Introduction
Hip fracture is an international public health
concern. There are approximately 1.5 million cases of hip fracture
worldwide each year. By the year 2050, it is estimated that there
will be 3.9 million hip fractures worldwide and >700,000 cases
in the United States (1). Femoral
neck fracture is one of the most common types of hip fracture.
Surgical treatment is usually required clinically. The purpose of
surgical treatment is to immediately relieve pain, accelerate
recovery and reduce the occurrence rate of surgical complications
(2,3). Currently, hip replacement surgery is
widely used for the treatment of severe hip injury, and it is a
very safe, reliable and effective surgical method. The 10-year
survival rate of patients with the implant is >99% (4). Hip replacement can successfully
restore the function and activity of the patient's joints, relieve
pain and improve the quality of life; however, the recovery of hip
joint function following surgery differs (5,6).
MicroRNAs (miRNAs or miRs), a type of small
non-coding RNA with approximately 22 nucleotides in length,
participate in the regulation of gene expression and are a type of
broad-spectrum RNA that coordinates biological processes (7). A series of miRNAs has been proven to
regulate the osteogenic activity and bone formation of osteoblasts,
and play an important role in regulating bone regeneration and
remodeling (8). miR-142 has been
proven to be overexpressed in various pathological environments,
such as in atherosclerosis (9),
inflammation of the small intestine (10) and gastric cancer (11). Bone morphogenetic protein 2 (BMP-2)
is a hydrophobic acidic glycoprotein, which can induce the
proliferation, differentiation and migration of interstitial cells,
promote cartilage and bone formation, and can efficiently induce
osteogenic activity (12). A number
of studies have investigated the roles of miR-142 and BMP-2 in
osteoarthritis. For example, in the study by Chen et al
(13), miR-142-3p expression was
shown to be significantly decreased in patients with osteoporosis,
and was thus considered to be a biomarker for osteoporosis. Mi
et al (14) also revealed
that BMP-2 played an important role in fracture healing, and the
loss of chondrocyte BMP-2 induced the formation of cartilaginous
callus to be prolonged, thus affecting the process of fracture
healing. The receptor activator of NF-κB ligand
(RANKL)/osteoprotegerin (OPG) system is the main signaling pathway
regulating the differentiation and function of osteoblasts and
osteoclasts. RANKL is a cytokine synthesized and secreted by
osteoblasts, which can promote bone resorption (15,16).
Fractures can cause bone metabolism in the body. OPG originates
from bone cells and is an important cytokine in bone metabolism. It
can be combined with RANKL competitively to inhibit bone resorption
and promote bone healing (17).
The present study analyzed the changes in serum
miR-142 and BMP-2 in patients with femoral neck fracture before and
after hip replacement surgery in order to examine their association
with the post-operative recovery of the patients, as well as their
association with RANKL and OPG.
Materials and methods
General data
From April 2013 to August 2016, 142 patients with
femoral neck fracture undergoing total hip replacement at the
Orthopedic Department of The No. 4 Hospital, Jinan, Shandong were
selected as the research group. According to the American Society
of Anesthesiologists (ASA) classification standard, there were 101
cases classified as class II and 41 as class III. The
classification referred to the definition of the ASA grade
published by Davenport (18). The
inclusion criteria were as follows: Patients who met the diagnostic
criteria for femoral neck fracture (19); patients with obvious hip pain,
longitudinal percussion pain of the lower limbs, unilateral
displaced femoral neck fracture shown by X-ray; patients who
underwent total hip replacement surgery at the Orthopedic
Department of The No. 4 Hospital, met ASA Class II-III standards,
and patients without major organ dysfunction. The exclusion
criteria were as follows: Patients who received hemiarthroplasty in
the Orthopedic Department of The No. 4 Hospital; if the surgery was
performed >1 week after the fracture; patients had a history of
hip replacement, pathological fracture, lumbar disease and
rheumatoid arthritis; patients with complications such as
cerebrovascular diseases, mental diseases, peripheral neuropathy,
connective tissue disease, endocrine metabolic disease, severe
respiratory system disease, hematopoietic dysfunction, malignant
tumor and infectious diseases; patients who used immunosuppressive,
anti-inflammatory and hormone drugs over the past 1 month; patients
died within 6 months after operation. In addition, 50 cases of
healthy individuals who underwent a physical examination during the
same time period were selected as the control group, including 23
males and 27 females, aged 43-76 years, with an average age of
60.1±8.6 years. Patients without dysfunction of the heart, kidneys,
liver and other important organs, and with a normal physical
examination were selected for the present study. Patients
understood the situation of the study and signed informed consent
forms. This study did not violate any ethical regulations. The plan
was submitted to the Ethics Committee of Orthopedic Department of
The No. 4 Hospital for review and was implemented after obtaining
approval.
