Introduction
Essential hypertension (EHT) is one of the major
risk factors for cardiovascular and cerebrovascular diseases.
Approximately 62% of cerebrovascular diseases and 49% of ischemic
heart diseases are attributed to suboptimal blood pressure
worldwide. Pathologically, EHT may cause endothelial dysfunction
and artery remodeling and accelerate atherosclerosis (1). Left ventricular (LV) diastolic
dysfunction frequently presents as organ damage caused by EHT and
this dysfunction may be overt in the early stages of EHT (2).
Endothelin (ET) is the strongest intrinsic
vasoconstrictor and calcitonin gene-related peptide (CGRP) was
proven to be the endogenous antagonist to ET. Angiotensin II
(AngII) is a well-evidenced contributor to the pathophysiology of
cardiovascular system disorders. These three proteins are widely
distributed, particularly in the nervous and cardiovascular systems
(3,4). The balance among these factors
regulates the proliferation and tone of vascular smooth muscle
cells, as well as endothelial cell function. Increased plasma ET-1
and AngII levels, decreased CGRP levels and endothelial dysfunction
were reported in spontaneously hypertensive rats (SHRs) and EHT
patients (5,6).
Antihypertensive drugs have been widely used in
clinical practice, exerting protective effects on target organs
beyond lowering the blood pressure. However, these effects are
dose-dependent and the side effects are not negligible, and may
include severe complications, e.g., renal failure or carotid
stenosis. Traditional Chinese Medicine (TCM), an important part of
complementary and alternative medicine, is widely accepted in
Eastern Asia, particularly China, Japan and Korea. With TCM
receiving an increasing amount of attention worldwide, studies are
accumulating on the clinical efficacy of TCM formulations in the
treatment of hypertension and the underlying mechanisms (7). Radix Puerariae, the dry root of
the leguminous plant Puerariae (Willd.) Ohwi, the most
effective active component of which is puerarin, is used as a TCM
drug. It has been confirmed that Radix Puerariae is able to
inhibit platelet aggregation and adhesion (8). It is also able to dilate peripheral
arteries and improve the microcirculation. However, its effects on
LV diastolic function and the balance among ET, AngII and CGRP have
remained to be elucidated.
The present study reported on a prospective clinical
trial investigating the utility of Radix Puerariae as an
additive to guideline-directed medical treatment (GDMT) to
alleviate LV diastolic dysfunction and improve the levels of plasma
ET, AngII and CGRP in patients with EHT.
Materials and methods
Study design and population
The present study was a randomized controlled trial.
It was performed according to the principles outlined in the
Declaration of Helsinki and the General Principles for Clinical
Research of New Drugs of Traditional Chinese Medicine issued by the
State Drug Administration in 2015. The study protocol was approved
by the Ethics Committee of Qilu Hospital of Shandong University
(Jinan, China). Written informed consent was obtained from all
participants.
The enrolled patients were aged 18-60 years and were
initially diagnosed with EHT at the Qilu Hospital of Shandong
University (Jinan, China) between November 2016 and June 2018. The
exclusion criteria were as follows: Pregnancy, lactation, secondary
hypertension, acute cerebral or cardiac events and severe renal or
hepatic failure, contraindications to guideline-recommended
antihypertensive drugs, tumors and psychiatric disorders.
Radix puerariae
The Radix Puerariae granules were purchased
from China Resources Sanjiu Medical & Pharmaceutical Co., Ltd.
(batch no. 1611001w). The content of puerarin was 2.9% according to
the outgoing test report for this batch, which meets the quality
control criteria of the Chinese Pharmacopoeia Commission from 2015,
which state that the puerarin content should not be <2.4%
(9).
Radix Puerariae is the dried root of
Puerariae (Willd.) Ohwi. To date, 122 compounds have been
isolated from Radix Puerariae, which are mainly classified
into five categories: Flavonoids, puerosides, coumarins,
triterpenoids and triterpene saponins. Among these, flavonoids,
including puerarin, daidzin and daidzein, are the most abundant
compounds.
Study procedure
Subjects were randomized into two groups, namely the
GDMT group and the GDMT plus Radix Puerariae (GDMT + RP)
group. GDMT included the monotherapy with any category among
Ang-converting enzyme inhibitors, Ang receptor blockers,
beta-receptor blockers, calcium channel blockers or diuretics which
was prescribed to all patients, according to international
guidelines on the management of hypertension (10). Measurement of blood pressure was
performed biweekly during follow-up visits until the end of the
12th week. The dosage and combination of the abovementioned drugs
were adjusted biweekly, if necessary, to achieve the blood pressure
goal of <140/90 mmHg. As for the strategy of drug adjustment, a
second drug from the 5 categories mentioned above was added in
sequence. If the blood pressure goal was not achieved with four
drug categories, including diuretics, the dosage of the prescribed
drugs was doubled or titrated. For patients in the GDMT + RP group,
15 g of Radix Puerariae granules was taken twice daily
orally in addition to GDMT throughout the entire study.
Echocardiography was performed and plasma levels of ET, AngII and
CGRP were determined at baseline and the end of the follow-up. A
flow chart of the study is provided in Fig. 1. The trial was terminated when the
subject experienced a severe increase in blood pressure, developed
severe comorbidities or exhibited poor compliance.
