Introduction
Inflammatory bowel disease (IBD) involves ulcerative
colitis (UC), Crohn's disease (CD) and indeterminate colitis. These
subtypes of IBD display important differences in the behavior of
the natural course of the disease, including frequent remissions
and exacerbations, response to treatment and complications. Early
diagnosis is critical for proper treatment (1). In Mexico, in the last 10 years there
has been an increase with ~76 new UC cases per year, which is a
dramatic increase compared with the previous decade that recorded
an average of 28 cases per year, accumulating 150,000 cases in
Mexico (2,3). Despite increased use of
immunosuppressive therapy, the long-term risk of required
intestinal resection and permanent ileostomy in CD is ~80 and 10%,
respectively (4). In UC patients,
the risk of required colectomy is ~1% per year according to
population-based cohort studies in Northern Europe (5).
Remission in UC is defined as complete resolution of
symptoms and endoscopic mucosal healing, whereas in CD, a clinical
remission is considered as one with a clinical disease activity
index (CDAI) of <150 (6–8). In CD and UC, the early use of
aggressive therapy, including the combination of thiopurines and
anti-tumor necrosis factor-α (anti-TNF-α) is considered, with the
aim of achieving deep and sustained remission (9). However, certain CD patients present
with localized and uncomplicated (no perforation, no stricture)
disease at diagnosis. Similarly, UC may manifest without disabling
symptoms, biological abnormalities or severe endoscopic lesions at
diagnosis. In those patients, the early and prolonged use of
immunosuppressive therapy (anti-TNF-α), with its associated risk of
serious infections and cancer, may not be appropriate, as the
spontaneous evolution of the disease may have been benign (10,11).
The risk of over-treating patients may be reduced by
accurately diagnosing them with a combination of clinical and
endoscopic examination, as well as detection of serological markers
present in different stages of the disease, which may predict the
subsequent course of IBD; however, serological biomarkers for the
severity of IBD have been far lees studied in UC than in CD, and it
has been rarely applied in the clinical setting (12).
TNF-α is a cytokine involved in the regulation of a
wide spectrum of biological processes, including cell
proliferation, differentiation and apoptosis, as well as
coagulation and lipid metabolism. TNF-α may decrease the appetite,
body weight and body mass index (BMI), and induce the synthesis of
catabolic hormones, including insulin-like growth hormone-1, and
increase lipolysis in adipose tissue (13). As adipocytes have been recognized to
actively participate in systemic immune responses via the secretion
of peptides detectable in the systemic circulation, the so-called
adipocytokines (adipokines) (14–16),
increased lipolysis by increased TNF-α production results in
impaired production of certain adipokines, such as leptin (13). In metabolism, the plasma levels of
leptin serve as a signal of energy sufficiency to the hypothalamus,
resulting in anorexia and increased energy expenditure when fat
stores are exceeded (17). During
inflammation, leptin may falsely signal an excess of fat mass to
the hypothalamus and drive an inappropriate physiological response.
In addition, if the TNF-α concentration diminishes when the
immunologic response and inflammation decrease due to treatment
with anti-TNF-α drugs, including infliximab (17–19), the
deregulation of leptin by the use of biological therapy may be
expected. Therefore, the regulation of leptin and other adipokines
and its physiological consequences have been examined in human
inflammatory diseases, including IBD (19–21). In
one of these studies, Waluga et al (21), investigated serum adipokine levels
(transforming growth factor-β1, adiponectin, leptin, chemerin,
resistin and visfatin) in patients with IBD prior treatment and
after achieving clinical remission. Their results suggested that
IBD modulated serum adipokine levels by increasing resistin and
visfatin release and suppressing leptin production. These authors
proposed leptin concentrations in CD and UC subjects, may be the
result of TNF-α hyperactivity leading to a decrease in leptin
mediated chronic inflammation. Accordingly, the aim of the present
study was to evaluate the serum levels of 10 adipokines and their
association with disease activity on endoscopy in IBD. The
modulation of the adipokines by IBD therapy was also evaluated.
Materials and methods
Participants and biological
samples
A case-control study consisting of non-related
subjects from the Zacatecas state in Mexico was performed. Subjects
were recruited from the Gastroenterological service of the
Zacatecas Instituto de Seguridad y Servicios Sociales de los
Trabajadores del Estado (ISSSTE) General Hospital (Zacatecas,
Mexico) between July and October 2016. The protocol was approved by
the Committee on Education, Research, Training and Ethics of ISSSTE
General Hospital (approval ID, OFC226/2016-2-001). All participants
provided written informed consent for their participation in the
study, in accordance with the Helsinki declaration. IBD was
diagnosed according to clinical, endoscopic and pathological
criteria as previously described (18). All patients with previous diagnoses
of IBD were included in the case group (n=34; UC, n=23; CD, n=11).
All the cases at the time of recruitment had already received
pharmacological therapy according with the World Gastroenterology
Organization Global guidelines (22). The control group (n=19) consisted of
healthy subjects who were screened due to indications of colon
cancer in accordance with the World Gastroenterology Organization
guidelines (23) and absence of
treatment with anti-inflammatory drugs. In the two groups,
participants with comorbidities, including diabetes or autoimmune
diseases, or with any associated inflammatory or infectious
diseases, including tuberculosis, cytomegalovirus infection or
urinary tract infection, were excluded.
