Introduction
Acute respiratory distress syndrome (ARDS) is a
disease that poses a serious threat to human life and health
(1). After onset, it may cause
oxygen metabolism imbalance of the body and inflammatory cascade
reaction, and activate the body stress response system, thus
leading to the impairment or dysfunction of immune system,
coagulation system, cardiovascular system, liver and kidney
function (2), which eventually leads
to the occurrence of multiple organ failure (3). The effective improvement of the
clinical treatment of these patients, reduction of the body's
inflammatory response and antioxidant response, and improvement of
the oxygen delivery-consumption balance of the body are key and
difficult points in the treatment of ARDS at present (4).
Ulinastatin is mainly isolated and extracted from
the fresh urine of healthy adult males, which, as a kind of
glycoprotein, can effectively improve the stability of lysosomal
membrane and reduce the synthesis and delivery of lysosomal
enzymes, thus scavenging oxygen or hydroxyl radicals, thereby
inhibiting the body's inflammatory response (5,6) and
improving the body's immune capacity (7). Previously, ARDS patients were treated
with mechanical ventilation, but it was mainly used to maintain the
body's respiratory function without significant effects on the
inflammatory and stress response in the body (8). Therefore, in the present study,
ulinastatin combined with mechanical ventilation was mainly
discussed. The results showed that the technique improved oxygen
delivery-consumption balance of body, increased lung function,
reduced the inflammatory and stress response, and improved the
antioxidant capacity.
Materials and methods
General data
Eighty patients with ARDS treated in Yiwu Central
Hospital from January, 2015 to December, 2016 were selected. The
patients were diagnosed via clinical manifestation and pulmonary
blood gas analysis. Patients or their authorized persons signed the
informed consent and the study was approved by the Ethics Committee
of the Yiwu City Centre (Yiwu, China). Patients with acute heart
failure, accompanied with hypovolemic shock, other organ system
failure, systemic immune system diseases or malignant tumor, whose
estimated survival time was within 24 h or who refused to be
enrolled in the study, were excluded.
Patients were divided into the observation (n=40)
and control (n=40) groups according to a random number table. In
the observation group, there were 24 males and 16 females aged
50–79 years, with an average age of 65.6±1.2 years old. In terms of
the causes of disease, there were 17 cases of acute infection, 13
cases of acute trauma, 7 cases of acute poisoning and 3 cases of
other causes. The course of disease was 2–48 h with an average of
8.8±0.3 h. In the control group, there were 25 males and 15 females
aged 50–79 years, with an average age of 65.3±1.3 years. In terms
of the causes of disease, there were 18 cases of acute infection,
12 cases of acute trauma, 8 cases of acute poisoning, and 2 cases
of other causes. The course of disease was of 2–48 h with an
average of 8.7±0.2 h. There were no statistically significant
differences in sex, age, causes and course of disease between the
two groups (P>0.05).
Methods
The patients were treated in view of the primary
disease, such as improving the body's circulatory function,
preventing and treating the disseminated intravascular coagulation
(DIC), using effective antimicrobial treatment and infection
prevention, strengthening the nutrition intervention, and
maintaining water-electrolyte and acid-base balance. The control
group was treated with mechanical ventilation. First, the patients
were treated with pulmonary re-expansion for 10 consecutive
seconds. Then the Respironics 3100B mechanical ventilation
instrument (Sensor Medics, Homestead, FL, USA) was connected with
the airway pressure of 30 cm H2O under the SIMV mode;
the respiratory frequency was set as 5 Hz, the
inspiratory/expiratory ratio was set as 1:2 and the fraction of
inspired oxygen was set as 80–100%, and these parameters were
decreased step by step. The observation group, based on the
treatment of the control group, was treated with the ulinastatin
injection (NMPN H20040476; Guangdong Techpool Biochemical
Pharmaceutical Co., Ltd., Guangdong, China): 200,000 units were
added into 0.9% 100 ml normal saline for intravenous infusion once
every 12 h, and continuous application for 14 days was considered
one course of treatment.
Observational indexes
The changes in relevant indexes of oxygen
metabolism, lung function, time of ventilator treatment, total
hospital stay, and St. George's Respiratory Questionnaire (SGRQ)
score of the two groups after intervention were compared, and the
changes in inflammatory cytokine levels, dopamine receptor-related
hormone levels, superoxide dismutase (SOD), malondialdehyde (MDA)
and the total antioxidant capacity of the two groups before
intervention and at 1 and 4 weeks after intervention were
compared.
