Introduction
Neovascular glaucoma (NVG) is one of the most
refractory forms of glaucoma, caused by various ocular and
occasionally systemic conditions that produce retinal ischemia. NVG
often appears as an end-stage disease, resulting in blindness,
continuous pain, and eventually loss of the eye. In this stage, the
objective of the treatment is to lower the intraocular pressure
(IOP) to relieve the pain and preserve the globe (1). Numerous treatments have been attempted
for lowering IOP in NVG, but no consensus exists regarding the most
effective and safest procedure (2).
Trabeculectomy with antimetabolites, aqueous shunt implantation,
and cyclodestructive procedures are the main methods used to treat
high IOP in NVG. For many years, a variety of methods resulting in
cyclodestruction have been used to reduce the aqueous formation
and, subsequently, the IOP. Non-penetrating and penetrating
cyclodiathermy were introduced in the 1930s, cyclocryotherapy in
the 1950s, and later high-intensity focused ultrasound, but all of
these have been abandoned due to the high risk of devastating
complications (3,4). Cyclophotocoagulation is a form of
cycloablation that focuses high-intensity laser energy at the level
of ciliary epithelium, where it is absorbed by melanin and
transformed into heat with a coagulative effect, resulting in the
reduction of aqueous production and, consequently, in lowering of
the IOP (5). Although numerous
types of lasers have been used, diode lasers are currently
considered to be the most appropriate. The diode laser emits a beam
with a wavelength of 800-850 nm, which is best absorbed by the
melanin in the pigmentary epithelium, with less energy affecting
the sclera. The energy delivery periods are quite long, 2-3 sec,
and therefore, high energy is transferred to the ciliary stroma,
with coagulative effects. Traditionally, transscleral
cyclophotocoagulation (TSCPC) delivers laser energy in a continuous
manner. Continuous wave transscleral cyclophotocoagulation
(CW-TSCPC) is effective in lowering IOP, but has a risk of
important complications such as a decrease in visual acuity (VA),
hypotony, chronic uveitis, and phthisis bulbi (6-8).
These complications are likely the result of damage to the
surrounding tissues due to the spread of the thermal energy
(6). Another technique, micropulse
transscleral cyclophotocoagulation (MP-TSCPC), involves using a
novel probe that delivers a series of short pulses of laser energy
(‘on’) separated by rest periods (‘off’). During the ‘on’ period
the thermal energy acts on ciliary body epithelium, while during
‘off’ periods the adjacent structures are allowed to dissipate the
heat, protecting them from the thermal effect. Therefore MP-TSCPC
reduces the damage of the surrounding tissues and lowers the
incidence of complications while preserving the IOP lowering
activity (6,9,10-12).
The primary aim of the study was to compare the performance of
MP-TSCPC vs. CW-TSCPC over 12 months post-intervention. The
secondary aim of the study was to demonstrate the safety and
efficacy of MP-TSCPC over 12 months post-intervention.
Materials and methods
Study design
A retrospective cohort study was performed including
all patients with NVG that were treated with TSCPC between January
2017 and September 2019 at the Department of Ophthalmology of ‘Dr.
Carol Davila’ Central Military Emergency University Hospital
(Bucharest, Romania). While the study was not randomized, the
treatment modality (MP vs. CW) was not based on medical
considerations related to the case. All patients followed a fixed
postoperative visit schedule: day 1, day 7, months 1, 3, 6, 12, and
15. The primary time-point was 12 months post-intervention. The
study was approved (approval no. 445/03.03.2021) by the
Institutional Review Board of the hospital and followed the
principles of the Declaration of Helsinki (2013).
Data of patients
Data were collected at baseline, before the TSCPC
intervention on demographics of patients (age and sex), diagnosis
including etiology of NVG, IOP, the number of glaucoma medications,
including oral acetazolamide, best-corrected visual acuity (BCVA),
anterior segment evaluation, and type of TSCPC used, MP or CW. A
total of 51 eyes from 51 patients were treated, 27 with MP-TSCPC
and 24 with CW-TSCPC. However, 5 were later excluded due to
inadequate length of follow-up, and thus a remainder of 24 eyes for
MP-TSCPC and 22 eyes for CW-TSCPC were included. The age was
comparable between groups (P=0.45), with means of 55.6 years
(range, 44-79) for MP-TSCPC and 58.1 years (range, 32-87) for
CW-TSCPC. There were no differences between groups with regard to
sex (for example, males, 54.2 and 59.1% in the MP-TSCPC and the
CW-TSCPC groups, respectively; P=0.97), as demonstrated in Table I. At each follow-up visit, IOP, VA,
antiglaucoma medications, complications, and the need for
retreatment were recorded. IOP was assessed by Goldmann applanation
tonometry, or by I-care rebound tonometry when Goldmann applanation
tonometry was not accurate or possible. BCVA was at an extremely
low level, counting fingers (CF) or less. After the treatment, VA
was divided into three groups, namely improved, unchanged, and
worsened, compared with the baseline VA. A change in VA was defined
as improved if it changed from light perception (LP) to perception
of hand movements (HM) or improved, or from HM to CF, unchanged if
it remained the same or worsened, when there was a decline in VA,
either from CF to HM or LP or from HM to LP.
 | Table IPatient characteristics at
baseline. |
Table I
Patient characteristics at
baseline.
