Introduction
Stem cells have inherent chondrogenic potential and
serve an important role in healing articular cartilage defects
(1). Bone marrow stem cells, which
may be obtained by stimulation techniques and by subchondral
drilling, have been demonstrated to improve the cartilage healing
process; however, these methods result in a fibrocartilage-like
tissue that deteriorates over time (2). Other techniques, including autologous
chondrocyte implantation, have been used to improve the quality of
the repaired tissue to make it more similar to hyaline-like
cartilage tissue (3). However,
long-term follow-up has identified similar results in terms of
clinical outcome and histological scoring between microfracture and
autologous chondrocyte implantation techniques (3).
During articular cartilage repair, paracrine factors
may influence the inflammatory process involved in fibrocartilage
tissue formation. Hyaluronic acid, stem cells and growth factors
(GFs) have provided important results with regards to the
suppression of inflammatory process (4) and may act synergistically in cartilage
regeneration (5,6). Notably, experimental cartilage repair
studies have demonstrated promising results when combining
subchondral drilling with postoperative intraarticular injections
of autologous bone marrow aspirate and hyaluronic acid (4). Synovitis and synovial fluid alterations
as a response to the inflammatory process has also been indicated
to influence the articular environment and may affect cartilage
repair (7).
The use of platelet-rich plasma (PRP), a rich source
of autologous GFs, may be considered a useful approach for
cartilage repair (8). Platelets
serve a crucial role in the normal healing response of connective
tissues through the local secretion of GFs and recruitment of
reparative cells (9). PRP is a
potential scaffold option for tissue regeneration: It has been
suggested for the stimulation of chondrogenic differentiation and
proliferation of stem cells, chondrocyte proliferation and
cartilage formation (10–12).
The type of stem cell may influence the quality of
tissue repair (13). Human dental
pulp stem cell (hDPSC) subpopulations have been demonstrated to
have substantial angiogenic, neurogenic and regenerative potential
when compared with other stem cell sources (14,15).
The purpose of the present study was to evaluate the
potential of hDPSCs in a PRP scaffold to regenerate full-thickness
articular cartilage defects in rabbits. It was hypothesized that
hDPSCs in a PRP scaffold may improve articular cartilage
repair.
Materials and methods
A total of 32 New Zealand male rabbits (obtained
from the Department of coordinating production and maintenance of
rabbits, Serviço de Biotério, Prefeitura do Campus da USP
(Universidade de São Paulo) (aged 4–6 months, weighing ~3 kg) were
used in the present study. Rabbits were maintained in standardized
individual cages, at a temperature of ~21°C, a humidity of 45–55%
and a 12–14/24 h light/dark cycle. Additionally, rabbits and
received ad libitum access to ground solid rations (Anderson
and Clayton S.A.) and water. A total of 30 rabbits comprised the
experimental group (60 knees), and 2 rabbits were used to obtain
PRP. The study protocol of the present experiment was reviewed and
approved by the Ethics Committee at Faculdade de Medicina de
Marília, São Paulo, Brazil (EC No. 641/12).
hDPSC isolation and culture
Dental pulp cells were extracted from one tooth that
had been previously selected for exodontia from a healthy 10 year
old female patient at a private dental clinic, on June 2006
(16). Cells were extracted using
endodontic files under a biosafety hood and placed in culture
flasks with Dulbecco's modified Eagle's medium (DMEM) supplemented
with 10% fetal bovine serum (Cultilab, Campinas, SP, Brazil) and 50
mg/ml gentamicin at 37°C in an atmosphere containing 5%
CO2 as previously described by Jesus et al (2011)
(16). The growth medium was changed
every 3 days. Once cells reached confluence, the cells were
dissociated with 0.25% trypsin (Gibco, Thermo Fisher Scientific,
Inc., Waltham, MA, USA). Some of the cells were separated for
cryopreservation. A maximum of 106−107 cells
per tube were observed and a final volume of 1 ml was then achieved
through the addition of DMEM medium supplemented with 10% fetal
bovine serum 900 µl (cat. no. 12657029; Gibco; Thermo Fisher
Scientific, Inc.) and dimethyl sulfoxide (100 µl; Sigma-Aldrich;
Merck KGaA, Darmstadt, Germany). Cryopreservation tubes were then
subjected to cryostat reduction for 24 h at −80°C and then stored
in liquid nitrogen (−196°C). The procedures were performed in the
Center for Biotechnology and Cell Therapy, Monte Tabor Hospital São
Rafael (Salvador, Brazil).
Flow cytometry
Adherent cells in the sixth passage (P6) and
cultures with 60% confluence were selected for the detection of
surface and intracellular antigens. Antibody staining was performed
as follows: Cell aliquot (100 µl) containing at least
106 nucleated cells were placed into each tube and
incubated for 30 min at room temperature with 0.5% PBS/BSA
(Sigma-Aldrich, Merck KGaA) for blocking. Samples were then stained
with conjugated antibodies (all 1:100) for 15 min at room
temperature in the dark. Subsequently cells were resuspended twice
in 4 ml PBS (Sigma-Aldrich) and centrifuged at a speed of 540 × g
for 5 min at 4°C. Following centrifugation, the supernatant was
discarded and the cell pellet was ressuspended in 500 µl PBS + 0.5%
BSA and stored at 4°C. The antibodies used are listed in Table I. Data acquisition and analysis were
performed using a FACS Calibur flow cytometer (BD Biosciences) and
the Cell Quest program version 5.2 (BD Biosciences). At least
50,000 events were collected and analyzed. Unlabeled antibodies
cells were used as controls.
 | Table I.List of antibodies used for flow
cytometry. |
Table I.
List of antibodies used for flow
cytometry.
| Antibody | Source | Supplier/cat.
no. |
|---|
| CD44-FITC | Mouse clone
L178 | BD Biosciences, San
Jose, CA, USA/347943 |
| CD90-FITC | Mouse clone
5E10 | BD Biosciences, San
Jose, CA, USA/555595 |
| CD73-PE | Mouse clone
AD2 | BD Biosciences, San
Jose, CA, USA/550257 |
| CD34-PE | Mouse clone
8G12 | BD Biosciences, San
Jose, CA, USA/348057 |
| CD45-APC | Mouse clone
2D1 | BD Biosciences, San
Jose, CA, USA/340942 |
| CD105-FITC | Mouse clone
166707 | R&DSystems,
Inc., Minneapolis, MN, USA/FAB10971F |
| CD117-PE-CY5 | Mouse clone
YB5.B8 | BD Biosciences, San
Jose, CA, USA/559879 |
| CD133-PE | Mouse
monoclonal |
Miltenyi/120-000-425 |
| CD166-PE | Mouse clone
3A6 | BD Biosciences, San
Jose, CA, USA/559263 |
| CD54-PE-CY5 | Mouse clone
HA58 | BD Biosciences, San
Jose, CA, USA/555512 |
| STRO-1 | Mouse
monoclonal | R&DSystems,
Inc., Minneapolis, MN, USA/MAB1038 |
| CD31- FITC | Mouse clone
WM59 | BD Biosciences, San
Jose, CA, USA/555445 |
Immunofluorescence
hDPSCs from P6 were used for phenotypic
characterization using immunofluorescence. Cells were trypsinized
and seeded in 24-well plates containing 13 mm glass coverslips
(Waldemar Knittel Glasbearbeitungs GmbH, Braunschweig, Germany).
Following adherence for 24 h, the culture medium was removed and
two washes with PBS were performed. Cells were fixed with 4%
paraformaldehyde for 20 min at room temperature. Two wells were
then washed with PBS for 3 min. For the staining of nuclear
antigens, cells were permeabilized with 0.1% Triton X-100 for 10
min at room temperature. Blocking was then performed with 5%
PBS/BSA (Sigma-Aldrich) for 30 min at room temperature and
incubated overnight at 4°C with the following primary antibodies:
Anti-CD44 (1:100; cat. no. 08-0184; Zymed; Thermo Fisher
Scientific, Inc.), anti-cluster of differentiation (CD)45 (1:100;
cat. no. AHS4552; BioSource; Thermo Fisher Scientific, Inc.)
anti-CD90 (1:100; cat. no. 550402; BD Bioscences), anti-CD105
(1:100; cat. no. 555690; BD Bioscences) anti-CD73 (1:100; cat. no.