Evaluation criteria
Artery blood lactate was detected using whole
spectrophotometry (Beckman and Coulter, Brea, CA, USA), and the
normal value was 0.5–1.7 mmol/l (5–15 mg/day). The oxygen uptake
rate mainly reflected the affinity of hemoglobin and oxygen, and
the normal value was 25–33%. Arterial oxygen content was detected
using enzyme-linked immunosorbent assay (ELISA), and the normal
value was 8.55–9.45 mmol/l. FEV1 was considered the
total gas volume within 1 sec of maximal inspiration after maximal
expiration. SGRQ score was mainly used for the evaluation of
breathing difficulties in the past 4 weeks. There were a total of
76 questions, using the 5-point system and the higher the score,
the worse the respiratory function. Inflammatory factors were
determined using ELISA, including tumor necrosis factor-α (TNF-α)
(adult's reference value, 1–10 ng/ml), interleukin-1 (IL-1)
(adult's reference value, 130–250 ng/ml), IL-6 (adult's reference
value, 67.37–150.33 ng/l) and hs-CRP (adult's reference value,
<10 mg/l). The ELISA antibody-sandwich method was used to
determine the levels of serum cortisol (adult's reference value,
80–550 nmol/l), epinephrine (adult's reference value, within 480
pmol/l) and norepinephrine (adult's reference value, 615–3240
pmol/l). Oxidative stress factors were detected using a 450
full-automatic biochemical detector (Bio-Rad, Hercules, CA, USA),
including MDA (normal reference value, 3.52–4.78 nmol/ml), SOD
(normal reference value, 0.242–0.620 µU/ml). The activity of SOD
was measured using the Web Standard Tools (WST) method, the level
of MDA was measured using the thiobarbituric acid (TBA) method, and
the total antioxidant capacity of femoral venous blood was detected
using fluorescence recovery after the photobleaching (FRAP) method.
The total antioxidant capacity is the sum of large- and
small-molecule antioxidases, detected using the FRAP method, and
its normal value was 2.34–26.96 µU/ml.
Statistical analysis
Statistical Product and Service Solutions (SPSS) ±
13.0 was used to analyze the data. Measurement data were presented
as mean ± standard deviation (SD). The t-test was used for the
comparison of means between the two groups, and the Chi-square test
was used for the comparison of rate between the two groups.
P<0.05 indicated that the difference was statistically
significant.
Results
Comparisons of oxygen
metabolism-related indexes after intervention between the two
groups
After intervention, the arterial blood lactate in
the observation group was significantly lower than that in the
control group (P<0.05), the oxygen uptake rate was significantly
higher than that in the control group (P<0.05), and the arterial
oxygen content was significantly higher than that in the control
group (P<0.05) (Table I).
 | Table I.Comparisons of oxygen
metabolism-related indexes after intervention between the two
groups (mean ± SD). |
Table I.
Comparisons of oxygen
metabolism-related indexes after intervention between the two
groups (mean ± SD).
| Item | Arterial blood
lactate (mmol/l) | Oxygen uptake rate
(%) | Arterial oxygen
content (ml/l) |
|---|
| Observation
group | 2.1±0.2 | 33.3±2.4 | 156.5±10.5 |
| Control group | 3.9±0.3 | 25.6±1.7 | 89.9±5.1 |
| t-value | 31.574 | 16.558 | 36.084 |
| P-value |
0.000 |
0.000 |
0.000 |
Comparison of lung function after
intervention
In the lung function indexes, the FEV1
and FEV1/FVC levels in the observation group were larger
than those in the control group (P<0.05) (Table II).
| Table II.Comparison of lung function after
intervention (mean ± SD). |
Table II.
Comparison of lung function after
intervention (mean ± SD).
| Item | FEV1
(%) |
FEV1/FVC |
|---|
| Observation
group | 58.2±1.2 | 41.7±2.3 |
| Control group | 42.1±3.0 | 61.0±3.2 |
| t-value | 31.514 | 30.974 |
| P-value |
0.000 |
0.000 |
Comparisons of duration of ventilator
treatment and total hospital stay of all the subjects
The duration of ventilator treatment in the
observation group was significantly shorter than that of the
control group (P<0.05). In addition, the hospital stay was
significantly less in the observation group than that in the
control group (P<0.05) (Table
III).
| Table III.Comparisons of duration of ventilator
treatment and total hospital stay of all the subjects (d, mean ±
SD). |
Table III.