| Characteristics | Micropulse
transscleral cyclophotocoagulation | Continuous
wave-transscleral cyclophotocoagulation | P-value |
|---|
| Age (years) | 55.6 (range,
44-79) | 58.1 (range,
32-87) | 0.30 |
| Sex | | | 0.74 |
|
Male | 13 (54.2%) | 13 (59.1%) | |
|
Female | 11 (45.8%) | 9 (40.9%) | |
| Etiology of
neovascular glaucoma | | | |
|
Retinal vein
occlusion | 8 (33.3%) | 8 (36.3%) | 0.83 |
|
Diabetic
retinopathy | 9 (37.5%) | 7 (31.8%) | 0.69 |
|
Chronic
uveitis | 2 (8.3%) | 1 (4.5%) | 1.0 |
|
Chronic
retinal detachment | 2 (8.3%) | 4 (18.9%) | 0.41 |
|
Retinal
artery occlusion | 0 | 1 (4.5%) | 0.49 |
|
Radiotherapy
induced | 1 (4.2%) | 0 | 1.0 |
|
Carotid
artery occlusive disease | 2 (8.3%) | 1 (4.5%) | 1.0 |
| Previous
surgery | | | |
|
Trabeculectomy | 10 | 11 | 0.57 |
|
Iridectomy/iridotomy | 3 | 2 | 1.0 |
|
Posterior
vitrectomy | 10 | 8 | 0.71 |
|
Cataract
surgery | 5 | 3 | 0.70 |
|
Ahmed valve
implantation | 1 | 1 | 1.0 |
|
Penetrating
keratoplasty | 0 | 1 | 0.49 |
|
Anti-VEGF
injection | 1.33 (range,
0-5) | 0.95 (range,
0-5) | 0.54 |
|
No previous
surgery | 8 | 7 | 0.91 |
Treatment
All procedures were performed in the operating room,
under regional anesthesia; specifically, retrobulbar block with a
mixture of 3 ml of lidocaine 4% and 1 ml of bupivacaine 1%.
Transillumination was used when the position of the ciliary body
was in doubt (high myopes, multiple surgeries on the anterior
pole). Methylcellulose was used as a coupling agent, to facilitate
the movement of the probe tip and to increase the laser power
transmission.
MP-TSCPC was performed with an MP P3 handpiece with
the Iridex Cyclo G6 (IRIDEX Laser System). The power was set at
2000 mW and a duty cycle of 31.35% (micropulse ‘on’ for 0.5 msec
and ‘off’ for 1.1 msec). The probe was applied using firm, moderate
pressure in a continuous, sweeping motion over the superior and
inferior quadrants, 90 sec for each hemiglobe. The 3 and 9 o'clock
meridians, areas of scleral thinning, filtering blebs, and glaucoma
drainage devices were avoided.
CW-TSCPC was performed with the G probe of Iridex
Cyclo G6 (IRIDEX Laser System). A total of 75% of the eye
circumference was treated. This usually required 6-7 applications
in each quadrant, for a total of 20-21 shots. The initial power was
1,250 mW and the duration was 4 sec. The power of the laser was
reduced by 200 mW if more than two ‘pops’ from disruption of the
ciliary processes were heard.
Postoperatively dexamethasone 0.1% every 6 h and
cyclopentolate 1% twice daily were indicated. Patients continued
their antiglaucoma therapy after the procedure. Therapy was later
adjusted with the oral acetazolamide according to the IOP values
recorded during the follow-up visits.
Follow-up
Patients were examined the following day, at one
week, at 1, 3, 6, 9, 12, and 15 months. A minimum of 12 months of
follow-up was required for study inclusion.
Outcome measures
The primary outcome measure was a successful
reduction of IOP: A ‘favorable outcome’ at any time-point was
defined as postprocedural IOP ≤21 mm Hg or IOP reduction from
baseline of ≥30%, with or without additional antiglaucoma
medications. Hypotony was defined as an IOP of <5 mm Hg and was
considered a failure of the treatment.
Secondary outcome measures included the change in
BCVA, the number of antiglaucoma medications, the necessity of oral
acetazolamide, the complications, and the need for retreatment.
Statistical analysis
Baseline characteristics were summarized (number and
proportions for categorical variables; mean and standard deviation
for continuous variables), and compared between the two groups
using Pearson's Chi-square test for categorical variables, and the
Wilcoxon rank-sum test for continuous variables.
For the first study aim, the comparison of CW-TSCPC
and MP-TSCPC procedures, the primary endpoint was the success of
the intervention at 12 months. This was compared between the two
arms using Pearson's Chi-squared test, and a 95% confidence
interval (CI95) of the difference in proportions of
favorable outcomes between arms was reported. The proportion of
favorable outcomes over time was compared between arms using
longitudinal logistic regression using generalized estimating
equations (GEE), which accounts for the correlation of outcomes
within individuals. Moreover, the proportion of times with a
favorable outcome over time between arms was compared using a
one-degree of freedom Wald test within the GEE logistic regression
model.
The secondary outcome was IOP, which was compared
longitudinally between groups using a longitudinal general linear
model (LGLM), including time treated as a factor, treatment, and
their interaction. The model allows within-patient correlation and
time-varying variance. The selection of best correlation structure
(unstructured, constant, exponential and autoregressive of order
1), and time-constant vs. time-varying variance was made based on
the Akaike information criterion. The comparison of the two
treatment arms at month 12 used the Wald test of the LGLM. The
overall comparison of IOP trajectories over time between the two
arms used the Wald test for the interaction in the LGLM.
