Introduction
Acute kidney injury (AKI; also referred to as acute
kidney failure or acute renal failure) is defined as a sudden loss
of renal function. AKI has a high incidence in critically-ill
patients, particularly those in intensive care units (1). Delayed diagnosis of AKI may result in
deterioration of renal function, long hospital stays or even death.
In addition, sepsis has been consistently found to be an important
contributing factor of AKI (2,3).
Mortality associated with septic AKI is significantly higher than
that of non-septic AKI, and >50% of AKI cases are considered
septic (4,5). Sepsis-induced AKI has been
independently associated with an increased risk of longer hospital
stays and mortality (6). Thus, due
to the high morbidity and mortality of septic AKI, early prediction
and diagnosis of this condition is essential.
Neutrophil gelatinase-associated lipocalin (NGAL)
has been identified as a biomarker for AKI, as its concentration is
significantly increased in urine, plasma and serum following
ischemic kidney injury (7). NGAL is
a 24-kDa secreted glycoprotein, which was originally purified from
a culture of murine kidney cells infected with simian virus 40
(7,8). Zhang et al (6) demonstrated that NGAL was an
independent predictor of AKI that is not influenced by age, sex,
ethnicity, severity of injury and factors unrelated to renal
function. Serum, urine and plasma are the main fluid types used in
the diagnosis of AKI via the detection of NGAL (7). Previous studies have evaluated the
diagnostic value of NGAL and its potential value in predicting
outcomes of treatment, such as renal replacement therapy (6,9)
Although NGAL appears to hold promise in the prediction of AKI
among patients with suspected sepsis, the diagnostic accuracy of
NGAL according to sample source (serum, urine or plasma) is still
unclear. In the present study, the diagnostic performance of NGAL
for AKI was evaluated using a meta-analysis. The secondary
objective of this study was to identify an optimal source of NGAL
for the diagnosis of sepsis-induced AKI.
Materials and methods
Literature search
The present study was based on previously published
articles and, as such, did not require ethics approval or patient
consent. Eligible studies were identified using an electronic
database search and by cross-checking the references of relevant
papers up to June 2020. The PubMed, ScienceDirect, Web of Science,
Embase, OVID, Cochrane Library and China National Knowledge
Infrastructure databases were systematically searched using search
terms, including ‘neutrophil gelatinase-associated lipocalin’,
‘sepsis’, ‘severe sepsis and septic shock’, ‘acute kidney injury’,
‘serum NGAL’, ‘plasma NGAL’ and ‘urine NGAL’, as well as their
abbreviations and synonyms and all possible combinations. Moreover,
references from the retrieved articles were also reviewed to
identify additional relevant studies.
Study selection
Two investigators (JC and YL) independently
extracted data from the eligible papers complying with the
inclusion and exclusion criteria. Disagreements were subsequently
reviewed and resolved through discussion. Studies were included in
the analysis if they met the following inclusion criteria without
time limitation: i) Use of serum, urine or plasma NGAL for
prediction of AKI in patients with suspected sepsis; ii)
stratification of septic patients into an AKI group and a non-AKI
group; iii) definition of sepsis according to the standards of The
American College of Chest Physicians/Society of Critical Care
Medicine (ACCP/SCCM) (10), Society
of Critical Care Medicine/European Society of Intensive Care
Medicine/American College of Chest Physicians/American Thoracic
Society/Surgical Infection Society (SCCM/ESICM/ACCP/ATS/SIS)
(11), or the Survival Sepsis
Campaign 2012 consensus criteria (12); iv) definition of AKI according to
the Risk, Injury, Failure, Loss, End-Stage Kidney Disease (RIFLE)
(13), Acute Kidney Injury Network
(AKIN) (14) or Kidney Disease
Improving Global Outcomes (KDIGO) criteria (15); v) full-text articles written in
English or Chinese; and vi) presence of detailed clinical data that
can be used to calculate sensitivity and specificity, including and
the number of true positive (TP), false positive (FP), true
negative (TN) and false negative (FN) cases.
Exclusion criteria were defined as follows: i)
Studies not including patients with sepsis; ii) studies not
reporting data for the diagnostic accuracy of NGAL; and iii)
studies providing insufficient data regarding the TP, FP, TN and FN
numbers within the original published study. Only original articles
were considered. Other publications, including letters, reviews,
case reports or editorial articles were excluded. The two
investigators reached a consensus on each item through
discussion.
Data extraction and quality
assessment
For each eligible study, the first author's name,
year of publication, admission setting (intensive care unit or
emergency room), country, study design, number of participants and
the reference standards used to define sepsis and AKI were
recorded. Diagnostic accuracy data for serum, urine and plasma
NGAL, the area under the curve (AUC), optimal cut-off values,
sensitivity, specificity and the number of true positive (TP),
false positive (FP), true negative (TN) and false negative (FN)
responses were recorded or calculated. The same two investigators
(JC and YL) also evaluated the quality of the included studies in
the data extraction process. The Quality Assessment for Diagnostic
Accuracy studies-2 (QUADAS-2) tool by RevMan version 5.3 was used
to assess the quality of eligible studies (16). The risk of bias for each item was
graded as ‘low’, ‘unclear’ and ‘high’. Two investigators appraised
the study quality independently and discrepancies were resolved by
discussion. Each study was ranked as having a high, low or unclear
risk of bias according to four different areas: i) Patient
selection; ii) index test; iii) reference standard; and iv) flow of
patients through the study and timing of the index tests and
reference standard (flow and timing).
