Introduction
Hematological malignant tumors represent a group of
major diseases carrying a substantial risk to the lives of affected
patients (1). Allogeneic
hematopoietic stem cell transplantation (allo-HSCT) stands as the
primary treatment approach for a wide range of hematologic
conditions (such as acute myeloid leukemia and acute lymphoblastic
leukemia) (2). The considerable
advancement in the HSCT technique has resulted in a significant
improvement in the survival rate of these patients (3).
However, post-hematopoietic stem cell
transplantation has significant and potentially severe
complications. These complications encompass organ damage resulting
from pretreatment toxicity, prolonged impairment of immune
reconstitution and concomitant opportunistic infections (4-6).
These adverse events collectively exert a considerable impact on
the prognosis of patients undergoing hematopoietic stem cell
transplantation (5-8).
In a comprehensive population-based cohort study involving 87,965
adults newly diagnosed with hematologic malignancies, patients
admitted to the intensive care unit (ICU) were primarily those
undergoing transplant procedures. The one-year incidence of ICU
admissions stood at 13.9%, with differences observed across
different hematologic conditions, ranging from 7.3% in cases of
indolent lymphoma to as high as 22.5% in cases of acute myeloid
leukemia (9). However, despite the
utilization of diverse rescue interventions, the prognosis of
patients with hematologic malignancies remains unsatisfactory
(10). This persistent challenge
underscores the critical and pressing imperative to identify the
risk factors associated with unfavorable prognoses in these
patients. Risk factors influencing mortality in critically ill
patients have been a research focus in recent studies, with various
variables being assessed. The acquired data have identified
mechanical ventilation, the initial acute physiologic and chronic
health assessment II (APACHE II) scores recorded on the day of ICU
admission, compromised performance status, vasoactive therapy and
the presence of malignant lymphoma as potential risk factors for
ICU mortality in patients with hematologic malignancies (11-17).
However, it is important to note that the identified risk factors
do not consistently align across different studies.
Some investigations have delved into specific
categories of hematologic malignancies or certain complications of
allo-HSCT to identify prognostic factors for ICU mortality
(18,19). Several studies have also focused on
allogeneic transplantation (20,21),
including a multicenter study in Brazil that explored a cohort of
patients that had undergone autologous hematopoietic stem cell
transplantation with ICU admission (22). Additionally, a retrospective study
in France evaluated whether haploidentical hematopoietic stem cell
transplantation (Haplo-SCT) procedures affect the prognosis of
critically ill recipients of allo-HSCT (23). However, few studies have explored
the ICU mortality of patients undergoing Haplo-SCT and those
undergoing identical sibling donor (ISD) transplantation.
Therefore, a retrospective analysis of the clinical
features, treatment approaches and outcomes among patients
undergoing allo-HSCT was conducted, aiming to identify risk factors
for ICU mortality and develop predictive models. Furthermore, the
present study analyzed and compared the mortality rate of patients
who underwent Haplo-SCT and those who underwent ISD
transplantation.
Materials and methods
Study design
The present single-center retrospective study
collected data anonymously from adult patients diagnosed with
hematological malignancies who underwent allo-HSCT at the ICU of
the Haidian Branch of Peking University People's Hospital (Beijing,
China). The data collection process spanned a defined timeframe,
commencing on February 1, 2019, and concluding on March 30, 2021.
The present study was approved by The Ethics Committee of Peking
University People's Hospital (approval no. 2022PHB267-001; Beijing,
China). Decisions regarding patient transfer to the ICU and
informed consent procedures were jointly made by the ICU staff and
hematologists, with consent obtained from the patients, their
parents or their guardians.
Inclusion and exclusion criteria
The inclusion criteria were as follows: i) Adult
patients aged 18 years or older; ii) patients diagnosed with one or
more hematologic malignancies; and iii) patients admitted to the
ICU due to severe diseases during the specified period from
February 1, 2019, to March 30, 2022. The exclusion criteria were as
follows: i) Patients under the age of 18; and ii) those with
nonmalignant hematologic disorders.