Comparisons of duration of ventilator
treatment and total hospital stay of all the subjects (d, mean ±
SD).
| Item | Ventilator
support | Hospital stay |
|---|
| Observation
group | 3.0±0.1 | 31.9±3.6 |
| Control group | 4.7±0.3 | 42.3±5.1 |
| t-value | 34.000 | 10.537 |
| P-value |
0.000 |
0.000 |
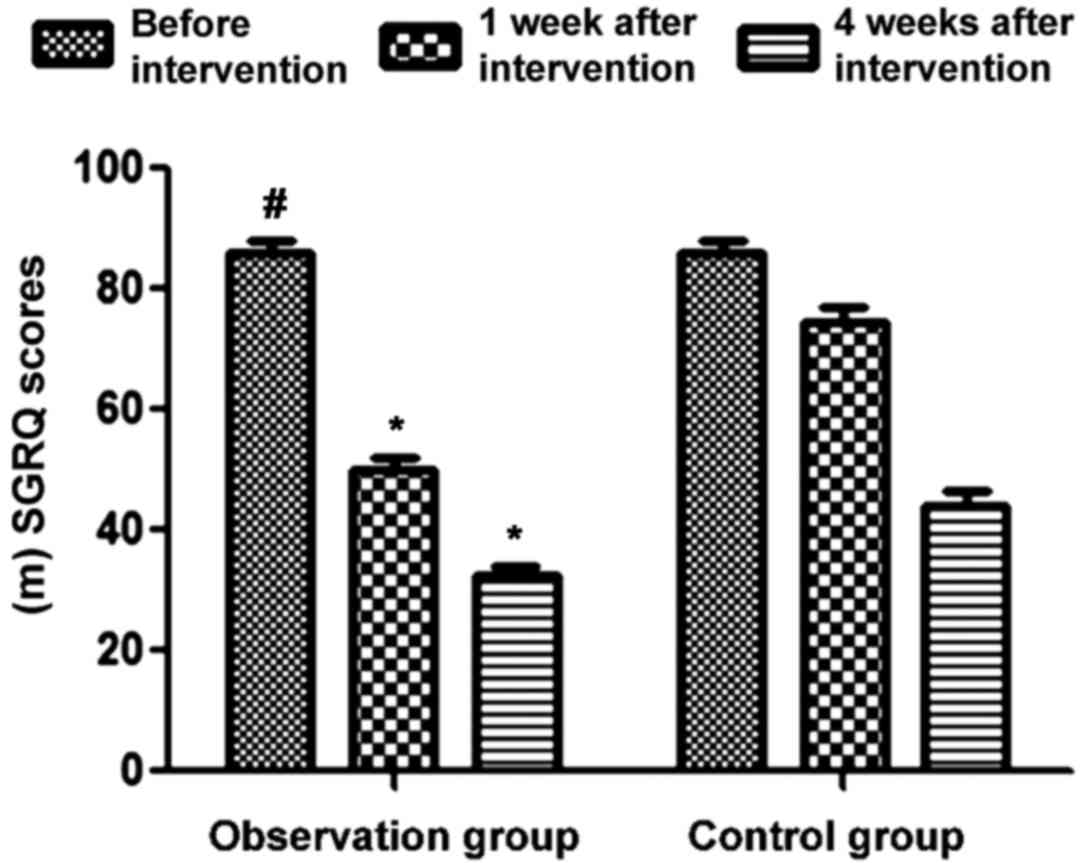
Comparison of changes in SGRQ scores
during intervention
Prior to intervention, the SGRQ scores in the two
groups were not statistically significant (P>0.05). At 1 and 4
weeks after intervention, the SGRQ scores of the observation group
were significantly decreased compared to those of the control group
(P<0.05) (Table IV and Fig. 1).
| Table IV.Comparison of changes in the SGRQ
scores during intervention (point, mean ± SD). |
Table IV.
Comparison of changes in the SGRQ
scores during intervention (point, mean ± SD).