550738; BD Bioscences), anti-CD117 (1:100; cat. no. ab16832; Abcam,
Cambridge, MA, USA), anti-CD133 (1:25; cat. no. ab19898; Abcam)
anti-myosin (1:100; cat. no. M7523; Sigma-Aldrich), anti-collagen
type I (1:50; cat. no. sc-8788; Santa Cruz Biotechnology Inc.,
Dallas, TX, USA), anti-glial fibrillary acidic protein (1:50; cat.
no. Z0334; Dako; Agilent Technologies, Inc., Santa Clara, CA, USA)
and anti-myelin (1:100; cat. no. 18-0038; Zymed; Thermo Fisher
Scientific, Inc.). Slides were visualized and images were captured
using a confocal microscope (magnification, ×400; FluoView 1000;
Olympus, Tokyo, Japan).
Cytogenetic analysis
hDPSCs were prepared for cytogenetic analysis as
previously described and analyzed using the G-banding technique
(17). Slides were observed using an
optical microscope (magnification, ×1,000) and ~20 metaphases of
each sample were analyzed for the presence of numerical and/or
structural cytogenetic abnormalities according to the International
System for Chromosome Nomenclature (18). Images were captured using Image-Pro
Plus software, version 7.0 (Media Cybernetics, Inc., Rockville, MD,
USA). All cells obtained from P5 and P6 demonstrated a normal
female karyotype (karyotype: 46, XX) (18).
Obtaining and preparing PRP
PRP was obtained from 2 adult New Zealand rabbits
(age, 4–6 months; weight, ~3–5 kg). The animals underwent general
anesthesia by administering an intramuscular injection of 10 mg/kg
xylazine hydrochloride (VET Brands International, Inc., Miramar,
FL, USA) followed by an intramuscular injection of 30 mg/kg
ketamine hydrochloride (VET Brands International, Inc.). Animals
were deemed to be anesthetized when the following parameters were
observed: The presence of muscular paralysis, the absence of
reflexes and pain. These animals were not used in the experimental
groups and following blood extraction, rabbits were euthanized with
an overdose (20 mg/kg) of Propofol (Cristália Produtos Químicos
Farmacêuticos Ltda., Itapira, São Paulo, Brazil) administered by
intravenous injection. Death was confirmed by the lack of a
heartbeat, lack of respiration, lack of corneal reflex and the
presence of rigor mortis. Cardiac puncture and blood extraction
were performed with a 10-ml disposable syringe containing 1 ml 3.2%
sodium citrate and a 30×8 mm needle. A total of 9 ml of arterial
blood was collected in each syringe and a total of 18 ml of
arterial blood was obtained to prepare the PRP. Following
collection, the blood was homogenized and transferred to collection
tubes (BD Vacutainer; BD Biosciences).
The collected tubes containing the blood were
subjected to two centrifugation steps, the first of which was
performed at 200 × g for 10 min at 24°C to separate the blood
cells. The supernatant plasma and buffy coat were transferred to a
new sterile tube and underwent a second centrifugation step at 400
× g for 10 min at 24°C. The collected plasma underwent a further
centrifugation step at 400 × g for 10 min at 24°C to concentrate
the platelets to ~1,000,000 per µl. Subsequently, the supernatant
was removed to achieve a final volume of 1,600 µl of PRP for every
9 ml of arterial blood. PRP was separated into two 800-µl aliquots,
placed into sterile cryotubes and stored in a freezer at −80°C for
subsequent experiments. A sample was obtained for platelet
counting, which was performed manually using a hemocytometer
(Hausser Scientific, Horsham, PA, USA) and was used as a control in
order to ensure the minimum concentration of platelets was
1,000,000 per µl.
Prior to the surgical procedure, hDPSCs were
grown in α-MEM medium (Gibco; Thermo Fisher Scientific, Inc.)
supplemented with 10% fetal bovine serum (Gibco; Thermo Fisher
Scientific, Inc.) at 37°C and 5% CO2 until 80% confluent
cultures were obtained. Cells were then detached from the growth
surface with 0.25% trypsin (Gibco; Thermo Fisher Scientific, Inc.)
and immediately transferred to a tube containing α-MEM medium
(supplemented with 10% fetal bovine serum. Samples were centrifuged
twice at 175 × g for 10 min at room temperature and the supernatant
was removed. Then, PRP was thawed completely, homogenized, divided
into 200-µl samples and added to 2,8×106 hDPSCs (P5 and
P6). The PRP thawing procedure and preparation of the cells was
synchronized with the start of surgery and maintained for
approximately 10–15 min at room temperature (23–25°C).
Cell viability
hDPSCs were suspended in PRP and stained with
blue tripan reagent (1.6%; v/v; Sigma-Aldrich; Merck KGaA; cat. no.
T6146) for 1 min at room temperature and cell viability of ~80% was
confirmed by the manual counting technique using a hemocytometer
(Hausser Scientific, Horsham, PA, USA).
Surgical procedure and experimental
groups
Rabbits received general anesthesia with of 10 mg/kg
intramuscular xylazine hydrochloride (Vet Brands International,
Inc., Miramar, FL, USA) followed by an intramuscular injection of
30 mg/kg ketamine hydrochloride (Vet Brands International, Inc.,
Miramar, FL, USA). Each rabbit's right and left knees were shaved
and the overlying fur was removed. Antisepsis was performed with
10% polyvinylpyrrolidone topical solution (RioquímicaIndústria
Farmaceutica, São José do Rio Preto, Brazil). An incision was made
on the anteromedial section of the knees and the patella was
dislocated laterally to expose the patellar groove of the femur.
Full-thickness cartilage defects (5×5 mm) down to the subchondral
bone were created in the patellar groove using an odontologycal
surgical motor for dental implants (Gnatus Produtos Médicos e
Odontológicos Ltda EPP, São Paulo, Brazil) quipped with a 5-mm
diameter trephine drill and constant irrigation with 0.9% saline
solution (Fig. 1A).
Rabbits were allocated into three experimental
groups: Control (CTL), PRP and PRP with stem cells (PRP+SC) groups.
Both knees of each rabbit were operated on and the 5 mm critical
defects were created. In the CTL group, the defects received no
further treatment. In the PRP group, the defects in both knees were
filled with 100 µl of PRP gel activated with 10% calcium gluconate
(Fresenius Kabi Brasil Ltda, Barueri, São Paulo, Brazil). In the
PRP+SC group, the defects in both knees were filled with
1.4×106 hDPSCs resuspended in 100 µl of PRP gel
activated with 10% calcium gluconate (Fig. 1B and C). The patella was carefully
repositioned and the capsule and skin were closed with 4-0 nylon
sutures in all of the operated knees. In each group, 5 rabbits were
euthanized at 6 weeks and 5 were euthanized at 12 weeks
post-surgery.
Macroscopic evaluation
Macroscopic evaluation of cartilage repair was
performed at 6 and 12 weeks by two independent observers. The
International Cartilage Repair Society (ICRS) evaluation grading
system was used as indicated in Table
II (19,20).
| Table II.International Cartilage Repair
Society macroscopic evaluation of cartilage repair. |
Table II.