Surgical treatment
The patients in the research group underwent total
hip replacement surgery (20), and
all patients underwent surgery within 1 week after sustaining
injury. Prior to the surgery, a hip X-ray film was obtained to
confirm the fracture status and evaluate the length, size and
femoral offset reconstruction during the surgery. Skin preparation
was performed for continuous epidural general anesthesia, the
patients were placed in the lateral position and the lateral hip
joint approach was performed. The attachment of 1/3 of gluteus
medius muscle was cut and the structures of the hip joint were
exposed. The femoral head was removed following osteotomy. The
acetabulum was removed and the acetabulum prosthesis was placed.
The neck was removed and the distance of the femur was
approximately 12 cm. The femoral stem prosthesis was implanted and
the lateral soft tissue of the hip joint was reconstructed. A
routine cleaning inspection was performed, and the incision was
closed after cleaning. Following surgery, 3 g of anti-infective
cefotaxime sodium and 0.5 g of metronidazole were administered
intravenously twice a day. Low molecular weight heparin (LMWH) was
injected subcutaneously 8 h following surgery, and then once a day
for 3 days.
Evaluation index
The Harris score (21) was applied 6 months after surgery to
evaluate the recovery of the patients, including mobility (47
points), pain (44 points), deformity (4 points) and joint mobility
surface (5 points). The total score was 100 points. The high score
was closely related to better joint function and recovery.
According to the Harris scale, the scoring was as follows:
Excellent, >90 points; good, 80-90 points; fair, 70-79 points;
and poor, <70 points.
Detection method
Following admission into the control group or prior
to surgery, at 1 month after surgery and at 6 months after surgery
in the research group, 5 ml of venous blood was obtained from the
patients on an empty stomach and placed in a vacuum blood
collection vessel without anticoagulant, and centrifuged at 1,006.2
x g for 10 min (with a centrifuge radius of 10 cm and a centrifuge
temperature of 4˚C), and the separated upper serum was placed in EP
tube for later use.
Serum total RNA was extracted according to the
instructions provided with the TRIzol total RNA kit (Invitrogen;
Thermo Fisher Scientific, Inc.). The concentration and purity of
the RNA were determined using a 751GD UV-Vis spectrophotometer
(Beijing Qianming Gene Technology Co., Ltd.). A total of 2 µl of
total RNA was used to prepare the cDNA according to the
instructions provided with the PrimeScript RT Master Mix (RR036A;
Takara Biotechnology Co., Ltd.). The synthesized cDNA sample was
placed at -20˚C for later use. The primer sequences were designed
and synthesized by Tiangen biotech (Beijing) Co., Ltd. and are
listed in Table I. The PCR reaction
included the following: 10 µl of 2X miR qPCR Mix, 0.4 µl of
upstream primer, 0.4 µl of downstream primer, 0.4 µl of sample, the
sample was supplemented to 20 µl with dd water (RNase- and
DNase-free). The PCR reaction conditions were as follows:
Pre-denaturation at 90˚C for 3 min, denaturation at 90˚C for 20
sec, annealing at 60˚C for 20 sec, and extension at 72˚C for 40
sec, for a total of 40 cycles. Amplification data analysis was
performed using 7500 fluorescence quantitative PCR (Applied
Biosystems; Thermo Fisher Scientific, Inc.) manufacturer software,
and the results were analyzed using the
2-ΔΔCq method (22).
 | Table ISequences of primers used in the
present study. |
Table I
Sequences of primers used in the
present study.