Statistical analysis
TPs, TNs, FPs and FNs recorded in the included
studies are the primary data used to assess the sensitivity,
specificity, positive likelihood ratio (PLR), negative likelihood
ratio (NLR), diagnostic odds ratios (DOR) and AUC using Stata
(version 15.1). The diagnostic performance of serum, urine and
plasma NGAL was determined by calculating pooled sensitivity,
specificity, PLR, NLR and DOR, with 95% CIs. Likelihood ratios
(positive and negative likelihood ratio) are a ratios of the
probabilities that a test result is correct to the probability that
the test is incorrect [positive likelihood
ratios=sensitivity/(1-specificity); negative likelihood
ratios=specificity/(1-sensitivity)]. The larger the ratio of PLR,
the greater probability of a true positive when the result is
positive. The smaller the ratio of NLR, the greater probability of
a true negative when the result is negative. The DOR [(TP x TN)/(FP
x FN)] was used to reflect the relationship between diagnostic test
and disease. Higher numbers would indicate improved performance in
diagnosing patients with/without sepsis-AKI. Summary receiver
operating characteristic (SROC) curves were generated to estimate
the effect of sensitivity and specificity and were constructed
based on TP and FP rates. TP and FP rates can be calculate through
the following two formulas: TP rates=TP/(TP + FP) x100; FP
rates=FP/(FP + TN) x100. The area under the curve (AUC) of the SROC
was calculated to assess the performance of serum, urine and plasma
NGAL individually.
The heterogeneity between studies was assessed using
the χ2 test and the inconsistency index (I2).
An I2>50% with P<0.05 from the χ2 test
is indicative of significant heterogeneity (17). In this case, a random effect model
was chosen to pool the data of sensitivity, specificity and AUC.
Otherwise, a fixed effect model was used.
The threshold effect is considered as a possible
cause of heterogeneity in diagnostic accuracy analysis (18). Spearman correlation was used to
analyse the logit of sensitivity and the logit of (1-specificity)
and to verify the existence of threshold effect. A strong positive
correlation (correlation >0.6) between sensitivity and
(1-specificity), with P<0.05 was considered to indicate a
statistically significant threshold effect (18).
Sensitivity analyses and subgroup analyses were also
conducted to determine if a certain variance could affect the
heterogeneity and overall diagnostic effect. Sensitivity analysis
was performed by omitting one study at a time to examine stability
of the pooled results. Meta-regression and subgroup analyses were
performed to identify factors that could influence heterogeneity
and the overall diagnostic effect.
Publication bias was analyzed by using the Deeks'
funnel plot and an asymmetry test (19). P<0.05 is considered to indicate
the existence of publication bias.
Statistical analysis was performed using Stata
version 15.1 (StataCorp LP). Quality assessment of the included
studies was conducted using RevMan version 5.3 (The Nordic Cochrane
Centre; The Cochrane Collaboration).
Results
Study evaluation
Overall, 1,383 potential citations were identified
for inclusion into the study through multiple database searches and
cross-checking of reference lists. After removing duplicates, 338
studies were excluded. Of these, 259 articles were included based
on titles and abstracts. A further 217 studies were excluded since
they did not meet the eligibility of the present study and 42
studies remained as potential candidates for our meta-analysis.
After reviewing the full text according to the inclusion and
exclusion criteria, 28 studies were ultimately considered eligible
and used for subsequent analysis (5,13,20-45).
The study selection process is illustrated in Fig. 1.
Study characteristics
The included studies were conducted on different
continents (Europe, Asia, North and South America) over a period
spanning 10 years (2010-2020). Of the 28 studies, 9 described the
diagnostic performance of serum NGAL (5,20,21,24,28,31,34,37,41),
10 of plasma NGAL (13,23,25,27,32,35,38,39,43,44)
and 14 of urine NGAL (22,24,26,29-31,33,34,36,37,40,42,44,45).
Collectively, these studies included a total of 2,561 participants.
Prospective studies took up ~43% of the included studies. The
samples of NGAL were taken in two admission settings (ICU or ER)
and samples from ICU took up 24 studies of the included studies.
The remaining studies were of ER. Detailed information regarding
study design, sample sizes and reference standards from the
included studies are included in Table
I.
 | Table ICharacteristics of included studies
for NGAL to predict sepsis-induced AKI. |
Table I
Characteristics of included studies
for NGAL to predict sepsis-induced AKI.