International Cartilage Repair
Society macroscopic evaluation of cartilage repair.
| Variable | Score |
|---|
| Degree of defect
repair |
|
| In
level with surrounding cartilage | 4 |
| 75%
repair of defect depth | 3 |
| 50%
repair of defect depth | 2 |
| 25%
repair of defect depth | 1 |
| 0%
repair of defect depth | 0 |
| Integration to
border zone |
|
|
Complete integration with
surrounding cartilage | 4 |
|
Demarcating border <1
mm | 3 |
| 3/4 of
graft integrated, 1/4 with a notable border >1 mm in width | 2 |
| 1/2 of
graft integrated with surrounding cartilage, 1/2 with a notable
border >1 mm | 1 |
| From no
contact to 1/4 of graft integrated with surrounding cartilage | 0 |
| Macroscopic
appearance |
|
| Intact
smooth surface | 4 |
|
Fibrillated surface | 3 |
| Small,
scattered fissures or cracks | 2 |
| Several
small or few large fissures | 1 |
| Total
degeneration of grafted area | 0 |
| Total overall
repair assessment |
|
| Grade
I: Normal | 12 |
| Grade
II: Nearly normal | 8–11 |
| Grade
III: Abnormal | 4–7 |
| Grade
IV: Severely abnormal | 1–3 |
Histological cartilage evaluation
The distal femur was removed, placed in 10%
formalin, decalcified in EDTA, embedded in paraffin and sagittally
cut into 5-µm thick sections. Sections were stained with
hematoxylin and eosin (H&E) and a Masson-Goldner kit was used
for histomorphometric tissue analysis. The microscopic evaluations
were performed by two different researchers and scored according to
a modified version of the grading system developed by O'Driscoll
(21,22), as indicated in Table III. The investigators who performed
the evaluations were blind to the treatment.
| Table III.O'Driscoll's microscopic histological
evaluation of articular cartilage. |
Table III.
O'Driscoll's microscopic histological
evaluation of articular cartilage.
| Variable | Score |
|---|
| Tissue
morphology |
|
| Mostly
hyaline cartilage | 4 |
| Mostly
fibrocartilage | 3 |
| Mostly
non-cartilage | 2 |
|
Exclusively non-cartilage | 1 |
| Matrix
staining |
|
|
None | 1 |
|
Slight | 2 |
|
Moderate | 3 |
|
Strong | 4 |
| Structural
integrity |
|
| Severe
disintegration | 1 |
| Cysts
or disruption | 2 |
| No
organization of chondrocytes | 3 |
|
Beginning of columnar
organization of chondrocytes | 4 |
| Normal,
similar to healthy mature cartilage | 5 |
| Chondrocyte
clustering in implant |
|
| 25–100%
of cells clustered | 1 |
| <25%
of cells clustered | 2 |
| No
clusters | 3 |
| Intactness of
calcified layer; tidemark formation |
|
| <25%
of calcified layer intact | 1 |
| 25–49%
of calcified layer intact | 2 |
| 50–75%
of calcified layer intact | 3 |
| 76–90%
of calcified layer intact | 4 |
|
Complete intactness of
calcified cartilage layer | 5 |
| Subchondral bone
formation |
|
| No
formation | 1 |
|
Slight | 2 |
|
Strong | 3 |
| Histological
assessment of surface architecture |
|
| Severe
fibrillation of disruption | 1 |
|
Moderate fibrillation or
irregularity | 2 |
| Slight
fibrillation or irregularity | 3 |
|
Normal | 4 |
| Histological
assessment of defect filling |
|
|
<25% | 1 |
|
26–50% | 2 |
|
51–75% | 3 |
|
76–90% | 4 |
|
91–110% | 5 |
| Lateral integration
of implanted material |
|
| Not
bonded | 1 |
| Bonded
at one hand/partially at both ends | 2 |
| Bonded
at both sides | 3 |
| Basal integration
of implanted material |
|
|
<50% | 1 |
|
50–70% | 2 |
|
70–90% | 3 |
|
91–100% | 4 |
| Inflammation: |
|
| No
inflammation | 1 |
| Slight
inflammation | 3 |
| Strong
inflammation | 5 |
| Maximum total
score | 45 |
Histology of the synovial
membrane
Synovial membrane samples were collected from the
lateral parapatellar region for analysis when the animals were
euthanized at 6 and 12 weeks. The synovial membrane was placed in
10% formalin at room temperature for 24 h and subsequently embedded
in paraffin, sectioned at a thickness of 5 µm and stained with
H&E at room temperature for 15 min. The specimens were
evaluated by two independent observers using a conventional
photonic microscope at a magnification of ×40 (Olympus BX41;
Olympus Corporation, Tokyo, Japan). The sections were each
allocated a Krenn's synovitis score (23), the details of which are indicated in
Table IV. A slice of each sample
was examined according to the scores and the mean and median scores
were calculated for each group.
| Table IV.Krenn's synovitis score. |
Table IV.
Krenn's synovitis score.
| Variable | Score |
|---|
| Enlargement of the
synovial lining cell layer |
|
| The
lining cells form one layer | 0 |
| The
lining cells form 2–3 layers | 1 |
| The
lining cells form 4–5 layers, few multinucleated cells might
occur | 2 |
| The
lining cells form >5 layers, the lining might be ulcerated and
multinucleated cells might occur | 3 |
| Density of the
resident cells |
|
| The
synovial stroma shows normal cellularity | 0 |
| The
cellularity is slightly increased | 1 |
| The
cellularity is moderately increased, multinucleated cells might
occur | 2 |
| The
cellularity is greatly increased, multinucleated giant cells,
pannus formation and rheumatoid granulomas might occur | 3 |
|
Inflammatory infiltrate |
|
| No
inflammatory infiltrate | 0 |
| Few
mostly perivascular situated lymphocytes or plasma cells | 1 |
|
Numerous lymphocytes or plasma
cells, sometimes forming follicle-like aggregates | 2 |
| Dense
band-like inflammatory infiltrate or numerous large follicle-like
aggregates | 3 |
| Total overall
assessment |
|
| Sum, 0
or 1 | No synovitis |
| Sum,
2–4 | Low-grade
synovitis |
| Sum,
5–9 | High-grade
synovitis |
Statistical analysis
The mean values, standard deviations and medians
were obtained for each group. The Kruskall-Wallis test was used to
determine statistical significance in the differences between the
three groups' Krenn synovitis score, the modified O'Driscoll score
and the ICRS score, respectively. In cases where this test
exhibited significant differences among the three groups, the
Kruskall Wallis post-hoc multiple comparisons of mean ranks of all
pairs of groups, with Bonferroni's correction was applied.
P<0.05 was used to indicate a statistically significant
difference. The software used for statistical analysis was
performed using the Statistica 8.0. software [STATISTICA (data
analysis software system) version 8.0. www.statsoft.com; TIBCO software, Inc., Palo Alto, CA,
USA].
Results
Macroscopic analysis at 6 weeks
The CTL group exhibited irregular tissue repair with
several fissures, and in some knees the defect was not completely
filled. The PRP group revealed irregularly repaired cartilage with
several fissures that were thinner compared with the surrounding
cartilage. Furthermore, in some specimens the center of the defect
still had the subchondral bone exposed. Notably, the PRP+SC group
demonstrated more regular tissue repair that was level with the
surrounding cartilage and exhibited small fissures. At 6 weeks, the
PRP+SC group grades were significantly improved compared with those
of the PRP group (P=0.003; Table V).
However, the PRP group exhibited a lower score compared with the
CTL group, though this difference was not statistically significant
(P=0.31).
| Table V.Macroscopic evaluation scoring. |
Table V.
Macroscopic evaluation scoring.
|
| International
cartilage repair society score mean ± standard deviation |
|
|
|---|
|
|
|
|
|
|---|
| Follow-up
Period | CTL group | PRP group | PRP + SC group | Kruskal-Wallis
P-value | Kruskall Wallis
post-hoc multiple comparison with Bonferroni's correction
P-value |
|---|
| 6 weeks | 6.67±3.01 | 3.60±2.37 | 8.86±1.35 | 0.0040a | CTL × PRP,
P=0.308 |
|
|
|
|
|
| CTL × PRP+SC,
P=0.516 |
|
|
|
|
|
| aPRP × PRP+SC, P=0.003 |
| 12 weeks | 5.50±2.22 | 7.22±1.92 | 9.88±0.99 | 0.0007a | CTL × PRP,
P=0.549 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.001 |
|
|
|
|
|
| aPRP × PRP+SC, P=0.049 |
Macroscopic analysis at 12 weeks
Tissue repair in the CTL group did not significantly
improve at 12 weeks post-surgery and the group exhibited irregular
tissue repair with several fissures and partial border integration.