| Gene | Upstream primer
sequence | Downstream primer
sequence |
|---|
| miR-142 |
5'-TGCAGGGCAGCAGAGGAGCTGCTGT-3' |
5'-ACTGAGGCTCTGGGCAGTCAGGACC-3' |
| U6 |
5'-CTCGCTTCGGCAGCACA-3' |
5'-AACGCTTCACGAATTTGCGT-3' |
| BMP-2 |
5'-AACCTGCAACAGCCAACT-3' |
5'-GCTCAGTGTAGCCCAGGAT-3' |
| GAPDH |
5'-GAAGGTCGGAGTCAACGG-3' |
5'-GCTCAGTGTAGCCCAGGAT-3' |
The levels of serum BMP-2, RANKL and OPG were
detected by enzyme-linked immunosorbent assay (ELISA) as previously
described, and the detection was carried out with reference to the
operating instructions of the human BMP-2, RANKL, OPG ELISA kits
(all purchased from Zhenyu Biotechnology Co., Ltd.). The OD value
of each well was detected at a 450 nm wavelength using an Elx-800
enzyme linked immunosorbent assay meter (BioTek Instruments, Inc.),
and the BMP-2, RANKL, OPG levels were calculated. Serum alanine
aminotransferase (ALT), aspartate aminotransferase (AST),
creatinine (Cre) and blood glucose (Glu) levels were detected using
a BS-280 automatic biochemical analyzer. White blood cell (WBC)
count and platelet (PLT) count in peripheral blood were measured
using a BC-5000 automatic blood cell analyzer. D-dimer, prothrombin
time (PT), thrombin time (TT) and activated partial thromboplastin
time (APTT) were detected using a C2000-A automatic coagulation
analyzer. The instrument was purchased from Vedeng Medical Co.,
Ltd.
Statistical analysis
SPSS 20.0 (IBM Corp.) was used for statistical
analysis, and GraphPad Prism 6 software was used to visualize the
data. Measurement data are expressed as the mean ± standard
deviation (means ± SD). The t-test was used for comparisons between
2 groups of normally distributed data, and a paired t-test was used
for comparisons before and after treatment. Non-normal distribution
data are expressed as M(P25-P75). Count data are expressed as
numbers and percentages [n (%)], and the Chi-squared
(χ2) test was used for the comparisons of count data
between groups. Repeated measurement analysis of variance was used
for data comparisons at multiple time points, one-way analysis of
variance was used for comparisons among multiple groups of mean.
Pairwise comparisons were conducted using the Tukey's test.
Pearson's correlation analysis was used for correlation analysis
among continuous data, while Spearman's correlation analysis was
used for grade data. ROC was used to plot the diagnostic value of
preoperative serum miR-142 and BMP-2 levels for clinical efficacy.
The P-value less than 0.05 was regarded as statistical
significance.
Results
General data of the research group and
control group
No significant differences were observed in sex,
age, body mass index (BMI), smoking history, alcohol consumption
history, alanine aminotransferase (ALT), aspartate aminotransferase
