Introduction
Osteoarthritis (OA) is the most prevalent type of
arthritis, and it is characterized by a progressive degradation of
articular cartilage, new bone formation and acute inflammation
(1). Knee osteoarthritis (KOA) with
hip osteoarthritis is primarily responsible for the pain and
locomotor disability worldwide (2,3). With
the increasing trend of ageing and obesity of the population of the
world, health services for KOA with hip OA will be in higher demand
(4). OA is characterized by chronic
pain and tissue destruction, which is concomitant with inflammation
in some cases, and patients with OA suffer from constant chronic
pain, consequently resulting in disabilities and a heavy social
burden (5). The risk factors for KOA
include knee extensor muscle weakness, lower extremity muscle
strength, afferent sensory dysfunction and genetic issues (6,7). Joint
swelling is one clinical feature of OA that is attributed to
inflammation (8). Data in a previous
study supported the crucial role of inflammation in determining the
severity, progression risk, and clinical symptoms of OA (9). Evidence also indicated that
inflammation, as evidenced by synovitis or effusion, is a main
driver for pain sensitization in KOA (10). Therefore, a better understanding of
the inflammatory mechanisms in KOA is required to better manage KOA
pain.
In addition to its role in cancer initiation and
progression, the NF-κB family of transcription factors also serves
an essential role in inflammation and innate immunity (11). Notably, NF-κB is a pivotal regulator
of inflammation in rheumatoid arthritis because, in rheumatoid
arthritis, persistent NF-κB activation mediates the over-expression
of inflammatory cytokines and tissue injury (12,13).
Chondrocytes are the primary cell type in articular cartilage, and
the loss of these cells induces fatigue of the extracellular matrix
(ECM), which results in failure of the cartilage and impairment of
the entire joint (14). The
pathogenesis of OA is closely related with pro-inflammatory
cytokines production by chondrocytes, such as interleukin (IL)-1,
which leads to the activation of matrix metalloproteinases (MMPs)
and deterioration of OA (15).
Mechanical and inflammatory stresses to articular cartilage may
disturb the chondrocyte energy balance during the progression of
OA, which may deteriorate the pathogenesis of OA (16). However, the exact mechanism of these
pro-inflammatory cytokines in OA progression remains an area of
active research. Furthermore, no clinical data regarding the
expression levels of IL-1β, MMP-13 and NF-κB in KOA has been
reported. In this regard, the present study, from a perspective
view of a clinical study, was conducted to investigate the
expression of pro-inflammation cytokines, MMP-13, NF-κBp65 and
IL-1β, in synovial tissue to determine their function in the
progression of KOA. A possible mechanism is proposed based on the
results raised in this study with the hope of shedding light for
better understanding of KOA inflammation.
Materials and methods
Subjects
A total of 100 KOA patients admitted to Nanjing Luhe
People's Hospital to receive knee replacements from December 2015
to December 2017 were included in the case group, which had an
average age of 60.5 years old (range, 56-81 years old). The body
mass index (BMI) for the included subjects was 22.58±3.27
kg/m2. There were 49 males and 51 females. There were 57
subjects with lesions in their left knee, and 43 subjects with
lesions in their right knee. The following inclusion criteria were
used for the case group: i) meeting the diagnostic basis for OA
(17); ii) disease progression for
more than 6 months; iii) in cases of bilateral KOA, selecting the
more severe side for inclusion; iv) lacking lesions in the heart,
blood vessels, liver or kidney; and v) discontinuing medication
use, such pain killers, corticosteroids, or any other Chinese
herbal preparation 4 weeks before surgery. The criteria for
exclusion were as follows: i) patients with active gastroenteric
disease or with a history of peptic ulcer or duodenal bleeding; and
ii) patients with joint diseases, such as rheumatoid arthritis or
infectious arthritis. Patients in case group were classified
according to the Outerbridge grade (18) into a mild KOA group (n=59;
Outerbridge grades 1 and 2) or a severe KOA group (n=41;
Outerbridge grades 3 and 4). A total of 72 patients with injury of
the cruciate ligament of the knee joint or meniscus injury in our
hospital were included as the control group; the control group had
an average age of 54 years (range, 41-81 years old). The time from
injury to enrollment of patients in the control group was within
three weeks. The control group consisted of 31 males and 41
females; 39 patients had lesions on their left knee, and 33
patients had lesions on their right knee. The living style of
patients in the case and control groups, such as smoking history
and exercise habits, were recorded for comparison. Sex, age, BMI,
smoking history and exercise habits between the two groups were not
significantly different, which indicated the comparability of the
two groups. A 1.0x1.0x0.5 cm synovial sample of the anterior
cruciate of the knee was collected, sealed in double plastic bags
and immediately stored in a freezer at -70˚C. Cartilage tissues
from the unloaded surface of the condyle were collected in the case
and control groups and stored in a freezer at -70˚C until further
usage. The present study was performed based on protocols proposed
by the Ethics Committee of Nanjing Luhe People's Hospital. All
patients signed written informed consent prior to participation in
the study.