| First author/s,
year | Country | Design | Setting | AKI definition | Sepsis
definition | Source | Number of patients,
AKI/total number of patients | Sampling time
(h) | NGAL assay
type | (Refs.) |
|---|
| Aydoğdu et
al, 2013 | Turkey | PC | ICU | RIFLE | SCCM, ESICM, ACCP,
ATS | Urine | 63/129 | NR | ELISA | (40) |
| Camou et al,
2013 | France | PC | ICU | RIFLE, AKIN | SCCM, ESICM, ACCP,
ATS, SIS | Plasma | 43/50 | Admission | ELISA | (39) |
| De Geus et
al, 2013 | The
Netherlands | PC | ICU | AKIN | ACCP, SCCM | Plasma | 50/75 | Admission | ELISA | (38) |
| El-Farghail et
al, 2012 | Egypt | NR | NICU | AKIN | NR | Serum | 35/60 | Admission | ELISA | (41) |
| Fan et al,
2014 | China | PC | ICU | RIFLE | SCCM, ESICM, ACCP,
ATS, SIS | Urine | 58/126 | Peak | RIA | (36) |
| Hjortrup et
al, 2015 | Denmark | PC | ICU | KDIGO | ACCP, SCCM | Plasma | 31/124 | Admission | NR | (32) |
| Huang et al,
2016 | China | PC | ICU | KDIGO | NR | Plasma | 30/76 | NR | ELISA | (27) |
| Khawaja et
al, 2019 | Pakistan | NR | ICU | RIFLE | NR | Plasma | 32/46 | 12 | NR | (13) |
| Li and Xu,
2010 | China | PC | ICU | AKIN | ACCP, SCCM | Urine | 17/74 | 24 | ELISA | (45) |
| Liu et al,
2019 | China | NR | ICU | KDIGO | SSC | Serum | 42/89 | Admission | ELISA | (21) |
| Mårtensson et
al, 2010 | Sweden | NR | ICU | RIFLE, AKIN | ACCP, SCCM | Plasma, Urine | 18/45 | 12 | RIA | (44) |
| Md Ralib et
al, 2017 | Malaysia | NR | ICU | NR | ACCP, SCCM | Plasma | 67/129 | 24 | NR | (25) |
| Meng et al,
2015 | China | NR | ICU | AKIN | SSC | Serum, Urine | 34/66 | Peak | ELISA | (31) |
| Nga et al,
2015 | Brazil | PC | ER | AKIN | SSC | Urine | 34/168 | 24 | ELISA | (30) |
| Niu et al,
2015 | China | PC | ER | AKIN | SCCM, ESICM, ACCP,
ATS, SIS | Urine | 26/60 | 12 | ELISA | (29) |
| Patel et al,
2016 | India | PC | NR | RIFLE, AKIN | SSC | Urine | 88/155 | 12 | NR | (26) |
| Rocha et al,
2018 | Brazil | NR | ICU | KDIGO | SSC | Urine | 47/75 | 48 | ELISA | (22) |
| Shang et al,
2017 | China | NR | ICU | RIFLE | NR | Serum, Urine | 35/50 | Admission | ELISA | (24) |
| Shapiro et
al, 2010 | USA | PC | ER | RIFLE | ACCP, SCCM | Plasma | 24/66 | Admission | ELISA | (43) |
| Wang HX et
al, 2014 | China | NR | ICU | KDIGO | ACCP, SCCM | Plasma | 38/90 | 48 | ELISA | (35) |
| Wang and Zhang,
2014 | China | NR | ICU | KDIGO | ACCP, SCCM | Serum, Urine | 28/51 | 48 | ELISA | (34) |
| Wu et al,
2019 | China | NR | ICU | KDIGO | ESICM, SCCM | Serum | 29/60 | Admission | NR | (5) |
| Xing et al,
2013 | China | NR | ICU | AKIN | SCCM, ESICM, ACCP,
ATS, SIS | Serum | 35/73 | NR | ELISA | (37) |
| Yan et al,
2011 | China | PC | ICU | AKIN | ACCP, SCCM | Urine | 27/112 | 2 | ELISA | (42) |
| Yang et al,
2019 | China | NR | ICU | NR | NR | Serum | 71/156 | NR | ELISA | (20) |
| Zhang et al,
2016 | China | NR | ICU | NR | SSC | Serum | 30/58 | NR | ELISA | (28) |
| Zheng et al,
2017 | China | NR | ICU | NR | ACCP, SCCM | Plasma | 52/150 | Admission | ELISA | (23) |
| Zhou et al,
2014 | China | NR | ICU | AKIN | SCCM, ESICM, ACCP,
ATS, SIS | Urine | 46/148 | 8 | ELISA | (33) |
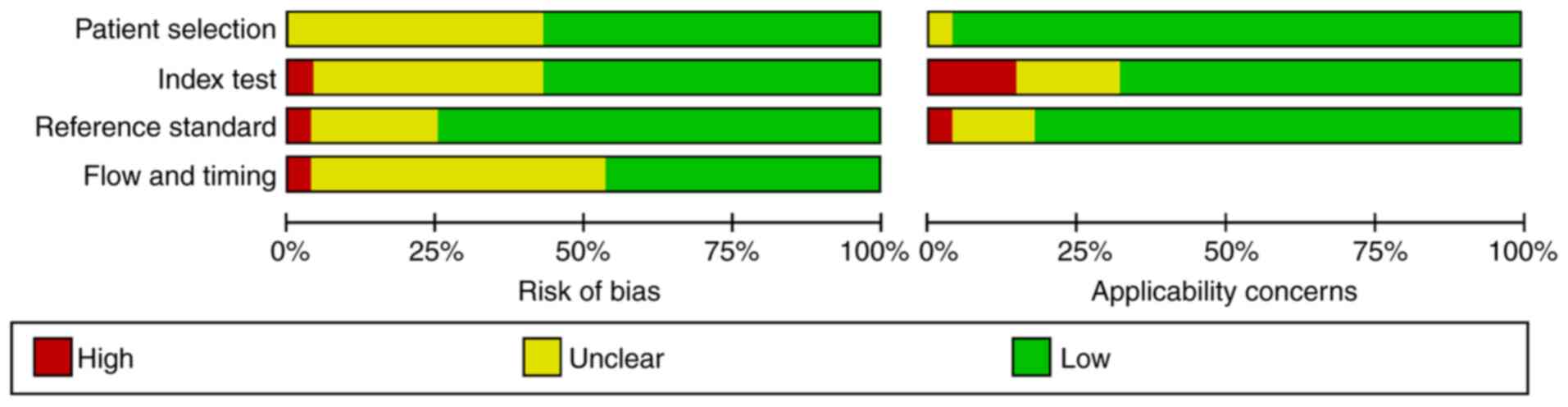
Quality assessment
The quality and potential bias of the studies were
assessed using the QUADAS-2 tool. The ‘risk of bias’ tool evaluates
four items, patient selection, index test, reference standard and
flow and timing. High risk was mostly observed in the ‘index test’
category because many studies did not provide the interpretation
method of the NGAL test results and did not provide a threshold.
Detailed information of the included studies and the results of
distribution are presented in Fig.
2.
Diagnostic accuracy of urine NGAL
The discriminatory accuracy of a diagnostic test is
commonly assessed by measuring how well it correctly identifies
true-positive and true-negative result in terms of sensitivity and
specificity (46). The pooled
sensitivity of the 14 studies that reported the use of urine NGAL
was 0.87 (95% CI, 0.83-0.90) and the pooled specificity was 0.84
(95% CI, 0.79-0.88; Fig. 3A). The
pooled positive likelihood ratio (PLR) was 5.5 (95% CI, 4.0-7.5)
and the pooled negative likelihood ratio (NLR) was 0.16 (95% CI,
0.12-0.20; Table II). Using a
random effect model, the DOR was 35 (95% CI, 21-58). There was no
threshold effect, as indicated by Spearman correlation analysis
(ρ=0.50; P=0.25; data not shown). An SROC analysis was conducted to
evaluate the diagnostic accuracy of urine NGAL (Fig. 4A). An AUC of 0.92 was obtained from
the SROC curve, suggesting that urine NGAL achieved high diagnostic
accuracy in diagnosing sepsis-AKI, due to the observation that AUC
>0.9.
| Table IIDiagnostic value of NGAL to predict
AKI in septic patients. |
Table II
Diagnostic value of NGAL to predict
AKI in septic patients.