(AST), white blood cell (WBC) count, D-dimer, prothrombin time
(PT), thrombin time (TT), activated partial thromboplastin time
(APTT), platelet (PLT) count, creatinine (Cre) and blood glucose
(Glu) between the research group and control group (P>0.05)
(Table II).
| Table IIGeneral data of the study group and
control group. |
Table II
General data of the study group and
control group.
| Category | Study group
(n=142) | Control group
(n=50) | t/χ2
value | P-value |
|---|
| Sex | | | 0.810 | 0.368 |
|
Male | 55 (38.73) | 23 (46.00) | | |
|
Female | 87 (61.27) | 27 (54.00) | | |
| Age (years) | 62.3±6.9 | 60.1±8.6 | 1.814 | 0.071 |
| BMI
(kg/m2) | 23.4±4.2 | 22.8±4.9 | 0.831 | 0.407 |
| Smoking
history | | | 0.364 | 0.546 |
|
Yes | 31 (21.83) | 13 (26.00) | | |
|
No | 111 (78.17) | 37 (74.00) | | |
| Alcohol consumption
history | | | 0.142 | 0.706 |
|
Yes | 35 (24.65) | 11 (22.00) | | |
|
No | 107 (75.35) | 39 (78.00) | | |
| ALT (U/l) | 26.58
(16.86-34.22) | 22.98
(16.12-29.86) | 1.349 | 0.179 |
| AST (U/l) | 17.29
(12.26-21.90) | 16.26
(11.98-24.48) | 0.169 | 0.866 |
| WBC
(x109/l) | 5.38±2.26 | 5.26±2.48 | 0.315 | 0.753 |
| D-dimer
(µl/ml) | 0.40
(0.19-0.61) | 0.36
(0.18-0.50) | 1.513 | 0.132 |
| PT (sec) | 11.35±2.26 | 10.61±3.53 | 1.700 | 0.091 |
| TT (sec) | 14.49±1.67 | 14.25±1.37 | 0.913 | 0.362 |
| APTT (sec) | 33.51±5.92 | 34.56±6.47 | 1.053 | 0.294 |
| PLT
(x109/l) | 199.37
(156.01-237.51) | 169.67
(146.21-220.44) | 1.501 | 0.135 |
| Cre (µmol/l) | 70.10
(45.15-108.23) | 79.42
(50.51-106.24) | 0.268 | 0.789 |
| Glu (mmol/l) | 5.62±0.81 | 5.51±1.02 | 0.770 | 0.442 |
| Surgery duration
(min) | 95.4±17.6 | - | - | - |
| ASA
classification | | | - | - |
|
II | 101 (71.13) | - | | |
|
III | 41 (28.87) | - | | |
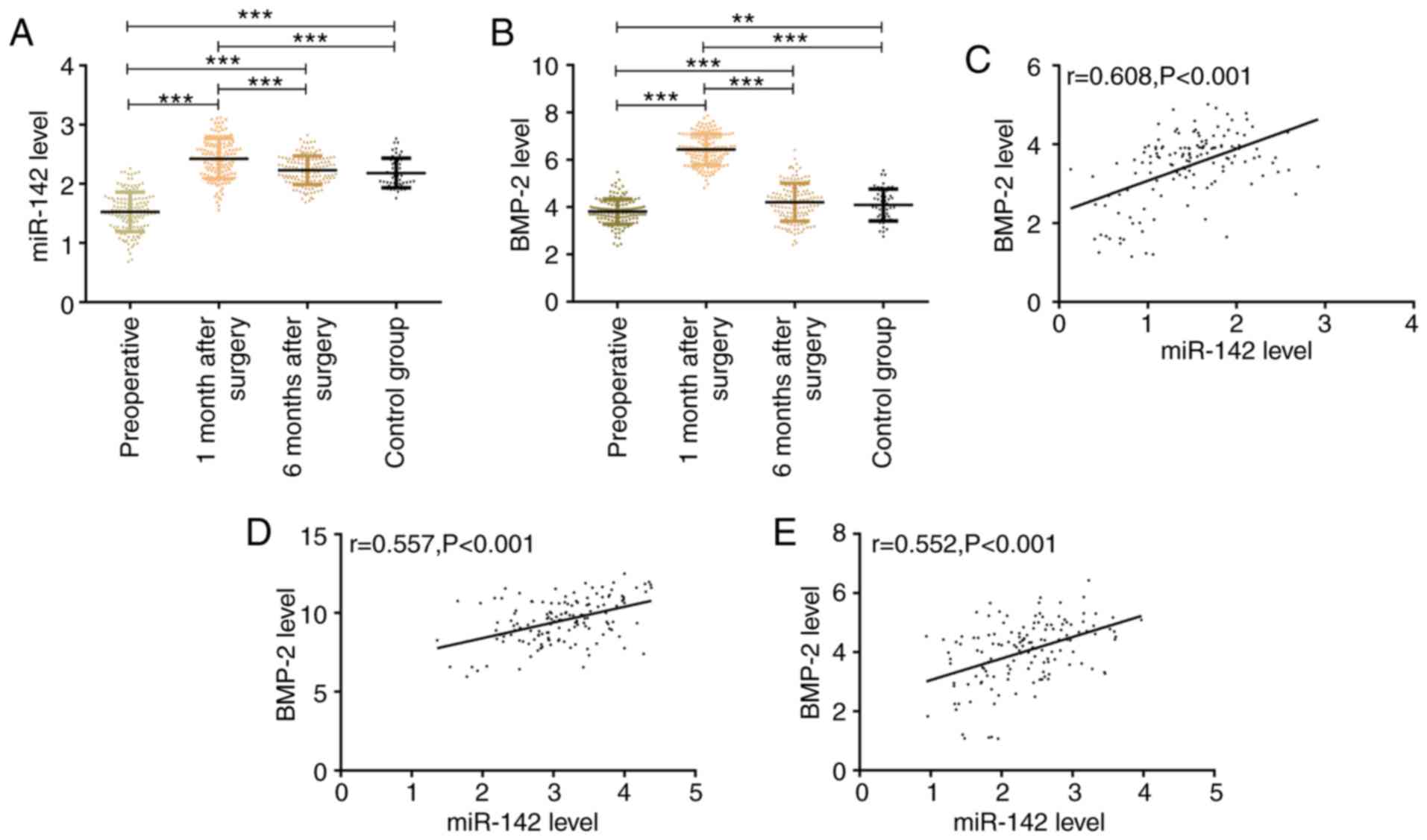
Serum miR-142 and BMP-2 levels in the
research group and control group before and after surgery
The levels of serum miR-142 and BMP-2 in the
research group before surgery were significantly lower than those
in the control group (P<0.01). The levels of serum miR-142 and
BMP-2 in the research group at 1 month after surgery were
significantly higher than those before surgery and those at 6
months after surgery, and those in the research group were higher
than those in the control group at 1 month after surgery
(P<0.001). The levels of serum miR-142 and BMP-2 in the research
group reached peak levels at 1 month after surgery, and no
significant differences were found between the research group and
control group at 6 months after surgery (P>0.05). The results of
Pearson's correlation analysis revealed that the serum miR-142
level in the research group positively correlated with the BMP-2
level before surgery, at 1 month after surgery and at 6 months
after surgery (P<0.001) (Fig.