The PRP group was notably improved and tissue repair was more level
with the surrounding cartilage, with small fissures and partial
border integration. Furthermore, the PRP+SC group revealed smoother
surface cartilage repair that was level with the surrounding
cartilage and almost complete border integration. At 12 weeks, the
macroscopic grades of the PRP+SC group were significantly improved
compared with those of the CTL and the PRP group (P=0.001 and
P=0.049, respectively; Table V).
Histological cartilage evaluation
CTL group
A total of 6 weeks following the surgical procedure,
the defects were filled with a thick mixture of hyaline-like and
fibrocartilaginous tissue in addition to viable cells. Some
irregularities were indicated on the surface. No cellular or tissue
organization was noted and there was no distinction between the
cartilaginous, calcified cartilage and subchondral bone zones. The
zone corresponding to the calcified zone sometimes exhibited
continuity with fibrous connective tissue; in other cases, this
zone exhibited continuity with the mineralized bone remodeling
matrix. Furthermore, highly vascularized tissue was above the bone
marrow region, which was composed of large blood vessels and
occasional sites of clustered inflammatory mononuclear cell
infiltrate. In the majority of cases, one of the edges of the
defects was not continuous with the adjacent normal cartilage and
was occasionally interspersed with fibrous connective tissue or
gaps revealing bare bone surface (Fig.
2).
At 12 weeks, the defects were primarily filled with
fibrocartilage. Cellular distribution was disorganized, cells were
predominantly viable and the surface exhibited irregularities. The
majority of the samples exhibited a gap in the central region of
the defect. Furthermore, the subchondral bone in the more central
portions were replaced by highly vascularized connective tissue. In
some samples, there was abnormal mineralization of cartilage in the
focal points outside of the calcification zone. Partial continuity
of the repaired cartilage with the normal adjacent cartilage was
observed.
PRP group
A total of 6 weeks following the surgical procedure,
the defects were filled with a mixture of hyaline-like and
fibrocartilaginous tissue, in addition to disorganized viable
cells. The surface exhibited fibrillation and irregularities.
Notably, improved subchondral bone remodeling was observed. There
was also partial continuity with the adjacent normal cartilage
(Fig. 2).
At 12 weeks, the defects were filled mostly with
hyaline-like cartilage and the surface exhibited fibrillation and
irregularities. On the border of the defect, some areas
demonstrated features similar to those of normal cartilage
organization with regular bone trabeculae, whereas in the center of
the defect, thicker cartilage had begun to exhibit columnar cell
organization with increased subchondral bone remodeling. In some
samples, the subchondral bone was replaced by fibrous connective
tissue. There was partial continuity with the adjacent normal
cartilage (Fig. 2).
PRP+SC group
At 6 weeks, the defects were predominantly filled
with hyaline-like cartilage. Cellular distribution was
disorganized, cells were viable and the surface was moderately
smooth. In the subchondral region, half of the samples exhibited
fibrous connective tissue with areas of granulation without
continuity and with the bone corresponding to the central region of
the defect. Islands of cartilage were observed amid the medullary
bone in the region corresponding to the defect. In some cases,
granulation tissue or foci of calcification were identified to be
interposed in the cartilaginous layer. Notably, there was partial
continuity with the adjacent normal cartilage (Fig. 2).
At 12 weeks, the defects were predominantly filled
with hyaline-like cartilage and early signs of columnar cell
organization were apparent. The surface was smooth and lamina
splendens were present. Bone trabeculae in the subchondral region
were regular and in the process of remodeling. Furthermore, lateral
integration with the adjacent normal cartilage partially occurred
in the majority of the defects (Fig.
2).
As indicated in Table
VI, histological scoring assessment at 6 weeks demonstrated
that the PRP+SC group had a significantly higher mean score
compared with the CTL group regarding the histological assessment
of surface architecture and lateral integration of implanted
material (P=0.0009 and P=0.0069, respectively). Regarding
histological assessment of surface architecture, the PRP group
exhibited no significant differences with the CTL group.
Furthermore, the PRP+SC group exhibited a significantly higher
score compared with the PRP group regarding the histological
assessment of surface architecture and lateral integration of
implanted material (P=0.0148 and P=0.0059, respectively).
| Table VI.Histological evaluation at 6
weeks. |
Table VI.
Histological evaluation at 6
weeks.
|
| Mean ± standard
deviation |
|
|
|---|
|
|
|
|
|
|---|
| Variable | CTL group | PRP group | PRP + SC group | Kruskal-Wallis
P-value | Kruskall Wallis
post-hoc multiple comparison with Bonferroni's correction
P-value |
|---|
| Tissue
morphology | 3.83±0.41 | 3.50±0.53 | 3.86±0.38 | 0.216 | – |
| Matrix
staining | 3.83±0.41 | 3.40±0.70 | 3.86±0.38 | 0.193 | – |
| Structural
integrity | 4.0±0.00 | 3.60±0.52 | 4.00±0.00 | 0.050 | – |
| Chondrocyte
clustering in implant | 2.00±0.00 | 1.80±0.42 | 2.43±0.53 | 0.025a | CTL × PRP,
P=1,000 |
|
|
|
|
|
| CTL × PRP+SC,
P=0.699 |
|
|
|
|
|
| PRP × PRP+SC,
P=0.155 |
| Intactness of
calcified layer, formation of tidemark | 1.17±0.41 | 1.90±1.10 | 1.57±0.53 | 0.280 | – |
| Subchondral bone
formation | 2.00±0.00 | 2.40±0.52 | 2.29±0.49 | 0.222 | – |
| Histological
assessment of surface architecture | 2.00±0.00 | 2.50±0.53 | 3.86±0.38 |
<0.001a | CTL × PRP,
P=0.675 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.001 |
|
|
|
|
|
| aPRP × PRP+SC, P=0.015 |
| Histological
assessment of defect filling | 4.83±0.41 | 4.50±0.53 | 5.00±0.00 | 0.065 | – |
| Lateral integration
of implanted material | 2.00±0 | 2.10±0.32 | 3.00±0 |
<0.001a | CTL × PRP,
P=1.000 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.007 |
|
|
|
|
|
| aPRP × PRP+SC, P=0.006 |
| Basal integration
of implanted material | 3.00±0 | 3.50±0.53 | 3.43±0.79 | 0.156 | – |
| Inflammation:
Maximum total score | 1.00±0 | 1.40±0.84 | 1.00±0 | 0.256 | – |
| Total score | 29.67±1.03 | 30.60±4.30 | 34.29±1.60 | 0.047a | CTL × PRP,
P=1,000 |
|
|
|
|
|
| CTL × PRP+SC,
P=0.062 |
|
|
|
|
|
| PRP × PRP+SC,
P=0.164 |
As indicated in Table
VII, at 12 weeks the PRP+SC group was indicated to have a
significantly higher mean histological evaluation score compared
with the CTL group for the following variables: Tissue morphology,
matrix staining, chondrocyte clustering in implant, histological
assessment of surface architecture, subchondral bone formation and
total score (P=0.0037, P=0.0172, P=0.0323, P=0.0006, P=0.0465 and
P=0.0021, respectively; Table
VII). Additionally, the PRP group scores were higher compared
with those of the CTL group in the cases of tissue morphology,
matrix staining, intactness of calcified layer and tidemark
formation, histological assessment of surface architecture,
subchondral bone formation and total score (P=0.0363, P=0.0024,
P=0.0132, P=0.0209, P=0.0323 and P=0.0076, respectively; Table VII). There were no significant
differences between the PRP+SC group and the PRP group.
| Table VII.Histological evaluation at 12
weeks. |
Table VII.