Haematoxylin & eosin staining
Tissue samples were fixed in 4% paraformaldehyde at
20˚C for 24 h and embedded in paraffin. Paraffin-embedded tissues
were sliced into 4-µm thick sections. Some of the sections were
subsequently dewaxed twice in xylene at 20˚C for 10 min and
rehydrated in a descending alcohol series (90, 80 and 70%), prior
to being washed with distilled water for 2 min. The slices were
stained using haematoxylin for 5 min before rinsing and re-staining
in 5% eosin for 2 min, both at 20˚C. Sections were sealed by using
neutral resins for observation under a light microscope
(magnification, x200; Olympus Corporation). The remaining tissue
sections were stored at -20˚C until further use for Safranin O-Fast
Green staining and immunohistochemistry.
Safranin O-Fast Green staining
Safranin O-Fast Green staining (Sigma-Aldrich; Merck
KGaA) was performed to observe the morphology of cartilage tissues
under a light microscope. Paraffin-embedded slices were dewaxed in
xylene at 20˚C for 10 min and rehydrated with absolute alcohol for
5 min, 95% alcohol for 5 min and 80% alcohol for 5 min, prior to
being washed with distilled water for 2 min. Sections were
subsequently stained with haematoxylin at 20˚C for 3 min, before
being washed three times with distilled water. Hydrochloric acid
(1%) and ethanol were used for 15 sec at 20˚C to differentiate the
slices. The slices were washed three times with distilled water and
immersed in a 0.02% Fast Green solution at 20˚C for 3 min. The
stained slices were washed in 1% glacial acetic acid and stained in
0.1% Safranin O at 20˚C for 3 min. The slices were sealed to
observe the cellular matrix staining, tidemark and calcification of
cartilage tissues under a light microscope (magnification,
x100).
Immunohistochemistry
A 3% H2O2 solution was
incubated with the paraffin-embedded sections at 20˚C for 10 min to
terminate the activity of endogenous peroxidase and antigen
retrieval buffer was added to the sections prior to boiling for
5-10 min; the sample was cooled for 5 min, and this boiling-cooling
cycle was repeated twice. The slices were cooled to room
temperature, and 5% BSA (Boster Biological Technology) blocking
buffer was added at room temperature for 20 min. Primary mouse
anti-human antibodies against MMP-13 (1:500; cat. no. ab219620;
Abcam), NF-κBp65 (1:100; cat. no. ab16502; Abcam) and GAPDH
(1:1,000; cat. no. ab181602; Abcam) were incubated at 4˚C
overnight. Biotinylated goat anti-mouse IgG (1:2,000; cat. no.
ab64257; Abcam) was added for incubation at 37˚C for 40 min. The
slices were washed, and DAB (Beijing ZSGB-BIO; OriGene
Technologies, Inc.) was applied for colour development. The dried
slices were observed and photographed under a microscope. Cells
with brownish yellow or dark brown particles were positive cells.
Five high-powered fields (magnification, x400) were selected to
calculate the percentage of positive cells in all cells and the
positive cell rate, which was the relative protein expression. Two
independent technicians observed and assessed all slices by using a
double-blind method.
Reverse transcription-quantitative PCR
(RT-qPCR)
Total RNA was extracted from frozen tissues using
TRIzol® reagent (Invitrogen; Thermo Fisher Scientific,
Inc.) and preserved at -80˚C. The PrimeScript™ RT reagent kit
(Perfect Real-Time; Takara Biotechnology Co., Ltd.) was used to
reverse-transcribe the total RNA into cDNA, according to the
manufacturer's protocol, which was stored at -20˚C until further
use. GAPDH was used as an internal control. An ABI7500 quantitative
PCR instrument (ABI; Thermo Fisher Scientific, Inc.) and a
SYBR-Green PCR reagent kit (Thermo Fisher Scientific, Inc.) was
used to perform the qPCR. The reaction was performed using the
following conditions: Initial denaturation at 95˚C for 5 min;
followed by 40 cycles of denaturation at 90˚C for 30 sec, annealing
at 60˚C for 40 sec and extension at 72˚C for 40 sec. The primer
sequences used for RT-qPCR are listed in Table I. Each sample was measured three
times, and the 2-ΔΔCq method (19) was used to calculate the relative
expression of target genes, and expression levels were normalized
to GAPDH.
 | Table IPrimer sequences used for reverse
transcription-quantitative PCR. |
Table I
Primer sequences used for reverse
transcription-quantitative PCR.