Each of the participants donated a blood sample at
the moment of their recruitment. Subsequently, they underwent a
colonoscopy procedure according the guidelines of the American
Society for Gastrointestinal Endoscopy (24). Tissue samples from colon segments
were obtained for histopathologic evaluation using
Multibite™ biopsy forceps (Boston Scientific, Boston,
MA, USA) (24). Blood samples were
centrifuged at 1,000 × g for 15 min at room temperature (RT). Serum
was collected, aliquoted and stored at −80°C until use.
Epidemiological and clinical data, including clinical
activity/disease activity on endoscopy by appropriate scales [UC
Mayo endoscopic score (UC-MES), UC endoscopic index of severity
(UCEIS), UC/CD Montreal classification, CD activity index (CDAI),
simple endoscopic scale for CD (SES-CD) and Truelove-Witts score]
(25,26), date of diagnosis, initial and current
treatment, phenotype, extraintestinal manifestations of the disease
and laboratory parameters, were obtained from clinical records. The
presence of endoscopic activity for each IBD subtype was defined as
the UC-MES and the UCEIS suggesting at least the mild stage for UC,
and at least score 1 of the SES-CD and B2 of the Montreal
classification for CD. The size of mucosal ulcers, ulcerated
surface, endoscopic extension and stenosis features were
evaluated.
Marker quantification
The levels of 10 biomarkers, C-peptide, ghrelin,
gastric inhibitory polypeptide (GIP), glucagon-like peptide-1
(GLP), glucagon (GCG), insulin (INS), leptin (LEP), total
plasminogen activator inhibitor-1 (PAI-1), resistin (RETN) and
visfatin, were analyzed using the Bio-Plex Pro Human Diabetes
10-Plex Panel (Bio-Rad Laboratories, Hercules, CA, USA). Serum
quantification was performed as follows: Samples (aliquots of 200
µl) were centrifuged at 30,000 × g for 5 min at RT to remove any
precipitate. The appropriate analyte standards and samples were
diluted in standard diluent and sample diluent, respectively. A
standard curve composed of eight points was prepared from the
recombinant analyte standard. Standards, blanks and samples were
added to a 96-well plate containing antibodies that were chemically
attached to fluorescent-labeled microbeads. The samples were
incubated in the dark at room temperature in constant motion for 1
h. The plate was washed three times, a detection antibody was added
to each well, and the plate was incubated in the dark for 30 min at
RT with agitation, followed by three washes.
Streptavidin-phycoerythrin was added to each well and the plate was
incubated in the dark for 10 min at RT with agitation. The beads
were re-suspended in 125 µl buffer, and the reaction was quantified
using the BioPlex®200 Multiplex System platform (Bio-Rad
Laboratories). Each sample was analyzed in duplicate and the data
were automatically analyzed and processed using Bio-Plex Manager
6.1 software (Bio-Rad Laboratories).
Statistical analysis
Risk factors and clinical and personal
characteristics were compared using a Chi-square or Fisher's exact
test for categorical variables, and a Student's t-test,
Mann-Whitney U test or analysis of variance (ANOVA) as appropriate,
for numerical variables. ANOVA was coupled to Holm-Sidak or Dunn's
Method as appropriate for the multiple comparison procedure. The
usefulness of serum leptin levels to correctly classify the study
groups according to their disease status was evaluated using a
receiver operating characteristic curve (ROC) analysis. In this
analysis, leptin sensitivity and specificity values were used to
calculate the related area under the curve and the positive and
negative predictive values at fixed protein concentration cutoffs.
Each cutoff value for serum leptin level was obtained considering
the ROC curve in which the value of the sum of sensitivity and
specificity was maximal (sensitivity + specificity closest to two).
The odds ratios with Yates continuity correction were calculated
for significant comparisons. To evaluate the correlation between
two variables, a Spearman Rank Order Correlation test was
performed. P<0.05 was considered to indicate a statistically
significant difference. Data analysis was performed using Sigma
Plot v.11 (Systat Software Inc., San Jose, CA, USA) and GraphPad
Prism v.5.03 (GraphPad Software, Inc., La Jolla, CA, USA).
Results
Patient characteristics
A total of 53 participants were enrolled in the
present study, including 34 patients diagnosed with IBD (UC, 23;
CD, 11) and 19 healthy controls. General data and clinical
characteristics of the study population are listed in Tables I and II. The median of age was 59 years (range,
26–78) for the cases and 54 (range, 31–49) years for the controls
(P=0.312). There were no differences between the study groups in
terms of risk factors and/or clinical variables, including gender,
family history of IBD, smoking, BMI, hemoglobin, glucose,
triglycerides, total cholesterol, high-density lipoprotein (HDL),
low-density lipoprotein (LDL), very LDL (VLDL) or
systolic/diastolic blood pressure (P>0.05).
 | Table I.Classification of patients with
inflammatory bowel disease (n=34). |
Table I.
