin resistance (15,16). Using a glucose tolerance test, Elbein
et al have discovered that first-degree relatives of type 2
diabetic individuals with normal glucose tolerance already possess
the characteristic signs of β-cell dysfunction (17). Cnop et al have also reported
that in first-degree relatives of type 2 diabetic individuals, the
decline in glucose tolerance over time is strongly associated with
the loss of β-cell function (18).
Thus, early interventions to slow the decline in β-cell function
should be considered in high-risk individuals.
Insulin secretion includes two states, the basal
(postabsorptive) and stimulated (postprandial) states (19). The postabsorptive state predominates
during the interprandial phases and plays a key effect during the
period of overnight fast; the postprandial state regulates glucose
metabolism as carbohydrate is abundant and must be get rid of
(20). Under normal physiological
status, postprandial insulin secretion is biphasic and divided into
two phases, first-phase and second-phase insulin release (20). Early-phase insulin secretion contains
the first phase and part of the second-phase of insulin secretion.
Shen et al (21) have found
that early-phase insulin secretion is involved in preventing
hypernomic postprandial blood glucose and reducing plasma glucose
fluctuations.
As the glucagon stimulation test is widely used to
evaluate endogenous insulin secretion and shows good
reproducibility in the clinic, it is frequently employed to assess
β-cell function (22,23). The first measurable sign of β-cell
dysfunction that can be observed in type 1 and type 2 diabetes is a
defect in the first phase of insulin secretion (24). At 6 min after glucagon stimulation
insulin is rapidly secreted, reaching an initial peak value, and
this early phase of insulin release lasts no more than 10 min
(25). Furthermore, as the 6-min
C-peptide level response to 1 mg glucagon is significantly
correlated with the area under the curve of C-peptide levels, it is
used to assess the first phase of insulin secretion and the
residual pancreatic β-cell function (26).
In the present study, glucagon stimulation test (0
and 6 min C-peptide: CPR0 and CPR6) was used to evaluated the
β-cell function once a year during the 3-year follow-up in patients
with type 2 diabetes. The results suggested that the subjects with
EOD had lower BMI, SBP, DBP, CPR0, CPR6 and greater HbA1c and TG
compared to subjects with LOD. In the EOD patients, the islet
β-cell function declined and could not secrete sufficient insulin,
so the plasma glucose was not well controlled and the HbA1c level
increased. Hyperglycemia and blood lipid disorder play important
roles in the course of islet β-cell deterioration (27). Glucotoxicity and lipotoxicity induced
the progressive loss of β-cell function (28).
Currently, there are a number of hypotheses
regarding the possible mechanism underlying impaired β-cell
function (29). First, chronic
hyperglycemia has been shown to inhibit β-cell response, which has
been demonstrated both in vitro and in vivo (30). Exposure of β-cells to sustained
levels of hyperglycemia may deplete the insulin secretory granules
from the β-cell, leaving less insulin available for release in
response to further hyperglycemia (31). Lowering of glucose levels allows more
complete granulation of β-cells and thus improved acute insulin
responses (32). In addition, it has
been suggested that increased glucose levels activate the
hexosamine pathway and contribute to excess generation of reactive
oxygen species, resulting in the inhibition of insulin gene
transcription and insulin secretion (33).
Another potential cause of β-cell dysfunction is
lipotoxicity, accumulated fatty acids and their metabolic products
may have a negative effect on the conversion of proinsulin to
insulin, resulting in insulin deficiency (34). Additionally, Zhou and Grill has found
that continuous sustained exposure to free fatty acids reduces
insulin release in response to glucose by inhibiting glucose
oxidation in isolated rat islets (35). It has been shown that the accumulated
free fatty acids generated by the hydrolysis of TGs in the islets
can decrease an elevation in nitric oxide production, inducing
β-cell apoptosis (36). Previous
epidemiological studies have demonstrated that triglyceride level
is an independent determinant of cardiovascular risk, particularly
in association with coronary heart disease (37), and reducing the triglyceride level
may restrain atherosclerosis progression. The incidence rate of
cardiovascular risk in diabetes mellitus is >3 times compared
with the healthy population (38),
and the lipid disorder displays a significant effect on the
occurrence of macrovascular complications in diabetes mellitus
(39).