Data collection
The researchers collected a comprehensive dataset
for each individual, including information regarding the age, sex,
time of ICU admission, underlying disease, reason for ICU
admission, laboratory test results, APACHE II score, treatment
received on the day of admission, duration of ICU stay and
hospitalization, therapeutic regimen prior to ICU admission and
presence of organ failure of the patients. Additionally, for
patients who survived, follow-up continued until August 1, 2022, to
monitor their progress and outcomes.
Definition
Acute heart failure and infectious toxic shock were
defined per the 2021 European Society of Cardiology Guidelines and
the 2016 Infectious Toxic Shock Guidelines, respectively (24,25).
Acute kidney injury was defined and treated per the 2012 Kidney
Disease Outcomes Quality Initiative clinical guidelines (26). Liver failure was defined and
treated in line with international recommendations (27,28).
Patients received comprehensive treatment, including anti-infective
therapy, continuous renal replacement therapy (CRRT),
plasmapheresis, mechanical ventilation (MV) which encompassed both
non-invasive ventilation (NIV) and invasive MV (IMV), hormone
therapy and immunotherapy selected in accordance with the
international recommendations (26,29-34).
Vasoactive drug administration upon admission was
defined as any vasoactive drug or inotrope initiated within two
hours of ICU admission. Neutropenia was defined as a neutrophil
count <0.5x109/l.
Statistical analysis
The statistical methods employed in the present
study were designed to analyze and evaluate the clinical outcomes.
The primary clinical outcome was the ICU mortality, with a
secondary emphasis on the 60-day mortality after ICU admission.
Enumeration data were presented as percentages, and the inter-group
comparisons were conducted utilizing the chi-square test. In cases
where continuous variables did not conform to a normal
distribution, the data were presented as median (interquartile
range) [M (QL, QU)], and comparisons between independent samples
were made via the Mann-Whitney U test. The ICU mortality hazard
ratio was estimated utilizing both univariate and multivariate Cox
regression analyses. These analyses provided insights into the risk
factors associated with ICU mortality. The Kaplan-Meier curve, a
valuable tool in survival analysis, was employed to estimate the
probability of survival. P<0.05 was considered to indicate a
statistically significant difference. The statistical analyses were
carried out using SPSS 24.0 software (IBM Corp.) and R software (v
4.2.0; http://www.r-project.org).
Results
General features of the patients
The present research included a total of 108
patients, 58 of whom died in the ICU (53.7% ICU mortality); their
general characteristics are described in Table SI, Table SII and Table SIII.
The primary causes leading to their admission to the
ICU are outlined in Table SI.
Among these, respiratory failure emerged as the most prevalent
cause, accounting for a substantial portion of cases (52; 48.1% of
the total study population). Following closely was liver failure,
which constituted the cause of ICU admission in 23 patients (21.3%
of the total study population). The median APACHE II score during
admission was 20.0 (10.0-39.0). On the day of ICU admission,
vasoactive drugs were administered to 29 patients (26.9%).
Additionally, on the same day, 64 patients (59.3%) received NIV, 23
patients (21.3%) received IMV, 9 patients (8.3%) received CRRT and
28 patients (25.9%) received plasma exchange treatment (Table II).
 | Table IICharacteristics of clinical tests on
the day of ICU admission and treatments in ICU. |
Table II
Characteristics of clinical tests on
the day of ICU admission and treatments in ICU.