| Gene | Primer sequence
(5'→3') |
|---|
| MMP-13 | F:
AATATCTGAACTGGGTCTTCCAAAA |
| | R:
CAGACCTGGTTTCCTGAGAACAG |
| NF-κBp65 | F:
TGGAGCAAGCCATTAG |
| | R:
GGGCACGGTTATCAA |
| IL-1β | F:
AGTGCCTACGCACATGTCTTC |
| | R:
TGCGTCACACAGAAACTCGTC |
| GAPDH | F:
GCACCGTCAAGGCTGAGAAC |
| | R:
ATGGTGGTGAAGACGCCAGT |
Western blotting
RIPA protein lysis buffer (Beyotime Institute of
Biotechnology) was added to frozen tissues for collection of total
protein. The Bradford method (Thermo Fisher Scientific, Inc.) was
used for protein quantitation. Then, 50 µg protein was subjected to
12% SDS-PAGE, and the separated proteins were transferred to
polyvinylidene fluoride membranes. The membranes were blocked in 5%
skimmed milk powder at 37˚C for 1 h. Primary rabbit anti-human
antibodies against MMP-13 (1:3,000; cat. no. ab39012; Abcam),
NF-κBp65 (1:2,000; cat. no. ab16502; Abcam) and IL-lβ (1:1,000;
cat. no. ab9722; Abcam) and a monoclonal antibody against GAPDH
(1:1,000; cat. no. ab181602; Abcam) were incubated with the
membranes at 4˚C overnight. PBS-0.05% Tween-20 was then used to
wash the membrane three times, each for 5 min. Horseradish
peroxidase-conjugated goat anti-rabbit secondary antibodies
(1:4,000; cat. no. ab6721; Abcam) were added for incubation at room
temperature for 2 h. The membranes were washed after incubation
with antibodies. Luminol Reagent and Peroxide Solution (EMD
Millipore) was prepared at a 1:1 ratio for colour development and
imaging. The ratio of the grey values of the target band and
control band indicated the relative protein expression. Relative
protein levels were semi-quantified using ImageJ 1.40 software
(National Institutes of Health). Each measurement was performed
three times to calculate an average value.
Statistical analysis
All data were processed by the SPSS version 20.0
software (IBM Corp.). Enumeration data were expressed as a ratio or
a percentage. Measurement data were presented as the mean ± SD and
the comparisons among groups was conducted using one-way ANOVA and
Tukey's multiple comparison test. The correlation analysis between
the expression levels of MMP-13 and NF-κBp65 were determined by
Pearson's correlation coefficient. The correlation between the
expression levels of MMP-13, NF-κBp65 and IL-1β with the
clinicopathological factors of patients were determined using
Spearman's correlation coefficient. P<0.05 was considered to
indicate a statistically significant difference.
Results
Severe KOA tissues exhibit
inflammatory cell infiltration and collagen deposition
Synovial tissues of the control group contained few
cells in the synovial intima with smooth cell surfaces, and cells
in the synovial lining and synovial subintima were evenly
distributed without inflammatory cell infiltration (Fig. 1A). Loosening synovial tissues, uneven
cell distribution, some proliferative collagenous fibres and
inflammatory cell infiltration were observed in the synovial
tissues of the mild KOA group (Fig.
1B), and substantial cell infiltration in the synovial lining,
irregular cell arrangement, inflammatory cell infiltration and
increased collagen disposition in the synovium were observed in the
synovial tissues of the severe KOA group (Fig. 1C).