Classification of patients with
inflammatory bowel disease (n=34).
| Item | N (%) |
|---|
| Diagnosis |
|
| UC | 23 (67.6) |
| CD | 11 (32.4) |
| Mayo endoscopic
activity |
|
|
Remission | 8 (23.5) |
|
Mild | 14 (41.2) |
|
Moderate | 1 (2.9) |
|
Severe | 0 (0) |
| Montreal UC |
|
| E1 | 7 (20.6) |
| E2 | 8 (23.5) |
| E3 | 8 (23.5) |
| UCEIS |
|
|
Remission | 8 (23.5) |
|
Mild | 14 (41.2) |
|
Moderate | 1 (2.9) |
|
Severe | 0 (0) |
| Truelove-witts
clinical |
|
|
Remission | 14 (41.2) |
|
Mild | 6 (17.6) |
|
Moderate | 3 (8.8) |
|
Severe | 0 (0) |
| CDAI |
|
|
<150 | 11 (32.4) |
|
150–220 | 0 (0) |
|
220–450 | 0 (0) |
|
>450 | 0 (0) |
| Montreal CD |
|
|
Location |
|
| SB | 3 (8.8) |
|
Colon | 4 (11.8) |
|
SB-colon | 4 (11.8) |
| Upper
GI | 0 (0) |
|
Behavior |
|
|
Inflammatory | 6 (17.6) |
|
Stricturing | 2 (5.9) |
|
Fistulizing | 3 (8.8) |
| Endoscopy simple CD
score |
|
| 0 | 5 (14.7) |
| 1 | 5 (14.7) |
| 2 | 1 (2.9) |
| 3 | 0 (0) |
| Table II.Comparison of clinical parameters
between the study groups. |
Table II.
Comparison of clinical parameters
between the study groups.
| Characteristic | IBD (n=34) | Control (n=19) | P-value |
|---|
| Age (years) |
54.8±15.1 |
53.2±9.6 | 0.312 |
| Gender (female/male
ratio) | 1.43 | 5.3 | 0.111 |
| Family history of
IBD | 1 (2.9%) | 1 (5.2%) | 1.000 |
| HDL (mg/dl) |
45.2±12.3 |
45.7±12.5 | 0.905 |
| LDL (mg/dl) | 110.5±27.6 |
123.2±32.7 | 0.155 |
| VLDL (mg/dl) |
25.7±10.8 |
23.2±6.5 | 0.37 |
| Triglycerides
(mg/dl) | 131.7±51.5 |
120.9±38.3 | 0.446 |
| Cholesterol
(mg/dl) | 181.0±28.6 |
191.6±41.3 | 0.288 |
| TIA (mg/dl) |
4.0±1.1 |
4.3±1.1 | 0.374 |
| Glucose
(mg/dl) |
90.2±20.2 |
87.7±7.7 | 0.953 |
| Hemoglobin
(g/dl) | 14.6±1.9 |
14.1±1.8 | 0.293 |
| Hematocrit (%) | 44.2±9.5 |
41.0±4.3 | 0.108 |
| BMI
(kg/m2) | 27.6±5.9 |
28.4±6.5 | 0.711 |
| SBP (mm/Hg) | 114.1±9.8 | 110.0±5.8 | 0.228 |
| DBP (mm/Hg) | 77.2±5.8 |
75.4±6.6 | 0.315 |
| ESR (mm/h) |
1.5±0.51 |
1.3±0.49 | 0.322 |
| CRP (mg/l) |
0.51±0.63 |
0.35±0.29 | 0.888 |
IBD and endoscopic activity
In the case group, the clinical activity in UC
patients according to the Truelove-Witts scale was as follows: 14
patients were in remission, 6 had mild activity and 3 had moderate
activity. In the group of CD patients, the clinical activity was
determined as <150 points on the CDAI scale. In the UC group,
maximal endoscopic involvement (E1) was observed in 7 cases, E2 was
observed in 8 subjects and the E3 stage was observed in the
remaining 8 UC cases. The location of CD according to the Montreal
classification was in the small bowel for 3 participants, in the
colon for 4 cases and in the colonic ileum for the remaining 4 CD
cases. Evaluation of the endoscopic activity of UC according to the
UC-MES indicated that 8 cases were in remission, 14 had mild
activity and one had moderate endoscopic activity. In CD patients,
no endoscopic activity (SES-CD score=0) was observed in 5 patients,
while 5 and 1 patients displayed activity with score of 1 and 2,
respectively (Table I).
Extraintestinal manifestations were observed in 4 UC cases (27.3%)
and in 3 CD cases (17.4%), respectively.
Leptin levels are associated with
IBD
Table III displays
the results of the adipokine quantification determined at baseline
in the serum of IBD patients and control subjects. Of note, the
serum levels of leptin in the IBD group were significantly lower
than those in the controls (5,039.2±5,219.8 vs. 8,847.6±4,044.2
pg/ml; P=4.9×10−4). However, there were no significant
differences in the serum levels of the 9 remaining adipokines
(P>0.05).
| Table III.Serum concentrations of the ten
proteins evaluated in the IBD and control groups. |
Table III.
Serum concentrations of the ten
proteins evaluated in the IBD and control groups.
| Analyte | IBD (n=34) | Control (n=19) | P-value |
|---|
| C-peptide
(pg/ml) | 972.3±512.2 | 975.4±281.0 | 0.414 |
| Ghrelin
(pg/ml) |
3,781.5±1,498.4 | 3,471.4±878.9 | 0.781 |
| GIP (pg/ml) | 524.9±381.9 | 426.4±197.6 | 0.549 |
| GLP-1 (pg/ml) | 834.9±126.9 | 817.5±46.7 | 0.838 |
| Glucagon
(pg/ml) | 1,155.4±118.9 | 1,119.4±64.9 | 0.182 |
| Insulin
(pg/ml) | 961.8±306.6 | 911.8±236.1 | 0.656 |
| Leptin (pg/ml) |
5,039.2±5,219.8 |
8,847.6±4,044.2 |
4.9×10−4a |
| PAI-1 (pg/ml) |
78,984.5±58,986.9 |
82,870.7±38,624.1 | 0.541 |
| Resistin
(pg/ml) |
4,491.8±1,984.1 |
5,131.0±3,061.5 | 0.738 |
| Visfatin
(pg/ml) |
11,622.4±3,6291.3 | 4,494.1±883.1 | 0.656 |
When the IBD participants were stratified into UC
and CD groups (Table IV), the serum
levels of leptin in UC patients were significantly lower than those
in CD patients (P=0.001). Leptin serum levels did not significantly
differ between UC and CD groups (P>0.05). No differences in the
serum levels of the other adipokines were identified between the
UC, CD and healthy controls groups.
| Table IV.Comparison of serum adipokine levels
between the study groups. |
Table IV.