| Item | Before
intervention | At 1 week after
intervention | At 4 weeks after
intervention |
|---|
| Observation
group | 85.9±2.3 | 50.3±1.6 | 32.7±1.3 |
| Control group | 86.0±2.3 | 74.6±2.4 | 44.3±2.1 |
| t-value | 0.194 | 53.281 | 29.705 |
| P-value | 0.846 |
0.000 |
0.000 |
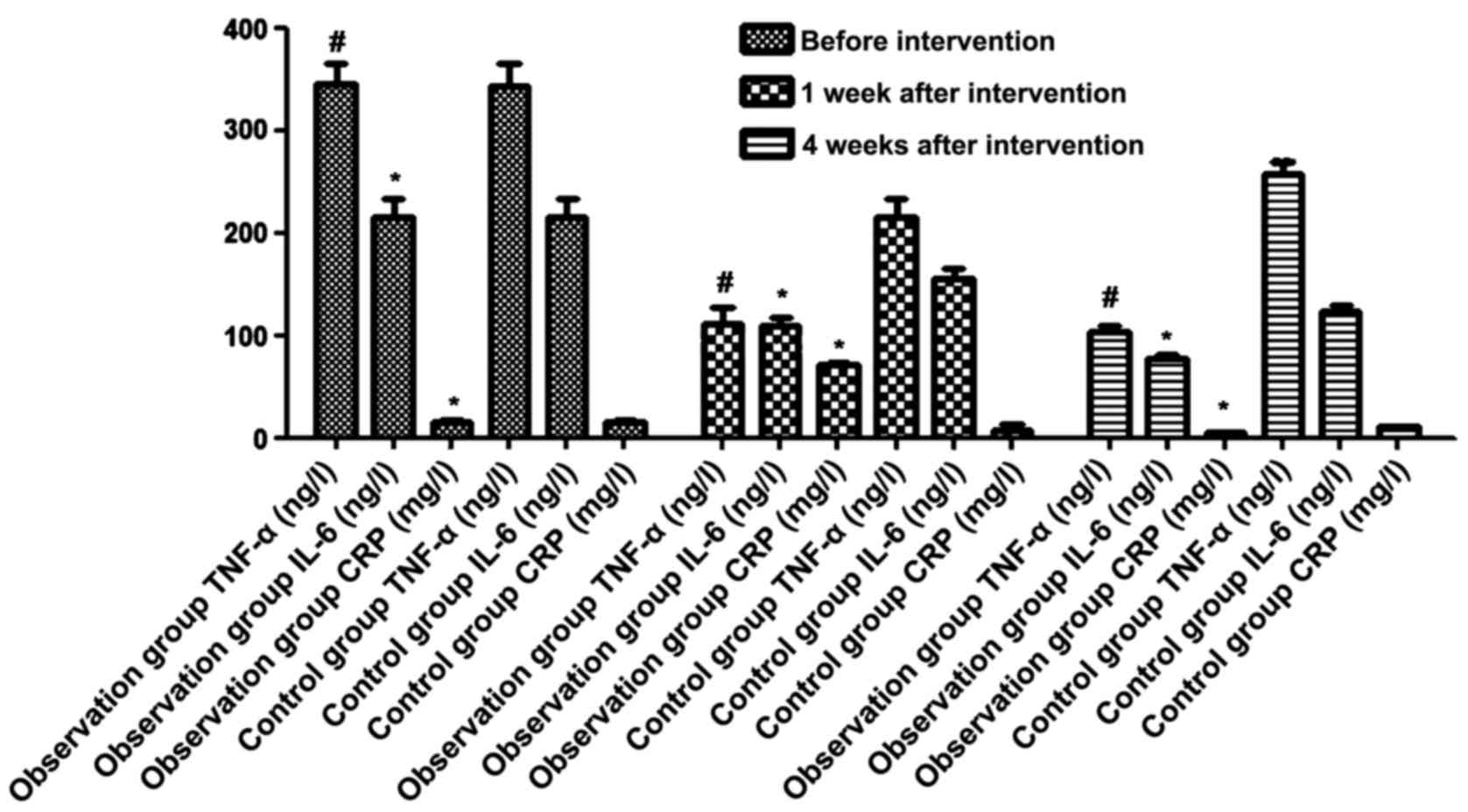
Changes in inflammatory cytokine
levels during intervention
There were no statistically significant differences
in the levels of TNF-α, IL-6 and CRP between the two groups before
intervention (P>0.05). At 1 and 4 weeks after intervention, the
levels of TNF-α in the observation group were 113.1±14.5 and
105.0±5.0 ng/l, the levels of IL-6 were 110.4±7.4 and 79.0±3.1
ng/l, and the levels of CRP were 7.20±0.3 and 6.0±0.1 mg/l, which
were significantly lower than those in control group, except CRP
levels at 1 week (P<0.05) (Fig.
2).