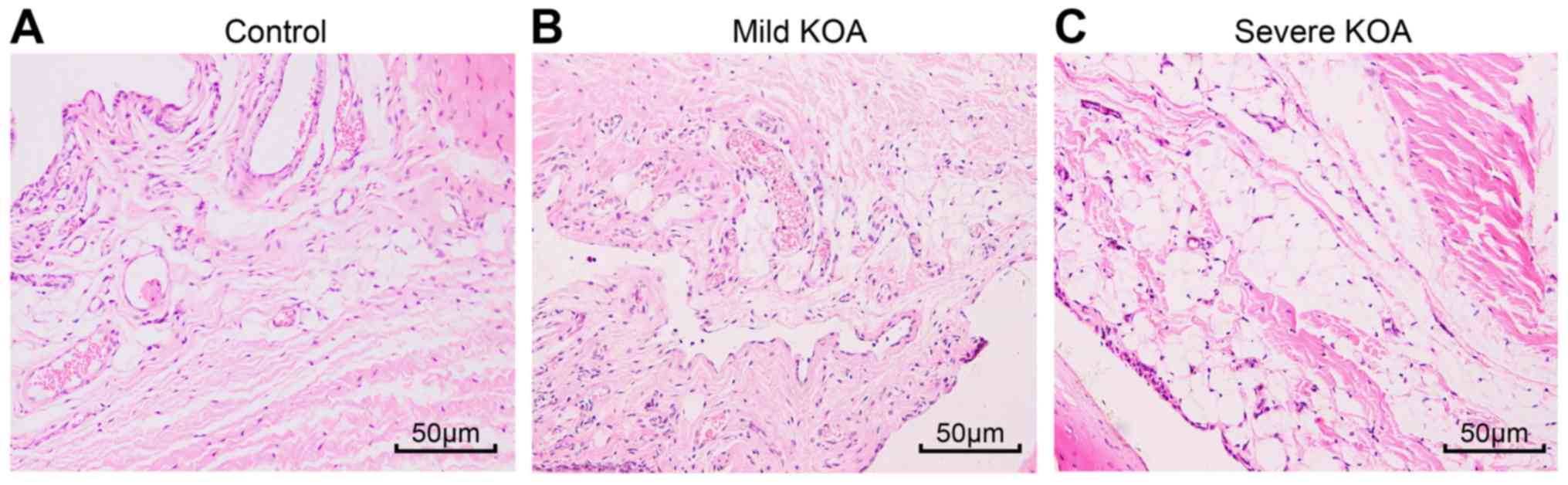 | Figure 1Haematoxylin and eosin staining of
synovial tissues reveals that the severe KOA group has the worst
inflammatory cell infiltration and the most collagen deposition.
(A) Control group, cells in synovial lining without inflammatory
cell infiltration. (B) Mild KOA group, looser synovial tissues,
irregular cell distribution, inflammatory cell infiltration. (C)
Severe KOA group, substantial cell infiltration, irregular cell
distribution, increased collagen deposition. Magnification, x200;
scale bars, 50 µm. KOA, knee osteoarthritis. |
Irregular cell arrangement and thin
cartilage in KOA
Safranin O-Fast Green staining was performed to
observe chondrocytes under a light microscope. The cartilage and
subchondral bone of the control group were stained red and blue,
and the cell nuclei were stained dark blue. Based on the boundary
of the tidemark along the cartilage and subchondral bone, the
control group exhibited many chondrocytes of uniform size that were
well arranged and distributed. The tidemark in the mild KOA group
was enlarged; the chondrocytes were not evenly stained and
exhibited an irregular arrangement. Safranin O-fast green staining
also revealed that the chondrocytes in the severe KOA group were
markedly disordered compared to the mild KOA group, presenting many
enlarged chondrocytes, irregular round and columnar cells, thin
trabecular bone, numerous cartilage spaces and a discontinuous
tidemark (Fig. 2).
 | Figure 2Safranin O-Fast Green staining of
synovial tissues to observe the morphology of chondrocytes. (A)
Control group, chondrocytes were well arranged and distributed. (B)
Mild KOA group, chondrocytes were not evenly stained and exhibited
an irregular arrangement. (C) Severe KOA group, chondrocytes were
markedly disordered, presenting many enlarged chondrocytes,
irregular round and columnar cells, thin trabecular bone, numerous
cartilage spaces and a discontinuous tidemark. Magnification, x100;