Blood pressure measurement
Blood pressure was measured using a mercurial
sphygmomanometer. Blood pressure records were acquired for each
patient from baseline to the end of the follow-up at biweekly
intervals. At each visit, blood pressure was measured 3 times on
the dominant arm in the sitting position after 10 min of rest and
the mean reading was recorded.
Plasma ET, AngII and CGRP testing
The plasma levels of ET, CGRP and AngII were
measured by radioimmunoassay at the Radiation and Immunology Center
of Beijing People's Liberation Army General Hospital, (Beijing,
China), according to methods described previously (11).
Detection of LV diastolic
dysfunction
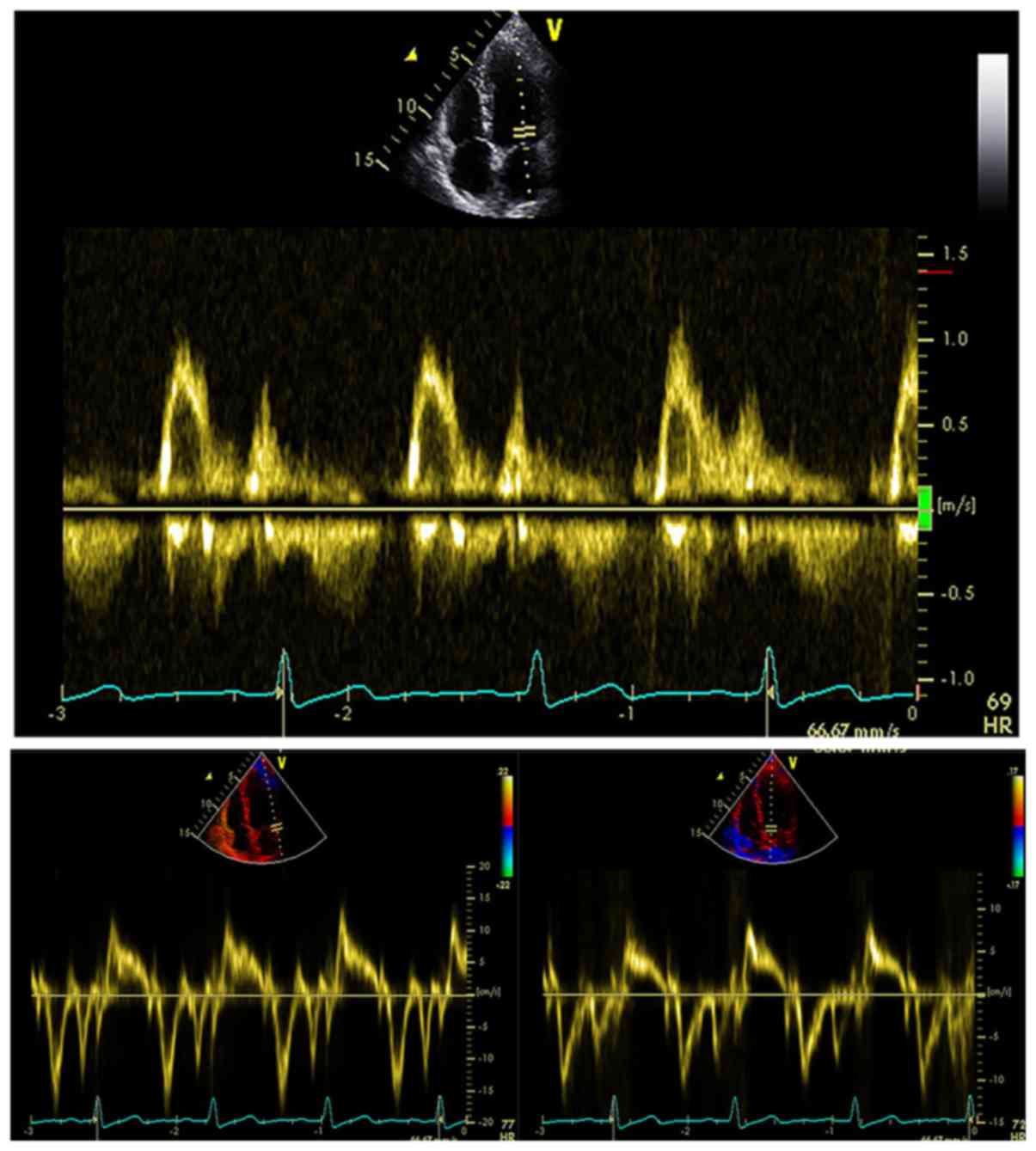
Echocardiography was performed using Vivid E90
equipment (GE Healthcare) with the M5s transducer (frequency,
1.5-4.5 MHz). The peak velocities of E and A waves across the
mitral valve in diastole were acquired by pulsed-wave Doppler
echocardiography. Mitral valve annulus velocity (e') was measured
by tissue Doppler imaging. The mean value of the septal and lateral
e' velocity was used to calculate the E/e' ratio (Fig. 2). The left atrial maximum volume
indexed to body surface area (LAv, ml/m2) was measured
from apical four- and apical two-chamber views with the area-length
method (Fig. 3). Body surface area
(BSA) was calculated with the formula of Dubois and Dubois: BSA
(m2)=[weight (Kg)0.425 x height
(cm)0.725] x 0.007184. Continuous-wave Doppler
echocardiography was adopted to measure the systolic regurgitation
velocity of the tricuspid valve (TRv) (Fig. 4). All parameters were measured 3
times and the mean value was calculated. E/e' >14, LAv >34
ml/m2 or TRv >2.8 m/sec were considered as indicators
of abnormal LV diastolic function. LV diastolic dysfunction was
diagnosed if at least two of the abovementioned indicators were
positive, according to the guidelines of the American Society of
Echocardiography (12).