Histological evaluation at 12
weeks.
|
| Mean ± standard
deviation |
|
|
|---|
|
|
|
|
|
|---|
| Variable | CTL group | PRP group | PRP + SC group | Kruskal-Wallis
P-value | Kruskall Wallis
post-hoc multiple comparison with Bonferroni's correction
P-value |
|---|
| Tissue
morphology | 3.10±0.32 | 3.78±0.44 | 4.0±0.00 | 0.003a | aCTL × PRP, P=0.036 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.004 |
|
|
|
|
|
| PRP × PRP+SC,
P=1.000 |
| Matrix
staining | 2.90±0.32 | 3.89±0.33 | 3.75±0.46 | 0.002a | aCTL × PRP, P=0.002 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.017 |
|
|
|
|
|
| PRP × PRP+SC,
P=1.000 |
| Structural
integrity | 3.30±0.95 | 4.22±0.67 | 4.38±0.52 | 0.020a | CTL × PRP,
P=0.163 |
|
|
|
|
|
| CTL × PRP+SC,
P=0.073 |
|
|
|
|
|
| PRP × PRP+SC,
P=1.000 |
| Chondrocyte
clustering in implant | 1.80±0.42 | 2.00±0.50 | 2.63±0.52 | 0.007a | CTL × PRP,
P=1.000 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.032 |
|
|
|
|
|
| PRP × PRP+SC,
P=0.172 |
| Intactness of
calcified layer, formation of tidemark | 1.30±0.48 | 2.67±1.12 | 2.25±0.71 | 0.005a | aCTL × PRP, P=0.013 |
|
|
|
|
|
| CTL × PRP+SC,
P=0.069 |
|
|
|
|
|
| PRP × PRP+SC,
P=1.000 |
| Subchondral bone
formation | 2.20±0.42 | 2.89±0.33 | 2.88±0.35 | 0.002a | aCTL × PRP, P=0.032 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.046 |
|
|
|
|
|
| PRP × PRP+SC,
P=1.000 |
| Histological
assessment of surface architecture | 1.70±0.48 | 2.89±0.78 | 3.38±0.52 |
<0.001a | aCTL × PRP, P=0.021 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.001 |
|
|
|
|
|
| PRP × PRP+SC,
P=0.816 |
| Histological
assessment of defect filling | 4.80±0.42 | 5.00±0.00 | 5.00±0.00 | 0.171 | – |
| Lateral integration
of implanted material | 2.20±0.42 | 2.22±0.44 | 2.50±0.53 | 0.335 | – |
| Basal integration
of implanted material | 3.80±0.42 | 3.89±0.33 | 3.25±0.46 | 0.013a | CTL × PRP,
P=1.000 |
|
|
|
|
|
| CTL × PRP+SC,
P=0.146 |
|
|
|
|
|
| PRP × PRP+SC,
P=0.076 |
| Inflammation
maximum total score | 1.00±0.00 | 1.00±0.00 | 1.00±0.00 | 1.000 | – |
| Total score | 28.10±2.56 | 34.44±3.88 | 35.00±2.27 | 0.001a | aCTL × PRP, P=0.008 |
|
|
|
|
|
| aCTL × PRP+SC, P=0.002 |
|
|
|
|
|
| PRP × PRP+SC,
P=1.000 |
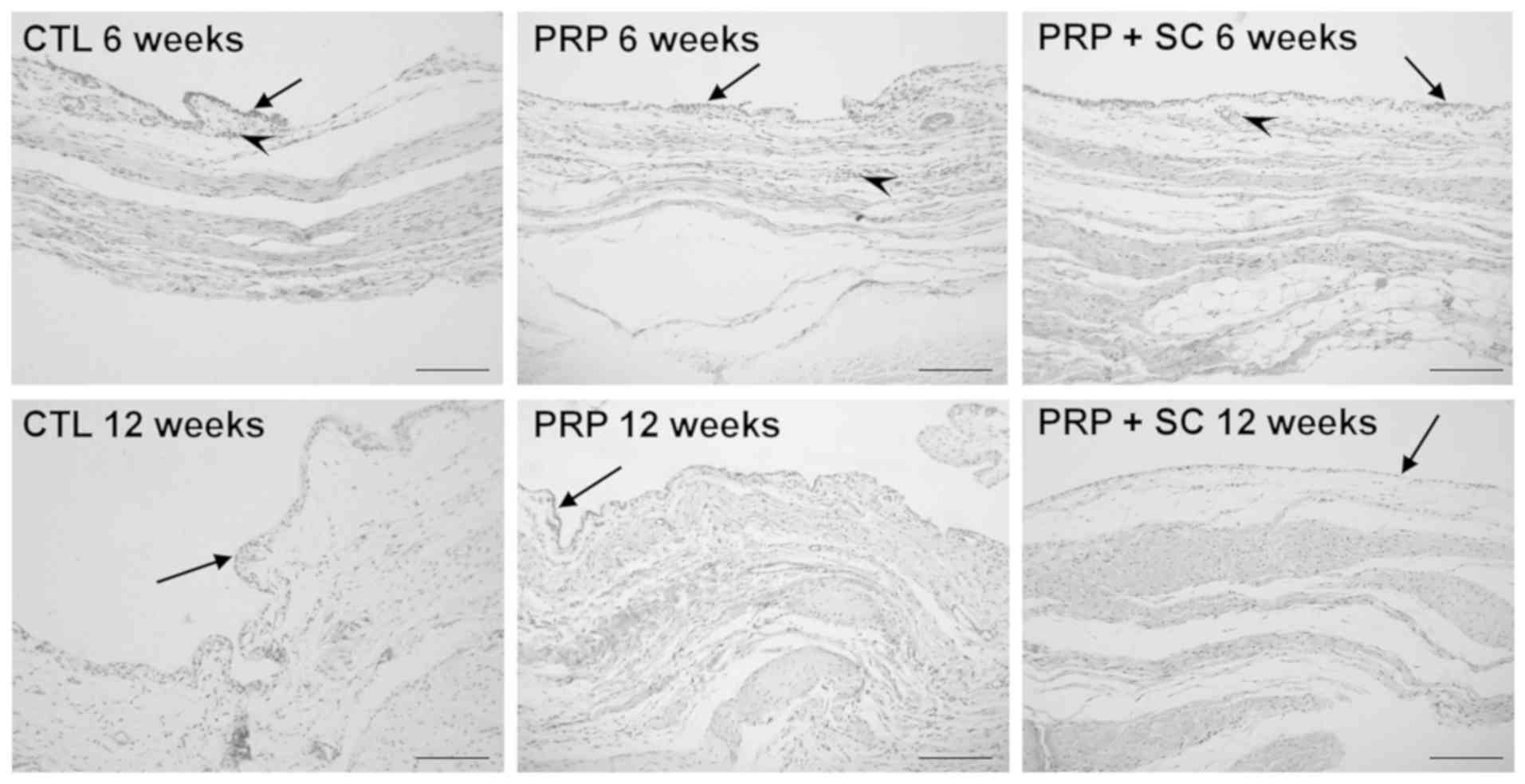
Synovial membrane microscopic
morphological analysis using Krenn's synovitis scoring
At 6 weeks, the synovial membranes of all three
groups exhibited loose connective tissue with slightly increased
cellularity and were permeated by discrete perivascular lymphocytic
inflammatory infiltrate (Fig. 3).
Furthermore, the layer of synovial lining cells was enlarged in the
CTL group and consisted of two to three smaller cell layers.
Conversely, the PRP and PRP+SC groups typically exhibited a single
layer of synovial lining cells. As indicated in Table VIII, the enlargement of the
synovial lining cell layer was significantly increased in the CTL
group when compared with the PRP group (P=0.037) and had a tendency
to be increased when compared with the PRP+SC group. In addition, a
low degree of synovitis was identified in all three groups at 6
weeks (Table VIII).
| Table VIII.Synovitis evaluation scoring. |
Table VIII.
