Introduction
Neurogenic pulmonary edema (NPE) is characterized by
abruptly increased pulmonary interstitial and alveolar fluid
following central nervous system (CNS) events, including traumatic
brain injury (TBI), subarachnoid hemorrhage (SAH) or spinal cord
injury (1). It is a relatively rare
clinical syndrome with high mortality, and is frequently
misdiagnosed due to its unspecific clinical presentation. TBI
contributes to the majority of injury-associated mortality and
permanent disability cases worldwide (2), with the incidence of such cases
reported to be ~20% in patients with TBI (3). However, the incidence of NPE has
reportedly increased to 50% (4) in
patients succumbing within 96 h after suffering TBI, rendering NPE
a life threatening complication in these patients.
The clinical manifestations of NPE are almost
identical to those of acute respiratory distress syndrome and
cardiogenic pulmonary edema, posing a great challenge for timely
differential diagnosis and correct treatment decision in TBI
patients (1). Although the
underlying pathogenesis of NPE is poorly understood, it has been
suggested that, on the basis of increased intracranial pressure,
factors including direct cardiac injury, systemic sympathetic
discharge, pulmonary vascular permeability and pulmonary venule
adrenergic hypersensitivity may serve an essential role in NPE
development (1,5). These postulated mechanisms may alone or
synergically drive the development of NPE, suggesting that the
actual pathophysiological alteration may be complicated and that
appropriate monitoring is required. Since neurohemodynamic
interaction serves a central role in the development of NPE,
theoretically, hemodynamic monitoring would contribute to the
evaluation of the patient's condition (5). Detection of global end diastolic volume
index (GEDVI), intrathoracic blood volume index (ITBVI) and
extravascular lung water (EVLWI) through an advanced transpulmonary
thermodilution device is known as the pulse index continuous
cardiac output (PiCCO) (6). This
method allows the differentiation between permeability and
hydrostatic pulmonary edema, and the guidance of fluid management
(6). PiCCO has also shown favorable
agreement with pulmonary artery catheterization (PAC) in monitoring
cardiac output (7), making it a
promising strategy for handling the cardiac involvement in NPE.
However, to the best of our knowledge, only one previous study has
utilized this novel method for guiding the management of NPE
(6).
Specific treatments, such as α-adrenergic blocking
agents for underlying neurological insult, have been occasionally
administered in patients with NPE (8). However, an α-adrenergic blocking agent
can not be used in the case of systemic hypotension, thus an
alternative treatment is required. Levosimendan, a novel positive
inotropic agent, has been recommended for the treatment of acute
heart failure in the European Society of Cardiology guidelines
(9). In addition, a previous study
unveiled the vasorelaxation ability of levosimendan on pulmonary
vessels (10), suggesting that it
can be used to alleviate pulmonary edema by directly reducing the
hydrostatic pressure. However, its role in the management of NPE
has not been investigated.
In the current study, a TBI case with NPE diagnosed
when performing lumbar cistern drainage was reported. PiCCO
monitoring was applied, and showed a favorable ability to interpret
the pathophysiological progression and provide compelling
assistance for the diagnosis and treatment of this complication. To
the best of our knowledge, the present study was the first to
report the use of levosimendan to improve cardiac output, and
demonstrated a potential neuroprotective effect in the treatment of
NPE.
Case report
The present case was approved by the Ethics
Committee of the Second Affiliated Hospital, Zhejiang University
School of Medicine (Hangzhou, China). Written informed consent was
obtained from the patient for the publication of this
manuscript.
A 67-year-old male patient was transferred to the
General Intensive Care Unit (ICU) of the Second Affiliated
Hospital, Zhejiang University School of Medicine (Hangzhou, China)
in November 2014, 4 days after falling from a height of 2 meters.
The patient was diagnosed with multiple injuries with severe TBI,
spleen contusion, clavicle and multiple rib fractures at a local
hospital. Upon initial admission, emergency decompressive
craniectomy and hematoma removal were performed initially when
progressive intracranial hypertension was suspected. A second
craniotomy was performed due to increased volume of drain output on
the same day. Other treatments including respiration support,
antibiotics and fluid administration were also administrated. The
patient had no medical history other than administration of
amlodipine due to hypertension for 5 years.