The important adverse events were considered
worsening of VA, hypotony, and phthisis bulbi. The total of these
three events was computed for each patient, and the rate of these
events was compared between groups using a Poisson model, with a
check for overdispersion (none was detected). Prevalence of
individual important adverse events was compared between arms using
Fisher's exact test.
All analyses were conducted using the R statistical
language and the ‘nlme’ package version 3.1-148 was used. P<0.05
was considered to indicate a statistically significant
difference.
Results
Demographic and clinical
characteristics
A total of 24 eyes from 24 patients with NVG treated
using MP-TSCPC and 22 eyes from 22 patients with NVG treated using
CW-TSCPC, were analyzed. The underlying causes of retinal ischemia
are presented in Table I. Most eyes
in both groups had undergone multiple surgeries. Only 8 eyes in the
MP-TSCPC group and 7 eyes in the CW-TSCPC group had no previous
surgery (P=0.91). The surgery types are listed in Table I.
Follow-up
The mean follow-up period was 15.5±2.1 months
(range, 12-19) for the MP-TSCPC group; all the eyes reached 12
months and 19 eyes had 15 months of follow-up. For CW-TSCPC, the
mean follow-up period was 15.9±2.3 months (range, 12-21) with all
the eyes reaching 12 months and 19 eyes reaching 15 months of
follow-up.
Primary outcome
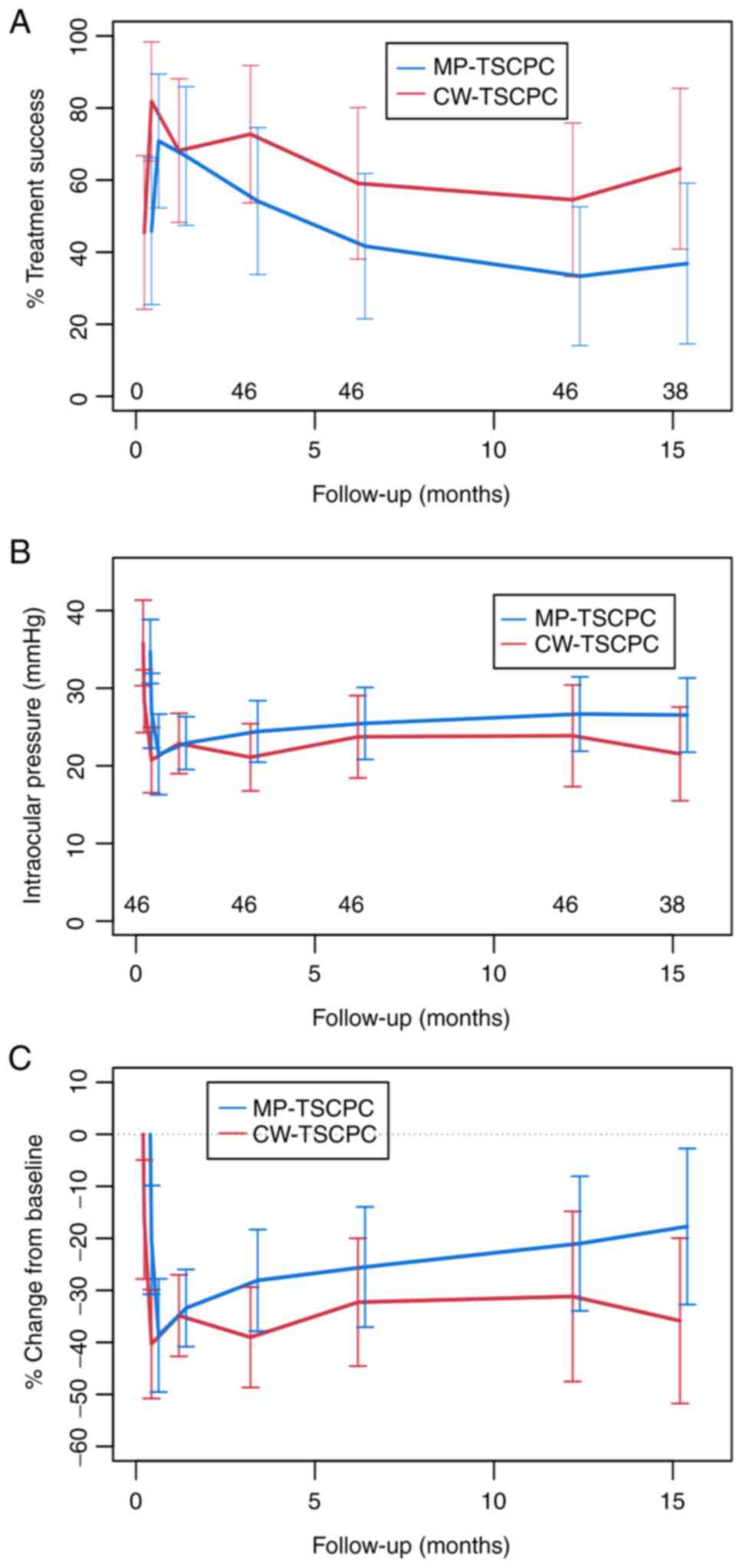
The percentage of favorable outcome (or successes)
at month 12 was 54.5% in the CW-TSCPC group, (95% CI, 34.1 to
73.5%), and 33.3% in the MP-TSCPC group (95% CI, 17.6 to 53.9%).