Statistical analysis
Continuous variables are expressed as the mean ±
standard deviation and their normal distribution was tested with
the one-sample Kolmogorov-Smirnov test. Categorical data are
expressed as numbers and percentages. Differences between groups
were analyzed by t-test for normally distributed continuous
variables or Mann-Whitney U-test for non-normally distributed
continuous variables. For categorical data analysis, the
χ2 test was performed. Analysis of covariance was used
to analyze the interaction of Radix Puerariae and the blood
pressure-lowering effect on LV diastolic function. All the analyses
were performed with SPSS 13.0 (SPSS Inc.), and the P<0.05 was
considered to indicate a statistically significant difference.
Results
Demographic data
A total of 150 patients were included at the
beginning of the study and 7 patients were excluded as they were
lost to follow-up. Of the 143 patients included in the final
analysis, 75 (52%) were in the GDMT + RP group and 68 were in the
GDMT group. There were no significant differences between the two
groups in terms of patient sex, age, body mass index and smoking
history. Blood pressure was also comparable between groups at
baseline (Table I). LV diastolic
dysfunction was detected in 32% (n=24) of patients in the GDMT + RP
group and in 29% (n=20) in the GDMT group.
 | Table IDemographic data. |
Table I
Demographic data.
| Variable | Group GDMT + RP
(n=75) | Group GDMT
(n=68) |
|---|
| Age (years) | 40.4±13.2 | 39.8±11.5 |
| Male sex | 40(54) | 38(56) |
| BMI
(kg/m2) | 24.3±2.9 | 24.8±2.9 |
| Systolic blood
pressure (mmHg) | 147.9±13.3 | 144.5±13.1 |
| Diastolic blood
pressure (mmHg) | 94.0±9.2 | 94.4±8.4 |
| Smoking
history | 27(20) | 26(18) |
| Left ventricular
diastolic dysfunction | 24(32) | 20(29) |
| Guideline-directed
antihypertensive drugs | | |
|
Monotherapy | | |
|
ACEI | 5(7) | 4(6) |
|
ARB | 11(15) | 9(13) |
|
CCB | 7(9) | 5(7) |
|
BB | 3(4) | 2(3) |
|
Diuretics | 2(3) | (1) |
|
Double
therapy | | |
|
ACEI
+ CCB | 8(11) | 9(13) |
|
ACEI
+ diuretics | 4(5) | 5(7) |
|
ARB
+ CCB | 15(20) | 16(24) |
|
ARB
+ diuretics | 12(16) | 12(18) |
|
CCB
+ BB | 3(4) | 2(3) |
|
Triple
therapy | | |
|
ACEI
+ CCB + BB | 2(3) | 1(1) |
|
ARB
+ CCB + BB | 3(4) | 2(3) |
Blood pressure
At the end of the follow-up, the blood pressure was
lowered in the two groups compared with the baseline. In the two
groups, a similar strategy with antihypertensive drugs was applied.
Monotherapy with Ang receptor blockers and the combination of Ang
receptor blockers with calcium channel blockers or diuretics were
the most prevalent. Lower blood pressure (124.3±8.4/88.4±4.2 vs.
139.1±5.8/89.3±3.4 mmHg, P<0.001) was observed in the GDMT + RP
group compared with that in the GDMT group. The systolic blood
pressure-lowering effect was more prominent when Radix
Puerariae was added (-23.6 vs. -5.4 mmHg with P<0.001for
Δsystolic blood pressure, -5.6 vs. -5.1 mmHg for Δdiastolic blood
pressure; Table II).
| Table IIDifferences in Blood pressure between
the two groups at baseline and at the end of the follow-up. |
Table II
Differences in Blood pressure between
the two groups at baseline and at the end of the follow-up.