During the admission in our ICU, the patient was
unconscious with Glasgow Coma Scale (GCS) score (11) of 3 (E1VTM1), with possible scores
ranging from 3–15; GCS scores of 3–8, 9–12 and 13–15 indicate
severe, moderate and mild brain injury respectively. The patient's
body temperature, pulse rate, blood pressure and respiratory rate
were 38°C, 88 beat per minute (bpm), 124/67 mmHg and 18 count per
minute (cpm), respectively. Physical examination revealed wheezing
rales of bilateral lungs upon auscultation. A head computed
tomography (CT) scan showed bilateral frontal lobe and right
temporal lobe contusion and laceration, subdural hematoma and SAH
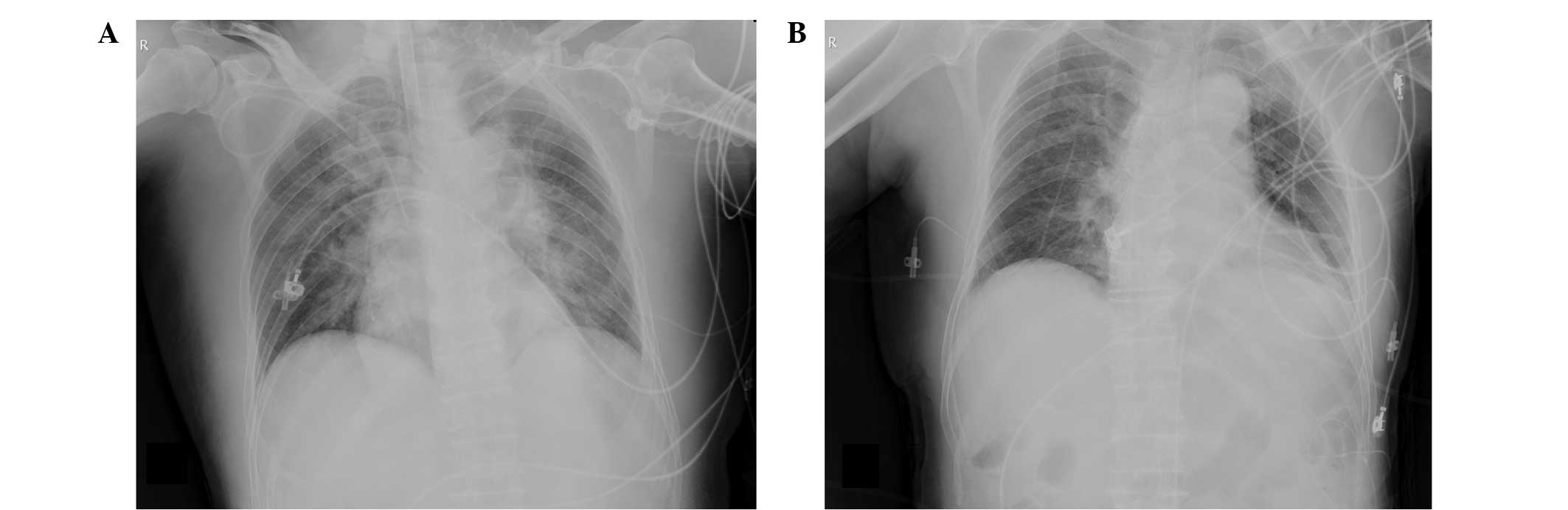
with post decompressive craniectomy presentation (Fig. 1). In addition, a chest X-ray scan
indicated board bilateral infiltrates, consolidation and pleural
effusion (Fig. 2A). Subsequently,
pulmonary infection was confirmed based on the findings of further
laboratory tests, including elevated percentage of neutrophils
(91.2%; normal range, 50–70%) in complete blood counting,
C-reactive protein (patient level, 92.6 mg/l; normal range, 0–8
mg/l) and serum procalcitonin (PCT; patient level, 4.2 ng/ml;
normal range, 0–0.05 ng/ml). Subsequently, cefoperazone/sulbactam
(Pfizer, Inc., New York, NY, USA) was intravenously administered
every 8 hours from days 1–3 as treatment for the pulmonary
infection, and 20% mannitol (100 ml; Baxter Healthcare Co., Ltd.,
Shanghai, China) was intravenously infused every 8 h from days 1–11
post-admission, in order to reduce intracranial pressure. The
patient remained hemodynamically stable and moderate improvement of
the neurological status (GCS score, 5; E2VTM2) was observed over
the next few days.