Compared with the baseline, a decline in islet
β-cell function was observed in the EOD and LOD groups over a
3-year follow-up, most notably in the EOD group. An >50%
reduction in CPR0 or CPR6 was as the threshold β-cell function
failure, and the ratio of β-cell function failure in the EOD group
was higher compared with the LOD group. These results suggested
that islet β-cell function deteriorated more rapidly in patients
with EOD compared with LOD. A correlation analysis indicated that
during the β-cell function decline, CPR0 showed a positive
association with BMI in the EOD group and with WHR and HbA1c in the
LOD group. These results suggest that progressive insulin
resistance may accelerate β-cell function failure. Furthermore, the
loss of insulin sensitivity contributed to adaptive increase in
insulin secretion.
The UK prospective diabetes study group (40) has reported that islet β-cell function
is reduced by 50% at the time of diagnosis, and a decreasing rate
of 5% every year is observed in patients with type 2 diabetes.
Along with the increasing age of the normal glucose tolerance
population, the islet β-cell function decreases at a rate of 0.5%
every year (41). van Haeften et
al (42) has reported that the
adaptivity of β-cell function to insulin sensitivity already
reaches the maximal degree and the β-cell function may decline in
patients with abnormal glucose tolerance. During the chronic
progression from normal glucose tolerance to overt diabetes, β-cell
function failure may be a more important factor than insulin
resistance (6).
Previous investigations have shown that lowering the
plasma glucose to near normal by intensive insulin therapy may
partially recover the β-cell function and insulin secretion
(43). Thus, this schema is
consistent with therapeutic interventions aimed at preserving
β-cell function/insulin secretion and at reducing the burden of
insulin resistance to prevent the cardiovascular disease in the
patients with EOD.
References
|
1
|
Shaw JE, Sicree RA and Zimmet PZ: Global
estimates of the prevalence of diabetes for 2010 and 2030. Diabetes
Res Clin Pract. 87:4–14. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kahn CR, Vicent D and Doria A: Type II
non-insulin-dependent diabetes mellitus. Annu Rev Med. 47:509–531.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chan JC, Cho NH, Tajima N and Shaw J:
Diabetes in the western pacific Region-past, present and future.
Diabetes Res Clin Pract. 103:244–255. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chan JC, Malik V, Jia W, Kadowaki T,
Yajnik CS, Yoon KH and Hu FB: Diabetes in Asia: Epidemiology, risk
factors and pathophysiology. JAMA. 301:2129–2140. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Xu Y, Wang L, He J, Bi Y, Li M, Wang T,
Wang L, Jiang Y, Dai M, Lu J, et al: Prevalence and control of
diabetes in Chinese adults. JAMA. 310:948–958. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ferrannini E, Gastaldelli A, Miyazaki Y,
Matsuda M, Mari A and DeFronzo RA: Beta-cell function in subjects
spanning the range from normal glucose tolerance to overt diabetes:
A new analysis. J Clin Endocrinol Metab. 90:493–500. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Warram JH, Martin BC, Krolewski AS,
Soeldner JS and Kahn CR: Slow glucose removal rate and
hyperinsulinemia precede the development of type II diabetes in the
offspring of diabetic parents. Ann Intern Med. 113:909–915. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khan S and Jena G: Valproic acid improves
glucose homeostasis by increasing Beta-Cell proliferation,
function, and reducing its apoptosis through HDAC inhibition in
Juvenile Diabetic Rat. J Biochem Mol Toxicol. Apr 15–2016.(Epub
ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
9
|
John E: Is reduced first-phase insulin
release the earliest detectable abnormality in individuals destined
to develop type 2 diabetes? Diabetes. 51:117–121. 2002. View Article : Google Scholar
|
|
10
|
Seghieri M, Rebelos E, Astiarraga BD,
Baldi S, Mari A and Ferrannini E: Impact of a mild decrease in
fasting plasma glucose on β-cell function in healthy subjects and
patients with type 2 diabetes. Am J Physiol Endocrinol Metab. Apr
12–2016.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Butler AE, Janson J, Bonner-Weir S, Ritzel
R, Rizza RA and Butler PC: β-cell deficit and increased β-cell
apoptosis in humans with type 2 diabetes. Diabetes. 1:102–110.