1).
Value of pre-operative and
post-operative levels of miR-142 and BMP-2 in evaluating patient
recovery
Following surgical treatment, the recovery in the
research group was assessed as excellent in 60 cases, good in 55
cases, fair in 21 cases and poor in 6 cases. At 6 months after
surgery, the Harris score was used to evaluate the recovery status
of the patients. According to the recovery status, 60 patients
exhibited excellent recovery and 55 patients exhibited good recover
and were selected as Group A (115 cases); in addition, 21 patients
exhibited a fair recovery and 6 patients exhibited a poor recovery
and were selected as Group B (27 cases). The levels of serum
miR-142 and BMP-2 in group A before treatment were significantly
higher than those in group B (P<0.01). ROC curve analysis of
pre-operative serum miR-142 and BMP-2 levels for the evaluation of
the recovery of patients following of hip arthroplasty was created.
The AUC values of serum miR-142 and BMP-2 for evaluating the
recovery of patients were 0.911 and 0.861, respectively. Further
evaluation of the association between post-operative miR-142 and
BMP-2 levels with recovery revealed that the serum miR-142 and
BMP-2 levels in group A were significantly higher than those in
group B at 1 month after surgery. According to the recovery, the
patients with poor, fair, good and excellent recovery were set to
1, 2, 3 and 4 respectively. According to Spearman's correlation
coefficient, serum miR-142 and BMP-2 levels positively correlated
with recovery effect (Fig. 2 and
Table III).
| Table IIIROC curve analysis of pre-operative
serum miR-142 and BMP-2 in predicting the recovery of hip
arthroplasty. |
Table III
ROC curve analysis of pre-operative
serum miR-142 and BMP-2 in predicting the recovery of hip
arthroplasty.
| Indicator | AUC | 95% CI | Std. Error | Cut-off | Sensitivity
(%) | Specificity
(%) |
|---|
| miR-142 | 0.911 | 0.843-0.978 | 0.034 | 1.81 | 95.65 | 88.89 |
| BMP-2 (ng/ml) | 0.861 | 0.789-0.933 | 0.037 | 3.97 | 81.36 | 85.18 |
Serum RANKL and OPG levels before and
after surgery in the research group
The serum RANKL levels in the research group were
6.19±1.44 and 11.15±2.36 ng/ml before surgery and at 1 month after
surgery, respectively (Fig. 3A);
the OPG levels were 5.36±1.26 and 9.47±2.28 ng/ml before and at 1
month after surgery, respectively (Fig.
3B). The levels of serum RANKL and OPG in the research group at
1 month after surgery were significantly higher than those before
surgery (P<0.001) (Fig. 3A and
B). Pearson's correlation analysis
revealed that the levels of serum miR-142 and BMP-2 positively
correlated with the levels of RANKL and OPG before surgery and at 1
month after surgery (P<0.001) (Fig.
3C-J).
Discussion
In recent years, the total number of hip fractures
has markedly increased, and the majority of these occur in Asia
(23). Clinically, the effect of
hip replacement is to relieve joint pain, restore and improve joint
mobility. However, some patients will suffer from dislocation of
prosthesis bone and aseptic loosening after surgery, which prevents
hip joint function returning to normal levels (24,25).
Therefore, it is of utmost significance for the post-operative
rehabilitation of patients to identify indicators related to the
recovery after surgery and to intervene in time.