scale bars, 50 µm. KOA, knee osteoarthritis. |
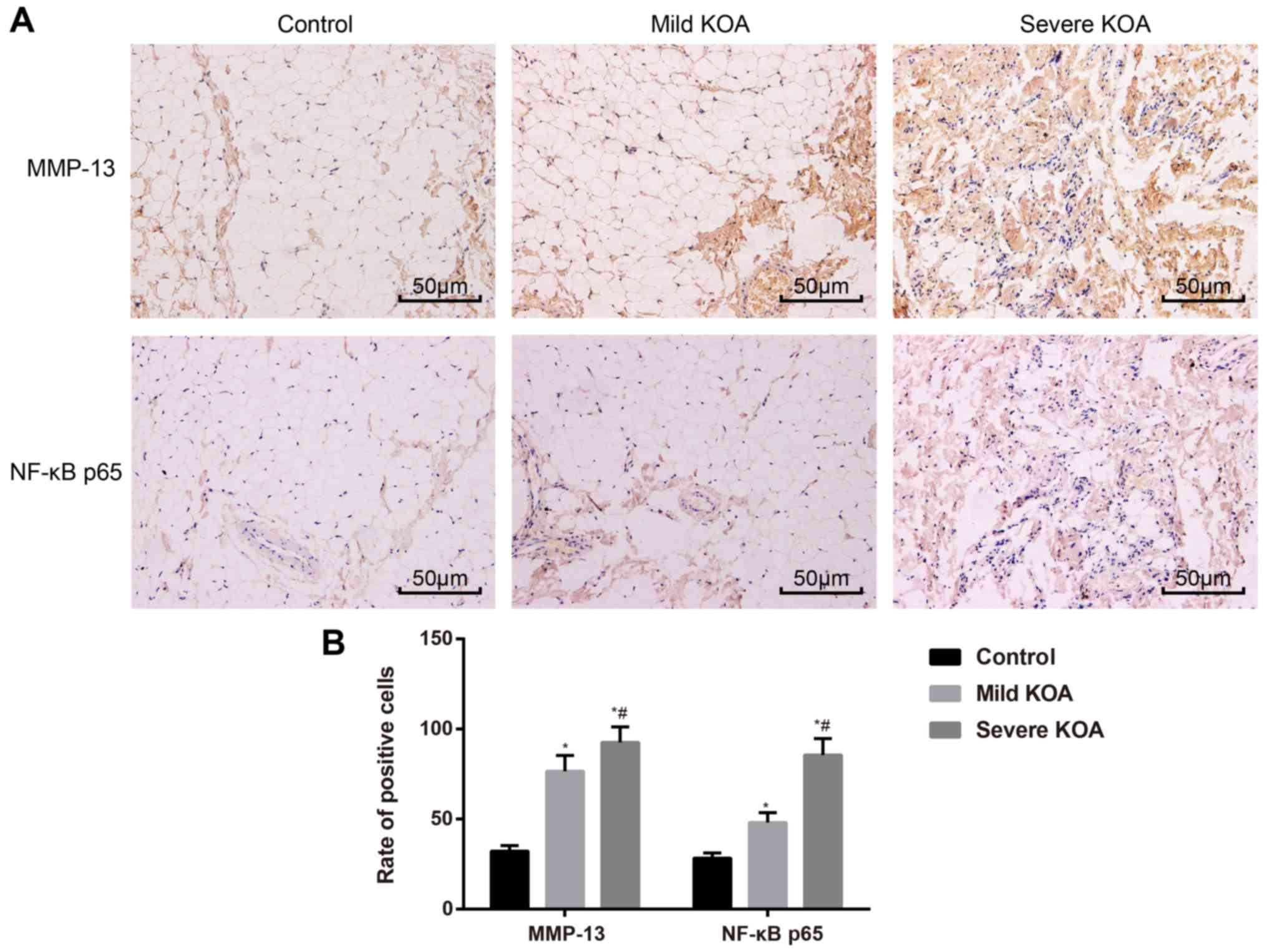
Expression of MMP-13 and NF-κBp65 is
associated with KOA severity
Immunohistochemistry was used to evaluate the
expression of MMP-13 and NF-κBp65 in synovial tissues. In the
synovial tissues of the case group, MMP-13 and NF-κBp65 stained
weakly or were stainless, while in the mild KOA group, MMP-13 and
NF-κBp65 were stained brown-yellow and were localized
intercellularly. In the severe KOA group, MMP-13 and NF-κBp65 were
stained brown-yellow or dark brown and localized both
intercellularly and in the cytoplasm (Fig. 3A). The rate of MMP-13-positive
staining in the three groups was as follows: (76.52±8.76%) in the
mild KOA group; (92.54±8.67%) in the severe KOA group; and
(32.14±3.23%) in the control group. The rate of NF-κBp65-positive
staining in the three groups is as follows: (48.12±5.44%) in the
mild KOA group; (85.56±9.16%) in the severe KOA group; and
(28.32±2.92%) in the control group. The rates of MMP-13- and
NF-κBp65-positive staining in the mild KOA group and the severe KOA
group were substantially higher than those of the control group
(all P<0.05). A comparison of positive rates of MMP-13 and
NF-κBp65 staining between the mild KOA group and severe KOA group
also revealed a significant difference (both P<0.05; Fig. 3B). These results support the
association of MMP-13 and NF-κBp65 expression with KOA
severity.
Positive correlation of MMP-13 and
NF-κBp65 in KOA
RT-qPCR and western blotting assessed the mRNA and
protein expression, respectively, of MMP-13, NF-κBp65 and IL-1β.
The results revealed that the mRNA and protein expression of
MMP-13, NF-κBp65 and IL-1β in the KOA groups were increased
compared to the control group (all P<0.05). The expression of
MMP-13, NF-κBp65 and IL-1β in the severe KOA group was higher than
the mild KOA group (all P<0.05). Correlation analysis revealed
that the expression of MMP-13 in KOA synovial tissues was
positively correlated with NF-κBp65 (Fig. 4).