| | Group GDMT + RP
(n=75) | Group GDMT
(n=68) |
|---|
| Variable | Baseline | End | P-value | Baseline | End | P-value |
|---|
| SBP (mmHg) | 147.9±13.3 | 124.3±8.4 | <0.001 | 144.5±13.1 |
139.1±5.8a | <0.001 |
| DBP (mmHg) | 94.0±9.2 | 88.4±4.2 | <0.001 | 94.4±8.4 | 89.3±3.4 | <0.001 |
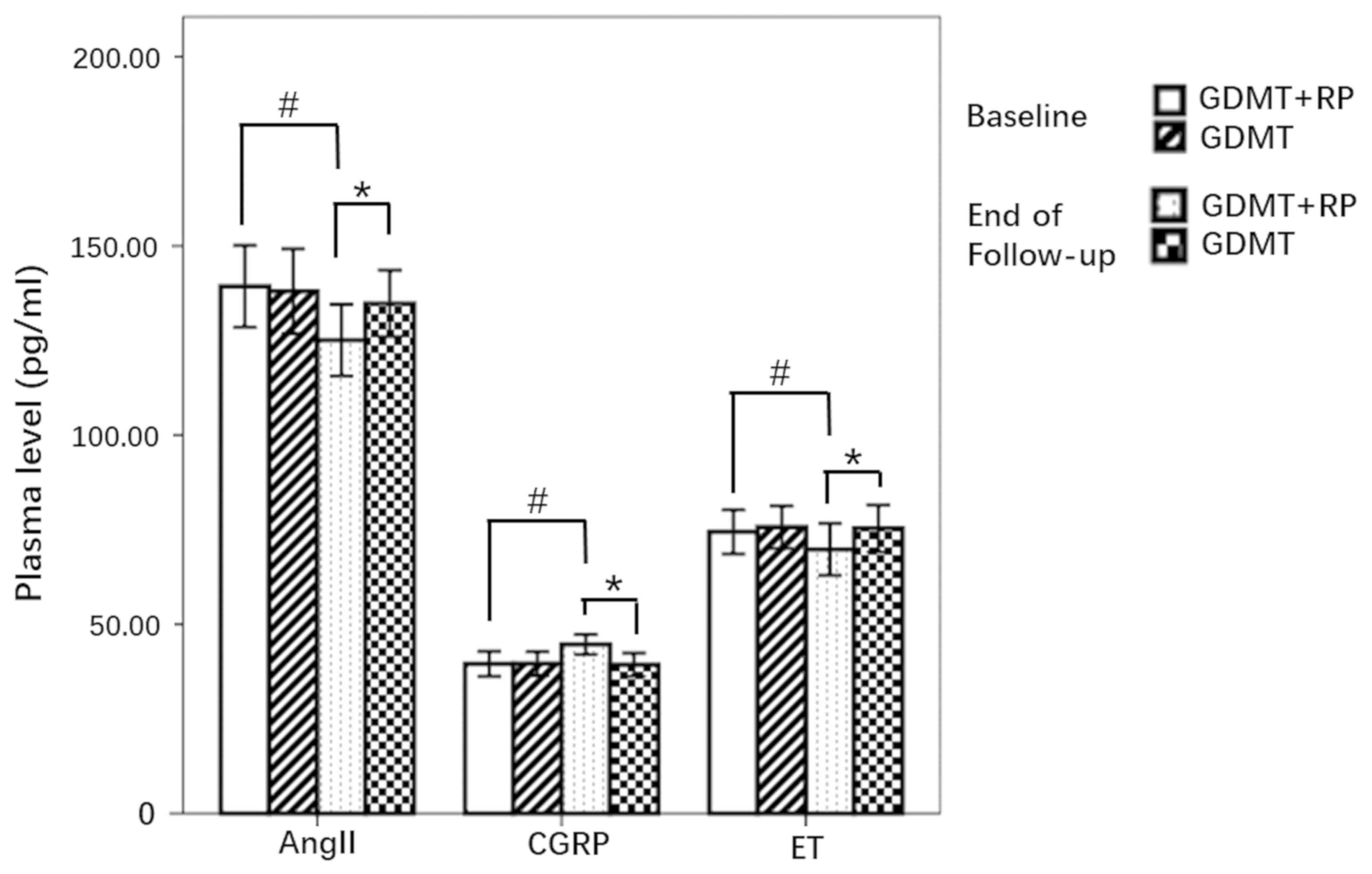
Plasma levels of ET, CGRP and
AngII
The plasma levels of ET, CGRP and AngII did not
significantly differ between the groups at baseline. At the end of
the follow-up in the GDMT + RP group, the plasma levels of ET and
AngII were found to be significantly reduced, whilst the plasma
level of CGRP increased significantly compared with those at
baseline. No such changes could be observed in the GDMT group. It
was notable that at the end of the follow-up, the plasma levels of
ET and AngII were also lower, whereas the level of CGRP was even
higher in GDMT + RP group compared with those in the GDMT group
(Fig. 5, Table III).
| Table IIIDifferences in plasma ET, CGRP and
Ang II levels between groups at baseline and at the end of the
follow-up. |
Table III
Differences in plasma ET, CGRP and
Ang II levels between groups at baseline and at the end of the
follow-up.