Synovitis evaluation scoring.
|
|
| Enlargement of the
synovial lining cell layer | Density of the
resident cells | Inflammatory
infiltrate | Sum of Krenn's
synovitis score |
|
|---|
|
|
|
|
|
|
|
|
|---|
| Follow-up
period | Groups | Mean (SD) | Kruskall Wallis
(P-value) | Post hoc test with
Bonferroni correction | Mean (SD) | Kruskall Wallis
(P-value) | Mean (SD) | Kruskall Wallis
(P-value) | Kruskall Wallis
post-hoc multiple comparison with Bonferroni correction | Mean (SD) | Kruskall Wallis
(P-value) | Synovitis
grade |
|---|
| 6 weeks | CTL | 1.17 (0.41) | 0.017a | aCTL × PRP, P=0.037 | 0.83 (0.41) | 0.622 | 0.83 (0.41) | 0.835 | – | 2.83 (0.75) | 0.107 | Low |
|
| PRP | 0.30 (0.67) |
| CTL × PRP+SC,
P=0.200 | 0.90 (0.32) |
| 0.70 (0.48) |
|
| 1.80 (1.14) |
| Low |
|
| PRP+SC | 0.43 (0.53) |
| PRP × PRP+SC,
P=1.000 | 0.71 (0.49) |
| 0.71 (0.49) |
|
| 1.86 (0.90) |
| Low |
| 12 weeks | CTL | 0.70 (0.48) | 0.007a | CTL × PRP,
P=0.067 | 0.20 (0.42) | 0.174 | 0.00 (0.00) | 0.005a | CTL × PRP,
P=0.171 | 0.90 (0.74) | 0.096 | No |
|
| PRP | 0.10 (0.32) |
| CTL × PRP+SC,
P=0.120 | 0.50 (0.53) |
| 0.50 (0.53) |
| CTL × PRP+SC,
P=1.000 | 1.10 (0.99) |
| No |
|
| PRP+SC | 0.13 (0.35) |
| PRP × PRP+SC,
P=1.000 | 0.13 (0.35) |
| 0.00 (0.00) |
| PRP × PRP+SC,
P=0.218 | 0.25 (0.46) |
| No |
At 12 weeks, the three groups exhibited normal
cellularity and no evident inflammation. The layer of synovial
lining in the CTL group continued to be comprised of two to three
smaller cell layers and the PRP and PRP+SC groups exhibited a
normal single layer; however, the difference between the synovitis
evaluation scoring in these groups was not statistically
significant. Notably, no synovitis was indicated in any of the
three groups at 12 weeks (Fig. 3;
Table VIII).
Discussion
A primary advantage of mesenchymal stem cells (MSCs)
is their capacity to differentiate into osteocytes and
chondrocytes, and their ability to regenerate cartilage and the
underlying subchondral bone essential for adequate healthy
cartilage support (24). The use of
stem cells in articular cartilage repair is promising, and has been
demonstrated to enhance repair; however, its experimental
application through intraarticular MSC injections may result in
fibrocartilaginous tissue formation (25). This outcome reflects the fact that
other factors are involved in adequate cell differentiation and
tissue repair (24–28).
Synovial fluid serves a key role in osteoarthritis
by allowing for different tissue communication inside the joint in
multidirectional pathways (29,30). In
cases of osteoarthritis, the synovial fluid is a predominant source
of extrinsic signaling factors and proinflammatory cytokines, and
there is an increased number of MSCs present (31). This increase in MSCs in the synovial
fluid and the cases of synovitis with infiltration of inflammatory
cells in the synovium maybe interpreted as responses to
inflammation and tissue injury. It has been reported that signaling
molecules contribute to cartilage repair involving the synovial
fluid and the calcified cartilage of the subchondral bone, which
allows for these locations to interact as functional units
(32).
In the present study, synovial analysis revealed
low-grade synovitis at 6 weeks in all groups and decreased
synovitis at 12 weeks. Although the degree of synovitis was similar
between the groups, the CTL group exhibited pronounced enlargement
of the synovial lining layer, which persisted at 12 weeks. This
finding validated the interaction and signaling of tissue repair
with the synovium after the creation of the defect and raises the
question whether the synovium and synovial fluid should also be
targeted to improve cartilage tissue repair. A previous
experimental study on rabbits indicated multiple joint injections
of PRP to be beneficial in reducing synovitis and inflammatory
factors and in restoring damaged tissue (7). In addition, PRP has been demonstrated
to stimulate cell proliferation and superficial zone protein
secretion by articular cartilage and synovium in the human knee
joint (33). The mechanisms of
action in PRP therapy are complex, multifaceted and remain to be
fully elucidated. However, in osteoarthritis, PRP has been
suggested to exhibit pro-anabolic or anti-catabolic mechanisms and
to provide pain relief (29). In the
present study, although the difference was not statistically
significant, the PRP and PRP+SC groups exhibited reduced synovitis
at 6 and 12 weeks compared with the respective CTL groups. However,
further study is warranted to determine whether synovitis maybe
attenuated by PRP or stem cells, and thus influence cartilage
repair.
MSCs differ in their chondrogenic potential. When
the synovial fluid, synovium, bone marrow, adipose tissue and
muscle MSCs were compared, those of the synovial fluid, synovium
and bone marrow exhibited improved chondrogenic potential (13,34,35). The
present study examined hDPSCs because hDPSC subpopulations have
been demonstrated to have higher angiogenic, neurogenic and
regenerative potential compared with bone marrow stem cells or
adipose stem cells (14). The
chondrogenic potential of hDPSCs has not been compared to that of
other MSCs; however several in vitro and in vivo
studies have suggested hDPSCs as a promising tool for cartilage
repair (15,36,37),
which was corroborated by the present study.
A review of in vitro studies has indicated a
positive interaction between PRP and MSCs with regards to
stimulation of stem cell proliferation, the lack of interference
with lineage differentiation, preservation of multipotency and the
immune-privileged characteristics of the MSCs and the delay of the
development/emergence of the senescent phenotype (38). In the case of articular cartilage
repair, a review has demonstrated that PRP may stimulate
chondrogenic differentiation in vitro and enhance cartilage
repair in animal studies (39).
Notably, PRP has diverse compositions, concentrations and
activation methods, which produce conflicting results on its
effects on cartilage repair (40,41).
Carneiro et al (42) reported
the use of autologous PRP gel with the presence of leukocytes
concentrated two to three times in a full-thickness cartilage
defect in an ovine model. The study indicated improved results
after 12 weeks, though the repair did not consist of hyaline
cartilage. Serra et al (43)
reported the use of multiple injections of autologous PRP in a
full-thickness defect in a rabbit model and observed no differences
in repair relative to controls after 19 weeks. Additionally, Milano
et al (22,44) reported a positive effect of PRP on
cartilage repair after microfractures and identified the effect to
be more pronounced when PRP was mixed with fibrin glue and used as
a gel in comparison with a liquid intraarticular injection;
however, hyaline cartilage formation was not observed (22). The PRP gel scaffold used in the
present study was homologous and contained leukocytes, which may
influence the hDPSCs and autologous bone marrow cells present in
the defect (45).
In the present study, the use of PRP gel containing
hDPSCs at the defect site contributed to improved subchondral bone
formation, with repaired tissue consisting primarily of
hyaline-like cartilage. In addition, a smooth articular cartilage
surface was indicated. By contrast, the CTL group exhibited a more
irregular and fibrillated articular cartilage surface and the
repaired tissue consisted mostly of fibrocartilage. Notably, the
full-thickness cartilage defect created in the present study
allowed exposure of the subchondral bone. As a result, a more
pronounced migration of bone marrow cells can occur, which promotes
interaction with the PRP and the hDPSCs (46). This type of interaction may be useful
in a surgical intervention for cartilage repair but requires
further exploration.