Expression of MMP-13, NF-κBp65 and
IL-1β is positively correlated with KOA grade
Demographic data, such as sex, age, BMI, smoking
history, exercise habits and KOA grade, of patients with KOA were
recorded. These factors underwent correlation analyses with the
expression of MMP-13, NF-κBp65 and IL-1β. The results indicated
that the protein expression of MMP-13, NF-κBp65 and IL-lβ was
positively associated with the KOA grade (all P<0.05), but no
association was revealed for other factors, such as sex, age, BMI,
smoking history or exercise habits (Table II).
| Table IICorrelation of the expression of
MMP-13, NF-κBp65 and IL-1β with clinicopathological factors of
patients with knee osteoarthritis. |
Table II
Correlation of the expression of
MMP-13, NF-κBp65 and IL-1β with clinicopathological factors of
patients with knee osteoarthritis.
| Variables | | MMP-13 | NF-κBp65 | IL-lβ |
|---|
| Sex | r | 0.012 | 0.022 | 0.015 |
| | P-value | 0.665 | 0.496 | 0.581 |
| Age | r | 0.019 | 0.058 | 0.059 |
| | P-value | 0.897 | 0.312 | 0.692 |
| Body Mass Index | r | 0.123 | 0.202 | 0.143 |
| | P-value | 0.745 | 0.516 | 0.642 |
| Smoking history | r | 0.043 | 0.039 | 0.049 |
| | P-value | 0.543 | 0.475 | 0.611 |
| Exercise habits | r | 0.145 | 0.179 | 0.212 |
| | P-value | 0.321 | 0.411 | 0.549 |
| KOA grade | r | 0.443 | 0.398 | 0.541 |
| | P-value | 0.018 | 0.037 | 0.031 |
Discussion
Numerous studies have investigated the pathology of
KOA over the past decades, and a consensus was reached that
inflammation plays a central role in the progression of cartilage
damage (20). The present study
assessed three inflammation-related factors, MMP-13, IL-1β and
NF-κBp65, in synovial tissues of patients with KOA. The results of
the present study revealed that the severity of cartilage damage
was positively correlated with KOA progression. The expression of
MMP-13 and NF-κBp65 indicated that the activation of the NF-κB
signalling pathway occurs in KOA patients, which upregulates the
expression of MMP-13 and its downstream inflammation factor, IL-1β,
to accelerate the degradation of articular cartilage.
To support this hypothesis, the morphology of
chondrocytes in each group was first observed, and the results
revealed that patients with severe KOA had worse inflammatory cell
infiltration and collagen deposition. The expression of three
cytokines (MMP-13, IL-1β and NF-κBp65) in each group was next
assessed, and the expression of MMP-13, IL-1β and NF-κBp65 was
revealed to correlated with KOA severity. These results revealed
that the expression of these three factors indicated articular
cartilage damage. Chondrocytes stimulate the secretion of
cytokines, chemokines and adipokines, and numerous cell surface
receptors for these molecules exist; further, activation of these
receptors stimulates intracellular signalling pathways involved in
inflammatory and stress responses in chondrocytes in OA joints
(21). Many mediators are implicated
in the initiation and development of KOA, including
pro-inflammatory cytokines IL-1β and tumour necrosis factor-α
(TNF-α), which are synthesized locally by synovial cells and
chondrocytes and play a critical role in maintaining cartilage
damage in arthritis by creating an imbalance between the
degradation and repair processes of cartilage (22). IL-1β could influence the anabolism of
chondrocytes by increasing the production of MMPs, which are well
known for their role in suppressing cartilage matrix formation
(23).
MMP-13 has been revealed to play a role in the
physiological turnover of cartilage via cleavage of various ECM
molecules, such as type II collagen. Aberrant expression of MMP-13
was revealed to be closely related with numerous diseases,
including arthritis, cancer, atherosclerosis and fibrosis (24). One study on rheumatoid arthritis in
animal models revealed that rats receiving anti-IL-17 treatment
exhibited decreased MMP-13 expression and alleviated inflammation,
which supports the role of MMP-13 in the progression of arthritic
diseases (25). Notably, an animal
study evaluating rodents after hind limb immobilization revealed
that a loss of proteoglycan content was associated with increased
MMP-3, whereas joint movement prevented protease increase and
proteoglycan loss (26). SIRT1 is
also a key regulator of inflammation in mammalian cells via its
interaction with pro-inflammatory factors (22). A previous study also demonstrated a
role for NAD-dependent deacetylase sirtuin-1 (SIRT1) in OA
progression, which confirms that SIRT1 inactivation induced the
expression of the chondrocyte marker RUNX2 and the secretion of
MMP-13 in OA chondrocytes (16). The
correlation of MMP-13 and NF-κBp65 was also analysed in patients
with KOA. MMP-13 expression was positively correlated with
NF-κBp65, which indicates that the activation of the NF-κB
signalling pathway induced the production of MMP-13. Once the NF-κB
signalling pathway is activated (27), mechanical forces also trigger cell
surface mechanoreceptors, which induce mitogen-activated protein
kinase (MAPK) signalling (28); MAPK
signalling thus mediates the expression levels of downstream target
genes, such as MMP-13, NOS2, COX2, ADAMTS and IL-1β genes (21).