| | Group GDMT + RP
(n=75) | Group GDMT
(n=68) |
|---|
| Variable | Baseline | End | P-value | Baseline | End | P-value |
|---|
| ET | 74.43±5.84 | 69.78±6.87 | <0.001 | 75.7±5.61 |
75.32±6.23a | 0.730 |
| CGRP | 39.56±3.30 | 44.69±2.65 | <0.001 | 39.60±3.19 |
39.31±3.08a | 0.565 |
| AngII | 139.32±10.83 | 125.08±9.47 | <0.001 | 138.01±11.24 |
134.78±8.78a | 0.064 |
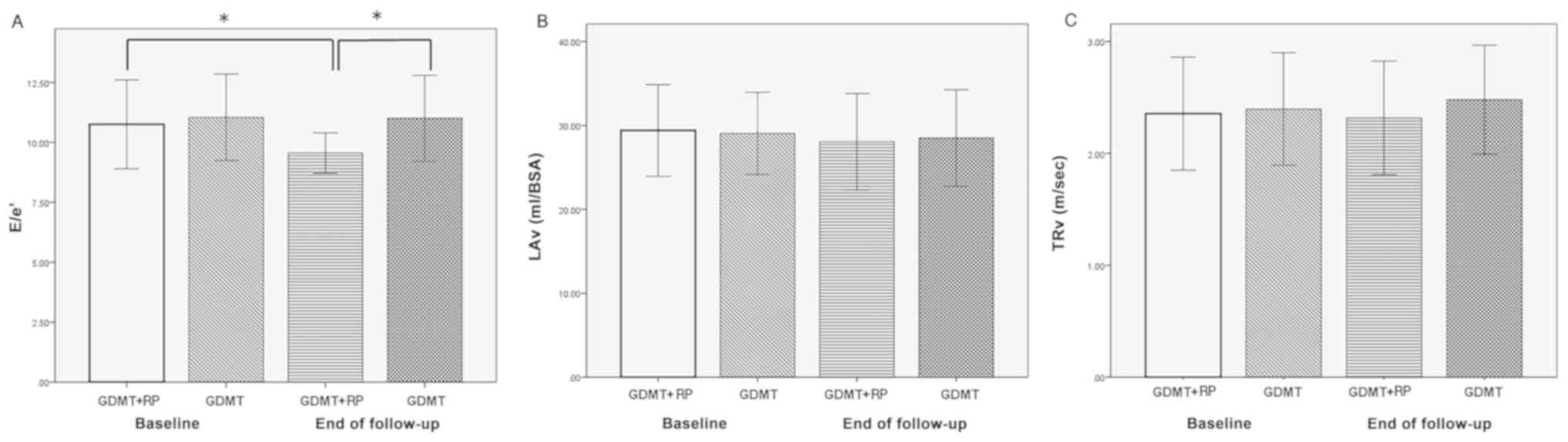
LV diastolic dysfunction
A significant E/e' ratio reduction was only observed
in the GMDT + RP group at the end of the study vs. baseline
(10.75±1.86 vs. 9.55±0.84, P<0.001; Fig. 6, Table
IV). No significant difference was identified in left atrial
volume at the end of week 12 in either group. The peak velocity of
tricuspid regurgitation tended to be marginally decreased in the
GDMT + RP group compared with that in the GMDT group (2.32±0.51vs.
2.48±0.49, P=0.05; Fig. 6, Table IV). However, the percentage of LV
diastolic dysfunction was significantly reduced in the GDMT + RP
group (32% vs. 9%, P=0.001). The improvement in LV diastolic
dysfunction was not obvious in the GDMT group, as the percentage
had only decreased from 29 to 21% at the end of the study
(P=0.115). This beneficial effect of Radix Puerariae was
independent of the blood pressure-lowering effect, as revealed by
analysis of covariance.
| Table IVDifferences in E/e', TRv and LAv
between groups at baseline and at the end of follow-up. |
Table IV
Differences in E/e', TRv and LAv
between groups at baseline and at the end of follow-up.
| | Group GDMT + RP
(n=75) | Group GDMT
(n=68) |
|---|
| Variables | Baseline | End | P-value | Baseline | End | P-value |
|---|
| E/e' | 10.75±1.86 | 9.55±0.84 | <0.001 | 11.04±1.80 |
11.00±1.79a | 0.900 |
| TRv (m/sec) | 2.36±0.51 | 2.32±0.51 | 0.641 | 2.40±0.50 |
2.48±0.49b | 0.309 |
| LAv (ml/BSA) | 29.41±5.47 | 28.06±5.76 | 0.143 | 29.06±4.91 | 28.52±5.75 | 0.554 |
| Left ventricular
dysfunction | 24(32) | 7(9) | 0.001 | 20(29) | 14(21) | 0.115 |
Discussion
In addition to blood pressure control, management of
hypertension should focus more on preventing damage of target
organs, including the heart, brain and kidney. For the
cardiovascular system, endothelial dysfunction and LV diastolic
dysfunction are the preconditions of arterial and cardiac
remodeling. ET, AngII and CGRP are important factors involved in
the pathological process of cardiac dysfunction and remodeling.
Antihypertensive drugs recommended by the guidelines on the
management of adult hypertension have been indicated to exert a
protective effect against cardiovascular remodeling (10). The present study demonstrated that
Radix Puerariae, when used as an adjuvant to GDMT, had
beneficial properties of improving LV diastolic function and
rebalancing ET, AngII and CGRP levels. Although the blood pressure
was lower in the GDMT + RP group, these beneficial effects of Radix
Puerariae may be independent of its blood pressure-lowering
action.
It was previously demonstrated that diastolic
function may be reduced in the early stages of hypertension
(13). This dysfunction may be
accurately detected by echocardiography. Choi et al
(14) observed a significant
increase in left atrial volume index and E/e' ratio in a remodeled
hypertension group. Furthermore, with the progression of myocardial
remodeling, the gradual increase in the E/e' ratio became more
overt, suggesting that diastolic function may be an important
method for predicting LV remodeling in patients with hypertension.
The tissue Doppler-derived e' velocity decreased with the decrease
in LV relaxation. The present study demonstrated that, after
treatment with Radix Puerariae in addition to standard
antihypertensive therapy, the E/e' ratio decreased more
significantly compared with that in the GDMT only group, suggesting
reduced LV filling pressure. This result is in accordance with the
results reported by Cai et al (15) and Gao et al (16). More importantly, it was evidenced
that the LV diastolic dysfunction may be improved by combination of
antihypertensive agents with Radix Puerariae.
ET is the most potent and longest-lasting vasoactive
peptide secreted by vascular endothelial cells (17). ET binds to its receptor ETA, thereby
leading to impaired endothelial cell function and proliferation of
vascular muscle cells and myocytes. It has been reported that there
is a negative association between plasma ET levels and mitral valve
E/A ratio, which is accompanied by LV diastolic dysfunction on
pulsed-wave Doppler echocardiography. This supports the role of ET
in LV diastolic function (18).