On day 7 of hospitalization, a lumbar puncture
revealed substantially elevated intracranial pressure (ICP; >300
mmH2O; normal range, 70–200 mmH2O), although
relevant therapies including decompressive craniectomy and
osmotherapy were adequately provided. Therefore, the patient was
subjected to lumbar cistern drainage. The condition of the patient
was generally stable prior to the surgery, with a pulse rate, blood
pressure, and respiratory rate of 94 bpm, 123/78 mmHg and 22 cpm,
respectively. His arterial blood peripheral oxygen saturation
(SpO2) was maintained at 100% under ventilation support
of 40% fraction of inspired oxygen (FiO2) and 5
cmH2O positive end-expiratory pressure (PEEP). However,
at the end of the procedure, the patient suffered sudden profuse
sweating, tachypnea (25–35 cpm), tachycardia (140–90 bpm), systemic
hypertension (160–200/90–120 mmHg) and decreasing SpO2
(85–95%). Pink frothy sputum was observed upon airway aspiration,
while board bilateral crackles and rales were detected upon
auscultation. The diagnosis of acute left heart failure and
cardiogenic pulmonary edema was initially suspected, and thus 5 mg
midazolam (Jiangsu Nhwa Pharmaceutical Co., Ltd., Xuzhou, China),
40 mg furosemide (Kingyork, Tianjin, China), 40 mg
methylprednisolone (Pfizer, Inc.) and 10 mg morphine (Northeast
Pharmaceutical Group Co., Ltd., Shenyang, China) were intravenously
injected following the lumbar drainage procedure, and adjustment of
ventilation parameters was performed (IPPV mode; FiO2,
100%; PEEP, 15 cmH2O; pressure support, 30
cmH2O; tidal volume, 600–700 ml; respiratory rate, 20
cpm). After 30 min, the vital signs gradually became relatively
stable, with a pulse rate of 102 bpm, blood pressure of 120/68
mmHg, respiratory rate of 30 cpm and SpO2 of 95–98%;
thus, the patient was transferred back to the general ICU.
In the ICU, the symptoms of tachypnea (32 cpm) and
tachycardia (122 bpm) remained, but hypotension (85/45 mmHg) was
newly developed. Symptoms of hypovolemia, including cold limbs,
cyanosis of the lips and oliguria, were subsequently observed, and
thus norepinephrine (Grand Pharmaceutical Co. Ltd., Wuhan, China)
was administered intravenously at 0.05 µg/kg/min with an increment
of 0.05 µg/kg/min when the blood pressure was below 90/60 mmHg for
a total of 13 h. Arterial blood gas measurement showed a pH of
7.299, CO2 partial pressure of 46.2 mmHg (normal range,
36–44), O2 partial pressure of 98.5 mmHg (normal range,
75–95), blood base excess of −3.7 mmol/l and oxygen saturation of
98.5%, while receiving 100% of FiO2. Elevated levels of
serum markers were also detected, including brain natriuretic
peptide (BNP) of 3,438.60 pg/ml (normal range, 2–4 pg/ml),
myocardial enzyme (troponin I) of 0.935 ng/ml (normal range,
<0.1 ng/ml) and C-reactive protein (CRP) of 221.9 mg/l. On the
same day, chest X-ray imaging showed typical signs of pulmonary
edema (Fig. 2B).
In order to further clarify the pathogenesis of
pulmonary edema, PiCCO monitoring by transpulmonary thermodilution
technique was performed (day 7). The initial PiCCO measurements
revealed elevated GEDVI of 860 ml/m2 (normal range,
680–800 ml/m2), EVLWI of 12 ml/kg (normal range, 3–7
ml/kg), and mild reduced cardiac index (CI) of 2.84
l/min/m2 (normal range, 3.0–5.0 l/min/m2)
combined with normal pulmonary vascular permeability index (PVPI)
of 1.4 (normal range, 1–3). Thus, the diagnosis of hydrostatic-type
pulmonary edema was established. Bedside two-dimensional
echocardiography excluded marked left ventricular dysfunction [left
ventricle ejection fraction (EF), 50%; normal range, 50–70%] or
left abnormal ventricular wall motion, thus eliminating the
possibility of cardiogenic pulmonary edema. A diagnosis of NPE was
finally established based on the aforementioned findings.