| First author/s,
year | Source | AUC | 95% CI | Cut-off value | Sensitivity, | Specificity, | DORb | TP, n | FP, n | FN, n | TN, n | (Refs.) |
|---|
| Aydoğdu et
al, 2013 | Urine | 0.44 | NR | 29.5 ng/ml | 0.88 | 0.73 | 18.33 | 55 | 18 | 8 | 48 | (40) |
| Camou et al,
2013 | Plasma | 0.90 | NR | 150 ng/ml | 0.93 | 0.44 | 10.00 | 40 | 4 | 3 | 3 | (39) |
| De Geus et
al, 2011 | Plasma | 0.80 | 0.69-0.88 | 979 ng/ml | 0.80 | 0.80 | 16.00 | 40 | 5 | 10 | 20 | (50) |
| El-Farghail et
al, 2012 | Serum | 0.95 | NR | 117.5 ng/ml | 0.82 | 0.89 | 8.18 | 29 | 13 | 6 | 22 | (41) |
| Fan et al,
2014 | Urine | 0.86 | 0.81-0.93 | 402 ng/ml | 0.89 | 0.74 | 24.07 | 52 | 18 | 6 | 50 | (36) |
| Hjortrup et
al, 2015 | Plasma | 0.66 | 0.54-0.77 | 558 ng/ml | 0.58 | 0.76 | 4.47 | 18 | 22 | 13 | 71 | (32) |
| Huang et al,
2016 | Plasma | 0.73 | 0.61-0.85 | 150 ng/ml | 0.90 | 0.35 | 4.80 | 27 | 30 | 3 | 16 | (27) |
| Khawaja et
al, 2019 | Plasma | 0.82 | 0.68-0.96 | 150 ng/ml | 0.71 | 0.91 | 33.22 | 23 | 1 | 9 | 13 | (13) |
| Li and Xu,
2010 | Urine | 0.94 | 0.68-0.97 | 50 ng/ml | 0.94 | 0.88 | 114.29 | 16 | 7 | 1 | 50 | (45) |
| Liu et al,
2019 | Serum | 0.78 | 0.76-0.82 | 16.32 ng/ml | 0.75 | 0.79 | 11.84 | 32 | 10 | 10 | 37 | (21) |
| Mårtensson et
al, 2010 | Plasma | 0.85 | 0.39-0.94 | 120 ng/ml | 0.83 | 0.86 | 28.75 | 15 | 4 | 3 | 23 | (44) |
| | Urine | 0.86 | 0.68-1.00 | 68 ng/ml | 0.71 | 1.00 | 135.00 | 13 | 0 | 5 | 27 | |
| Md Ralib et
al, 2017 | Plasma | 0.72 | 0.66-0.83 | 454 ng/ml | 0.72 | 0.74 | 7.26 | 48 | 16 | 19 | 46 | (25) |
| Meng et al,
2015 | Serum | 0.89 | 0.82-0.97 | 93.5 ng/ml | 0.83 | 0.84 | 25.20 | 28 | 5 | 6 | 27 | (31) |
| | Urine | 0.99 | 0.89-1.00 | 117.5 ng/ml | 0.94 | 0.91 | 154.67 | 32 | 3 | 2 | 29 | |
| Nga et al,
2015 | Urine | 0.83 | 0.64-0.81 | 3.36 ng/ml | 0.77 | 0.66 | 6.30 | 26 | 16 | 8 | 31 | (30) |
| Niu et al,
2015 | Urine | 0.91 | NR | NRa | 0.88 | 0.87 | 44.47 | 23 | 5 | 3 | 29 | (29) |
| Patel et
al,2016 | Urine | 0.81 | 0.73-0.89 | 34.32 ng/ml | 0.86 | 0.81 | 26.31 | 76 | 13 | 12 | 54 | (26) |
| Rocha et al,
2018 | Urine | 0.61 | 0.48-0.73 | 13.3 ng/ml | 0.92 | 0.93 | 139.75 | 43 | 2 | 4 | 26 | (22) |
| Shang et al,
2017 | Serum | 0.69 | 0.50-0.88 | 2.37 ng/ml | 0.91 | 0.47 | 9.33 | 32 | 8 | 3 | 7 | (24) |
| | Urine | 0.83 | 0.70-0.97 | 4.85 ng/ml | 0.78 | 0.87 | 21.94 | 27 | 2 | 8 | 13 | |
| Shapiro et
al, 2010 | Plasma | 0.82 | 0.76-0.88 | NR | 0.96 | 0.51 | 23.00 | 23 | 21 | 1 | 21 | (43) |
| Wang HX et
al, 2014 | Plasma | 0.86 | 0.83-0.90 | 119.30 ng/ml | 0.79 | 0.80 | 15.75 | 30 | 10 | 8 | 42 | (35) |
| Wang and Zhang,
2014 | Serum | 0.83 | 0.79-0.87 | 162.2 ng/ml | 0.88 | 0.80 | 30.00 | 25 | 5 | 3 | 18 | (34) |
| | Urine | 0.81 | 0.71-0.91 | 150 ng/ml | 0.79 | 0.90 | 38.50 | 22 | 2 | 6 | 21 | |
| Wu et al,
2019 | Serum | 0.84 | 0.74-0.94 | NR | 0.79 | 0.81 | 15.97 | 23 | 6 | 6 | 25 | (5) |
| Xing et al,
2013 | Serum | 0.86 | 0.77-0.94 | 70 ng/ml | 0.85 | 0.87 | 39.60 | 30 | 5 | 5 | 33 | (37) |
| | Urine | 0.93 | 0.88-0.93 | 101.5 ng/ml | 0.93 | 0.89 | 90.67 | 32 | 4 | 3 | 34 | |
| Zheng et al,
2017 | Plasma | 0.82 | 0.75-0.90 | 171 ng/ml | 0.79 | 0.75 | 11.49 | 41 | 24 | 11 | 74 | (23) |
| Zhou et al,
2014 | Urine | 0.80 | 0.71-0.93 | 85 ng/ml | 0.78 | 0.80 | 14.76 | 36 | 20 | 10 | 82 | (33) |
| Yan et al,
2011 | Urine | 0.93 | 0.88-0.98 | 65 ng/ml | 0.95 | 0.86 | 105.75 | 54 | 8 | 3 | 47 | (42) |
| Yang et al,
2019 | Serum | 0.78 | 0.71-0.86 | 69.7 ng/ml | 0.72 | 0.73 | 6.87 | 51 | 23 | 20 | 62 | (20) |
| Zhang et al,
2015 | Serum | 0.88 | NR | NR | 0.90 | 0.99 | 447.86 | 27 | 0 | 3 | 28 | (28) |
Estimation of the inconsistency index for
sensitivity and specificity (I2=42.06% and 60.16%,
respectively; P=0.07 and 0.01, respectively; Fig. 3A) indicated that there was
heterogeneity in the pooled specificity of urine NGAL between the
included studies. Therefore, a subgroup analysis and
meta-regression were conducted based on the study design
(prospective and non-prospective; Table III). The study design
significantly affected the results of sensitivity and specificity.