Blockade of ET receptor may suppress myocardial hypertrophy and
reduce the stiffness of the myocardium. Downregulation of ET
expression may counteract the cardiac remodeling and prove
beneficial in the therapy of heart failure by preserving the
ejection fraction (19).
CGRP is currently known as the strongest endogenous
vasodilating active polypeptide, which is widely distributed in the
nervous system (20). It has been
demonstrated that CGRP may antagonize the proliferation of vascular
endothelial cells and smooth muscle cells induced by ET, thereby
preventing the thickening of blood vessel walls and hypertension
(21). Plasma ET levels were
reported to be higher in patients with EHT compared with those in
normal controls, whereas the CGRP level was reported to be lower
(22). In the present study, it was
observed that conventional antihypertensive drugs may decrease
plasma AngII levels and increase the expression of CGRP, whilst
Radix Puerariae further reduced the ET levels. This suggests
that conventional antihypertensive therapy combined with the
application of Radix Puerariae may affect the plasma ET
level in hypertensive patients, thereby improving endothelial cell
function and exerting an antihypertensive therapeutic effect.
AngII is an important component of the renin-Ang
system. When combined with type I receptors, it may cause
pathological hypertrophy and fibrosis and generation of reactive
oxygen species within the arterial wall and the myocardium. This
contributes not only to increased blood pressure but also to
cardiovascular remodeling (23,24). As
reported by Choi et al (25),
following stimulation by AngII in a mouse model, the LV diastolic
function was hampered, as evidenced by increased E/e' ratio and
decreased e'/a' ratio determined by tissue Doppler
echocardiography. AngII is also a promoter of ET expression and an
inhibitor of CGRP expression (26).
Radix Puerariae is able to reduce plasma AngII levels and
downregulate the expression of AngII receptor type 1. Cai et
al (27) reported that total
flavone extracted from Radix Puerariae inhibited the plasma
Ang-converting enzyme and renin activities in a dose-dependent
manner, thus decreasing the blood pressure of 2K1C rats and SHRs.
In the present study, AngII levels were significantly reduced in
the Radix Puerariae group, which was also consistent with
the results of Cai et al (15). It may be inferred that the renin-Ang
system inhibitor drugs used in the present study are able to
alleviate the effect of AngII. However, the percentage of patients
receiving renin-Ang system inhibitors was comparable between the
two groups of the present study. At the end of the follow-up,
patients in the GDMT + RP group exhibited markedly lower levels of
AngII, ET and blood pressure compared with those in GDMT group. The
results suggest that Radix Puerariae was able to further
reduce the levels of AngII in patients receiving conventional
antihypertensive therapy. The reduction of AngII may act
synergistically along with the reduction of ET caused by Radix
Puerariae to regulate sympathetic nerve activity, achieving
a more significant antihypertensive effect, and improve endothelial
and LV diastolic dysfunction.
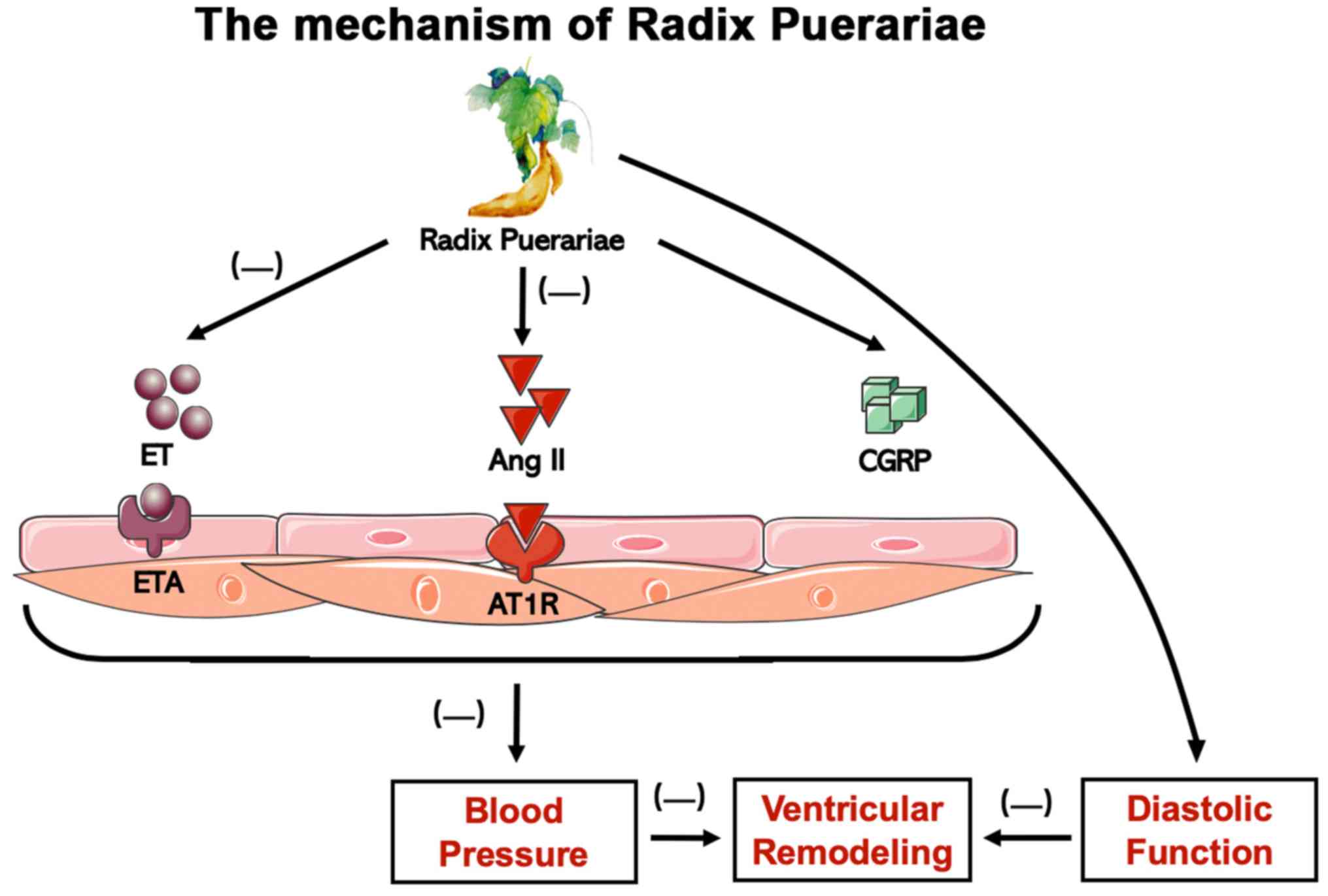
Ng et al (28)
reported that an aqueous extract comprising Radix Puerariae
exerted blood pressure-lowering effects in an in vivo SHR
animal model and the mechanism may be explained by its
endothelium-independent vasodilation via the opening of K(ATP), Kir
and K(v) channels. These results all favor the conclusions of the
present study. In addition, regulating potassium channels may also