The odds ratio (OR) of favorable outcome, CW-TSCPC vs. MP-TSCPC was
2.40 [95% CI (0.73, 7.92), P=0.15]. Averaged over the 12 months of
follow-up, the percentage of favorable outcomes in the two arms was
64.6% [95% CI (46.9, 79.1%] for the CW-TSCPC group, and 52.3% [95%
CI (35.4, 68.7%) for the MP-TSCPC group, with an OR of 1.67 [95% CI
(0.69, 4.04); P=0.25]. Results are presented in Fig. 1 and Table II.
| Table IIClinical and adverse events outcomes
in the MP-TSCPC (MP) and CW-TSCPC (CW) groups. |
Table II
Clinical and adverse events outcomes
in the MP-TSCPC (MP) and CW-TSCPC (CW) groups.
| Events | CW | MP | CW vs. MP | P-value |
|---|
| A, Favorable
outcome, proportion | % (95% CI) | % (95% CI) | OR (95% CI) | |
|
Month
12 | 54.5 (34.1,
73.5) | 33.3 (17.6,
53.9) | 2.40 (0.73,
7.92) | 0.15 |
|
Average over
day 1 to month 12 | 64.6 (46.9,
79.1) | 52.3 (35.4,
68.7) | 1.67 (0.69,
4.04) | 0.25 |
| B, IOP change from
baseline | Mean (95% CI), mm
Hg | Mean (95% CI), mm
Hg | Difference (95%
CI) | P-value |
|
Month
12 | -11.95 (-17.77,
-6.14) | -8.04 (-13.61,
-2.48) | -3.91 (-11.96,
3.91) | 0.34 |
|
Average over
day 1 to month 12 | -12.39 (-16.22,
-8.55) | -10.04 (-13.71,
-6.37) | -2.34 (-7.65,
2.96) | 0.39 |
| C, IOP (mmHg) | Mean (95% CI) | Mean (95% CI) | Difference (95%
CI) | P-value |
|
Baseline | 35.82 (30.90,
40.74) | 34.71 (30.00,
39.42) | 1.11 (-5.70,
7.92) | 0.75 |
|
Month
12 | 23.86 (18.07,
29.66) | 26.67 (21.12,
32.21) | 2.80 (-5.22,
10.82) | 0.49 |
| D, Important
adverse events | Rate (95% CI) | Rate (95% CI) | Rate ratio, (95%
CI) | P-value |
|
Day 0 to
month 12 | 0.636 (0.358,
1.030) | 0.250 (0.099,
0.507) | 2.55 (1.02,
7.19)a | 0.045 |
IOP
The change in IOP from baseline to 12 months was
-11.95 mm Hg [95% CI (-17.77, -6.14) mm Hg] in the CW-TSCPC group,
and -8.04 mm Hg [95% CI (-13.61, -2.48) mm Hg] in the MP-TSCPC
group, for a difference of -3.91 mm Hg [95% CI (-11.96, 3.91) mm
Hg; P=0.34]. Averaged over the 12-month follow-up, the mean change
in IOP from baseline was -12.39 mm Hg [95% CI (-16.22, -8.55) mm
Hg] for the CW-TSCPC group, and -10.04 mm Hg [95% CI (-13.71,
-6.37) mm Hg] for the MP-TSCPC group, for a difference of -2.34 mm
Hg [95% CI (-7.65, 2.96) mm Hg; P=0.39]. The mean IOP at month 12
in the two groups was 23.86 mm Hg [95% CI (18.07, 29.66) mm Hg] for
the CW-TSCPC group, and 26.67 mm Hg, [95% CI (21.12, 32.21) mm Hg]
for the MP-TSCPC group. Results are presented in Fig. 1 and Table II. The evolution of the IOP and of
the success rate at follow-up for both MP-TSCPC and CW-TSCPC are
revealed in Table III.
| Table IIIEvolution of the IOP and of the
success rate after MP-TSCPC and CW-TSCPC at different
time-points. |
Table III
Evolution of the IOP and of the
success rate after MP-TSCPC and CW-TSCPC at different
time-points.
| Procedure | Outcome | Baseline | 1 week | 1 month | 3 months | 6 months | 12 months |
|---|
| MP-TSCPC | Mean IOP (mm
Hg) | 34.7±10.3 | 21.4±12.9 | 23.1±8.5 | 24.3±9.9 | 25.4±1.6 | 26.7±12 |
| | IOP reduction (from
baseline) | | 38.3% | 32.6% | 29.9% | 26.8% | 23.0% |
| | Success rate | | 70.8% | 66.6% | 58.3% | 41.6% | 29.1% |
| CW-TSCPC | Mean IOP (mm
Hg) | 36.0±13.2 | 20.7±10 | 22.8±9.3 | 21.6±10.3 | 23.7±12.7 | 23.9±15.6 |
| | IOP reduction (from
baseline) | | 42.5% | 36.7% | 40% | 34.1% | 33.6% |
| | Success rate | | 77.2% | 68.1% | 72.2% | 59.1% | 54.5% |
Important adverse events
The mean number of important adverse events over the
primary 12-month follow-up was 0.636 [95% CI (0.358, 1.030) for CW,
and 0.250 [95% CI (0.099, 0.507) for the MP arm. The rate ratio was
2.55 [95% CI (1.02, 7.19)] for CW-TSCPC vs. MP-TSCPC; P=0.045.