The present results indicated that, in the PRP and
PRP+SC groups the formation of a homogeneous calcified cartilage
and tidemark was improved compared with the CTL group, particularly
on the border of the defect. Furthermore, the quality of the
adjacent repaired cartilage was also improved. In all three groups,
the center of the defect still had signs of subchondral bone
remodeling in which vascularized connective tissue was present,
particularly in the CTL group. The findings of the present study
suggest that adequate subchondral bone formation and remodeling
seem to be fundamental for restoring and obtaining high quality
repaired cartilage. Notably, a 12-week follow-up period is short
and differences in subchondral bone and any gaps in healed
cartilage may likely be more pronounced at 24 weeks (47).
The lamina splendens consists of collagen fibrils
that run parallel to the surface of the joint (48). It is responsible for maintaining the
mechanical response of the articular cartilage to load absorption
and is the first component to degrade in osteoarthritis (49). If the surface zone layer and adequate
superficial zone protein (lubricin) are not reestablished, their
loss may lead to the ultimate failure of any articular cartilage
repair as a result of the shear forces in the joint (49). In the present study, smoother
cartilage surfaces were observed in the PRP and PRP+SC groups and
the repaired cartilage of the PRP+SC group had the majority of its
surface layer covered by lamina splendens. This finding suggests
that the cartilage repaired in the PRP+SC group may resist longer
and more adequately to heavier loads. It was speculated that this
end point may be particularly important and that further
histological analyses are required in cartilage repair studies.
The present study had some limitations. The
follow-up period was too short to definitively understand the
outcome or the lasting effects of the repaired cartilage. In
addition, biomechanical evaluations to evaluate which group
demonstrated better cartilage mechanical resistance to load or
cartilage-derived extracellular matrix immunohistochemical staining
that may further evaluate cartilage and bone quality were not used
in the present cartilage repair analysis. However, full-thickness
cartilage defects treated with hDPSCs in a PRP gel scaffold
resulted in fewer signs of synovitis, as exhibited by reduced
synovial lining cell layer thickening. In addition, enhanced
histological cartilage repair was indicated to consist
predominantly of hyaline-like cartilage at 12 weeks post-surgery.
To conclude, the present results support the therapeutic use of
hDPSCs for the treatment of full-thickness articular cartilage
defects; however, further studies are warranted.
Acknowledgements
The authors would like to thank Professor Corina da
Costa Freitas from the Brazilian National Institute for Space
Research (INPE; São José dos Campos, Brazil) for their assistance
with statistical analysis. The authors would also like to thank Mr.
Milton Alves Junior and Mr. Wilson Orcini for their technical
assistance. The present article represents part of the Master's
degree thesis project by RHY at Marília Medical School (FAMEMA) in
Marília, São Paulo State, Brazil.
Funding
The present study was supported by São Paulo
Research Foundation (FAPESP) (grant no. 12/21007-0).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RY, RL, SP and LM performed the experiments,
analysis and wrote the manuscript; JF, RS, AK, MM, SF and BS
generated data and performed analyses; and RS and SP interpreted
the data, drafted the manuscript and made critical revisions. All
authors discussed the results and reviewed the manuscript.
Ethics approval and consent to
participate
The study protocol of the present experiment was
reviewed and approved by the Ethics Committee at Faculdade de
Medicina de Marília, São Paulo, Brazil (EC No. 641/12).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Dominici M, Le Blanc K, Mueller I,
Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A,
Prockop Dj and Horwitz E: Minimal criteria for defining multipotent
mesenchymal stromal cells. The international society for cellular
therapy position statement. Cytotherapy. 8:315–317. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Steadman JR, Briggs KK, Rodrigo JJ, Kocher
MS, Gill TJ and Rodkey WG: Outcomes of microfracture for traumatic
chondral defects of the knee: Average 11-year follow-up.
Arthroscopy. 19:477–484. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Knutsen G, Drogset JO, Engebretsen L,
Grøntvedt T, Isaksen V, Ludvigsen TC, Roberts S, Solheim E, Strand
T and Johansen O: A randomized trial comparing autologous
chondrocyte implantation with microfracture. Findings at five
years. J Bone Joint Surg Am. 89:2105–2112. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Saw KY, Hussin P, Loke SC, Azam M, Chen
HC, Tay YG, Low S, Wallin KL and Ragavanaidu K: Articular cartilage
regeneration with autologous marrow aspirate and hyaluronic Acid:
An experimental study in a goat model. Arthroscopy. 25:1391–1400.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen WH, Lo WC, Hsu WC, Wei HJ, Liu HY,
Lee CH, Tina Chen SY, Shieh YH, Williams DF and Deng WP:
Synergistic anabolic actions of hyaluronic acid and platelet-rich
plasma on cartilage regeneration in osteoarthritis therapy.
Biomaterials. 35:9599–9607. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Abate M, Verna S, Schiavone C, Di Gregorio
P and Salini V: Efficacy and safety profile of a compound composed
of platelet-rich plasma and hyaluronic acid in the treatment for
knee osteoarthritis (preliminary results). Eur J Orthop Surg
Traumatol. 25:1321–1326. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liu J, Yuan T and Zhang C: Effect of
platelet-rich plasma on synovitis of rabbit knee. Zhongguo Xiu Fu
Chong Jian Wai Ke Za Zhi. 25:285–290. 2011.(In Chinese). PubMed/NCBI
|
|
8
|
Gotterbarm T, Richter W, Jung M, Berardi
Vilei S, Mainil-Varlet P, Yamashita T and Breusch SJ: An in vivo
study of a growth-factor enhanced, cell free, two-layered
collagen-tricalcium phosphate in deep osteochondral defects.
Biomaterials. 27:3387–3395. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Andia I, Sanchez M and Maffulli N: Basic
science: Molecular and biological aspects of platelet-rich plasma
therapies. Oper Tech Orthop. 22:3–9. 2012. View Article : Google Scholar
|
|
10
|
Drengk A, Zapf A, Stürmer EK, Stürmer KM
and Frosch KH: Influence of platelet-rich plasma on chondrogenic
differentiation and proliferation of chondrocytes and mesenchymal
stem cells. Cells Tissues Organs. 189:317–326. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mishra A, Tummala P, King A, Lee B, Kraus
M, Tse V and Jacobs CR: Buffered platelet-rich plasma enhances
mesenchymal stem cell proliferation and chondrogenic
differentiation. Tissue Eng Part C Methods. 15:431–435. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Akeda K, An HS, Okuma M, Attawia M,
Miyamoto K, Thonar EJ, Lenz ME, Sah RL and Masuda K: Platelet-rich
plasma stimulates porcine articular chondrocyte proliferation and
matrix biosynthesis. Osteoarthritis Cartilage. 14:1272–1280. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Koga H, Muneta T, Nagase T, Nimura A, Ju
YJ, Mochizuki T and Sekiya I: Comparison of mesenchymal
tissues-derived stem cells for in vivo chondrogenesis: Suitable
conditions for cell therapy of cartilage defects in rabbit. Cell
Tissue Res. 333:207–215. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ishizaka R, Hayashi Y, Iohara K, Sugiyama
M, Murakami M, Yamamoto T, Fukuta O and Nakashima M: Stimulation of
angiogenesis, neurogenesis and regeneration by side population
cells from dental pulp. Biomaterials. 34:1888–1897. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Daltoé FP, Mendonça PP, Mantesso A and
Deboni MC: Can SHED or DPSCs be used to repair/regenerate
non-dental tissues? A systematic review of in vivo studies. Braz
Oral Res. 28:S1806–83242014000100401. 2014. View Article : Google Scholar
|
|
16
|
Jesus AA, Soares MBP, Soares AP, Nogueira
RC, Guimarães ET, Araújo TM and Santos RR: Collection and culture
of stem cells derived from dental pulp of deciduous teeth:
Technique and clinical case report. Dent Press J Orthodont.