Indeed, the use of a prospective design resulted in a significantly
lower sensitivity (P≤0.01) and specificity (P≤0.01), compared with
a non-prospective design.
| Table IIIResult of meta-regression, subgroup
analysis. |
Table III
Result of meta-regression, subgroup
analysis.
| Source | Number of
studies | Sensitivity (95%
CI) | P-value | Specificity (95%
CI) | P-value |
|---|
| Plasma NGAL | | | | | |
|
Prospective | 3 | 0.89
(0.82-0.95) | <0.01 | 0.71
(0.52-0.91) | 0.36 |
|
Non-prospective | 7 | 0.76
(0.70-0.82) | | 0.74
(0.62-0.85) | |
| Urine NGAL | | | | | |
|
Prospective | 7 | 0.86
(0.82-0.90) | <0.01 | 0.74
(0.69-0.78) | <0.01 |
|
Non-prospective | 2 | 0.87
(0.80-0.95) | | 0.82
(0.76-0.89) | |
Diagnosis accuracy of serum NGAL
A total of nine studies reported the use of serum
NGAL. The pooled sensitivity for these studies in the diagnosis of
sepsis-related AKI was 0.83 (95% CI, 0.77-0.87), whereas the pooled
specificity was 0.79 (95% CI, 0.69-0.87; Fig. 3B). The pooled PLR was 4.00 (95% CI,
2.6-6.2), while the pooled NLR was 0.22 (95% CI, 0.16-0.30). The
DOR was 18 (95% CI, 9-36) with higher values indicating better
discriminatory performance. An SROC analysis was carried out to
evaluate the diagnostic accuracy of serum NGAL, demonstrating an
AUC of 0.87 (95% CI, 0.84-0.90; Fig.
4B). There was no notable threshold effect in the nine studies
included in this meta-analysis (ρ=0.34; P=0.12; data not
shown).
An I2 of 32.29% for sensitivity (P=0.17)
and 69.86% for specificity (P<0.001; Fig. 3B) indicated that there was a
significant heterogeneity in the pooled specificity in the included
studies. A sensitivity analysis was conducted to eliminate factors
that influence of heterogeneity. In the interpretation of the
heterogeneity of the diagnostic accuracy of serum NGAL, sensitivity
analysis suggested that the study by Zhang et al (28) had an impact on heterogeneity.
Omitting the study by Zhang et al (28) decreased the I2 both in
sensitivity (from 31.29 to 22.4%; P=0.25) and specificity (from
69.86 to 53.70%; P=0.03; Table
IV). The value of I2 in the pooled specificity
reduced by 16% but the heterogeneity did not disappear.
| Table IVResult of sensitivity analysis. |
Table IV
Result of sensitivity analysis.
| A, Serum NGAL |
|---|
| Included
studies | Sensitivity | I2
(%) | P-value | Specificity | I2
(%) | P-value |
|---|
| All | 0.83
(0.77-0.87) | 32.29 | 0.17 | 0.79
(0.69-0.87) | 69.86 | 0.00 |
| Without Zhang et
al (23) | 0.82
(0.76-0.86) | 22.40 | 0.25 | 0.75
(0.68-0.82) | 53.70 | 0.03 |
| B, Urine NGAL |
| Included
studies | Sensitivity | I2
(%) | P-value | Specificity | I2
(%) | P-value |
| All | 0.87
(0.83-0.90) | 42.06 | 0.05 | 0.84
(0.79-0.80) | 60.16 | 0.00 |
| Without Mårtensson
et al (44) | 0.88
(0.84-0.91) | 38.37 | 0.08 | 0.82
(0.78-0.86) | 52.28 | 0.01 |
| C, Plasma NGAL |
| Included
studies | Sensitivity | I2
(%) | P-value | Specificity | I2
(%) | P-value |
| All | 0.81
(0.73-0.87) | 61.32 | 0.01 | 0.71
(0.59-0.81) | 86.17 | 0.00 |
| Without Hjortrup
et al (32) | 0.83
(0.75-0.88) | 48.24 | 0.05 | 0.71
(0.57-0.82) | 87.21 | 0.00 |
Diagnostic accuracy of plasma
NGAL
In total, 10 studies reported the use of plasma NGAL
for AKI diagnosis. These studies had a pooled sensitivity of 0.81
(95% CI, 0.73-0.87) and a pooled specificity of 0.71 (95% CI,
0.59-0.81; Fig. 3C). The pooled PLR
was 2.8 (95% CI, 2.0-3.9) and the pooled NLR was 0.26 (95% CI,
0.20-0.36). The DOR was 11 (95% CI, 7-16), which was the worst
performer among the three NGALs tested using a random effect model.
In addition, the AUC obtained from SROC analysis was 0.84 (95% CI,
0.80-0.87; Fig. 4C). There was no
notable threshold effect in the meta-analysis (ρ=-0.93; P=0.87;
data not shown). The estimation of sensitivity and specificity
(I2=61.32 and 86.17%, respectively; P=0.01 and
<0.001, respectively; Fig. 3C)
indicated that there was heterogeneity between the studies. Thus, a
subgroup analysis was performed based on study design (prospective
and non-prospective). Meta-regression and subgroup analysis
revealed that study design had a significant effect on the
diagnostic accuracy of plasma NGAL. The use of a prospective design
resulted in a significantly higher sensitivity (P≤0.01) but no
effect on specificity (P=0.36), compared with those from a
non-prospective design (Table
III).