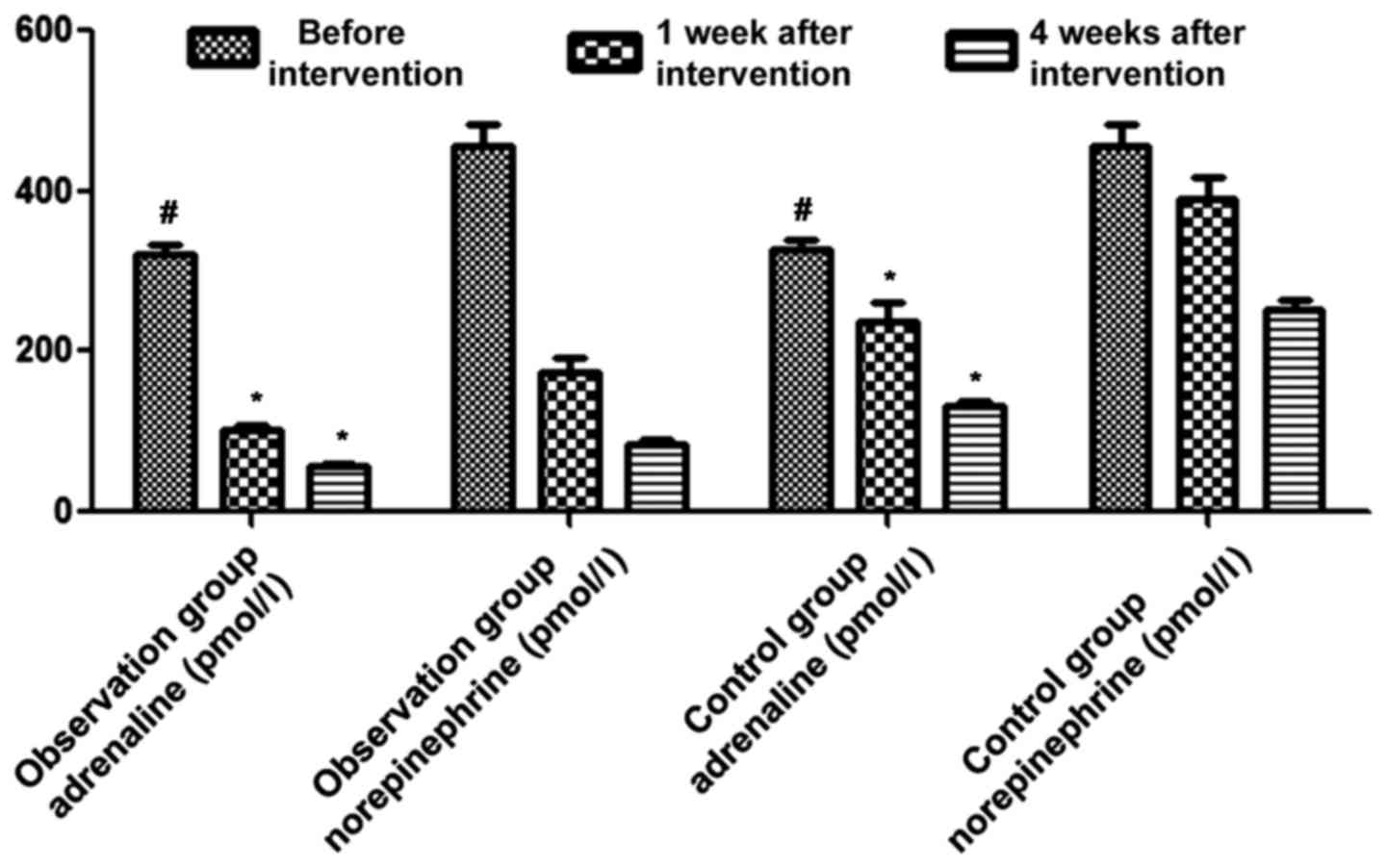
Changes in dopamine receptor-related
hormone levels of the two groups during intervention
There were no statistically significant differences
in adrenaline and norepinephrine levels between the two groups
before intervention (P>0.05). At 1 and 4 weeks after
intervention, the levels of adrenaline in the observation group
were 103.2±6.4 and 58.0±2.1 pmol/l, respectively, and the levels of
norepinephrine were 174.7±17.9 and 84.5±6.1 pmol/l, respectively,
which were significantly lower than those in the control group
(P<0.05) (Fig. 3).