The present study however, also has its limitation.
As indicated in other studies, females are more prone to suffer
from KOA or hip osteoarthritis than males. However, the present
study revealed that sex was not a risk factor for KOA. This
inconsistency may be explained by the limited sample size of this
study or this result may be a random phenomenon that occurred
haphazardly. Although the present data failed to demonstrate sex as
a risk factor for KOA in this study, more research is required to
verify the effect of sex on KOA and attention will be paid on sex
distribution in KOA in our future study.
In conclusion, the evidence in the present study
indicated that the expression of MMP-13, NF-κBp65 and IL-1β was
correlated with the severity of KOA. A positive correlation between
MMP-13 and NF-κBp65 and KOA severity was revealed, which indicated
that activation of the NF-κB signalling pathway occurs in KOA
progression. The activation of this pathway upregulated the
expression of MMP-13 and its downstream inflammatory factor IL-1β,
which accelerates the degradation of articular cartilage. However,
the knowledge gained from studies of cartilage derived clinically
and from animal models has elucidated many important biological
processes that may be involved in KOA progression. More studies on
KOA pathologies are required to further investigate the
interactions between inflammation, genetic issues and other factors
in this disease.
Acknowledgements
Not applicable.
Funding
This work was financially supported by the Nanjing
Medical Science and Technique Development Foundation (grant nos.
YKK17242 and YKK18223).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FQL and QHZ designed and performed the experiments;
QHZ and RZ analyzed the data and wrote the manuscript; LPL and YXG
guided and supervised the experimental process, and interpreted the
results; RZ, ZW and ZPS collected the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was performed based on protocols
proposed by the Ethics Committee of Nanjing Luhe People's Hospital.
All patients signed written informed consent prior to participation
in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Srivastava R, Das SK, Goel G, Asthana A
and Agarwal GG: Does long term colchicine prevent degradation of
collagen fiber network in osteoarthritis? Int J Rheum Dis.
21:114–117. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Lluch E, Torres R, Nijs J and Van
Oosterwijck J: Evidence for central sensitization in patients with
osteoarthritis pain: A systematic literature review. Eur J Pain.
18:1367–1375. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
McAlindon TE, Bannuru RR, Sullivan MC,
Arden NK, Berenbaum F, Bierma-Zeinstra SM, Hawker GA, Henrotin Y,
Hunter DJ, Kawaguchi H, et al: OARSI guidelines for the
non-surgical management of knee osteoarthritis. Osteoarthritis
Cartilage. 22:363–388. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cross M, Smith E, Hoy D, Nolte S, Ackerman
I, Fransen M, Bridgett L, Williams S, Guillemin F, Hill CL, et al:
The global burden of hip and knee osteoarthritis: Estimates from
the global burden of disease 2010 study. Ann Rheum Dis.
73:1323–1330. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bayjensen AC, Abramson SB, Samuals J,
Byrjalsen I, Krasnokutsky S, Manonjensen T, Karsdal MA and Attur M:
SAT0437 osteoarthritis pain is differentially associated with
tissue degradation and joint inflammation. Osteoarthritis
Cartilage. 25(S353)2017.
|
|
6
|
Øiestad BE, Juhl CB, Eitzen I and Thorlund
JB: Knee extensor muscle weakness is a risk factor for development
of knee osteoarthritis. A systematic review and meta-analysis.
Osteoarthritis Cartilage. 23:171–177. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Roos EM, Herzog W, Block JA and Bennell
KL: Muscle weakness, afferent sensory dysfunction and exercise in
knee osteoarthritis. Nat Rev Rheumatol. 7:57–63. 2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Berenbaum F: Osteoarthritis as an
inflammatory disease (osteoarthritis is not osteoarthrosis!).
Osteoarthritis Cartilage. 21:16–21. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Daghestani HN, Pieper CF and Kraus VB:
Soluble macrophage biomarkers indicate inflammatory phenotypes in
patients with knee osteoarthritis. Arthritis Rheumatol. 67:956–965.
2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Neogi T, Guermazi A, Roemer F, Nevitt MC,
Scholz J, Arendt-Nielsen L, Woolf C, Niu J, Bradley LA, Quinn E, et
al: Association of joint inflammation with pain sensitization in
knee osteoarthritis: The multicenter osteoarthritis study.