Evaluation of publication bias
Publication bias was analysed using a Deeks' funnel
plot and an asymmetry test. No publication bias was detected among
the studies in the urine (P=0.16), serum (P=0.052) and plasma NGAL
(P=0.16) groups.
Discussion
The morbidity and mortality of patients with sepsis
in intensive care units remain high (2). In addition, AKI is among the most
severe complications of sepsis (4).
NGAL is the most extensively researched biomarker for the diagnosis
of AKI in blood and urine specimens. Zhang et al (6) previously examined the diagnostic
values of plasma and urine NGAL using meta-analysis. However, the
number of studies included in their analysis was limited, and the
reported high diagnostic value for urine NGAL was later questioned
by Törnblom et al (47).
Moreover, in the Zhang et al (6) study, the role of serum NGAL in
diagnosing AKI was not examined. Thus, the optimal source of NGAL
for the diagnosis of sepsis-induced AKI remains unknown.
The aim of the present meta-analysis was to assess
the diagnostic accuracy of serum, plasma and urine NGAL among
patients with suspected sepsis. In the present study, urine NGAL
presented improved performance compared with serum and plasma, with
a relatively high sensitivity, specificity and DOR, as well as the
highest AUC. The present findings further support the notion that
urine NGAL can predict sepsis-related AKI, which is consistent with
the prospective cohort studies carried out by da Rocha et al
and Patel et al (22,26).
Urine NGAL is an independent predictor of AKI, as it is not
affected by the presence of sepsis (48) By contrast, NGAL levels in the
bloodstream of patients with sepsis may increase due to injury to
the kidney, thereby influencing the diagnosis of AKI through plasma
and serum specimens (49).
Additionally, urine testing represents a convenient, fast and
non-invasive collection technique. Thus, the majority of patients
would be eligible for diagnosis of AKI through the urine,
especially paediatric patients. Notably, compared with serum
creatinine as a diagnostic reference, the time to diagnose AKI with
urine NGAL is 2 h shorter (45).
In the present study, serum NGAL also demonstrated a
relatively high AUC. Although only a limited number of studies
included in the present meta-analysis reported the use of serum
NGAL, a recent prospective cohort study has demonstrated that the
combined performance of serum and urine NGAL can increase the early
diagnostic accuracy of sepsis-induced AKI (50). Furthermore, previous studies by Meng
et al and Xing et al (31,37)
demonstrated that the predictive performance of serum and urine
NGAL for sepsis-related AKI increased significantly in combination
compared with that in either alone. Notably, AKI diagnosis through
serum NGAL would be available to patients suffering from oliguria
or other conditions that cause inconvenience for urine
sampling.
The use plasma NGAL for the prediction of AKI in
septic patients remains controversial. There is no consensus on the
predictive ability of plasma NGAL according to previous studies
(40,44). Mårtensson et al (44) reported a poor predictive ability for
plasma NGAL and suggested that NGAL levels in the plasma may be
affected by other non-renal factors such as inflammation. Aydoğdu
et al (40) demonstrated
that concurrent sepsis could increase the levels of plasma NGAL in
the absence of AKI and thus, the diagnostic accuracy of plasma NGAL
may have been corrupted. By contrast, previous studies by Huang
et al and Shapiro et al (27,43)
suggested that plasma NGAL could predict sepsis-related AKI. The
different locations in which these studies were conducted may have
led to the discrepancies in study outcomes, as suggested by Md
Ralib et al (25). In the
present meta-analysis, plasma NGAL was less useful than other NGAL
sources in diagnosing sepsis-related AKI. Indeed, compared with
urine and serum specimens, plasma NGAL presented the poorest
sensitivity, specificity and AUC.
Nevertheless, the present study has certain
limitations that should be taken into consideration when
interpreting its findings. High heterogeneity performed in the
meta-analysis for plasma NGAL was a substantial problem. Although
sensitivity analysis omitted studies that affected heterogeneity,
the results only changed slightly. Subgroup analyses were performed
to identify factors that influenced heterogeneity, yet the causes
of heterogeneity could not be determined. Moreover, as
aforementioned, there is still a controversial in the use of plasma
NGAL. Further prospective studies focusing on plasma NGAL should
also be considered in the future.
In conclusion, the present findings suggested that
urine NGAL was a robust diagnostic biomarker of AKI, with the
highest sensitivity, specificity and AUC. However, each specimen
type had its own advantages and weaknesses. For instance, the use
of serum and plasma NGAL in combination may enhance the strengths
and reduce the deficiencies of each, resulting in a more accurate
diagnosis. Further studies are encouraged to provide more robust
evidence.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HZ analysed the research data and was the major
contributor in the preparation and writing of the manuscript. JC
collected the original data and quality assessment and conducted
the data processing of the meta-analysis. YL collected the original
data and quality assessment. JS is responsible for interpretation
of data for the work, visualization and tables and figures
production. JL made substantial contributions to the conception and
design of the study and drafted the manuscript. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lameire NH, Bagga A, Cruz D, De Maeseneer
J, Endre Z, Kellum JA, Liu KD, Mehta RL, Pannu N, Van Biesen W and
Vanholder R: Acute kidney injury: An increasing global concern.
Lancet. 382:170–179. 2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kellum JA, Wen X, de Caestecker MP and
Hukriede NA: Sepsis-associated acute kidney injury: A problem
deserving of new solutions. Nephron. 143:174–178. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zarbock A, Gomez H and Kellum JA:
Sepsis-induced acute kidney injury revisited: Pathophysiology,
prevention and future therapies. Curr Opin Crit Care. 20:588–595.
2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bellomo R, Kellum JA, Ronco C, Wald R,
Martensson J, Maiden M, Bagshaw SM, Glassford NJ, Lankadeva Y,
Vaara ST and Schneider A: Acute kidney injury in sepsis. Intensive
Care Med. 43:816–828. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
JX W, HS Z and XL C: Clinical significance
of renal biomarkers for early evaluation of acute kidney injury in
sepsis. Chin J Crit Care Intensive Care Med. 5:132–138. 2019.
|
|
6
|
Zhang A, Cai Y, Wang PF, Qu JN, Luo ZC,
Chen XD, Huang B, Liu Y, Huang WQ, Wu J and Yin YH: Diagnosis and
prognosis of neutrophil gelatinase-associated lipocalin for acute
kidney injury with sepsis: A systematic review and meta-analysis.