contribute to the antihypertensive effect of Radix
Puerariae. The probable mechanism of action of Radix
Puerariae in benefitting patients with EHT is provided in
Fig. 7.
Although the biological mechanisms of TCM treatments
remain largely elusive, various patients benefit from this
practice. Recently, an increasing number of studies have been
focusing on the standardization of TCM diagnosis and the use of
gene sequencing technology for biomedical studies (7,29).
Combining TCM with precision medicine may broaden the field of
medical research, help better understand disease mechanisms and
promote advances in medicine.
In conclusion, the present study demonstrated that
Radix Puerariae, as an adjunct to antihypertensive therapy,
is able to regulate plasma endothelin, Ang II and CGRP levels in
patients with EHT, significantly lower blood pressure and improve
the clinical symptoms of hypertension. By improving LV diastolic
function and preventing the occurrence of hypertensive ventricular
remodeling, it may be a promising novel treatment for improving the
clinical symptoms of hypertension and preventing the development of
associated complications.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Science Foundation of China (grant no. 81571689), the Fundamental
Research Funds of Shandong University (grant no. 2018JC009) and the
National Key R&D Program of China (grant no.
2017YFC1700502).
Availability of data and materials
The datasets generated and/or analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
PZ conceived and designed the study. YL and SL
performed the experiments. ESL, YFX and FFY analyzed the data. PLB
contributed to the echocardiographic examination. YL wrote the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The protocols of the present study were approved by
the Ethics Committee of Qilu Hospital of Shandong University
(Jinan, China) and written informed consent was obtained from all
participants.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bruno RM, Masi S, Taddei M, Taddei S and
Virdis A: Essential hypertension and functional microvascular
ageing. High Blood Press Cardiovasc Prev. 25:35–40. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Georgiopoulos G, Tsioufis CP, Kalos T,
Magkas N, Rousos D, Chrysohoou C, Sarri G, Syrmali K,
Georgakopoulos P and Tousoulis D: Serum uric acid is independently
associated with diastolic dysfunction in apparently healthy
subjects with essential hypertension. Curr Vasc Pharmacol.
17:99–106. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mordi I, Mordi N, Delles C and Tzemos N:
Endothelial dysfunction in human essential hypertension. J
Hypertens. 34:1464–1472. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mihalj M, Tadzic R, Vcev A, Rucevic S and
Drenjancevic I: Blood pressure reduction is associated with the
changes in oxidative stress and endothelial activation in
hypertension, regardless of antihypertensive therapy. Kidney Blood
Press Res. 41:721–735. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Gao Y, Yang J and Wang S: Effects of
telemetry implantation surgery on blood pressure and its underlying
mechanism. Clin Exp Hypertens. 38:359–364. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Laffin LJ and Bakris GL: Endothelin
antagonism and hypertension: An evolving target. Semin Nephrol.
35:168–175. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hao P, Jiang F, Cheng J, Ma L, Zhang Y and
Zhao Y: Traditional Chinese medicine for cardiovascular disease:
Evidence and potential mechanisms. J Am Coll Cardiol. 69:2952–2966.