Results are presented in Table
II.
Effects on antiglaucoma
medication
For MP-TSCPC, the mean number of topical
antiglaucoma medications at baseline was 2.6±1; oral acetazolamide
was initially used by 14 patients (58.3%). The number of topical
medications decreased during the first 3 months after treatment to
1.7±1.3 and then started to increase, reaching 2.1±1.3 at 12
months. The number of patients requiring oral acetazolamide
exhibited a more pronounced decrease to only 25% at the end of the
first month, 16.7% at the end of the 3rd and 6th months, and 20.8%
at one year. The evolution of the antiglaucoma medication after
MP-TSCPC is presented in Table IV
and Fig. 2.
| Table IVVariation in the number of topical
antiglaucoma medications and in oral acetazolamide use at different
time-points after MP-TSCPC and CW-TSCPC. |
Table IV
Variation in the number of topical
antiglaucoma medications and in oral acetazolamide use at different
time-points after MP-TSCPC and CW-TSCPC.
| Procedure | Medication | Baseline | 1 month | 3 months | 6 months | 12 months |
|---|
| MP-TSCPC | Mean number of
topical antiglaucoma medications | 2.6±1 | 2.3±1.2 | 1.7±1.3 | 1.9±1.3 | 2.1±1.3 |
| | Oral acetazolamide
users (%) | 58.3% | 25% | 16.7% | 16.7% | 20.8% |
| CW-TSCPC | Mean number of
topical antiglaucoma medications | 2.8±0.8 | 1.7±1.3 | 1.4±1.4 | 1.7±0.9 | 1.9±1.1 |
| | Oral acetazolamide
users (%) | 63.6% | 38% | 27.2% | 13.6% | 27.2% |
For CW-TSCPC, the mean number of topical
antiglaucoma drugs used at baseline was 2.8±0.8 and 14 patients
(63.6%) used oral acetazolamide. The number of antiglaucoma drops
was significantly reduced after the procedure, reaching the lowest
level after 3 months (1.4±1.4) and remained quite stable during the
follow-up period. The same effect, but more pronounced, was
achieved in the case of oral acetazolamide users. The number of
patients using oral acetazolamide was the lowest at 6 months
(13.6%), with a subsequent increase at 12 months (27.2%). The
results are revealed in Table IV
and Fig. 2.
Complications
All complications encountered during our study are
comparatively listed for both groups in Table V. Complications were more frequent
in the CW-TSCPC group. Moreover, the incidence of important adverse
events (worsening of the VA, hypotony, and phthisis bulbi) was, as
already stated, significantly greater in the CW-TSCPC group than in
the MP-TSCPC group (P=0.045). VA was at an extremely low level in
our cohort at baseline. VA worsened in 8 (36.4) cases in the
CW-TSCPC, vs. 4 (16.6%) in the MP-TSCPC group. Only the VA of 1
patient improved and that occurred in the MP-TSCPC group. The more
frequent worsening of VA in the CW-TSCPC group was not
statistically significant, but it reached a trend level (P=0.1), as
demonstrated in Table VI. Hypotony
was present in 4 cases (18.2%) in the CW-TSCPC group and in 2 cases
(8.3%) in the MP-TSCPC group (P=0.41). The devastating complication
of phthisis bulbi appeared in 2 cases (9.1%), both in the CW-TSCPC
group. Retreatment was necessary in 6 cases in the MP-TSCPC group;
4 cases underwent retreatment 3 months after the first procedure,
one case after 4 months, and one case after 6 months. In the
CW-TSCPC group, 7 cases were retreated, most of them after 3 months
(5 cases), one case after 6 months, and one case after 10
months.
| Table VComplications encountered after
TSCPC. |
Table V
Complications encountered after
TSCPC.
| Complications | Micropulse
TSCPC | Continuous wave
TSCPC | P-value |
|---|
| Important adverse
events | | | 0.045 |
|
Worsening of
visual acuity | 4 (16.6%) | 8 (36.4%) | 0.1 |
|
Hypotony | 2 (8.3%) | 4 (18.2%) | 0.41 |
|
Phtisis
bulbi | 0 (0%) | 2 (9.1%) | 0.22 |
| Other adverse
events | | | |
|
Prolonged
inflammation | 1 (4.1%) | 3 (13.6%) | |
|
Choroidal
detachment | 1 (4.1%) | 4 (18.2%) | |
|
Postoperative
intraocular pressure spike | 4 (16.6%) | 4 (18.2%) | |
|
Retinal
detachment | 0 (0%) | 3 (13.6%) | |
|
Hyphema | 3 (12.5%) | 2 (9.1%) | |
|
Neurotrophic
keratitits | 0 (0%) | 1 (4.5%) | |
|
Intravitreal
hemorrhage | 0 (0%) | 3 (13.6%) | |
| Table VIChanges in VA after TSCPC. |
Table VI
Changes in VA after TSCPC.