Crit Care. 20:41. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Mishra J, Ma Q, Prada A, Mitsnefes M,
Zahedi K, Yang J, Barasch J and Devarajan P: Identification of
neutrophil gelatinase-associated lipocalin as a novel early urinary
biomarker for ischemic renal injury. J Am Soc Nephrol.
14:2534–2543. 2003.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Chakraborty S, Kaur S, Guha S and Batra
SK: The multifaceted roles of neutrophil gelatinase associated
lipocalin (NGAL) in inflammation and cancer. Biochim Biophys Acta.
1826:129–169. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Haase M, Bellomo R, Devarajan P,
Schlattmann P and Haase-Fielitz A: NGAL Meta-analysis Investigator
Group. Accuracy of neutrophil gelatinase-associated lipocalin
(NGAL) in diagnosis and prognosis in acute kidney injury: A
systematic review and meta-analysis. Am J Kidney Dis. 54:1012–1024.
2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bone RC, Balk RA, Cerra FB, Dellinger RP,
Fein AM, Knaus WA, Schein RM and Sibbald WJ: Definitions for sepsis
and organ failure and guidelines for the use of innovative
therapies in sepsis. The ACCP/SCCM consensus conference committee.
American college of chest physicians/society of critical care
medicine. Chest. 101:1644–1655. 1992.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Levy MM, Fink MP, Marshall JC, Abraham E,
Angus D, Cook D, Cohen J, Opal SM, Vincent JL and Ramsay G:
SCCM/ESICM/ACCP/ATS/SIS. 2001 SCCM/ESICM/ACCP/ATS/SIS international
sepsis definitions conference. Crit Care Med. 31:1250–1256.
2003.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Dellinger RP, Levy MM, Rhodes A, Annane D,
Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke
R, et al: Surviving sepsis campaign: International guidelines for
management of severe sepsis and septic shock, 2012. Intensive Care
Med. 39:165–228. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Khawaja S, Jafri L, Siddiqui I, Hashmi M
and Ghani F: The utility of neutrophil gelatinase-associated
Lipocalin (NGAL) as a marker of acute kidney injury (AKI) in
critically ill patients. Biomark Res. 7(4)2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Mehta RL, Kellum JA, Shah SV, Molitoris
BA, Ronco C, Warnock DG and Levin A: Acute Kidney Injury Network.
Acute kidney injury network: Report of an initiative to improve
outcomes in acute kidney injury. Crit Care. 11(R31)2007.PubMed/NCBI View
Article : Google Scholar
|
|
15
|
Kellum JA and Lameire N: KDIGO AKI
Guideline Work Group. Diagnosis, evaluation, and management of
acute kidney injury: A KDIGO summary (Part 1). Crit Care.
17(204)2013.PubMed/NCBI View
Article : Google Scholar
|
|
16
|
Whiting PF, Rutjes AW, Westwood ME,
Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA and Bossuyt
PM: QUADAS-2 Group. QUADAS-2: A revised tool for the quality
assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Higgins JP and Green S (eds): Cochrane
Handbook for Systematic Reviews of Interventions. Version 5.0.1,
2009.
|
|
18
|
Arends LR, Hamza TH, van Houwelingen JC,
Heijenbrok-Kal MH, Hunink MG and Stijnen T: Bivariate random
effects meta-analysis of ROC curves. Med Decis Making. 28:621–638.
2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sterne JA, Sutton AJ, Ioannidis JP, Terrin
N, Jones DR, Lau J, Carpenter J, Rücker G, Harbord RM, Schmid CH,
et al: Recommendations for examining and interpreting funnel plot
asymmetry in meta-analyses of randomised controlled trials. BMJ.
343(d4002)2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Yang YB, Li YH, Chen XQ, Lv LH and Mei WL:
Diagnostic value of serum NGAL and CysC levels in sepsis patients
with acute kidney injury. Zhejiang Med J. 41:1025–1029. 2019.
|
|
21
|
RQ L, ZY M, HG C and ZC L: Diagnostic
efficacy of serum NGAL, KIM-1 and Cys-C for acute kidney injury in
sepsis patients. China Med Herald. 16:128–131. 2019.
|
|
22
|
da Rocha EP, Yokota LG, Sampaio BM,
Cardoso Eid KZ, Dias DB, de Freitas FM, Balbi AL and Ponce D:
Urinary neutrophil gelatinase-associated lipocalin is excellent
predictor of acute kidney injury in septic elderly patients. Aging
Dis. 9:182–191. 2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Zheng J, He HL and Zhang GY: Neutrophil
gelatinase-associated lipocalin as diagnosis biomarker for acute
renal injury in pediatric patients with sepsis in intensive care
unit. J Third Mil Med Univ. 39:196–200. 2017.
|
|
24
|
Shang Y, Li J, Zhang J, Wang W, Qiao Y and
Ren X: Predictive performance of neutrophil gelatinase-associated
lipocalin (NGAL) in acute kidney injury in septic patients. Chin J
Emerg Med. 26:538–543. 2017.
|
|
25
|
Md Ralib A, Mat Nor MB and Pickering JW:
Plasma neutrophil gelatinase-associated lipocalin diagnosed acute
kidney injury in patients with systemic inflammatory disease and
sepsis. Nephrology (Carlton). 22:412–419. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Patel ML, Sachan R, Shyam R, Kumar S,
Kamal R and Misra A: Diagnostic accuracy of urinary neutrophil
gelatinase-associated lipocalin in patients with septic acute
kidney injury. Int J Nephrol Renovasc Dis. 9:161–169.
2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Huang CY, Shih CC, Chung K, Kao KC and Wu
HP: Predictive value of plasma neutrophil gelatinase-associated
lipocalin for acute renal failure in patients with severe sepsis. J
Chin Med Assoc. 79:428–434. 2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhang JG, Zhang DH, Zhu HP and Liu S: The
clinical value of NGAL in the early diagnosis of sepsis-induced
kidney injury. China Pract Med. 10:46–47. 2015.
|
|
29
|
Niu KY, Yang F, Yang XY, Ye J and Cheng
JJ: Diagnostic value of urinary liver-type fatty acid binding
proteins and urinary neutrophil gelatinase-associated lipocalin in
severe sepsis patients with acute kidney injury. Clin Focus.