Comparison of serum adipokine levels
between the study groups.
| Analyte | Control (n=19) | CD (n=11) | UC (n=23) | P-value |
|---|
| C peptide
(pg/ml) | 975.4±281.0 | 1,112.6±468.2 | 905.19±528.5 | 0.208 |
| Ghrelin
(pg/ml) | 3,471.4±878.9 |
4,192.5±1,929.8 |
3,584.94±1,245.1 | 0.745 |
| GIP (pg/ml) | 426.4±197.6 | 635.3±506.2 | 469.7±301.1 | 0.150 |
| GLP-1 (pg/ml) | 817.5±46.7 | 860.4±133.0 | 822.71±125.0 | 0.292 |
| Glucagon
(pg/ml) | 1,119.4±64.9 | 1,184.7±163.7 | 1,141.4±91.5 | 0.251 |
| Insulin
(pg/ml) | 911.8±236.1 | 1,052.0±291.4 | 918.68±310.5 | 0.176 |
| Leptin (pg/ml) |
8,847.6±4,044.22 |
7,257.4±8,051.3 |
3,978.26±2,787.0 | 0.001a |
| PAI-1 (pg/ml) |
82,870.7±38,624.1 |
109,456.2±93,303.5 |
64,411±23,996.3 | 0.090 |
| Resistin
(pg/ml) |
5,131.0±3,061.5 |
5,189.8±2,282.6 |
41,58.01±1,782.3 | 0.457 |
| Visfatin
(pg/ml) | 4,494.1±883.2 |
6,230.6±6,232.3 |
14,201.0±44,005 | 0.745 |
Leptin levels are associated with
endoscopic activity in IBD patients
Leptin serum concentrations were determined at
baseline and as presented in Fig. 1,
the leptin levels were compared between patient groups stratified
by the presence/absence of disease activity on endoscopy. Compared
with the control group, IBD patients with and without disease
activity on endoscopy had lower serum leptin levels (P<0.001).
In CD (Fig. 1B) and UC patients
(Fig. 1C), significant differences
in serum leptin levels were observed between controls and patients
with and without disease activity on endoscopy (P=0.001). Compared
with those in the controls and IBD without disease activity on
endoscopy, the serum leptin levels in IBD patients with positive
endoscopic activity was significantly lower (P<0.001; data not
shown).
To determine whether the circulating leptin
concentration was affected by IBD treatment, IBD cases were
stratified according to their pharmacological therapy, and the
leptin levels were compared between the groups (Fig. 2A; Table
V). Compared with the controls, serum leptin levels were
reduced in patients treated with 5-aminosalicylic acid (5-ASA)
monotherapy (P=0.008), 5-ASA + azathioprine (P=0.002) and 5-ASA +
adalimumab (P=0.036). IBD participants then evaluated separately as
CD (Fig. 2B) or UC groups (Fig. 2C). Compared with the controls, the
serum leptin levels were significantly lower in UC patients with
5-ASA monotherapy (P=0.0015) and 5-ASA + azathioprine (P=0.002),
but not in those with 5-ASA + adalimumab (P=0.165). Leptin levels
in CD patients receiving various treatments were not significantly
different from those in healthy controls (P>0.05). In the same
sense, additional differences between pairs of treatments were not
found with or without stratification of the IBD participants
(P>0.05).
| Table V.General description of the treatment
of patients with inflammatory bowel disease. |
Table V.
General description of the treatment
of patients with inflammatory bowel disease.
| Treatment/item | Ulcerative
colitis | Crohn's
disease |
|---|
| Current
treatment |
|
|
|
5-ASA | 15 | 2 |
| 5-ASA +
Azathioprine | 5 | 7 |
| 5-ASA +
Adalimumab | 3 | 2 |
| Use of anti-TNF-α
in the course of the disease |
|
|
|
Yes | 5 | 2 |
| No | 15 | 7 |
| Change in
anti-TNF-α regimen |
|
|
|
Maintenance treatment | 3 | 2 |
|
Failure | 2 | 1 |
|
Allergic reaction | 1 | 0 |
| Restart
treatment due to relapse | 2 | 0 |
| Azathioprine
intolerance | 0 | 1 |
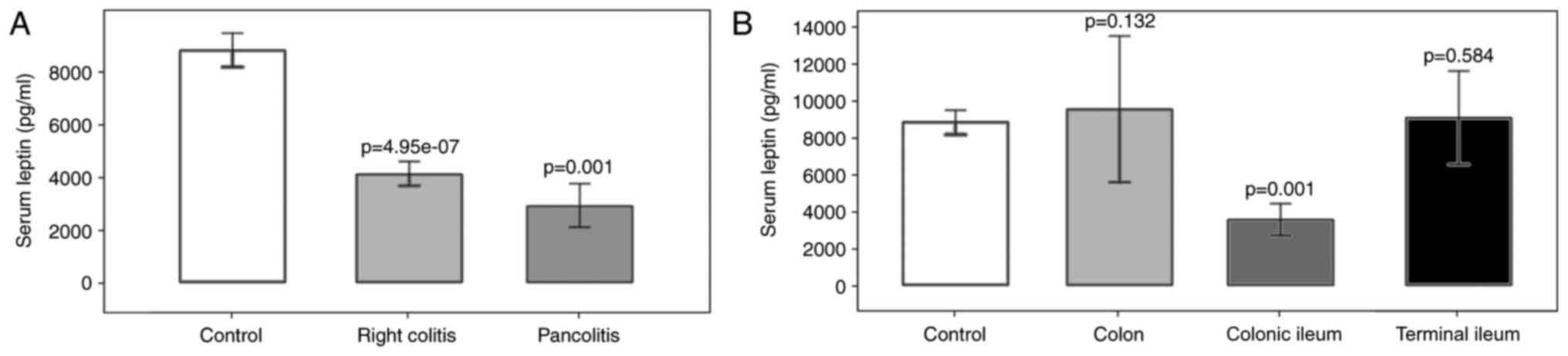
Association of leptin with the
location of IBD
Regarding the location of IBD, leptin levels were
significantly decreased in UC patients with right colitis
(P=4.95×10−7) and pancolitis (P=0.001) compared with
those in the controls. In the CD group, a significant reduction of
the leptin concentration was observed in patients with disease
located in the colonic ileum compared with that in the control
group (P=0.001; Fig. 3). Significant
differences in leptin levels between right colitis and pancolitis,
or colon, colonic ileum or terminal ileum were not identified
(P>0.05).