| Evolution of
best-corrected VA | Micropulse TSCPC N
(%) | Continuous wave
TSCPC N (%) |
P-valuea |
|---|
| Worsened | 4 (16.6%) | 8-(36.4%) | 0.10 |
| Unchanged | 19 (79.2%) | 14- (63.6%) | |
| Improved | 1 (4.2%) | 0 (0%) | |
Discussion
NVG is one of the most difficult to treat types of
glaucoma. Numerous treatment methods have been used with varying
degrees of success. TSCPC is a classic method used to treat NVG,
belonging to the broad category of cycloablative procedures. This
method has some advantages: i) it is incision-free, and thus, has a
very low risk of infection; ii) it is easy to perform (in the
operating room or even in an office setting); iii) it has a very
short learning curve (compared with trabeculectomy and glaucoma
drainage devices); iv) there is no need to stop anticoagulants; v)
there is a rapid onset of the effect; and, what is more, vi) it is
repeatable (12). The results of
our study confirmed that TSCPC can be a safe and reliable method
for managing NVG, using both of its variants, MP-TSCPC and
CW-TSCPC, each of them with advantages and disadvantages. A
successful result was defined as a postprocedural IOP between 5 and
21 mm Hg with or without additional medications or an IOP reduction
of more than 30% compared with the baseline. Hypotony, defined as
an IOP of <5 mm Hg was considered to be a failure of the
treatment. The definition of a successful result is a major problem
because it shows great variation among different studies. The
majority of other studies defined success as an IOP between 5 and
21 mm Hg (13-15);
other studies also included a reduction in IOP with at least 30%
from the baseline, as for example in a study by Aquino et al
(5), or a reduction with at least
20% from the baseline IOP, as for example in a study by Grueb et
al (16). Our cohort included
patients with advanced NVG, with high initial IOP and poor initial
VA and therefore it was considered that a reduction of IOP with 20%
would be inefficient in most cases.
Effects on IOP
MP-TSCPC proved to be short-term effective. The
success rate was 70.8% after the first week, 66.6% after the first
month, and 58.3% after 3 months. The success rate decreased after
three months and reached a level of only 29.1% at 12 months.
Numerous studies have reported better results than ours for
MP-TSCPC. Tan et al reported a success rate of 80% after 18
months of follow-up (10), Aquino
et al revealed a 75% success rate after 12 months (5), Preda et al reported a 65.63%
success rate at 18 months (17),
and Zaarour et al showed a 73.3% success rate at 12 months
(18), but all of these studies
included patients with different forms of refractory glaucoma, not
only NVG. Studies on cohorts with NVG revealed slightly poorer
outcomes, but some reported improved results, for example, Wong
et al reported a 26% success rate at 12 months and Souissi
et al revealed a 35% success rate at 9 months (19,20). A
total of 2 possible explanations were identified for this
difference. Firstly, our cohort was composed of patients with
advanced NVG (extremely low VA, multiple surgeries) and, secondly,
the laser settings, which were not at the highest possible level of
energy, may have contributed to inadequate control of IOP in the
long term. It is possible that to achieve a satisfactory IOP
control in patients with NVG, but an increase in the duration of
laser delivery may be necessary. A study by Williams et al
revealed improved results with a 74.7% success rate at 3 months
with a longer time interval of laser application, of up to 360 sec,
while using the same power (11).
CW-TSCPC exhibited a more constant effect during the follow-up
period. The success rate was 77.2% after the first week, 68.1%
after the first month, 72.2% at 3 months, and 54.5% at 12 months,
results that are similar to those of other studies. Singh et
al (21) reported a success
rate of 70% and Grueb et al (16), a 36.7% success rate, with different
periods of follow-up.
Effect on antiglaucoma medication
Both methods resulted in a decrease in the number of
topical antiglaucoma medications in the short term, which is
similar to the results reported by other studies. MP-TSCPC had the
most important reduction in medication number at 3 months, with the
mean number of medications decreasing from a baseline of 2.6±1 to
1.7±1.3, which was followed by a slight increase to 2.1±1.3 at 12
months. CW-TSCPC had similar results at 3 months, a decrease from
2.8±0.8 at baseline to 1.4±1.4 at 3 months, but the results tended
to be more stable in time reaching 1.9±1.1 at 12 months. The
possibility to stop the carbonic anhydrase inhibitor was an
important endpoint of the study and both methods proved effective
in reaching this goal. The number of patients requiring oral
acetazolamide decreased after both procedures: from 58.3% of
patients at baseline to 20.8% at 12 months in the MP-TSCPC group
and from 63.6% of patients at baseline to 27.2% at 12 months in the
CW-TSCPC group. Numerous studies have reported a decrease in the
number of antiglaucoma medications similar to our results (1,5,18,22).
Complications
Postoperative complications appeared in both groups,
but the incidence was higher in the CW-TSCPC group. There were 15
complications in 9 patients (37.5%) in the MP-TSCPC group and 34
complications in 15 patients (68.2%) in the CW-TSCPC group.
Potential complications in CW-TSCPC are considered to be secondary
to damage induced to the surrounding tissues by the thermal effect
of the laser. In MP-TSCPC the pulsatile pattern of the laser energy
delivery prevents excessive heating of the collateral tissues and
reduces the rate of complications (6). It is difficult to establish a
cause-and-effect relationship between TSCPC and the complications,
because some may appear as complications of the initial disease as
for example, tractional retinal detachment and intravitreal
hemorrhages in diabetic retinopathy, as well as late hyphema (2
cases in the MP-TSCPC group and one case in the CW-TSCPC appeared
more than 3 months after the procedure). The most frequent
complication was a decrease in VA; this occurred in 16.6% of cases
in the MP-TSCPC group and in 36.4% in the CW-TSCPC group. In other
studies worsening of the VA varies from 0 to 55.2% of the cases
(23-25).