5:536–539. 2015.
|
|
30
|
Nga HS, Medeiros P, Menezes P, Bridi R,
Balbi A and Ponce D: Sepsis and AKI in clinical emergency room
patients: The role of urinary NGAL. Biomed Res Int.
2015(413751)2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Meng DL, Xing HB, Mao RS, et al:
Predictive value of neutrophil gelatinase-associated lipocalin for
acute kidney injury patients with sepsis. Zhongguo Jijiu Yixue.
224–229. 2015.
|
|
32
|
Hjortrup PB, Haase N, Treschow F, Moller
MH and Perner A: Predictive value of NGAL for use of renal
replacement therapy in patients with severe sepsis. Acta
Anaesthesiol Scand. 59:25–34. 2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Zhou HQ, Chen MQ, Zhang HD and Wang X:
sTREM-1 and NGAL levels for the early diagnosis of sepsis
complicated by acute kidney injury. J Clin Exp Med. 21:1773–1775.
2014.
|
|
34
|
Wang XH and Zhang T: The value of NGAL in
early diagnosis of acute kidney injury in children with sepsis.
Pract Prev Med. 21:745–747. 2014.
|
|
35
|
Wang HX, Mu HB, Zheng RQ, Lin H, Yu JQ and
Wu XY: Early diagnosis of neutrophil gelatinase-associated
apolipoprotein in patients with acute kidney injury in sepsis.
Shiyong Linchuang Yiyao Zazhi. 18:183–184. 2014.
|
|
36
|
Fan H, Zhao Y, Zhu JH and Song FC: Urine
neutrophil gelatinase-associated lipocalin in septic patients with
and without acute kidney injury. Ren Fail. 36:1399–1403.
2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Xing HB, Lv T, Sheng PP, Chen JD, Mao RS
and Li D: The diagnostic value of new biomarkers in sepsis patients
with acute kidney injury. Zhongguo Jijiu Yixue. 33:507–510.
2013.
|
|
38
|
de Geus HR, Betjes MG, Schaick RV and
Groeneveld JA: Plasma NGAL similarly predicts acute kidney injury
in sepsis and nonsepsis. Biomark Med. 7:415–421. 2013.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Camou F, Oger S, Paroissin C, Guilhon E,
Guisset O, Mourissoux G, Pouyes H, Lalanne T and Gabinski C: Plasma
neutrophil gelatinase-associated lipocalin (NGAL) predicts acute
kidney injury in septic shock at ICU admission. Ann Fr Anesth
Reanim. 32:157–164. 2013.PubMed/NCBI View Article : Google Scholar : (In French).
|
|
40
|
Aydoğdu M, Gürsel G, Sancak B, Yeni S,
Sarı G, Taşyürek S, Türk M, Yüksel S, Senes M and Ozis TN: The use
of plasma and urine neutrophil gelatinase associated lipocalin
(NGAL) and Cystatin C in early diagnosis of septic acute kidney
injury in critically ill patients. Dis Markers. 34:237–246.
2013.PubMed/NCBI View Article : Google Scholar
|
|
41
|
El-Farghali OG, El-Raggal NM, Mahmoud NH
and Zaina GA: Serum neutrophil gelatinase-associated lipocalin as a
predictor of acute kidney injury in critically-ill neonates. Pak J
Biol Sci. 15:231–237. 2012.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Yan J, Xu HY, Zang D, Liang FM and Yang T:
Significance of early diagnosis of urinary neutrophil
gelatinase-associated lipocalin and urinary interleukin-18 in
patients with sepsis complicated with acute kidney injury. Suzhou
Univ J Med Sci. 31:785–788. 2011.
|
|
43
|
Shapiro NI, Trzeciak S, Hollander JE,
Birkhahn R, Otero R, Osborn TM, Moretti E, Nguyen HB, Gunnerson K,
Milzman D, et al: The diagnostic accuracy of plasma neutrophil
gelatinase-associated lipocalin in the prediction of acute kidney
injury in emergency department patients with suspected sepsis. Ann
Emerg Med. 56:52–59.e1. 2010.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Mårtensson J, Bell M, Oldner A, Xu S,
Venge P and Martling CR: Neutrophil gelatinase-associated lipocalin
in adult septic patients with and without acute kidney injury.
Intensive Care Med. 36:1333–1340. 2010.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Li PZ and Xu WX: Prediction of acute
kidney injury complicated by sepsis with neutronphil
gelatinase-associated lipocalin as an early marker. Chin J Lab Med.
33:492–496. 2010.
|
|
46
|
Shapiro DE: The interpretation of
diagnostic tests. Stat Methods Med Res. 8:113–134. 1999.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Törnblom S, Nisulal S, Petäjä L, Vaara ST,
Haapio M, Pesonen E and Pettilä V: FINNAKI study group. Urine NGAL
as a biomarker for septic AKI: A critical appraisal of clinical
utility-data from the observational FINNAKI study. Ann Intensive
Care. 10(51)2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Seliger SL, Davis C and Stehman-Breen C:
Gender and the progression of renal disease. Curr Opin Nephrol
Hypertens. 10:219–225. 2001.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Mori K, Lee HT, Rapoport D, Drexler IR,
Foster K, Yang J, Schmidt-Ott KM, Chen X, Li JY, Weiss S, Mishra J,
et al: Endocytic delivery of lipocalin-siderophore-iron complex
rescues the kidney from ischemia-reperfusion injury. J Clin Invest.
115:610–621. 2005.PubMed/NCBI View Article : Google Scholar
|
|
50
|
de Geus HR, Woo JG, Wang Y, Devarajan P,
Betjes MG, le Noble JL and Bakker J: Urinary neutrophil
gelatinase-associated lipocalin measured on admission to the
intensive care unit accurately discriminates between sustained and
transient acute kidney injury in adult critically ill patients.
Nephron Extra. 1:9–23. 2011.PubMed/NCBI View Article : Google Scholar
|