Regarding the presence/absence of an extraintestinal
manifestation of IBD as a classifier and using the control group as
a reference, circulating leptin was lower in patients without
extraintestinal manifestations (6,404.4±5,133.4 pg/ml; P=0.002). No
significant differences were observed in serum leptin levels
between controls and IBD cases with extraintestinal manifestations
(P=0.053), or between IBD cases with or without extraintestinal
manifestations (P=0.848). The serum levels of the 9 remaining
markers evaluated were not affected by the presence of
extraintestinal manifestations (data not shown).
Correlation of leptin with clinical
parameters
To evaluate the correlation between leptin levels
and clinical features of the study population, a correlation
analysis was performed. A positive correlation was identified
between serum leptin levels and BMI (r=+0.35, P=0.017), while a
negative correlation between serum leptin levels and hemoglobin was
observed (r=−0.31, P=0.026). No significant correlation between
leptin levels and other clinical parameters, including C-reactive
protein (CRP) or the erythrocyte sedimentation rate (ESR), were
identified (P>0.05).
Circulating leptin as a marker for IBD
and endoscopic activity
To evaluate the usefulness of serum leptin levels to
correctly classify the study groups according to their disease
status, a receiver operating characteristic (ROC) analysis was
performed (Table VI). Regarding the
use of serum leptin for the diagnosis of IBD with a cutoff value of
5,494 pg/ml, the sensitivity and specificity values were calculated
as 71 and 84%, respectively. Serum leptin levels <5,494 pg/ml
significantly increased the odds of IBD by 12.8-fold among the
study population [odds ratio (OR)=12.8, 95% confidence interval
(CI)= 3.04–53.9, P=0.001]. The odds of disease activity on
endoscopy in patients with serum leptin levels of <2,498 pg/ml
was increased 5.8-fold among the IBD patients (OR=5.8, 95% CI
=1.52–22.4, P=0.013).
| Table VI.ROC analysis of serum leptin in IBD
patients. |
Table VI.
ROC analysis of serum leptin in IBD
patients.
| Parameter | IBD vs.
controls | Endoscopic activity
(presence vs. absence) |
|---|
| Area under ROC
curve | 0.791 | 0.651 |
| Leptin cutoff
(pg/ml) | 5,494 | 2,498 |
| Sensitivity
(%) | 71 | 45 |
| Specificity
(%) | 84 | 88 |
| Predictive positive
value (%) | 89 | 87 |
| Predictive negative
value (%) | 38 | 1 |
| Odds ratio | 12.8 | 5.8 |
| 95% Confidence
interval | 3.04–53.9 | 1.52–22.4 |
|
P-valuea | <0.001 | 0.013 |
Discussion
The traditional assessment of IBD patients is
somewhat complicated by the necessary, but rather invasive nature
of evaluation, including endoscopic procedures with biopsies
(27). To date, no ideal biomarker
has been identified for the assessment and management of IBD. The
aim of the present study was to evaluate the serum levels of
C-peptide, ghrelin, GIP, GLP, glucagon, insulin, leptin, PAI-1,
resistin and visfatin and their association with endoscopic
activity in IBD. These proteins are produced by white adipose
tissue (WAT), which functions not only as a reservoir of free fatty
acids (energy source) but also as an endocrine organ, sending out
and responding to signals that modulate appetite, energy
expenditure, insulin sensitivity, the endocrine and reproductive
systems, bone metabolism and immunity. Accordingly, WAT and its
signaling molecules provide an important link between obesity,
insulin resistance and inflammatory disorders (28,29). In
the present study, among the 10 adipokines evaluated, leptin levels
were significantly lower in patients with IBD compared with those
in healthy controls. Leptin, a 16-kDa polypeptide encoded by the
ob gene, is mainly produced by adipocytes in adipose tissue,
and at lower levels by fundic epithelium of peripheral tissues
including that of the gastric mucosa, skeletal muscle, lymph node,
liver, thyroid, placenta and spinal cord (30). The most important functions of leptin
are inhibition of appetite and modulation of immune and
inflammatory reactions. The results of the present study are in
agreement with those reported by Waluga et al (21) from 2014 and Karmiris et al
(31) from 2006, whose case-control
studies indicated decreased serum leptin levels in subjects with
the two types of IBD compared with those in healthy controls.