2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Li H, Luo K and Hou J: Inhibitory effect
of Puerariae Radix flavones on platelet-derived growth
factor-BB-induced proliferation of vascular smooth muscle cells via
PI3K and ERK pathways. Exp Ther Med. 9:257–261. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chinese Pharmacopoeia Commission:
Pharmacopoeia of the people's Republic of China (Part 1). China Med
Sci Technol Press, pp333, 2015.
|
|
10
|
James PA, Oparil S, Carter BL, Cushman WC,
Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML,
MacKenzie TD, Ogedegbe O, et al: 2014 evidence-based guideline for
the management of high blood pressure in adults: Report from the
panel members appointed to the eighth joint national committee (JNC
8). JAMA. 311:507–520. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Mao H, Gao F, Mao H, Zhang L, Guan W, Zhou
Q, Zhang Y, Bai L and Zhan Y: Changes of plasma calcitonin
gene-related peptide and other substances in healthy people who
rush to high altitude. Zhong Guo Ying Yong Sheng Li Xue Za Zhi.
22:315–316. 2006.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
12
|
Nagueh SF, Smiseth OA, Appleton CP, Byrd
BF III, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC,
Klein AL, Lancellotti P, et al: Recommendations for the evaluation
of left ventricular diastolic function by echocardiography: An
update from the American society of echocardiography and the
European association of cardiovascular imaging. J Am Soc
Echocardiogr. 29:277–314. 2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Marwick TH, Gillebert TC, Aurigemma G,
Chirinos J, Derumeaux G, Galderisi M, Gottdiener J, Haluska B,
Ofili E, Segers P, et al: Recommendations on the use of
echocardiography in adult hypertension: A report from the European
association of cardiovascular imaging (EACVI) and the American
society of echocardiography (ASE). J Am Soc Echocardiogr.
28:727–754. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Choi J, Pyun WB and Shin GJ: The influence
of the left ventricular geometry on the left atrial size and left
ventricular filling pressure in hypertensive patients, as assessed
by echocardiography. Korean Circ J. 39:145–150. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cai RL, Li M, Xie SH, Song Y, Zou ZM, Zhu
CY and Qi Y: Antihypertensive effect of total flavone extracts from
Puerariae Radix. J Ethnopharmacol. 133:177–183.
2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Gao Z, Wei B and Qian C: Puerarin
injection for treatment of unstable angina pectoris: A
meta-analysis and systematic review. Int J Clin Exp Med.
8:14577–14594. 2015.PubMed/NCBI
|
|
17
|
Rautureau Y and Schiffrin EL: Endothelin
in hypertension: An update. Curr Opin Nephrol Hypertens.
21:128–136. 2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Valero-Munoz M, Li S, Wilson RM,
Boldbaatar B, Iglarz M and Sam F: Dual endothelin-A/endothelin-B
receptor blockade and cardiac remodeling in heart failure with
preserved ejection fraction. Circ Heart Fail. 9:pii:
e003381:2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kim YJ, Goh CW, Byun YS, Lee YH, Lee JB
and Shin YO: Left ventricular hypertrophy, diastolic dysfunction,
pulse pressure, and plasma ET-1 in marathon runners with
exaggerated blood pressure response. Int Heart J. 54:82–87.
2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kee Z, Kodji X and Brain SD: The role of
calcitonin gene related peptide (CGRP) in neurogenic vasodilation
and its cardioprotective effects. Front Physiol.
9(1249)2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Watts SW: Serotonin and sensory nerves:
Meeting in the cardiovascular system. Vascul Pharmacol. 63:1–3.
2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Inrig JK, Van Buren P, Kim C,
Vongpatanasin W, Povsic TJ and Toto R: Probing the mechanisms of
intradialytic hypertension: A pilot study targeting endothelial
cell dysfunction. Clin J Am Soc Nephrol. 7:1300–1309.
2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ramalingam L, Menikdiwela K, LeMieux M,
Dufour JM, Kaur G, Kalupahana N and Moustaid-Moussa N: The renin
angiotensin system, oxidative stress and mitochondrial function in
obesity and insulin resistance. Biochim Biophy Acta Mol Basis Dis.
1863:1106–1114. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Wen KC, Lin SP, Yu CP and Chiang HM:
Comparison of Puerariae Radix and its hydrolysate on
stimulation of hyaluronic acid production in NHEK cells. Am J Chin
Med. 38:143–155. 2010.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Choi YS, de Mattos AB, Shao D, Li T,
Nabben M, Kim M, Wang W, Tian R and Kolwicz SC Jr: Preservation of
myocardial fatty acid oxidation prevents diastolic dysfunction in
mice subjected to angiotensin II infusion. J Mol Cell Cardiol.
100:64–71. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Te Riet L, van Esch JH, Roks AJ, van den
Meiracker AH and Danser AH: Hypertension:
Renin-angiotensin-aldosterone system alterations. Circ Res.
116:960–975. 2015.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Cai SA, Hou N, Zhao GJ, Liu XW, He YY, Liu
HL, Hua YQ, Li LR, Huang Y, Ou CW, et al: Nrf2 is a key regulator
on puerarin preventing cardiac fibrosis and upregulating metabolic
enzymes UGT1A1 in rats. Front Pharmacol. 9(540)2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ng CF, Koon CM, Cheung DW, Lam MY, Leung
PC, Lau CB and Fung KP: The anti-hypertensive effect of Danshen
(Salvia miltiorrhiza) and Gegen (Pueraria lobata) formula in rats
and its underlying mechanisms of vasorelaxation. J Ethnopharmacol.
137:1366–1372. 2011.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Liu BC and Ji G: Sparking thinking:
Studying modern precision medicine will accelerate the progression
of traditional chinese medicine patterns. J Altern Complement Med.
23:502–504. 2017.PubMed/NCBI View Article : Google Scholar
|