|
Characteristics | Haplo-SCT,
n=83 | ISD, n=25 | P-value |
|---|
| Laboratory test on
day of ICU admission | | | |
|
Median
lactate (range), mmol/l | 1.30
(0.20-30.0) | 1.10
(0.30-17.8) | 0.754 |
|
Median white
blood cell count (range), 109/l | 4.12
(2.27-7.18) | 5.47
(0.07-164.2) | 0.076 |
|
Median
neutrophil count (range), 109/l | 1.89 (0-17.42) | 3.03 (0-13.86) | 0.133 |
|
Neutropenia,
n (%) | 16 (19.27) | 4 (16.0) | 0.937 |
|
Median
lymphocyte count (range), 109/l | 0.38
(0.0-4.85) | 0.60
(0.0-2.48) | 0.116 |
|
Median
hemoglobin (range), g/l | 74.00
(40.00-115.00) | 88.00
(30.00-130.00) | 0.013 |
|
Median
platelet count (range), 109/l | 28.00
(2.00-213.00) | 43.00
(9.00-252) | 0.037 |
|
Median
creatinine (range), µmol/l | 72.00
(21.00-685.50) | 77.0
(37.0-346.0) | 0.613 |
|
Median
bilirubin (range), µmol/l | 15.55
(7.85-45.83) | 20.0
(4.2-595.0) | 0.807 |
|
Median serum
potassium (range), mmol/l | 3.78
(2.18-6.06) | 3.98
(2.83-5.82) | 0.325 |
|
Median brain
natriuretic peptide (range), pg/ml | 240 (10-4580) | 118 (8-4868) | 0.098 |
|
Median
fibrin degradation product (range), mg/l | 6.60
(0.7-115.2) | 6.80
(0.3-130.9) | 0.796 |
|
Median
D-dimer (range), µg/l | 649
(57.2-13183.0) | 714.0
(60.00-17594) | 0.997 |
| Median HCT-CI
(range) | 375 (2-592) | 375 (78-600) | 0.408 |
| Median APACHE II
score at admission (range) | 20.0
(10.00-39.00) | 22.0
(14.0-36.0) | 0.542 |
| Treatment at ICU
admission, n (%) | | | |
|
Use of
vasoactive drugs | 22 (26.5) | 7 (28.0) | 0.883 |
|
Invasive
mechanical ventilation | 18 (21.7) | 5 (20.0) | 0.857 |
|
Non-invasive
mechanical ventilation | 53 (63.9) | 11 (44.0) | 0.077 |
|
Continuous
renal replacement therapy | 9 (10.8) | 0 (0.0) | 0.191 |
|
Plasma
exchange | 21 (25.3) | 7 (28.0) | 0.787 |
| Median length of
ICU stay (range), days | 9.0 (0-39.0) | 9.0 (0-27.0) | 0.615 |
| Median follow-up of
survivors (range), days | 21 (0-1258) | 19 (0-1167) | 0.983 |
As shown in Table
I, ICU mortality was reported in 58 (53.7%) patients: of which
55.4 and 48.0% underwent Haplo-SCT and ISD, respectively (P=0.514).
The immediate causes of ICU mortality are shown in Table III. Furthermore, univariate Cox
regression analyses are presented in Table SV and Fig. S1 and show the independent risk
factors for the leading cause of ICU mortality.
| Table IClinical features of patients
admitted to the intensive care unit. |
Table I
Clinical features of patients
admitted to the intensive care unit.