However, in other previous studies, serum leptin levels were
reported to increase (32) or remain
unchanged (33,34) in IBD patients compared with those in
healthy controls. Despite the discrepancy in serum leptin levels,
an increase in leptin in close proximity to the site of
inflammation has been consistently reported, with a significant
increase in mRNA expression and secretion of leptin from mesenteric
adipose tissue of CD and UC patients compared with that in controls
(35,36). At the tissue level, where protein
production reflects local cellular behavior, the circulating
concentrations of molecules represent the total contribution of the
body tissues and therefore, they are useful to identify additional
changes associated with the general health state of the patient or
with other external variables. As observed in the present study,
leptin levels were associated with the BMI, the extent of the
affected area, disease activity and/or treatment. Accordingly, the
discrepancies observed in serum leptin concentrations between
studies may be explained in part by the differences in those
features between the populations evaluated.
In the present study, when the participants were
stratified according to the presence/absence of endoscopic
activity, the serum leptin levels in the group with disease
activity on endoscopy were significantly decreased relative to
those in the controls, as well as in patients with vs. without
disease activity on endoscopy, suggesting the involvement of a
defective regulation of the leptin pathway in the pathogenesis of
IBD. When the IBD participants were stratified into CD and UC
groups and compared with the controls, differences in serum leptin
levels were observed for the UC group but not for the CD group,
reflecting differences in the molecular mechanisms for the two
types of IBD. Although these results should be validated in other
IBD cohorts with large patient numbers, the present study obtained
a 12.8-fold increased odds of IBD among the study population when a
cutoff for serum leptin levels <5,494 pg/ml was chosen. In
addition, regarding the presence or absence of disease activity on
endoscopy, serum leptin levels with cutoff <2,498 pg/ml provided
a 5.8-fold increased odds of disease activity on endoscopy among
the IBD patients, suggesting that the leptin concentration may
represent an attractive marker to consider in IBD risk
determination. It is important to note that in the study
population, the known non-invasive biomarkers of IBD (CRP and ESR)
had normal values in most of the participants, and therefore, its
classifier value for disease activity on endoscopy was not
comparable with that of leptin. Additional studies are therefore
required to evaluate this comparison.
In the present study, a significant decrease in
leptin levels was identified between the control and different
treatment groups (5-ASA, 5-ASA + azathioprine, 5-ASA + adalimumab).
Of note, when IBD patients were evaluated separately as CD or UC
groups, differences in serum leptin levels compared with those in
the control group were only observed in the UC group for the 5-ASA
and 5-ASA + azathioprine, but not for the 5-ASA + adalimumab
treatment, suggesting that the treatment with 5-ASA + adalimumab
may partially restore the leptin levels in UC but no in CD
patients. As the present study was a transversal case-control study
and considering that the cohort did not include any IBD patients
without treatment, additional studies are required to determine
whether the downregulation of leptin in IBD patients compared with
that in healthy controls was independent of the prescribed
treatments. In this sense, Waluga et al (21) postulated that low leptin levels may
be a result of TNF-α hyperactivity. As TNF-α stimulates the
temporary release of substantial amounts of leptin in response to
inflammation, a decrease in leptin-mediated chronic inflammation
may eventually be expected. It has been demonstrated that serum
leptin levels increased in CD subjects treated with the TNF-α
antagonist infliximab, confirming the role of TNF-α in the
regulation of leptin release by adipocytes (37). In addition, in the study by Waluga
et al (21) reported that a
3-month treatment period with corticosteroids alone or with
azathioprine lead to an increased plasma concentration of leptin in
CD patients (21). Is important to
mention that large errors values in the leptin serum levels were
observed, mainly on the CD subjects, this may be due to the sample
size and/or the differences in pharmacologic treatment initiation
between patients. The large data dispersion may have an impact on
the statistical analysis, and may therefore be considered a
limitation of the present study.
Finally, the present study identified a significant
positive correlation between leptin and BMI and a negative
correlation between leptin and hemoglobin levels. A previous study
indicated that leptin and erythropoietin acted synergistically to
increase erythroid development in vitro (38). Although the effect of leptin on
hematopoiesis may be modest, the present results are in accordance
with that reported previously by Togo et al (39), whose identified a negative
correlation between the levels of leptin and those of hemoglobin in
Japanese men, suggesting that leptin may have a role in
hematopoiesis in humans.
Although CD and UC have certain clinical and
pathological features in common, they may be distinguished based on
their localization, endoscopic appearance, histology and behavior,
which suggests differences in the underlying pathophysiology. In
accordance with the present results, these differences are also
reflected in the circulating leptin levels, supporting the
involvement of leptin in the pathogenesis of IBD, suggesting the
suitability of leptin as a non-invasive marker to determine the
risk of disease activity on endoscopy and its potential utility as
a marker to optimize the treatment of UC.
In conclusion, the present study indicated that
serum leptin is decreased in IBD. Low serum leptin levels were
associated with an increased risk of IBD and disease activity on
endoscopy among the study population. Additional studies are
required to validate these results in populations with a greater
number of IBD patients.