In recent years, miRNAs and fractures have received
extensive attention (26,27). In the study by Liu et al
(28), miR-137 was shown to prevent
ALP activity and expression by inhibiting the expression of
leucine-rich repeated G protein-coupled receptor 4, making patients
prone to osteoporosis fracture. In the study by Yao et al
(29), miR-185 was shown to inhibit
the growth and proliferation of osteoblasts during fracture healing
by downregulating Wnt/β-catenin axis targeting the PTH gene. These
studies demonstrated that miRNAs play an important role in
fractures. However, there are few studies available to date on the
role of miR-142 in hip arthroplasty. BMP-2 is a classical
morphogenetic hormone and a molecule that affects cell behavior. In
mesenchymal cells, the level of BMP-2 affects myogenesis,
lipogenesis, cartilage formation and bone formation (30). In the present study, the levels of
serum miR-142 and BMP-2 in the pre-operative research group were
significantly lower than those in the control group, and
significantly increased at 1 month after surgery. There was a
positive correlation between the serum miR-142 and BMP-2 levels
both pre-operatively and post-operatively. The levels of serum
miR-142 and BMP-2 in patients with femoral neck fracture were
significantly lower than those in healthy individuals. The levels
of serum miR-142 and BMP-2 in patients following hip replacement
were significantly increased. In the study by Zhao et al
(31), the level of miR-142-5p in
older mice was lower than that in young mice, and was closely
related to the age-related bone healing delay, while miR-142-5p was
significantly upregulated and related to the generation of active
osteoblasts during bone healing. However, Tsuji et al
(32) considered that BMP-2 was an
essential component of fracture repair. In bones lacking BMP-2, the
earliest steps of fracture healing seemed to be blocked, and BMP-2
was identified as a necessary endogenous medium for fracture
repair. This may be that following a fracture, the production of
miR-142 and BMP-2 decreased, and miR-142 and BMP-2 played a similar
role as fracture repair media in the recovery process; however, the
mechanisms involved remain unclear. It was hypothesized that
miR-142 and BMP-2 may be involved in the healing process of bone
formation following hip replacement surgery. The Harris score is a
standard for the curative effect of artificial total hip joint,
which can reflect the recovery of hip joint function of patients
and evaluate the therapeutic effect of hip joint replacement
(33). The results of this study
showed that preoperative serum miR-142 and BMP-2 levels had certain
predictive value for the postoperative recovery of patients. As hip
replacement surgery is a hip joint repair surgery for patients with
fractures (34), the joint function
of the patients was markedly improved, and the levels of serum
miR-142 and BMP-2 were markedly increased at 1 month after surgery;
thus, the fracture site may be at the recovery stage at this time.
In addition, the levels of serum miR-142 and BMP-2 in patients with
good recovery were significantly higher than those in patients with
poor recovery at 1 month after surgery, and the serum miR-142 and
BMP-2 levels positively correlated with the recovery effect.
Therefore, the observation of miR-142 and BMP-2 has evaluating
value for the recovery of patients following hip replacement
surgery. In the study by de Amorim et al (35), the decrease in the number of RANKL-
and OPG-positive cells in the tissues of diabetic rats following
tibial fracture was significantly lower than that of healthy rats,
and the number of RANKL- and OPG-positive cells was still
significantly lower than that of the control group at 14 days.
However, in the study by Wang et al (36), the levels of RANKL and OPG were
significantly increased at 4 weeks after surgery for fracture
patients, which was closely related to the fracture healing
process. In the present study, the levels of serum RANKL and OPG in
the research group were lower than those in the control group
before surgery, but increased significantly at 1 month after
surgery. The levels of miR-142 and BMP-2 positively correlated with
the levels of RANKL and OPG before and after surgery. miR-142 and
BMP-2 may thus participate in bone formation and bone metabolism,
although the underlying mechanisms remain to be further
explored.
Of course, the present study has certain
limitations. Firstly, the present study did not observe the
complications of patients following hip replacement surgery.
Secondly, the regulatory mechanisms of miR-142 and BMP-2 in hip
replacement surgery for patients with femoral neck fracture were
not observed. These deficiencies need to be further attended to in
future research.