2003. View Article : Google Scholar
|
|
12
|
World Health Organization: WHO Expert
Committee on Diabetes Mellitus. Second report. World Health Organ
Tech Rep Ser. 646:1–80. 1980.PubMed/NCBI
|
|
13
|
McCoy RG, Van Houten HK, Ross JS, Montori
VM and Shah ND: HbA1c overtesting and overtreatment among US adults
with controlled type 2 diabetes, 2001–13: Observational population
based study. BMJ. 351:h61382015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gao W, Wang Q and Yu S: Efficacy, safety
and impact on β-cell function of dipeptidyl peptidase-4 inhibitors
plus metformin combination therapy in patients with type 2 diabetes
and the difference between Asians and Caucasians: A meta-analysis.
J Endocrinol Invest. Apr 12–2016.(Epub ahead of print). View Article : Google Scholar
|
|
15
|
Tura A, Mari A, Winzer C, Kautzky-Willer A
and Pacini G: Impaired beta-cell function in lean normotolerant
former gestational diabetic women. Eur J Clin Invest. 36:22–28.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mari A, Gastaldelli A, Natali A, Ostergard
T, Schmitz O and Ferrannini E: Characterization of beta-cell
function impairment in first-degree relatives of type 2 diabetic
subjects: Modeling analysis of 24-h triple-meal tests. Am J Physiol
Endocrinol Metab. 288:E541–E546. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Elbein SC, Hasstedt SJ, Wegner K and Kahn
SE: Heritability of pancreatic beta-cell function among nondiabetic
members of caucasian familial type 2 diabetic kindreds. J Clin
Endocrinol Metab. 84:1398–1403. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cnop M, Vidal J, Hull RL, Utzschneider KM,
Carr DB, Schraw T, Scherer PE, Boyko EJ, Fujimoto WY and Kahn SE:
Progressive loss of beta-cell function leads to worsening glucose
tolerance in first-degree relatives of subjects with type 2
diabetes. Diabetes Care. 30:677–682. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Malin SK, Samat A, Wolski K, Abood B,
Pothier CE, Bhatt DL, Nissen S, Brethauer SA, Schauer PR, Kirwan JP
and Kashyap SR: Improved acylated ghrelin suppression at 2 years in
obese patients with type 2 diabetes: Effects of bariatric surgery
vs standard medical therapy. Int J Obes (Lond). 38:364–370. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Del Prato S, Marchetti P and Bonadonna RC:
Phasic insulin release and metabolic regulation in type 2 diabetes.
Diabetes. 51(Suppl 1): S109–S116. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shen J, Chen Z, Chen C, Zhu X and Han Y:
Impact of incretin on early-phase insulin secretion and glucose
excursion. Endocrine. 44:403–410. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Scheen AJ, Castillo MJ and Lefèbvre PJ:
Assessment of residual insulin secretion in diabetic patients using
the intravenous glucagon stimulatory test: Methodological aspects
and clinical applications. Diabetes Metab. 22:397–406.
1996.PubMed/NCBI
|
|
23
|
Kondo Y, Satoh S, Nagakura J, Kimura M,
Nezu U and Terauchi Y: Defining criteria for the introduction of
liraglutide using the glucagon stimulation test in patients with
type 2 diabetes. J Diabetes. 4:571–575. 2013.
|
|
24
|
Ovalle F and Bell DS: Effect of
rosiglitazone versus insulin on the pancreatic beta-cell function
of subjects with type 2 diabetes. Diabetes Care. 27:2585–2589.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Del Prato S: Loss of early insulin
secretion leads to postprandial hyperglycaemia. Diabetologia.
46(Suppl 1): M2–M8. 2003.PubMed/NCBI
|
|
26
|
Bellin MD, Beilman GJ, Dunn TB, Pruett TL,
Chinnakotla S, Wilhelm JJ, Ngo A, Radosevich DM, Freeman ML,
Schwarzenberg SJ, et al: Islet autotransplantation to preserve beta
cell mass in selected patients with chronic pancreatitis and
diabetes mellitus undergoing total pancreatectomy. Pancreas.