However, it is difficult to compare our results with those of other
studies, because in our study the baseline BCVA was already
extremely poor (CF or less). Herein, although a higher incidence of
VA decline was reported after MP-TSCPC than in other studies such
as Aquino et al who revealed a 4% deterioration of BCVA and
Elhefney et al and Lee et al who revealed no decline
in BCVA, the fact that some of the cases probably had a decrease in
VA as a result of the evolution of the disease, and not as a result
of the procedure itself, must be taken into account (5,26,27).
Even though the difference between the two groups was not
statistically significant, it reached the trend level, and
therefore MP-TSCPC is considered to be safer than CW-TSCPC in what
post-procedural BCVA is concerned.
Another serious complication that was identified in
our study was ocular hypotony. It appeared in 2 patients (8.3% of
cases) in the MP-TSCPC group and in 4 patients (18.2% of cases) in
the CW-TSCPC group. Unfortunately, two of these cases finally
progressed to phthisis bulbi (9.1% of cases). In other studies,
some reported an incidence of hypotony similar to ours in the case
of CW-TSCPC, including Iliev and Gerber (15) with 17.6%, and Walland (28) with 18%, while some reported a higher
incidence such as the study by Nabili and Kirkness (22), but there were also studies reporting
a much lower incidence including studies by Vernon et al
(25) and Schlote et al
(8). Studies with a similar or
higher incidence of hypotony included a greater percentage of
patients with NVG, whereas the other ones had few or no patients
with NVG. This may be explained by the fact that eyes with NVG have
a disproportionate outflow resistance, while the aqueous humor
production is already damaged by ischemia. As such, any
cyclodestructive procedure, even a mild one, as is the case with
MP-TSCPC, can disturb the balance between outflow resistance and
the aqueous production, resulting in hypotony (22). Our study revealed that, with regard
to adverse effects (i.e., the decrease in VA, hypotony, and
phthisis bulbi), their higher occurrence rate in the CW-TSCPC group
vs. in the MP-TSCPC group was statistically significant
(P=0.045).
Limitations
The most important limitation of our study resides
in the small sample size for each group (24 and 22 cases,
respectively, for MP-TSCPC and CW-TSCPC). Another limitation
emerges from the retrospective nature of the study and from the
fact that not all the data were available for all the patients.
However, the patients were observed concurrently by the authors and
followed the same visit schedule and, what is more, the study had a
12-month follow-up on 46 of the 51, or 90%, of the patients who
underwent the intervention. Our center is a tertiary care center,
and thus the postoperative visits of some of the patients took
place in their primary care center. A lot of effort was made to
retrieve the data from those primary care centers, however, it
cannot be certain that the accuracy of the data is the same.
In conclusion, both methods, MP-TSCPC and CW-TSCPC,
could successfully manage NVG. CW-TSCPC exhibited higher IOP
control in the long term (which did not reach statistical
significance), but a significantly lower safety profile. MP-TSCPC
was revealed to be safer, but its efficacy may decline after three
months. Patients with advanced NVG may require higher laser energy
or longer application time.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MZ, DCB, FB, MB, IRB and FV conceived and designed
the study. MZ performed the surgical procedures. MZ, OMD, EAD, ACS
and IP performed the acquisition of data during the follow-up
visits. MZ, DCB, IRB, OMD, EAD, IP, ACS and FV participated in the
analysis and interpretation of the data. FV performed the
statistical analysis. MZ, FB and MB drafted the manuscript. MZ,
DCB, FB, MB and IRB critically reviewed the manuscript. MZ and OMD
confirm the authenticity of all the raw data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the institutional review
board of ‘Dr. Carol Davila’ Central Military Emergency University
Hospital (Bucharest, Romania) and followed the principles of the
Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fong AW, Lee GA, O'Rourke P and Thomas R:
Management of neovascular glaucoma with transscleral
cyclophotocoagulation with diode laser alone versus combination
transscleral cyclophotocoagulation with diode laser and
intravitreal bevacizumab. Clin Exp Ophthalmol. 39:318–323.
2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sivak-Callcott JA, O'Day DM, Gass JD and
Tsai JC: Evidence-based recommendations for the diagnosis and
treatment of neovascular glaucoma. Ophthalmology. 108:1767–1777,
1800. 2001.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ndulue JK, Rahmatnejad K, Sanvicente C,
Wizov SS and Moster MR: Evolution of cyclophotocoagulation. J
Ophthalmic Vis Res. 13:55–61. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Burgess SE, Silverman RH, Coleman DJ,
Yablonski ME, Lizzi FL, Driller J, Rosado A and Dennis PH Jr:
Treatment of glaucoma with high-intensity focused ultrasound.
Ophthalmology. 93:831–838. 1986.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Aquino MC, Barton K, Tan AM, Sng C, Li X,
Loon SC and Chew PT: Micropulse versus continuous wave transscleral
diode cyclophotocoagulation in refractory glaucoma: A randomized
exploratory study. Clin Exp Ophthalmol. 43:40–46. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ma A, Yu SWY and Wong JKW: Micropulse
laser for the treatment of glaucoma: A literature review. Surv
Ophthalmol. 64:486–497. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Pastor SA, Singh K, Lee DA, Juzych MS, Lin
SC, Netland PA and Nguyen NT: Cyclophotocoagulation: A report by
the American Academy of Ophthalmology. Ophthalmology.