Goal-directed therapy guided with PiCCO was selected
for the subsequent treatment of NPE. Fluid administration was
restricted and a low dose of furosemide at 0.5 µg/kg/min was
administered intravenously for 10 h to achieve negative fluid
balance until the EVLWI and GEDVI values reduced to the normal
level. Methylprednisolone (40 mg, once daily, intravenously) was
used to further relieve edema (day 7–8). A reduction in heart rate
(70–80 bpm) and respiratory rate (12–16 cpm) along with an
elevation of the mean arterial pressure (83–101 mmHg) was observed,
and thus a reduction of FiO2 to 40% and of
norepinephrine infusion to the initial dosage (0.05 µg/kg/min) was
performed, without affecting the blood oxygen saturation. On day 8,
PiCCO demonstrated normalized EVLWI at 7 ml/kg and GEDVI at 723
ml/m2. However, a reduced CI (2.08 l/min/m2)
was still observed, whereas the stroke volume variation (SVV) was
within the normal range, indicating inadequate cardiac reserve. On
day 8, levosimendan, an inotropic agent, was also administered
intravenously for 24 h to improve the cardiac output, with a
maintenance dose of 0.14 µg/kg/min (Qilu Pharmaceutical Co., Ltd.,
Jinan, China) subsequent to termination of norepinephrine
administration, due to the patient's blood pressure stabilizing. An
elevated CI of 2.79–4.06 l/min/m2 was then determined by
PiCCO monitoring during levosimendan administration, and was
returned to similar levels thereafter. Repeated bedside
echocardiography examinations also confirmed the improvement of
left ventricular systolic function (EF, 65%). PiCCO monitoring
continued for a total of 6 days after admission, and the patient
remained hemodynamically stable (Fig.
3).
On day 8 of hospitalization, a repeat chest X-ray
scan revealed the complete disappearance of pulmonary edema signs
(Fig. 4A). The patient regained
consciousness with intermittent confusion on the day 11 of
hospitalization (GCS score, 10; E3VTM6). Subsequently, the patient
recovered rapidly and mechanical ventilation was ceased on the day
13 after admission. On day 16, a chest X-ray scan revealed evident
improvement of lung infiltrates (Fig.
4B), along with marked reduction of serum inflammatory and
cardiac biomarkers (CRP, 41.9 mg/l; PCT, 1.67 ng/ml; BNP, 778.8
pg/ml), and thus the antibiotic therapy was stopped. On day 22
after admission, a repeat head CT scan revealed significantly
absorbed hematoma and reduced brain swelling (Fig. 5). The patient recovered uneventfully
and was transferred to a rehabilitation center at 27 days after
admission.
In the rehabilitation center, the patient
predominantly received exercise rehabilitation. One month later,
the patient regained almost complete consciousness, and ws able to
walk short distances. The patient was discharged from the
rehabilitation center in December 2014, requiring no additional
tests or treatment. At follow-up in June 2015, the patient had
recovered other than occasional confusion, and required no
medication other than hypertensive drugs.
Discussion
Secondary pathophysiological changes following TBI,
including alteration of cerebral blood flow, impairment of
cerebrovascular autoregulation and edema formation, contribute to
the elevation of ICP (12). Elevated
ICP is believed to form the basis of NPE, and results in
neurological compression, ischemia and disruption of the ‘trigger
zone’, known as the A1 and A5 groups of neurons, nuclei of the
solitary tract, the area postrema, the medial reticulated nucleus
and the dorsal motor vagus nucleus in the medulla oblongata
(1,5). There are generally two types of NPE:
The ‘early’ form develops within minutes to hours following the
injury, whereas the ‘late’ form develops 12–24 h after the injury
(1,5). In the case reported in the present
study, the patient developed NPE during lumbar cistern drainage
when significant increasing of ICP was detected. The possible
explanation for this late outbreak of NPE (10 days after the
initial TBI) may be that, after surviving the edema peak (usually
3–7 days post-TBI), the balance among cerebral blood flow, cerebral
perfusion pressure and metabolism was restored; however, lumbar
cistern drainage due to elevated ICP may cause the sudden
alteration to ICP, possibly disturbing the newly established
balance, inducing another brain injury and resulting in the
outbreak of NPE.
Although the exact pathophysiological process
remains unclear, sympathetic surge or ‘catecholamine storm’ is
considered to be the primary mechanism of NPE (1,5).