Acknowledgements
The authors would like to thank all of the study
participants. The authors also appreciate contributions from Dr
Adrian Lopez Saucedo and Dr Manuel Presno Bernal for their
scientific advice and to Miss Alma Martinez for her assistance and
technical support. The facilities for the development of the study
provided by the Department of Education of the General Hospital of
ISSSTE are also recognized. This work was funded in part by CONACYT
(grant nos. CONACYT-SEP-CB-2009-01-0128567,
-FOMIX-M0024-2013-01-203220, -SS/IMSS/ISSSTE-2010-138721,
-SS/IMSS/ISSSTE-2012-01-181124, -INFR-2014-225520, and
INFR-2015-254106). The editing costs of the manuscript were covered
in part by the Promotion of Quality Program (PFC) support (to the
academic team with registration number: CA-UAZ-207).
References
|
1
|
Kuna AT: Serological markers of
inflammatory bowel disease. Biochem Med (Zagreb). 23:28–42. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yamamoto-Furusho JK: Clinical epidemiology
of ulcerative colitis in Mexico: A single hospital-based study in a
20-year period (1987–2006). J Clin Gastroenterol. 43:221–224. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cronica, . In Mexico there was a triple
increase in the number of cases of inflammatory bowel disease.
http://www.cronica.com.mx/notas/2017/1015339.html(In
Spanish). July 21–2017
|
|
4
|
Cosnes J, Gower-Rousseau C, Seksik P and
Cortot A: Epidemiology and natural history of inflammatory bowel
diseases. Gastroenterology. 140:1785–1794. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Solberg IC, Lygren I, Jahnsen J, Aadland
E, Høie O, Cvancarova M, Bernklev T, Henriksen M, Sauar J, Vatn MH,
et al: Clinical course during the first 10 years of ulcerative
colitis: Results from a population-based inception cohort (IBSEN
Study). Scand J Gastroenterol. 44:431–440. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sandborn WJ, Feagan BG, Hanauer SB, Lochs
H, Löfberg R, Modigliani R, Present DH, Rutgeerts P, Schölmerich J,
Stange EF and Sutherland LR: A review of activity indices and
efficacy endpoints for clinical trials of medical therapy in adults
with Crohn's disease. Gastroenterology. 122:512–530. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stange EF, Travis SP, Vermeire S,
Beglinger C, Kupcinkas L, Geboes K, Barakauskiene A, Villanacci V,
Von Herbay A, Warren BF, et al: European evidence based consensus
on the diagnosis and management of Crohn's disease: Definitions and
diagnosis. Gut. 1 55 Suppl:11–15. 2006.
|
|
8
|
Van Assche G, Dignass A, Panes J,
Beaugerie L, Karagiannis J, Allez M, Ochsenkühn T, Orchard T,
Rogler G, Louis E, et al: The second European evidence-based
consensus on the diagnosis and management of Crohn's disease:
Definitions and diagnosis. J Crohns Colitis. 4:7–27. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Colombel JF, Sandborn WJ, Reinisch W,
Mantzaris GJ, Kornbluth A, Rachmilewitz D, Lichtiger S, D'Haens G,
Diamond RH, Broussard DL, et al: Infliximab, azathioprine, or
combination therapy for Crohn's disease. N Engl J Med.
362:1383–1395. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Beaugerie L, Brousse N, Bouvier AM,
Colombel JF, Lémann M, Cosnes J, Hébuterne X, Cortot A, Bouhnik Y,
Gendre JP, et al: Lymphoproliferative disorders in patients
receiving thiopurines for inflammatory bowel disease: A prospective
observational cohort study. Lancet. 374:1617–1625. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Peyrin-Biroulet L, Khosrotehrani K, Carrat
F, Bouvier AM, Chevaux JB, Simon T, Carbonnel F, Colombel JF, Dupas
JL, Godeberge P, et al: Increased risk for nonmelanoma skin cancers
in patients who receive thiopurines for inflammatory bowel disease.
Gastroenterology. 141:1621–1628.e1-5. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Beaugerie L and Sokol H: Clinical,
serological and genetic predictors of inflammatory bowel disease
course. World J Gastroenterol. 18:3806–3813. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ehsani AH, Mortazavi H, Balighi K,
Hosseini MS, Azizpour A, Hejazi SP, Goodarzi A and Darvari SB:
Changes in body mass index and lipid profile in psoriatic patients
after treatment with standard protocol of infliximab. Acta Med
Iran. 54:570–575. 2016.PubMed/NCBI
|
|
14
|
Kopp A, Buechler C, Neumeier M, Weigert J,
Aslanidis C, Schölmerich J and Schäffler A: Innate immunity and
adipocyte function: Ligand-specific activation of multiple
Toll-like receptors modulates cytokine, adipokine, and chemokine
secretion in adipocytes. Obesity (Silver Spring). 17:648–656. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Schäffler A, Schölmerich J and Salzberger
B: Adipose tissue as an immunological organ: Toll-like receptors,
C1q/TNFs and CTRPs. Trends Immunol. 28:393–399. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Schäffler A and Buechler C: CTRP family:
Linking immunity to metabolism. Trends Endocrinol Metab.