108:2130–2138. 2001.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Schlote T, Derse M, Rassmann K, Nicaeus T,
Dietz K and Thiel HJ: Efficacy and safety of contact transscleral
diode laser cyclophotocoagulation for advanced glaucoma. J
Glaucoma. 10:294–301. 2001.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Amoozgar B, Phan EN, Lin SC and Han Y:
Update on ciliary body laser procedures. Curr Opin Ophthalmol.
28:181–186. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Tan AM, Chockalingam M, Aquino MC, Lim ZI,
See JL and Chew PT: Micropulse transscleral diode laser
cyclophotocoagulation in the treatment of refractory glaucoma. Clin
Exp Ophthalmol. 38:266–272. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Williams AL, Moster MR, Rahmatnejad K,
Resende AF, Horan T, Reynolds M, Yung E, Abramowitz B, Kuchar S and
Waisbourd M: Clinical efficacy and safety profile of micropulse
transscleral cyclophotocoagulation in refractory glaucoma. J
Glaucoma. 27:445–449. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Stanca HT, Munteanu M, Jianu DC, Motoc
AGM, Tăbăcaru B, Stanca S, Ungureanu E, Boruga VM and Preda MA: New
perspectives in the use of laser diode transscleral
cyclophotocoagulation. A prospective single center observational
cohort study. Rom J Morphol Embryol. 59:869–872. 2018.PubMed/NCBI
|
|
13
|
Ramli N, Htoon HM, Ho CL, Aung T and
Perera S: Risk factors for hypotony after transscleral diode
cyclophotocoagulation. J Glaucoma. 21:169–173. 2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Murphy CC, Burnett CA, Spry PG, Broadway
DC and Diamond JP: A two centre study of the dose-response relation
for transscleral diode laser cyclophotocoagulation in refractory
glaucoma. Br J Ophthalmol. 87:1252–1257. 2003.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Iliev ME and Gerber S: Long-term outcome
of trans-scleral diode laser cyclophotocoagulation in refractory
glaucoma. Br J Ophthalmol. 91:1631–1635. 2007.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Grueb M, Rohrbach JM, Bartz-Schmidt KU and
Schlote T: Transscleral diode laser cyclophotocoagulation as
primary and secondary surgical treatment in primary open-angle and
pseudoexfoliatve glaucoma. Long-term clinical outcomes. Graefes
Arch Clin Exp Ophthalmol. 244:1293–1299. 2006.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Preda MA, Karancsi OL, Munteanu M and
Stanca HT: Clinical outcomes of micropulse transscleral
cyclophotocoagulation in refractory glaucoma-18 months follow-up.
Lasers Med Sci. 35:1487–1491. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zaarour K, Abdelmassih Y, Arej N, Cherfan
G, Tomey KF and Khoueir Z: Outcomes of micropulse transscleral
cyclophotocoagulation in uncontrolled glaucoma patients. J
Glaucoma. 28:270–275. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Wong KYT, Aquino CM, Macasaet AM,
Suwandono ME, Chew PTK and Koh VTC: MP3 plus: A modified micropulse
transscleral cyclophototherapy technique for the treatment of
refractory glaucoma. J Glaucoma. 29:264–270. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Souissi S, Baudouin C, Labbé A and Hamard
P: Micropulse transscleral cyclophotocoagulation using a standard
protocol in patients with refractory glaucoma naive of
cyclodestruction. Eur J Ophthalmol. 31:112–119. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Singh K, Jain D and Veerwal V: Diode laser
cyclophotocoagulation in Indian eyes: Efficacy and safety. Int
Ophthalmol. 37:79–84. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Nabili S and Kirkness CM: Trans-scleral
diode laser cyclophoto-coagulation in the treatment of diabetic
neovascular glaucoma. Eye (Lond). 18:352–356. 2004.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ishida K: Update on results and
complications of cyclophotocoagulation. Curr Opin Ophthalmol.
24:102–110. 2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ocakoglu O, Arslan OS and Kayiran A: Diode
laser transscleral cyclophotocoagulation for the treatment of
refractory glaucoma after penetrating keratoplasty. Curr Eye Res.
30:569–574. 2005.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Vernon SA, Koppens JM, Menon GJ and Negi
AK: Diode laser cycloablation in adult glaucoma: Long-term results
of a standard protocol and review of current literature. Clin Exp
Ophthalmol. 34:411–420. 2006.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Elhefney EM, Mokbel TH, Hagras SM, AlNagdy
AA, Ellayeh AA, Mohsen TA and Gaafar WM: Micropulsed diode laser
cyclophotocoagulation in recurrent pediatric glaucoma. Eur J
Ophthalmol. 30:1149–1155. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Lee JH, Shi Y, Amoozgar B, Aderman C, De
Alba Campomanes A, Lin S and Han Y: Outcome of micropulse laser
transscleral cyclophotocoagulation on pediatric versus adult
glaucoma patients. J Glaucoma. 26:936–939. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Walland MJ: Diode laser
cyclophotocoagulation: Longer term follow up of a standardized
treatment protocol. Clin Exp Ophthalmol. 28:263–267.
2000.PubMed/NCBI View Article : Google Scholar
|