Arthritis Rheumatol. 68:654–661. 2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hoesel B and Schmid JA: The complexity of
NF-κB signaling in inflammation and cancer. Mol Cancer.
12(86)2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Makarov SS: NF-kappa B in rheumatoid
arthritis: A pivotal regulator of inflammation, hyperplasia, and
tissue destruction. Arthritis Res. 3:200–206. 2001.PubMed/NCBI View
Article : Google Scholar
|
|
13
|
Mu N, Gu J, Huang T, Zhang C, Shu Z, Li M,
Hao Q, Li W, Zhang W, Zhao J, et al: A novel NF-κB/YY1/microRNA-10a
regulatory circuit in fibroblast-like synoviocytes regulates
inflammation in rheumatoid arthritis. Sci Rep.
6(20059)2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Xia Y, Darling EM and Herzog W: Functional
properties of chondrocytes and articular cartilage using optical
imaging to scanning probe microscopy. J Orthop Res. 36:620–631.
2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Ma CH, Wu CH, Jou IM, Tu YK, Hung CH,
Hsieh PL and Tsai KL: PKR activation causes inflammation and MMP-13
secretion in human degenerated articular chondrocytes. Redox Biol.
14:72–81. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yui N, Kobayashi H, Terauchi K, Yoshioka
H, Fujiya H, Niki H, Musha H and Yudoh K: The role of atp-activated
protein kinase(AMPK) in the chondrocyte energy balance and
IL-1β-induced production of MMP-13 in osteoarthritis(OA).
Osteoarthritis Cartilage. 24:S154–S155. 2016.
|
|
17
|
Kneer W, Rother M, Mazgareanu S and Seidel
EJ: European IDEA-033 study group. A 12-week randomized study of
topical therapy with three dosages of ketoprofen in
Transfersome® gel (IDEA-033) compared with the
ketoprofen-free vehicle (TDT 064), in patients with osteoarthritis
of the knee. J Pain Res. 6:743–753. 2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gabriel SM, Clifford AG, Maloney WJ,
O'Connell MK and Tornetta P III: Unloading the osteoarthritic knee
with a novel implant system. J Appl Biomech. 29:647–654.
2013.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408.
2001.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hayer S, Bauer G, Willburger M, Sinn K,
Alasti F, Plasenzotti R, Shvets T, Niederreiter B, Aschauer C,
Steiner G, et al: Cartilage damage and bone erosion are more
prominent determinants of functional impairment in longstanding
experimental arthritis than synovial inflammation. Dis Model Mech.
9:1329–1338. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Houard X, Goldring MB and Berenbaum F:
Homeostatic mechanisms in articular cartilage and role of
inflammation in osteoarthritis. Curr Rheumatol Rep.
15(375)2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Moon MH, Jeong JK, Lee YJ, Seol JW,
Jackson CJ and Park SY: SIRT1, a class III histone deacetylase,
regulates TNF-α-induced inflammation in human chondrocytes.
Osteoarthritis Cartilage. 21:470–480. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Song J, Jin EH, Kim D, Kim KY, Chun CH and
Jin EJ: MicroRNA-222 regulates MMP-13 via targeting HDAC-4 during
osteoarthritis pathogenesis. BBA Clin. 3:79–89. 2014.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Yamamoto K, Okano H, Miyagawa W, Visse R,
Shitomi Y, Santamaria S, Dudhia J, Troeberg L, Strickland DK,
Hirohata S, et al: MMP-13 is constitutively produced in human
chondrocytes and co-endocytosed with ADAMTS-5 and TIMP-3 by the
endocytic receptor LRP1. Matrix Biol. 56:57–73. 2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Shui XL, Lin W, Mao CW, Feng YZ, Kong JZ
and Chen SM: Blockade of IL-17 alleviated inflammation in rat
arthritis and MMP-13 expression. Eur Rev Med Pharmacol Sci.
21:2329–2337. 2017.PubMed/NCBI
|
|
26
|
Leong DJ, Gu XI, Li Y, Lee JY, Laudier DM,
Majeska RJ, Schaffler MB, Cardoso L and Sun HB: Matrix
metalloproteinase-3 in articular cartilage is upregulated by joint
immobilization and suppressed by passive joint motion. Matrix Biol.
29:420–426. 2010.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Nam J, Aguda BD, Rath B and Agarwal S:
Biomechanical thresholds regulate inflammation through the
NF-kappaB pathway: Experiments and modeling. PLoS One.
4(e5262)2009.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Fitzgerald JB, Jin M, Chai DH, Siparsky P,
Fanning P and Grodzinsky AJ: Shear- and compression-induced
chondrocyte transcription requires MAPK activation in cartilage
explants. J Biol Chem. 283:6735–6743. 2008.PubMed/NCBI View Article : Google Scholar
|