|
Characteristics | All patients,
n=108 | Haplo-SCT,
n=83 | ISD, n=25 | P-value |
|---|
| Median age (range),
years | 41 (18-69) | 39 (18-69) | 45 (20-63) | 0.274 |
| Sex, female, n
(%) | 35 (32.4) | 29 (34.9) | 6 (24.0) | 0.743 |
| Hematologic
malignancies, n (%) | | | | 0.758 |
|
Acute
leukemia | 77 (71.3) | 60 (72.3) | 17 (68.0) | |
|
Chronic
leukemia | 8 (7.4) | 6 (7.2) | 2 (8.0) | |
|
Lymphoma | 9 (8.3) | 7 (8.4) | 2 (8.0) | |
|
Myelodysplastic
syndromes | 11 (10.2) | 7 (8.4) | 4 (16.0) | |
|
Other | 3 (2.8) | 3 (3.6) | 0 (0.0) | |
| Median WBC counts
at diagnosis (range), x109/l | 7.9 (0.8-399) | 7.9
(0.8-310.0) | 7.9
(1.2-399.0) | 0.852 |
| Median bone marrow
blasts at diagnosis (range), % | 44 (0-98.0) | 42.7 (0-98.0) | 45.0 (0-97.0) | 0.748 |
| Disease risk index
before HSCT, n (%) | | | | 0.763 |
|
Low-risk | 26 (24.1) | 19 (22.9) | 7 (28.0) | |
|
Intermediate-risk | 55 (50.9) | 42 (50.6) | 13 (52.0) | |
|
High-risk | 27 (25.0) | 22 (26.5) | 5 (20.0) | |
| Donor-recipient sex
matching, n (%) | | | | 0.463 |
|
Male-female | 19 (17.6) | 15 (18.1) | 4 (16.0) | |
|
Male-male | 38 (35.2) | 30 (36.1) | 8 (32.0) | |
|
Female-female | 16 (14.8) | 14 (16.9) | 2 (8.0) | |
|
Female-male | 35 (32.4) | 24 (28.9) | 11 (44.0) | |
| Relationship of
donor, n (%) | | | | <0.001 |
|
Parental | 31 (28.7) | 31 (37.3) | 0 (0.0) | |
|
Sibling | 49 (45.4) | 24 (28.9) | 25 (100.0) | |
|
Children | 25 (23.1) | 25 (30.1) | 0 (0.0) | |
|
Other | 3 (2.8) | 3 (3.6) | 0 (0.0) | |
| Donor and recipient
blood groups, n (%) | | | | 0.606 |
|
Same | 61 (56.5) | 48 (57.8) | 13 (52.0) | |
|
Different | 47 (43.5) | 35 (42.2) | 12 (48.0) | |
| Homozygous loci, n
(%) | | | | <0.001 |
|
3/6 | 72 (66.7) | 72 (86.7) | 0 (0.0) | |
|
4/6 | 11 (10.2) | 11 (13.3) | 0 (0.0) | |
|
6/6 | 25 (23.1) | 0 (0.0) | 25 (100.0) | |
| GVHD after HSCT, n
(%) | | | | |
|
aGVHD | 32 (29.6) | 24 (28.9) | 8 (32.0) | 0.767 |
|
cGVHD | 10 (9.3) | 6 (7.2) | 4 (16.0) | 0.351 |
| Chimeric state
after HSCT, n (%) | | | | |
|
Partial
chimerism | 2 (1.9) | 2 (2.4) | 0 (0.0) | 1.000 |
|
Complete
chimerism | 106 (98.1) | 81 (97.6) | 25 (100.0) | |
| Leading cause for
ICU admission, n (%)a | | | | 0.134 |
|
Respiratory
failure | 52 (48.1) | 40 (48.2) | 12 (48.0) | |
|
Liver
failure | 23 (21.3) | 17 (20.5) | 6 (24.0) | |
|
Acute kidney
injury | 5 (4.6) | 5 (6.0) | 0 (0.0) | |
|
Disorders of
consciousness | 6 (5.6) | 5 (6.0) | 1 (4.0) | |
|
Alveolar
hemorrhage | 5 (4.6) | 5 (6.0) | 0 (0.0) | |
|
Septic
shock | 9 (8.3) | 6 (7.2) | 3 (12.0) | |
|
Cerebrovascular
disease | 2 (1.9) | 0 (0) | 2 (8.0) | |
|
Heart
failure | 1 (0.9) | 1 (1.2) | 0 (0.0) | |
|
Other | 5 (4.6) | 4 (4.8) | 1 (4.0) | |
|
ICU
death | 58 (53.7) | 46 (55.4) | 12 (48.0) | 0.514 |
| Table IIIImmediate causes of ICU
mortality. |
Table III
Immediate causes of ICU
mortality.