Evidence from animal models revealed that elevated heart rate, and
systemic and pulmonary hypertension upon CNS injury indicated a
rapid activation of the sympathetic nervous system (13,14). In
patients with a clinical diagnosis of NPE, levels of serum
catecholamine were consistently raised soon after the outbreak of
the syndrome and paralleled with the alleviation of the condition
(6,8). The proposed pathogenesis of NPE induced
by sympathetic surge includes hemodynamic disturbance, elevated
pulmonary endothelial permeability, (so called ‘blast theory’) and
direct cardiac injury (1,5). These mechanisms alone or in
combination, as observed in cases of NPE with Takotsubo's
cardiomyopathy (15–17), give rise to the hydrostatic or
permeable types of pulmonary edema, thus posing a substantial
challenge for the timely recognition and management of this
syndrome. In a previous case of postoperative NPE, Merenkov et
al (18) reported that on-site
bedside lung ultrasound was able to identify pulmonary edema,
exclude cardiac involvement and guide serial fluid management.
However, lung sonography testing cannot quantitatively measure the
EVLWI, which is considered as the most sensitive and accurate
parameter for accessing pulmonary edema (19–21).
EVLWI was also shown to be closely co-associated with the ICP level
in NPE (22), rendering it a
reliable parameter for the precise fluid and ICP management. The
newly developed PiCCO monitoring system, based on the
thermodilution technique, is extensively used for the assessment of
EVLWI and the estimation of intrathoracic volumes (GEDV and ITBV).
PiCCO has also been proven to show favorable accordance for
measuring cardiac output with the traditional ‘gold standard’
measurement by PAC in various groups of patients (7,23,24), and
to be less invasive. Mutoh et al (6) demonstrated that, with combination of
PVPI, GEDV and cardiac output monitoring, PiCCO was able to
differentiate between the hydrostatic and permeable types of
pulmonary edema in three NPE cases with aneurismal SAH. In the
present study, the patient initially presented with systemic
hypertension, increased heart rate and tachypnea during lumbar
cistern drainage, indicating a burst of sympathetic activation.
Following treatment with intravenous diuretics and morphine and
adjusting ventilation parameters under consideration of acute heart
failure, the patient developed hypotension and symptoms of
hypovolemia, including cold limbs, cyanosis of lips and oliguria.
At that time, PiCCO monitoring was decided to assist in reaching
the appropriate diagnosing and in further management. The elevated
GEDVI and EVLWI, normal PVPI, exclusion of major cardiac systolic
dysfunction or abnormal wall motion with bedside echocardiography,
the absence of excessive fluid administration and no history of
heart disease suggested a non-cardiac origin of hydrostatic
pulmonary edema. NPE was the most likely etiology in the current
patient. However, myocardial injury represented by mild decreased
CI and elevated cardiac enzyme (troponin I) and BNP levels, was
likely to contribute to systemic hypotension and aggravation of
hydrostatic edema. In a previous small sample study, all the NPE
cases resulting from TBI were found to present cardiac dysfunction
(25). The reversible myocardial
dysfunction may be caused by direct catecholamine cardiotoxicity or
indirect abruptly elevated afterload. Biomarkers such as BNP alone
for cardiac pulmonary edema identification and prognosis prediction
can be interfered by various factors, including hypovolemia
(26) and abnormal BNP released from
the injured CNS lesion (27).
However, BNP levels appeared to be associated with the disease
status evolution in the present study patient, possibly due to a
certain degree of cardiac involvement.
To date, ventilation with PEEP and ICP reduction has
been proven to be the most effective modality in handling NPE
(28,29). However, a specific treatment protocol
has not been developed. Regarding the heterogeneous hemodynamic
presentation of NPE due to the predominance of specific underlying
pathophysiological changes (1,5), an
individualized treatment decision, including fluid management, the
use of inotropic and vasoactive agents, is urgently required
(1,28–30).
These treatments constantly interfere with each other in managing
TBI patients with NPE. For instance, elevated PEEP for the lung
recruitment maneuver may limit venous return, further reduce
cardiac stroke volume and increase the ICP (31). In addition, fluid resuscitation to
help improve cardiac and brain perfusion may increase the
interstitial edema and thus impair pulmonary function (32). In the current study, rapid reduction
of EVLWI and normalized GEDVI along with improved clinical
situation, such as relief of respiratory failure and hemodynamic
instability, was obtained under guidance with the PiCCO system
(Fig. 3), without causing
deterioration of cardiac or neurological function; this implies
that intense and effective hemodynamic monitoring is the key to the
optimal management.