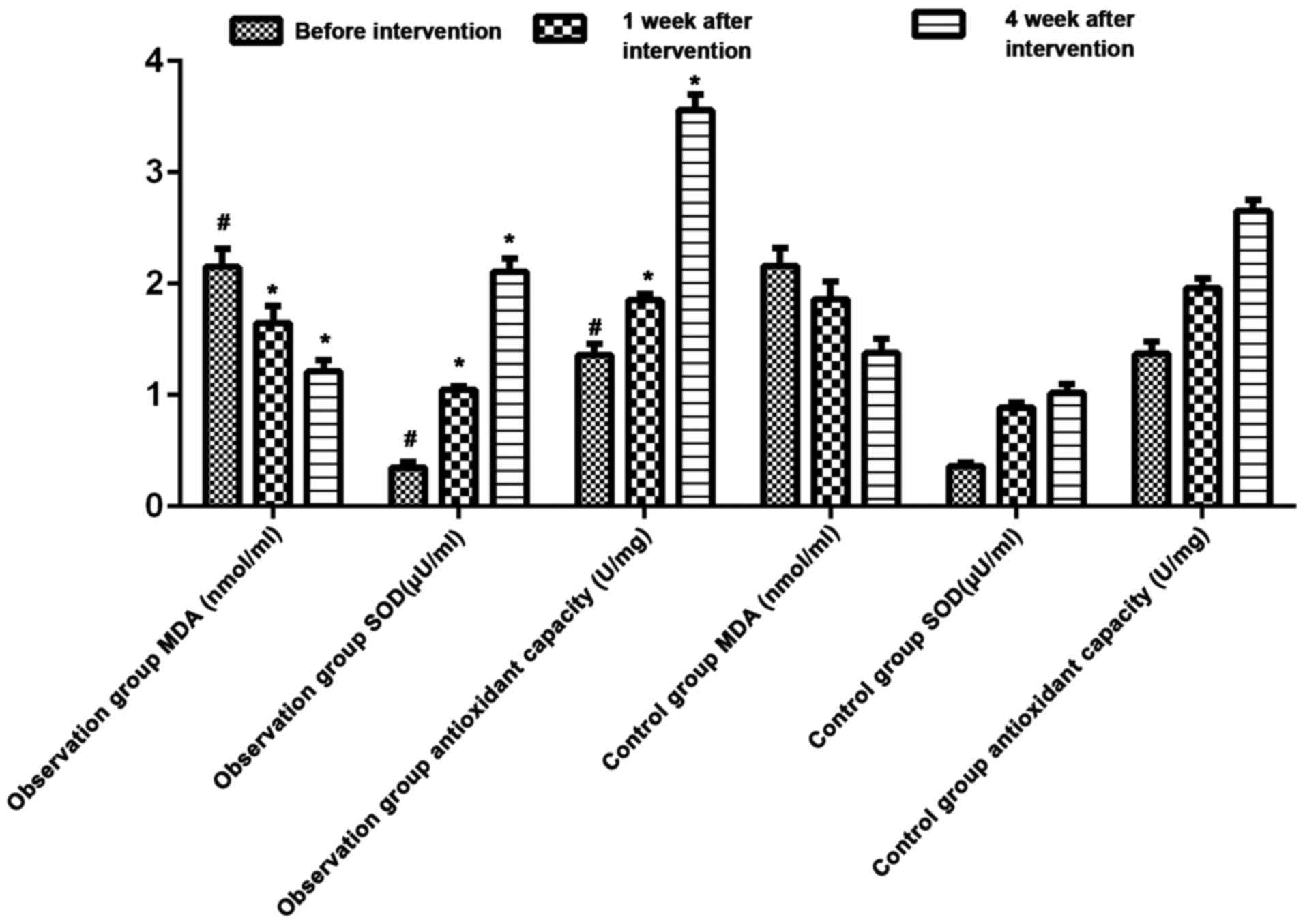
Comparisons of SOD, MDA, and the total
antioxidant capacity between the two groups during
intervention
There were no statistically significant differences
in MDA, SOD and the total antioxidant capacity between the two
groups before intervention (P>0.05). At 1 and 4 weeks after
intervention, the levels of MDA in the observation group were
1.65±0.15 and 1.21±0.11 nmol/ml, the levels of SOD were 1.36±0.11
and 0.35±0.05 µU/ml, and the total antioxidant capacity was
2.11±0.12 and 3.56±0.14 U/mg, which were significantly increased to
those in the control group (P<0.05) (Fig. 4).