| Causes | All patients, n=108
(%) | Haplo-SCT, n=83
(%) | ISD, n=25 (%) | P-value |
|---|
| Respiratory
failure | 26 (24.1) | 21 (25.3) | 5 (20.0) | 0.587 |
| Liver failure | 8 (7.4) | 6 (7.2) | 2 (8.0) | 1.000 |
| Gastrointestinal
bleeding | 5 (4.6) | 5 (6.0) | 0 (0) | 0.588 |
| Septic shock | 9 (8.3) | 6 (7.2) | 3 (12.0) | 0.429 |
| Cerebrovascular
disease | 4 (3.7) | 3 (3.6) | 1 (4.0) | 1.000 |
| Cardiopulmonary
arrest | 6 (5.6) | 5 (6.0) | 1 (4.0) | 1.000 |
The mortality of patients undergoing Haplo-SCT was
comparable to that of patients undergoing ISD. It was observed that
40 (37.0%) patients survived for more than 60 days after ICU
admission (Fig. 1A). Moreover, the
ICU mortality did not differ statistically between the ISD and
Haplo-SCT groups (Fig. 1B).
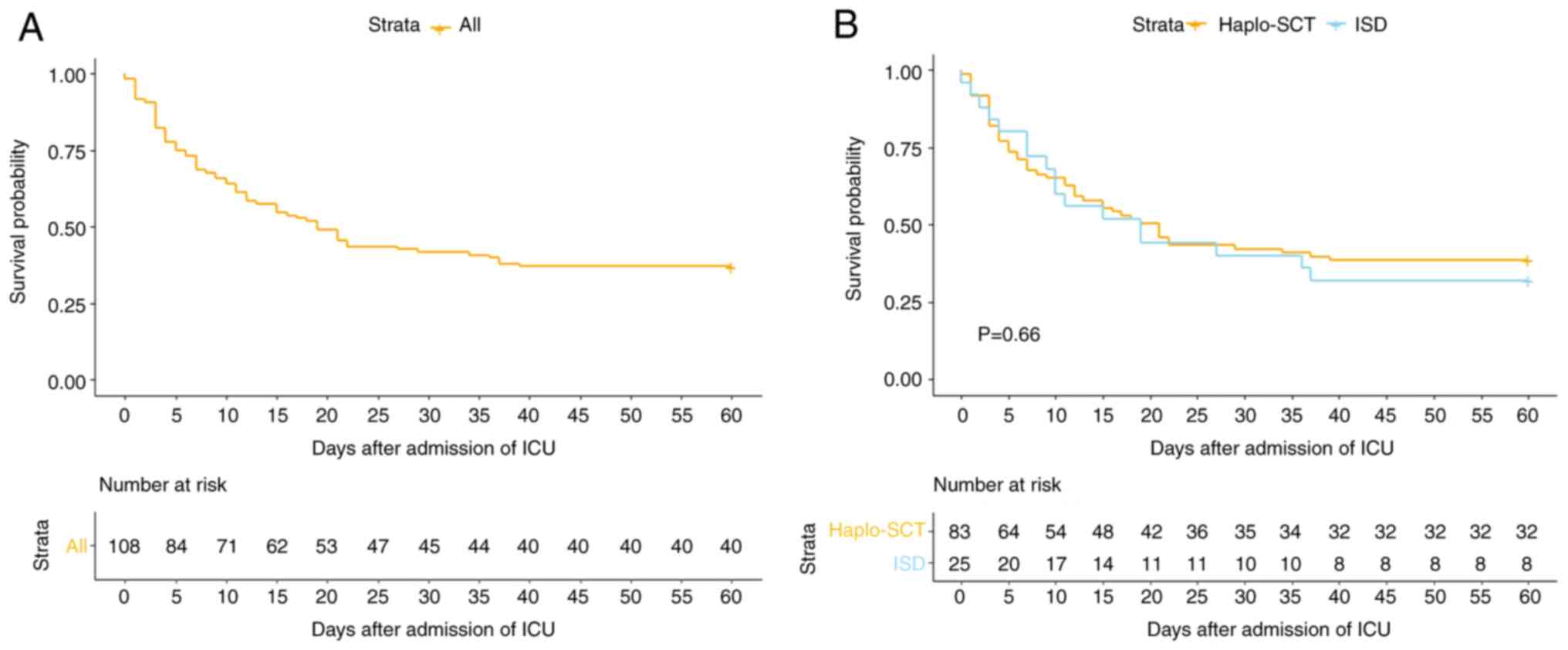 | Figure 1Kaplan-Meier curve showing the 60-day
survival probability for (A) all patients; and (B) Haplo-SCT
recipients and ISD HSCT recipients. The 60-day survival
probabilities for the three aforementioned populations were 37.0%
(95% CI, 29.0-47.4%), 38.5% (95% CI, 29.4-50.6%), 32.0% (95% CI,
18.1-56.7%), respectively, (P=0.66). Haplo-SCT, haploidentical
hematopoietic stem cell transplantation; ISD, identical sibling
donor; CI, confidence interval; HSCT, hematopoietic stem cell
transplantation; ICU, intensive care unit. |
Univariate analysis of ICU mortality
risk factors
In univariate analysis, ICU mortality was strongly
related to ICU admission due to respiratory failure, high
hematopoietic stem cell transplantation complication index score,
need for vasoactive therapy during ICU admission, neutropenia
during ICU admission, thrombocytopenia, reduced hemoglobin,
elevated bilirubin, elevated fibrinogen degradation products (FDP),
elevated brain natriuretic peptide (BNP), elevated lactate and high
APACHE II scores (Table SIV).
Multivariate analysis of risk factors
for ICU mortality
The patient condition-related indexes and
treatment-related indexes were divided into two groups for Cox