Only a limited number of studies have described the
specific treatment, such as the use of an α-adrenergic blocking
agent, for underlying adrenergic surge in patients with NPE. The
successful treatment with intravenous injection of phentolamine
(8) was reported in a previous case
of NPE caused by an intracranial hemorrhage from a ruptured
arteriovenous malformation, in which increased serum catecholamine
levels were documented. However, postoperative hypotension in the
present patient excluded the usage of an α-adrenergic blocking
agent. An inotropic agent was thus considered for correcting the
relatively low CI, as detected by PiCCO. Levosimendan, a calcium
sensitizer, is known to effectively improve cardiac function
without increasing myocardial oxygen consumption (33). Possibly owing to this unique
characteristic, several clinical trials or meta-analyses have
implied favorable benefits, including improved cardiac function and
reduction of mortality or length of hospital stay, upon
levosimendan treatment when compared with dobutamine treatment in
critically ill patients or those with a cardiology setting
(34–37). The neuroprotective effect of
levosimendan has been recently demonstrated in a TBI in
vitro model (38), and in a
cerebral reperfusion and spinal cord injury in vivo model
(39,40). The exact mechanism is unclear, and is
possibly attribute to the opening of ATP-sensitive K+
channels (mitoKATP channels) and to the suppression of nitric oxide
synthase expression, cell death and inflammatory response upon the
application of levosimendan (40–42).
Thus, treatment with levosimendan rather than dobutamine was
selected in the current study, attempting to correct cardiac
dysfunction without increasing oxygen consumption and preventing
further brain injury. The current patient demonstrated completely
reversed CI following levosimendan administration. To the best of
our knowledge, this is the first report presenting the application
of levosimendan in treating the cardiac dysfunction in NPE. The
improved GCS score was largely attributing to lumbar cistern
drainage therapy, while levosimendan treatment may partially help
accelerate the recovery of brain function with its neuroprotective
ability. Future clinical trials are needed to confirm the potential
role of levosimendan in managing NEP patients with TBI.
In conclusion, the present study reported a case of
NPE that was successfully diagnosed and treated with dynamic
monitoring of PiCCO. The study demonstrated that successful
identification and control of NPE was rapidly obtained through
comprehensive monitoring of serial serum biomarker tests, bedside
echocardiography and, most importantly, hemodynamic monitoring.
Fluid management remains the key element in treating NPE. The
application of the new medication, levosimendan, has extended our
experience in handling the cardiac involvement under CNS insult.
Further clinical trials are required to provide solid evidence on
the potential of this neuroprotective inotropic agent.
Acknowledgements
The present study was supported by grants from the
General Medical and Health Research Program (no. 2013KYA085), the
Research Fund for the Doctoral Program of Higher Education of China
(no. 20130101120035) and the Medical Science and Technology Project
of Zhejiang Province (no. 201480343).
References
|
1
|
Davison DL, Terek M and Chawla LS:
Neurogenic pulmonary edema. Crit Care. 16:2122012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Langlois JA, Rutland-Brown W and Wald MM:
The epidemiology and impact of traumatic brain injury: A brief
overview. J Head Trauma Rehabil. 21:375–378. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bratton SL and Davis RL: Acute lung injury
in isolated traumatic brain injury. Neurosurgery. 40:707–712;
discussion 712. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rogers FB, Shackford SR, Trevisani GT,
Davis JW, Mackersie RC and Hoyt DB: Neurogenic pulmonary edema in
fatal and nonfatal head injuries. J Trauma. 39:860–866; discussion
866–868. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sedy J, Zicha J, Kunes J, Jendelova P and
Syková E: Mechanisms of neurogenic pulmonary edema development.
Physiol Res. 57:499–506. 2008.PubMed/NCBI
|
|
6
|
Mutoh T, Kazumata K, Kobayashi S, Terasaka
S and Ishikawa T: Serial measurement of extravascular lung water
and blood volume during the course of neurogenic pulmonary edema
after subarachnoid hemorrhage: Initial experience with 3 cases. J
Neurosurg Anesthesiol. 24:203–208. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Friesecke S, Heinrich A, Abel P and Felix
SB: Comparison of pulmonary artery and aortic transpulmonary
thermodilution for monitoring of cardiac output in patients with
severe heart failure: Validation of a novel method. Crit Care Med.