42:317–321. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Doliba NM, Liu Q, Li C, Chen J, Chen P,
Liu C, Frederick DW, Baur JA, Bennett MJ, Naji A and Matschinsky
FM: Accumulation of 3-hydroxytetradecenoic acid: Cause or corollary
of glucolipotoxic impairment of pancreatic β-cell bioenergetics?
Mol Metab. 4:926–939. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Poitout V and Robertson RP:
Glucolipotoxicity: Fuel excess and beta-cell dysfunction. Endocr
Rev. 29:351–366. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Buchanan TA: Pancreatic beta-cell loss and
preservation in type 2 diabetes. Clin Ther. 25:B32–B46. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Leahy JL, Bonner-Weir S and Weir GC:
Beta-cell dysfunction induced by chronic hyperglycemia. Current
ideas on mechanism of impaired glucose-induced insulin secretion.
Diabetes Care. 15:4442–4455. 1992. View Article : Google Scholar
|
|
31
|
Khattab HA, El-Shitany NA, Abdallah IZ,
Yousef FM and Alkreathy HM: Antihyperglycemic potential of grewia
asiatica fruit extract against Streptozotocin-induced hyperglycemia
in rats: Anti-inflammatory and antioxidant mechanisms. Oxid Med
Cell Longev. 2015:5497432015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
van de Bunt M, Manning Fox JE, Dai X,
Barrett A, Grey C, Li L, Bennett AJ, Johnson PR, Rajotte RV,
Gaulton KJ, et al: Transcript expression data from human islets
links regulatory signals from genome-wide association studies for
type 2 diabetes and glycemic traits to their downstream effectors.
PLoS Genet. 11:e10056942015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kaneto H, Xu G, Song KH, Suzuma K,
Bonner-Weir S, Sharma A and Weir GC: Activation of the hexosamine
pathway leads to deterioration of pancreatic beta-cell function
through the induction of oxidative stress. J Biol Chem.
276:31099–31104. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhou YP and Grill V: Long-term exposure to
fatty acids and ketones inhibits B-cell functions in human
pancreatic islets of Langerhans. J Clin Endocrinol Metab.
80:1584–1590. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhou YP and Grill VE: Long-term exposure
of rat pancreatic islets to fatty acids inhibits glucose-induced
insulin secretion and biosynthesis through a glucose fatty acid
cycle. J Clin Invest. 93:870–876. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jeanne H and Edward S: Beta-cell failure
in the pathogenesis of type 2 diabetes mellitus. Curr Diab Rep.
4:169–175. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Patel A, Barzi F, Jamrozik K, Lam TH,
Ueshima H, Whitlock G and Woodward M: Asia Pacific Cohort Studies
Collaboration: Serum triglycerides as a risk factor for
cardiovascular diseases in the Asia-Pacific region. Circulation.
110:2678–2686. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Taskinen MR: Type 2 diabetes as a lipid
disorder. Curr Mol Med. 5:297–308. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Aldebasi YH, Mohieldein AH, Almansour YS
and Almutairi BL: Dyslipidemia and lipid peroxidation of Saudi type
2 diabetics with proliferative retinopathy. Saudi Med J.
34:616–622. 2013.PubMed/NCBI
|
|
40
|
No authors listed: U.K. prospective
diabetes study 16: Overview of 6 years' therapy of type II
diabetes: A progressive disease. U.K. Prospective diabetes study
group. Diabetes. 44:1249–1258. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Iozzo P, Beck-Nielsen H, Laakso M, Smith
U, Yki-Järvinen H and Ferrannini E: Independent influence of age on
basal insulin secretion in nondiabetic humans. European group for
the study of insulin resistance. J Clin Endocrinol Metab.
84:863–868. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
van Haeften TW, Pimenta W, Mitrakou A,
Korytkowski M, Jenssen T, Yki-Jarvinen H and Gerich JE: Relative
contributions of beta-cell function and tissue insulin sensitivity
to fasting and postglucose-load glycemia. Metabolism. 49:1318–1325.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kishikawa H, Araki E, Wake N and Shichiri
M: Intensive insulin therapy to prevent the progression of chronic
vascular complications in type 2 diabetes mellitus. Nippon Rinsho.
60(Suppl 9): 140–145. 2002.(In Japanese). PubMed/NCBI
|