multivariate regression analysis. Decreased hemoglobin, elevated
total bilirubin, elevated BNP, elevated FDP, and elevated APACHE II
scores were recorded to be independent risk factors for ICU
mortality in the patient condition-related group (Fig. 2A). On the other hand, the need for
immediate initiation of vasoactive therapy and the need for IMV
during ICU admission were recorded to function as independent risk
factors for ICU mortality in the treatment-related group (Fig. 2B).
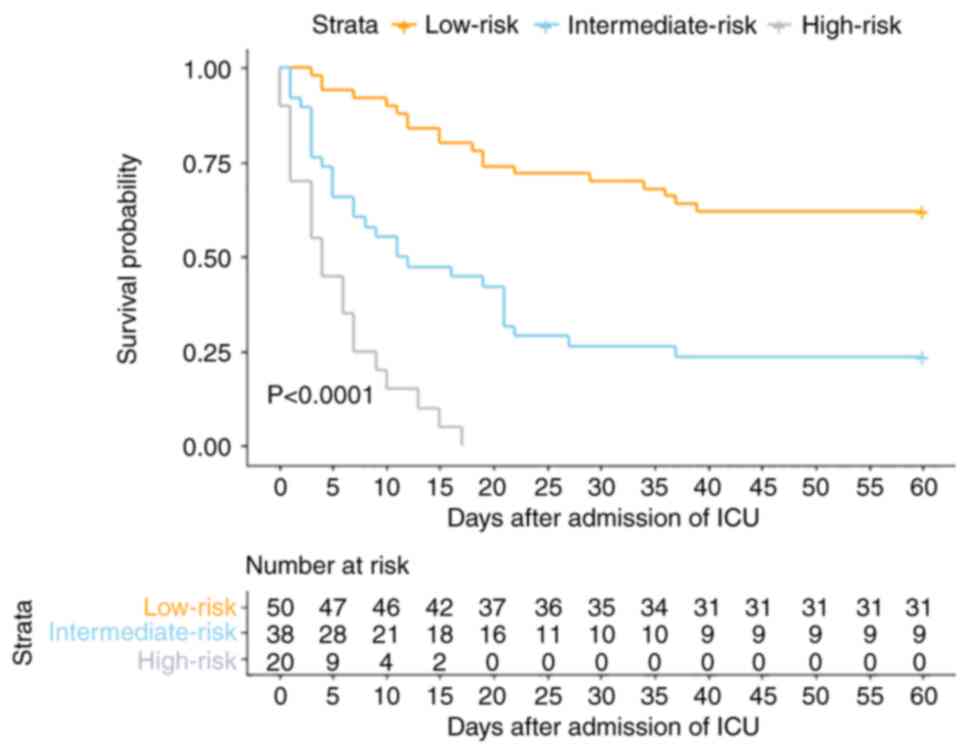
Risk model of ICU mortality
The patients were classified into the following
three groups based on the number of risk factors they presented: i)
Low-risk group, comprising patients with 0-2 risk factors (n=50);
ii) intermediate-risk group, comprising patients with 3-4 risk
factors (n=38); and iii) and high-risk group, comprising patients
with 5-7 risk factors (n=20). The ICU mortality rates in these
groups were as follows: 24.0% in the low-risk group, 68.4% in the
intermediate-risk group and 100.0% in the high-risk group
(χ2=38.295; P<0.001). Moreover, significant
differences were observed in the 60-day cumulative survival
following ICU admission among the three groups. The models
indicated a cumulative survival rate of 62.0% [95% confidence
interval (CI), 49.9-77.0%] in the low-risk group and 23.7% (95% CI,
13.4-41.9%) in the intermediate-risk group (Fig. 3).
Discussion
Critically ill patients suffering from hematologic
disorders typically necessitate an extended period of treatment and
care within medical facilities, which leads to a prolonged
hospitalization duration (11).
The intricate nature of their conditions often demands intensive
and specialized interventions, leading to increased investment in
healthcare resources and, consequently, elevated treatment costs
(35). Despite the extensive
medical attention and resources allocated, these patients commonly
face a poor prognosis (36). The
present study found that reduced hemoglobin, elevated total
bilirubin, elevated BNP, elevated FDP, need for vasoactive drugs at