Discussion
ARDS is caused by a variety of primary diseases,
which mainly manifest in progressive hypoxia and respiratory
failure (9). Its pathological
feature is primarily diffuse alveolar epithelial cell and pulmonary
microvascular endothelial cell damage, mostly accompanied with
severe pulmonary edema and the formation of pulmonary hyaline
membranes. With disease progression, the lung volume is
significantly reduced, lung compliance is decreased, and
ventilation/blood flow ratio is out of balance (10). The imbalance of oxygen metabolism,
inflammatory response and antioxidant capacity disorder are
important links in the occurrence and development of ARDS (11). High-frequency oscillatory ventilation
ventilates through the high airway positive pressure circuit formed
by the high speed continuous air flow, which is repeatedly
superimposed by the shock wave formed by the piston device, thus
reducing the gas and CO2 retention in the normal
breathing support (12), thereby
significantly improving the respiratory support effect. However,
single application of mechanical ventilation is mainly used to
improve the respiratory function of patients with ARDS, but has no
significant effect on the body's inflammatory response and stress
response (13). Thus, ulinastatin
and mechanical ventilation were combined.
Findings of the present study showed that after
intervention, the arterial blood lactate in the observation group
was significantly lower than that in the control group, the oxygen
uptake rate was significantly higher than that in the control
group, and the arterial oxygen content was significantly higher
than that in the control group. In the lung function indexes,
FEV1 and FEV1/FVC level in the observation group were
larger than those in the control group, suggesting that the
application of ulinastatin in ARDS patients can significantly
improve the body's oxygen supply-demand balance, improve the lung
function, reduce the lactic acid accumulation and improve the
patients' prognosis. In addition, the duration of ventilator
treatment was significantly shorter than that in the control group
and the hospital stay was significantly less than that in the
control group. At 1 and 4 weeks after intervention, the SGRQ scores
of the observation group were significantly increased compared to
those of the control group, further suggesting that the application
of ulinastatin in ARDS patients is important for shortening the
duration of ventilator treatment and hospital stay and improving
the overall respiratory function of patients. At the same time, the
levels of TNF-α, IL-6 and CRP were significantly lower than those
of the control group at 1 and 4 weeks after intervention,
suggesting that the application of ulinastatin in ARDS patients can
decrease the body's inflammatory cytokines. Finally, at 1 and 4
weeks after intervention, the levels of adrenaline and
norepinephrine’ were significantly lower than those of the control
group, while the level of SOD and total antioxidant capacity were
significantly increased compared to those of the control group,
indicating that the application of ulinastatin in ARDS patients has
a positive significance in reducing the oxygen-free radical damage
and decreasing the stress response.
Ulinastatin, as a kind of broad-spectrum protease
inhibitor, can effectively inhibit the activity of inflammatory
factors and reduce their levels, thus playing a role in protecting
the body organs and system (14).
Its intravenous administration can effectively inhibit a variety of
cell proteolytic enzymes in the body (15), reduce the damage of hydrolase to
normal tissues, stabilize the intracellular lysosomal membrane, and
reduce the body peroxidation reaction by inhibiting the production
of peroxide, thus inhibiting the inflammatory response (16). In addition, ulinastatin can inhibit
the proteolytic enzyme activity widely and improve body
microcirculation and tissue perfusion functions (17). The stability of intracellular
lysosomal membrane (18) can help
improve the organelle mitochondrial activity, improve cell
respiration (19), enhance cell
elastinase activity, and remove the body oxygen or hydroxyl-free
radicals (20).
In conclusion, the application of ulinastatin
combined with mechanical ventilation in ARDS patients is of great
significance in improving the oxygen delivery-consumption balance
of the body, increasing lung function, reducing the inflammatory
and stress response and improving the antioxidant capacity.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wang L, Huang X, Kong G, Xu H, Li J, Hao
D, Wang T, Han S, Han C, Sun Y, et al: Ulinastatin attenuates
pulmonary endothelial glycocalyx damage and inhibits endothelial
heparanase activity in LPS-induced ARDS. Biochem Biophys Res
Commun. 478:669–675. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Qiu Y, Lin J, Yang Y, Zhou J, Gong LN, Qin
Z and Du L: Lack of efficacy of ulinastatin therapy during
cardiopulmonary Bypass surgery. Chin Med J (Engl). 128:3138–3142.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sun R, Li Y, Chen W, Zhang F and Li T:
Total ginsenosides synergize with ulinastatin against septic acute
lung injury and acute respiratory distress syndrome. Int J Clin Exp
Pathol. 8:7385–7390. 2015.PubMed/NCBI
|
|
4
|
Leng YX, Yang SG, Song YH, Zhu X and Yao
GQ: Ulinastatin for acute lung injury and acute respiratory
distress syndrome: A systematic review and meta-analysis. World J
Crit Care Med. 3:34–41. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yuan S: Drugs to cure avian influenza
infection-multiple ways to prevent cell death. Cell Death Dis.