In conclusion, the present study demonstrates that
the pre-operative serum miR-142 and BMP-2 levels are valuable for
evaluating the recovery of patients with femoral neck fracture
following hip replacement surgery. In addition, at 1 month after
surgery, the levels of both miR-142 and BMP-2 were related to the
recovery of the patients, and positively correlated with the RANKL
and OPG levels.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HG wrote the manuscript, and analyzed and
interpreted the patient data. XW performed PCR and ELISA, and
assisted with the statistical analysis. Both authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Fourth Hospital of Jinan. Patients who
participated in this research, signed informed consent forms and
had complete clinical data. Signed written informed consents were
obtained from the patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yu L, Wang Y and Chen J: Total hip
arthroplasty versus hemiarthroplasty for displaced femoral neck
fractures: Meta-analysis of randomized trials. Clin Orthop Relat
Res. 470:2235–2243. 2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Lowe JA, Crist BD, Bhandari M and Ferguson
TA: Optimal treatment of femoral neck fractures according to
patient's physiologic age: An evidence-based review. Orthop Clin
North Am. 41:157–166. 2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Miyamoto RG, Kaplan KM, Levine BR, Egol KA
and Zuckerman JD: Surgical management of hip fractures: An
evidence-based review of the literature. II: Intertrochanteric
fractures. J Am Acad Orthop Surg. 16:596–607. 2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Alnahhal A, Aslam-Pervez N and Sheikh HQ:
Templating Hip arthroplasty. Open Access Maced J Med Sci.
7(672)2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Nemes S, Lind D, Cnudde P, Bülow E,
Rolfson O and Rogmark C: Relative survival following hemi-and total
hip arthroplasty for hip fractures in Sweden. BMC Musculoskelet
Disord. 19(407)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Maratt JD, Gagnier JJ, Butler PD,
Hallstrom BR, Urquhart AG and Roberts KC: No difference in
dislocation seen in anterior vs posterior approach total hip
arthroplasty. J Arthroplasty. 31:127–130. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Li D, Liu J, Guo B, Liang C, Dang L, Lu C,
He X, Cheung HY, Xu L, Lu C, et al: Osteoclast-derived exosomal
miR-214-3p inhibits osteoblastic bone formation. Nat Commun.
7(10872)2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lian JB, Stein GS, van Wijnen AJ, Stein
JL, Hassan MQ, Gaur T and Zhang Y: MicroRNA control of bone
formation and homeostasis. Nat Rev Endocrinol.
8(212)2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Xu R, Bi C, Song J, Wang L, Ge C, Liu X
and Zhang M: Upregulation of miR-142-5p in atherosclerotic plaques
and regulation of oxidized low-density lipoprotein-induced
apoptosis in macrophages. Mol Med Rep. 11:3229–3234.
2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Schaefer JS, Montufar-Solis D, Vigneswaran
N and Klein JR: Selective upregulation of microRNA expression in
peripheral blood leukocytes in IL-10-/- mice precedes expression in
the colon. J Immunol. 187:5834–5841. 2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zhang X, Yan Z, Zhang J, Gong L, Li W, Cui
J, Liu Y, Gao Z, Li J, Shen L and Lu Y: Combination of hsa-miR-375
and hsa-miR-142-5p as a predictor for recurrence risk in gastric
cancer patients following surgical resection. Ann Oncol.
22:2257–2266. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Wang YK, Yu X, Cohen DM, Wozniak MA, Yang
MT, Gao L, Eyckmans J and Chen CS: Bone morphogenetic
protein-2-induced signaling and osteogenesis is regulated by cell
shape, RhoA/ROCK, and cytoskeletal tension. Stem Cells Dev.
21:1176–1186. 2011.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Chen J, Li K, Pang Q, Yang C, Zhang H, Wu
F, Cao H, Liu H, Wan Y, Xia W, et al: Identification of suitable
reference gene and biomarkers of serum miRNAs for osteoporosis. Sci
Rep. 6(36347)2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Mi M, Jin H, Wang B, Yukata K, Sheu TJ, Ke
QH, Tong P, Im HJ, Xiao G and Chen D: Chondrocyte BMP2 signaling
plays an essential role in bone fracture healing. Gene.
512:211–218. 2013.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Krege JH, Lane NE, Harris JM and Miller
PD: PINP as a biological response marker during teriparatide
treatment for osteoporosis. Osteoporos Int. 25:2159–2171.
2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Martin TJ and Sims NA: RANKL/OPG; Critical
role in bone physiology. Rev Endocr Metab Disord. 16:131–139.
2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Cassuto J, Folestad A, Göthlin J, Malchau
H and Kärrholm J: The key role of proinflammatory cytokines, matrix
proteins, RANKL/OPG and Wnt/β-catenin in bone healing of hip
arthroplasty patients. Bone. 107:66–77. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Davenport DL, Bowe EA, Henderson WG, Khuri
SF and Mentzer RM Jr: National surgical quality improvement program
(NSQIP) risk factors can be used to validate American Society of
Anesthesiologists Physical Status Classification (ASA PS) levels.