37:119–123. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Davison DL, Chawla LS, Selassie L, Tevar
R, Junker C and Seneff MG: Neurogenic pulmonary edema: Successful
treatment with IV phentolamine. Chest. 141:793–795. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
McMurray JJ, Adamopoulos S, Anker SD,
Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C,
Gomez-Sanchez MA, et al: ESC guidelines for the diagnosis and
treatment of acute and chronic heart failure 2012: The Task Force
for the Diagnosis and Treatment of Acute and Chronic Heart Failure
2012 of the European Society of Cardiology Developed in
collaboration with the Heart Failure Association (HFA) of the ESC.
Eur J Heart Fail. 14:803–869. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rieg AD, Rossaint R, Verjans E, Maihöfer
NA, Uhlig S and Martin C: Levosimendan Relaxes Pulmonary Arteries
and Veins in Precision-Cut Lung Slices-The Role of KATP -Channels,
cAMP and cGMP. PLoS One. 8:e661952013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Teasdale G and Jennett B: Assessment of
coma and impaired consciousness. A practical scale. Lancet.
2:81–84. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Werner C and Engelhard K: Pathophysiology
of traumatic brain injury. Br J Anaesth. 99:4–9. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brashear RE and Ross JC: Hemodynamic
effects of elevated cerebrospinal fluid pressure: Alterations with
adrenergic blockade. J Clin Invest. 49:1324–1333. 1970. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nathan MA and Reis DJ: Fulminating
arterial hypertension with pulmonary edema from release of
adrenomedullary catecholamines after lesions of the anterior
hypothalamus in the rat. Circ Res. 37:226–235. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gekka M, Yamaguchi S, Kazumata K,
Kobayashi H, Motegi H, Terasaka S and Houkin K: Hemorrhagic onset
of hemangioblastoma located in the dorsal medulla oblongata
presenting with tako-tsubo cardiomyopathy and neurogenic pulmonary
edema: A case report. Case Rep Neurol. 6:68–73. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Manto A, De Gennaro A, Manzo G, Serino A,
Quaranta G and Cancella C: Early endovascular treatment of
aneurysmal subarachnoid hemorrhage complicated by neurogenic
pulmonary edema and Takotsubo-like cardiomyopathy. Neuroradiol J.
27:356–360. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Inamasu J, Nakatsukasa M, Mayanagi K,
Miyatake S, Sugimoto K, Hayashi T, Kato Y and Hirose Y:
Subarachnoid hemorrhage complicated with neurogenic pulmonary edema
and takotsubo-like cardiomyopathy. Neurol Med Chir (Tokyo).
52:49–55. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Merenkov VV, Kovalev AN and Gorbunov VV:
Bedside lung ultrasound: A case of neurogenic pulmonary edema.
Neurocrit Care. 18:391–394. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Patroniti N, Bellani G, Maggioni E, Manfio
A, Marcora B and Pesenti A: Measurement of pulmonary edema in
patients with acute respiratory distress syndrome. Crit Care Med.
33:2547–2554. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Berkowitz DM, Danai PA, Eaton S, Moss M
and Martin GS: Accurate characterization of extravascular lung
water in acute respiratory distress syndrome. Crit Care Med.
36:1803–1809. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Craig TR, Duffy MJ, Shyamsundar M,
McDowell C, McLaughlin B, Elborn JS and McAuley DF: Extravascular
lung water indexed to predicted body weight is a novel predictor of
intensive care unit mortality in patients with acute lung injury.
Crit Care Med. 38:114–120. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gupta YK, Chugh A, Kacker V, Mehta VS and
Tandon PN: Development of neurogenic pulmonary edema at different
grades of intracranial pressure in cats. Indian J Physiol
Pharmacol. 42:71–80. 1998.PubMed/NCBI
|
|
23
|
Goedje O, Hoeke K, Lichtwarck-Aschoff M,
Faltchauser A, Lamm P and Reichart B: Continuous cardiac output by
femoral arterial thermodilution calibrated pulse contour analysis:
Comparison with pulmonary arterial thermodilution. Crit Care Med.
27:2407–2412. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rocca G Della, Costa MG, Coccia C, Pompei
L, DiMarco P, Vilardi V and Pietropaoli P: Cardiac output
monitoring: Aortic transpulmonary thermodilution and pulse contour
analysis agree with standard thermodilution methods in patients
undergoing lung transplantation. Can J Anaesth. 50:707–711. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bahloul M, Chaari AN, Kallel H, Khabir A,
Ayadi A, Charfeddine H, Hergafi L, Chaari AD, Chelly HE, Ben Hamida
C, et al: Neurogenic pulmonary edema due to traumatic brain injury:
Evidence of cardiac dysfunction. Am J Crit Care. 15:462–470.