3:4835–4839. 2013.
|
|
6
|
Sekine Y and Ko E: The influence of
intraoperative oxygen inhalation on patients with idiopathic
pulmonary fibrosis. Masui. 60:307–313. 2011.(In Japanese).
PubMed/NCBI
|
|
7
|
Zhou LW, Wang YL, Yan XT and He XH:
Urinary trypsin inhibitor treatment ameliorates acute lung and
liver injury resulting from sepsis in a rat model. Saudi Med J.
29:368–373. 2008.PubMed/NCBI
|
|
8
|
Nakanishi K, Takeda S, Sakamoto A and
Kitamura A: Effects of ulinastatin treatment on the cardiopulmonary
bypass-induced hemodynamic instability and pulmonary dysfunction.
Crit Care Med. 34:1351–1357. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Inoue K, Takano H, Yanagisawa R, Sakurai
M, Shimada A, Sato H, Kato Y and Yoshikawa T: Antioxidative role of
urinary trypsin inhibitor in acute lung injury induced by
lipopolysaccharide. Int J Mol Med. 16:1029–1033. 2005.PubMed/NCBI
|
|
10
|
Inoue K, Takano H, Yanagisawa R, Sakurai
M, Shimada A, Yoshino S, Sato H and Yoshikawa T: Protective role of
urinary trypsin inhibitor in acute lung injury induced by
lipopolysaccharide. Exp Biol Med (Maywood). 230:281–287. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ito K, Mizutani A, Kira S, Mori M, Iwasaka
H and Noguchi T: Effect of ulinastatin, a human urinary trypsin
inhibitor, on the oleic acid-induced acute lung injury in rats via
the inhibition of activated leukocytes. Injury. 36:387–394. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gaudry S, Tuffet S, Lukaszewicz AC,
Laplace C, Zucman N, Pocard M, Costaglioli B, Msika S, Duranteau J,
Payen D, et al: Prone positioning in acute respiratory distress
syndrome after abdominal surgery: a multicenter retrospective
study: SAPRONADONF (Study of Ards and PRONe position After
abDOmiNal surgery in France). Ann Intensive Care. 7:212017.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Iii Fowler AA, Kim C, Lepler L, Malhotra
R, Debesa O, Natarajan R, Fisher BJ, Syed A, DeWilde C, Priday A,
et al: Intravenous vitamin C as adjunctive therapy for
enterovirus/rhinovirus induced acute respiratory distress syndrome.
World J Crit Care Med. 6:85–90. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Albert M, Corsilli D, Williamson DR,
Brosseau M, Bellemare P, Delisle S, Nguyen AQ and Varin F:
Comparison of inhaled milrinone, nitric oxide and prostacyclin in
acute respiratory distress syndrome. World J Crit Care Med.
6:74–78. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang T, Hou W and Fu Z: Preventative
effect of OMZ-SPT on lipopolysaccharide-induced acute lung injury
and inflammation via nuclear factor-kappa B signaling in mice.
Biochem Biophys Res Commun. 485:284–289. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ni YN, Luo J, Yu H, Wang YW, Hu YH, Liu D,
Liang BM and Liang ZA: Can body mass index predict clinical
outcomes for patients with acute lung injury/acute respiratory
distress syndrome? A meta-analysis. Crit Care. 21:362017.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Holopainen S, Hytönen MK, Syrjä P,
Arumilli M, Järvinen AK, Rajamäki M and Lohi H: ANLN truncation
causes a familial fatal acute respiratory distress syndrome in
Dalmatian dogs. PLoS Genet. 13:e10066252017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bolaki M, Amargianitakis V, Georgopoulos
D, Guervilly C and Papazian L: Effects of neuromuscular blockers on
transpulmonary pressures in moderate to severe acute respiratory
distress syndrome. Intensive Care Med. 43:600–601. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Takeshima M, Ishikawa H and Shimizu T:
Acute respiratory distress syndrome and lamotrigine: A case report.
Psychosomatics. 18:331–382. 2016.
|
|
20
|
Mohamed HS and Meguid MM: Effect of
nebulized budesonide on respiratory mechanics and oxygenation in
acute lung injury/acute respiratory distress syndrome: Randomized
controlled study. Saudi J Anaesth. 11:9–14. 2017. View Article : Google Scholar : PubMed/NCBI
|