Ann Surg. 243:636–644. 2006.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Wright NC, Saag KG, Dawson-Hughes B,
Khosla S and Siris ES: The impact of the new National Bone Health
Alliance (NBHA) diagnostic criteria on the prevalence of
osteoporosis in the USA. Osteoporos Int. 28:1225–1232.
2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sprague S, Bhandari M, Heetveld MJ, Liew
S, Scott T, Bzovsky S, Heels-Ansdell D, Zhou Q, Swiontkowski M and
Schemitsch EH: FAITH Investigators: Factors associated with
health-related quality of life, hip function, and health utility
after operative management of femoral neck fractures. Bone Joint J.
100-B:361–369. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Singh JA, Schleck C, Harmsen S and
Lewallen D: Clinically important improvement thresholds for Harris
Hip Score and its ability to predict revision risk after primary
total hip arthroplasty. BMC Musculoskelet Disord.
17(256)2016.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408.
2001.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Abdel MP, Watts CD, Houdek MT, Lewallen DG
and Berry DJ: Epidemiology of periprosthetic fracture of the femur
in 32 644 primary total hip arthroplasties: A 40-year experience.
Bone Joint J. 98:461–467. 2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Mahmood SS, Mukka SS, Crnalic S,
Wretenberg P and Sayed-Noor AS: Association between changes in
global femoral offset after total hip arthroplasty and function,
quality of life, and abductor muscle strength: A prospective cohort
study of 222 patients. Acta Orthop. 87:36–41. 2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Angerame MR, Fehring TK, Masonis JL, Mason
JB, Odum SM and Springer BD: Early failure of primary total hip
arthroplasty: Is surgical approach a risk factor? J Arthroplasty.
33:1780–1785. 2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lee WY, Li N, Lin S, Wang B, Lan HY and Li
G: miRNA-29b improves bone healing in mouse fracture model. Mol
Cell Endocrinol. 430:97–107. 2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Waki T, Lee SY, Niikura T, Iwakura T,
Dogaki Y, Okumachi E, Oe K, Kuroda R and Kurosaka M: Profiling
microRNA expression during fracture healing. BMC Musculoskelet
Disord. 17(83)2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Liu X and Xu X: MicroRNA-137 dysregulation
predisposes to osteoporotic fracture by impeding ALP activity and
expression via suppression of leucine-rich repeat-containing
G-protein-coupled receptor 4 expression. Int J Mol Med.
42:1026–1033. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Yao CJ, Lv Y, Zhang CJ, Jin JX, Xu LH,
Jiang J, Geng B, Li H, Xia YY and Wu M: MicroRNA-185 inhibits the
growth and proliferation of osteoblasts in fracture healing by
targeting PTH gene through down-regulating Wnt/β-catenin axis: In
an animal experiment. Biochem Biophys Res Commun. 501:55–63.
2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Rogers MB, Shah TA and Shaikh NN: Turning
bone morphogenetic protein 2 (BMP2) on and off in mesenchymal
cells. J Cell Biochem. 116:2127–2138. 2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Zhao R, Zhu Y and Sun B: Exploration of
the Effect of mmu-miR-142-5p on Osteoblast and the Mechanism. Cell
Biochem Biophys. 71:255–260. 2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Tsuji K, Bandyopadhyay A, Harfe BD, Cox K,
Kakar S, Gerstenfeld L, Einhorn T, Tabin CJ and Rosen V: BMP2
activity, although dispensable for bone formation, is required for
the initiation of fracture healing. Nat Genet.
38(1424)2006.PubMed/NCBI View
Article : Google Scholar
|
|
33
|
Singh JA, Schelck C, Harmsen S and
Lewallen D: AB0757 Clinically important improvement thresholds for
Harris hip score and its ability to predict revision risk after
primary total hip arthroplasty. BMC Musculoskelet Disord.
17(256)2016.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Higgins BT, Barlow DR, Heagerty NE and Lin
TJ: Anterior vs. posterior approach for total hip arthroplasty, a
systematic review and meta-analysis. J Arthroplasty. 30:419–434.
2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
de Amorim FP, Ornelas SS, Diniz SF,
Batista AC and da Silva TA: Imbalance of RANK, RANKL and OPG
expression during tibial fracture repair in diabetic rats. J Mol
Histol. 39(401)2008.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Wang XF, Zhang YK, Yu ZS and Zhou JL: The
role of the serum RANKL/OPG ratio in the healing of
intertrochanteric fractures in elderly patients. Mol Med Rep.
7:1169–1172. 2013.PubMed/NCBI View Article : Google Scholar
|