2006.PubMed/NCBI
|
|
26
|
Mees SM Dorhout, Hoff RG, Rinkel GJ, Algra
A and van den Bergh WM: Brain natriuretic peptide concentrations
after aneurysmal subarachnoid hemorrhage: Relationship with
hypovolemia and hyponatremia. Neurocrit Care. 14:176–181. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sviri GE, Soustiel JF and Zaaroor M:
Alteration in brain natriuretic peptide (BNP) plasma concentration
following severe traumatic brain injury. Acta Neurochir (Wien).
148:529–533; discussion 533. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fontes RB, Aguiar PH, Zanetti MV, Andrade
F, Mandel M and Teixeira MJ: Acute neurogenic pulmonary edema: Case
reports and literature review. J Neurosurg Anesthesiol. 15:144–150.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Baumann A, Audibert G, McDonnell J and
Mertes PM: Neurogenic pulmonary edema. Acta Anaesthesiol Scand.
51:447–455. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Busl KM and Bleck TP: Neurogenic Pulmonary
Edema. Crit Care Med. 43:1710–1715. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Videtta W, Villarejo F, Cohen M,
Domeniconi G, Cruz R Santa, Pinillos O, Rios F and Maskin B:
Effects of positive end-expiratory pressure on intracranial
pressure and cerebral perfusion pressure. Acta Neurochir Suppl.
81:93–97. 2002.PubMed/NCBI
|
|
32
|
Matsuyama T, Okuchi K, Nishiguchi T, Seki
T and Murao Y: Neurogenic pulmonary edema caused by a medulla
oblongata lesion after head trauma. J Trauma. 63:700–702. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kersten JR, Montgomery MW, Pagel PS and
Warltier DC: Levosimendan, a new positive inotropic drug, decreases
myocardial infarct size via activation of K (ATP) channels. Anesth
Analg. 90:5–11. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Huang X, Lei S, Zhu MF, Jiang RL, Huang
LQ, Xia GL and Zhi YH: Levosimendan versus dobutamine in critically
ill patients: A meta-analysis of randomized controlled trials. J
Zhejiang Univ Sci B. 14:400–415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Delaney A, Bradford C, McCaffrey J,
Bagshaw SM and Lee R: Levosimendan for the treatment of acute
severe heart failure: A meta-analysis of randomised controlled
trials. Int J Cardiol. 138:281–289. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Landoni G, Biondi-Zoccai G, Greco M, Greco
T, Bignami E, Morelli A, Guarracino F and Zangrillo A: Effects of
levosimendan on mortality and hospitalization. A meta-analysis of
randomized controlled studies. Crit Care Med. 40:634–646. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Oner E, Erturk M, Birant A, Mansıroglu A
Kurtar, Akturk IF, Karakurt H, Yalcin AA, Uzun F, Somuncu MU and
Yildirim A: Assessment of sustained effects of levosimendan and
dobutamine on left ventricular systolic functions by using novel
tissue Doppler derived indices in patients with advanced heart
failure. Cardiol J. 22:87–93. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Roehl AB, Hein M, Loetscher PD, Rossaint
J, Weis J, Rossaint R and Coburn M: Neuroprotective properties of
levosimendan in an in vitro model of traumatic brain injury. BMC
Neurol. 10:972010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hein M, Zoremba N, Bleilevens C, Bruells
C, Rossaint R and Roehl AB: Levosimendan limits reperfusion injury
in a rat middle cerebral artery occlusion (MCAO) model. BMC Neurol.
13:1062013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Lafci B, Yasa H, Ilhan G, Ortac R, Yilik
L, Kestelli M, Goktogan T and Gurbuz A: Protection of the spinal
cord from ischemia: Comparative effects of levosimendan and
iloprost. Eur Surg Res. 41:1–7. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Das B and Sarkar C: Pharmacological
preconditioning by levosimendan is mediated by inducible nitric
oxide synthase and mitochondrial KATP channel activation in the in
vivo anesthetized rabbit heart model. Vascul Pharmacol. 47:248–256.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Hönisch A, Theuring N, Ebner B, Wagner C,
Strasser RH and Weinbrenner C: Postconditioning with levosimendan
reduces the infarct size involving the PI3K pathway and
KATP-channel activation but is independent of PDE-III inhibition.
Basic Res Cardiol. 105:155–167. 2010. View Article : Google Scholar : PubMed/NCBI
|