23:194–204. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Friedman JM and Halaas JL: Leptin and the
regulation of body weight in mammals. Nature. 395:763–770. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lennard-Jones JE: Classification of
inflammatory bowel disease. Scand J Gastroenterol Suppl. 170:2–6;
discussion 16–19. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bruun JM, Pedersen SB, Kristensen K and
Richelsen B: Effects of pro-inflammatory cytokines and chemokines
on leptin production in human adipose tissue in vitro. Mol Cell
Endocrinol. 190:91–99. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kirchgessner TG, Uysal KT, Wiesbrock SM,
Marino MW and Hotamisligil GS: Tumor necrosis factor-alpha
contributes to obesity-related hyperleptinemia by regulating leptin
release from adipocytes. J Clin Invest. 100:2777–2782. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Waluga M, Hartleb M, Boryczka G, Kukla M
and Zwirska-Korczala K: Serum adipokines in inflammatory bowel
disease. World J Gastroenterol. 20:6912–6917. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bernstein CN, Eliakim A, Fedail S, Fried
M, Gearry R, Goh KL, Hamid S, Khan AG, Khalif I, Ng SC, et al:
World gastroenterology organisation global guidelines inflammatory
bowel disease: Update August 2015. J Clin Gastroenterol.
50:803–818. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Winawer SJ, Krabshuis J, Lambert R,
O'Brien M and Fried M; World Gastroenterology Organization
Guidelines Committee, : Cascade colorectal cancer screening
guidelines: A global conceptual model. J Clin Gastroenterol.
45:297–300. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
American Society for Gastrointestinal
Endoscopy Standards of Practice Committee, ; Shergill AK, Lightdale
JR, Bruining DH, Acosta RD, Chandrasekhara V, Chathadi KV, Decker
GA, Early DS, Evans JA, et al: The role of endoscopy in
inflammatory bowel disease. Gastrointest Endosc.
81:1101–1121.e1-13. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Travis SP, Schnell D, Krzeski P, Abreu MT,
Altman DG, Colombel JF, Feagan BG, Hanauer SB, Lémann M,
Lichtenstein GR, et al: Developing an instrument to assess the
endoscopic severity of ulcerative colitis: The Ulcerative colitis
endoscopic index of severity (UCEIS). Gut. 61:535–542. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
D'Haens G, Sandborn WJ, Feagan BG, Geboes
K, Hanauer SB, Irvine EJ, Lémann M, Marteau P, Rutgeerts P,
Schölmerich J and Sutherland LR: A review of activity indices and
efficacy end points for clinical trials of medical therapy in
adults with ulcerative colitis. Gastroenterology. 132:763–786.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Barnes EL and Burakoff R: New biomarkers
for diagnosing inflammatory bowel disease and assessing treatment
outcomes. Inflamm Bowel Dis. 22:2956–2965. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang P, Mariman E, Renes J and Keijer J:
The secretory function of adipocytes in the physiology of white
adipose tissue. J Cell Physiol. 216:3–13. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bastard JP, Maachi M, Lagathu C, Kim MJ,
Caron M, Vidal H, Capeau J and Feve B: Recent advances in the
relationship between obesity, inflammation, and insulin resistance.
Eur Cytokine Netw. 17:4–12. 2006.PubMed/NCBI
|
|
30
|
Sobhani I, Bado A, Vissuzaine C, Buyse M,
Kermorgant S, Laigneau JP, Attoub S, Lehy T, Henin D, Mignon M and
Lewin MJ: Leptin secretion and leptin receptor in the human
stomach. Gut. 47:178–183. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Karmiris K, Koutroubakis IE, Xidakis C,
Polychronaki M, Voudouri T and Kouroumalis EA: Circulating levels
of leptin, adiponectin, resistin, and ghrelin in inflammatory bowel
disease. Inflamm Bowel Dis. 12:100–105. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tuzun A, Uygun A, Yesilova Z, Ozel AM,
Erdil A, Yaman H, Bagci S, Gulsen M, Karaeren N and Dagalp K:
Leptin levels in the acute stage of ulcerative colitis. J
Gastroenterol Hepatol. 19:429–432. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ballinger A, Kelly P, Hallyburton E,
Besser R and Farthing M: Plasma leptin in chronic inflammatory
bowel disease and HIV: Implications for the pathogenesis of
anorexia and weight loss. Clin Sci (Lond). 94:479–483. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hoppin AG, Kaplan LM, Zurakowski D,
Leichtner AM and Bousvaros A: Serum leptin in children and young
adults with inflammatory bowel disease. J Pediatr Gastroenterol
Nutr. 26:500–505. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Barbier M, Vidal H, Desreumaux P, Dubuquoy
L, Bourreille A, Colombel JF, Cherbut C and Galmiche JP:
Overexpression of leptin mRNA in mesenteric adipose tissue in
inflammatory bowel diseases. Gastroenterol Clin Biol. 27:987–991.
2003.PubMed/NCBI
|
|
36
|
Paul G, Schäffler A, Neumeier M, Fürst A,
Bataillle F, Buechler C, Müller-Ladner U, Schölmerich J, Rogler G
and Herfarth H: Profiling adipocytokine secretion from creeping fat
in Crohn's disease. Inflamm Bowel Dis. 12:471–477. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Franchimont D, Roland S, Gustot T,
Quertinmont E, Toubouti Y, Gervy MC, Deviere J and Van Gossum A:
Impact of infliximab on serum leptin levels in patients with
Crohn's disease. J Clin Endocrinol Metab. 90:3510–3516. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Bennett BD, Solar GP, Yuan JQ, Mathias J,
Thomas GR and Matthews W: A role for leptin and its cognate
receptor in hematopoiesis. Curr Biol. 6:1170–1180. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Togo M, Tsukamoto K, Satoh H, Hara M,
Futamura A, Nakarai H, Nakahara K and Hashimoto Y: Relationship
between levels of leptin and hemoglobin in Japanese men. Blood.
93:4444–4445. 1999.PubMed/NCBI
|