16:82011.
|
|
17
|
Sanchez O, Escobar JI and Yunis JJ: A
simple G-banding technique. Lancet. 2:2691973. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brothman AR, Persons DL and Shaffer LG:
Nomenclature evolution: Changes in the ISCN from the 2005 to the
2009 edition. Cytogenet Genome Res. 127:1–4. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mainil-Varlet P, Aigner T, Brittberg M,
Bullough P, Hollander A, Hunziker E, Kandel R, Nehrer S, Pritzker
K, Roberts S, et al: Histological assessment of cartilage repair: A
report by the Histology Endpoint Committee of the international
cartilage repair society (ICRS). J Bone Joint Surg Am 85-A. (Suppl
2):S45–S57. 2003. View Article : Google Scholar
|
|
20
|
van den Borne MP, Raijmakers NJ, Vanlauwe
J, Victor J, de Jong SN, Bellemans J and Saris DB; International
Cartilage Repair Society, : International Cartilage Repair Society
(ICRS) and Oswestry macroscopic cartilage evaluation scores
validated for use in autologous chondrocyte implantation (ACI) and
microfracture. Osteoarthritis Cartilage. 15:1397–1402. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bonasia DE, Marmotti A, Massa AD, Ferro A,
Blonna D, Castoldi F and Rossi R: Intra- and inter-observer
reliability of ten major histological scoring systems used for the
evaluation of in vivo cartilage repair. Knee Surg Sports Traumatol
Arthrosc. 23:2484–2493. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Milano G, Sanna Passino E, Deriu L,
Careddu G, Manunta L, Manunta A, Saccomanno MF and Fabbriciani C:
The effect of platelet rich plasma combined with microfractures on
the treatment of chondral defects: An experimental study in a sheep
model. Osteoarthritis Cartilage. 18:971–980. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Krenn V, Morawietz L, Burmester GR, Kinne
RW, Mueller-Ladner U, Muller B and Haupl T: Synovitis score:
Discrimination between chronic low-grade and high-grade synovitis.
Histopathology. 49:358–364. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yan H and Yu C: Repair of full-thickness
cartilage defects with cells of different origin in a rabbit model.
Arthroscopy. 23:178–187. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lee KB, Hui JH, Song IC, Ardany L and Lee
EH: Injectable mesenchymal stem cell therapy for large cartilage
defects-a porcine model. Stem Cells. 25:2964–2971. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wakitani S, Goto T, Pineda SJ, Young RG,
Mansour JM, Caplan AI and Goldberg VM: Mesenchymal cell-based
repair of large, full-thickness defects of articular cartilage. J
Bone Joint Surg Am. 76:579–592. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wakitani S, Imoto K, Yamamoto T, Saito M,
Murata N and Yoneda M: Human autologous culture expanded bone
marrow mesenchymal cell transplantation for repair of cartilage
defects in osteoarthritic knees. Osteoarthritis Cartilage.
10:199–206. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Shao XX, Hutmacher DW, Ho ST, Goh JC and
Lee EH: Evaluation of a hybrid scaffold/cell construct in repair of
high-load-bearing osteochondral defects in rabbits. Biomaterials.
27:1071–1080. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Andia I, Sánchez M and Maffulli N: Joint
pathology and platelet-rich plasma therapies. Expert Opin Biol
Ther. 12:7–22. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Olson SA, Horne P, Furman B, Huebner J,
Al-Rashid M, Kraus VB and Guilak F: The role of cytokines in
posttraumatic arthritis. J Am Acad Orthop Surg. 22:29–37. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
E X, Cao Y, Meng H, Qi Y, Du G, Xu J and
Bi Z: Dendritic cells of synovium in experimental model of
osteoarthritis of rabbits. Cell Physiol Biochem. 30:23–32. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lories RJ and Luyten FP: The
bone-cartilage unit in osteoarthritis. Nat Rev Rheumatol. 7:43–49.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sakata R, McNary SM, Miyatake K, Lee CA,
Van den Bogaerde JM, Marder RA and Reddi AH: Stimulation of the
superficial zone protein and lubrication in the articular cartilage
by human platelet-rich plasma. Am J Sports Med. 43:1467–1473. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ando W, Kutcher JJ, Krawetz R, Sen A,
Nakamura N, Frank CB and Hart DA: Clonal analysis of synovial fluid
stem cells to characterize and identify stable mesenchymal stromal
cell/mesenchymal progenitor cell phenotypes in a porcine model: A
cell source with enhanced commitment to the chondrogenic lineage.
Cytotherapy. 16:776–788. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Jones E and Crawford A: High chondrogenic
potential of synovial fluid-derived mesenchymal stromal cells.
Cytotherapy. 16:1595–1596. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Rizk A and Rabie AB: Human dental pulp
stem cells expressing transforming growth factor β3 transgene for
cartilage-like tissue engineering. Cytotherapy. 15:712–725. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Martin-Piedra MA, Garzon I, Oliveira AC,
Alfonso-Rodriguez CA, Carriel V, Scionti G and Alaminos M: Cell
viability and proliferation capability of long-term human dental
pulp stem cell cultures. Cytotherapy. 16:266–277. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Rubio-Azpeitia E and Andia I: Partnership
between platelet-rich plasma and mesenchymal stem cells: In vitro
experience. Muscles Ligaments Tendons J. 4:52–62. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Abrams GD, Frank RM, Fortier LA and Cole
BJ: Platelet-rich plasma for articular cartilage repair. Sports Med
Arthrosc. 21:213–219. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Boswell SG, Cole BJ, Sundman EA, Karas V
and Fortier LA: Platelet-rich plasma: A milieu of bioactive
factors. Arthroscopy. 28:429–439. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sundman EA, Cole BJ and Fortier LA: Growth
factor and catabolic cytokine concentrations are influenced by the
cellular composition of platelet-rich plasma. Am J Sports Med.
39:2135–2140. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Carneiro Mde O, Barbieri CH and Barbieri
Neto J: Platelet-rich plasma gel promotes regeneration of articular
cartilage in knees of sheep. Acta Ortop Bras. 21:80–86.
2013.PubMed/NCBI
|
|
43
|
Serra CI, Soler C, Carillo JM, Sopena JJ,
Redondo JI and Cugat R: Effect of autologous platelet-rich plasma
on the repair of full-thickness articular defects in rabbits. Knee
Surg Sports Traumatol Arthrosc. 21:1730–1736. 2013.PubMed/NCBI
|
|
44
|
Milano G, Deriu L, Sanna Passino E, Masala
G, Manunta A, Postacchini R, Saccomanno MF and Fabbriciani C:
Repeated platelet concentrate injections enhance reparative
response of microfractures in the treatment of chondral defects of
the knee: An experimental study in an animal model. Arthroscopy.
28:688–701. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Dohan Ehrenfest DM, Bielecki T, Jimbo R,
Barbé G, Del Corso M, Inchingolo F and Sammartino G: Do the fibrin
architecture and leukocyte content influence the growth factor
release of platelet concentrates? An evidence-based answer
comparing a pure platelet-rich plasma (P-PRP) gel and a leukocyte-
and platelet-rich fibrin (L-PRF). Curr Pharm Biotechnol.
13:1145–1152. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Pot MW, Gonzales VK, Buma P, IntHout J,
van Kuppevelt TH, de Vries RBM and Daamen WF: Improved cartilage
regeneration by implantation of acellular biomaterials after bone
marrow stimulation: A systematic review and meta-analysis of animal
studies. PeerJ. 4:e22432016. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Shapiro F, Koide S and Glimcher MJ: Cell
origin and differentiation in the repair of full-thickness defects
of articular cartilage. J Bone Joint Surg Am. 75:532–553. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wu JP, Kirk TB and Zheng MH: Study of the
collagen structure in the superficial zone and physiological state
of articular cartilage using a 3D confocal imaging technique. J
Orthop Surg Res. 3:292008. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Hollander AP, Dickinson SC and Kafienah W:
Stem cells and cartilage development: Complexities of a simple
tissue. Stem Cells. 28:1992–1996. 2010. View Article : Google Scholar : PubMed/NCBI
|