ICU admission, need for IMV and elevated APACHE II scores were
independent risk factors for ICU mortality. Furthermore, the ICU
mortality rate considerably increased in patients with 5-7 risk
factors. To the best of our knowledge, the present study represents
the first analysis of risk factors for ICU mortality in patients
admitted to the ICU after allo-HSCT in China. It also introduces
the first prognostic model for predicting ICU mortality in such
patients.
ICU admissions have an elevated mortality rate
ranging from 27.6-84.1% (11,13-15,17).
Notably, the ICU mortality rate associated with patients having
undergone hematopoietic stem cell transplant is 53.7%, suggesting
that these patients have a poor prognosis. In the present research,
the median APACHE II score for admission was 20, a value consistent
with those reported in other investigations involving patients with
hematologic malignancies admitted to the ICU (initial APACHE II
score, 19.4-25) (12-15,17).
This similarity underscores the critical condition of patients upon
admission to the ICU, highlighting the severity of their
disease.
Short-term outcomes in critically ill patients with
hematologic malignancies primarily depend on organ failure rather
than the underlying malignancy features (37,38).
In the present study, independent risk factors for ICU mortality in
patients undergoing bone marrow transplantation included elevated
total bilirubin, the need for IMV support and the need for
vasoactive agents. These findings align with the results of
numerous studies associated with severe hematologic disorders
(38-40).
The present study observed a high risk of ICU
mortality among patients with low hemoglobin levels. Hemoglobin is
an important evaluation index for hematopoietic reconstruction
after hematopoietic stem cell transplantation, and patients with
poor hematopoietic reconstitution have an unfavorable prognosis
(41,42). It was also found that reduced
hemoglobin was an independent risk factor for mortality in
respiratory failure. Due to the fact that arterial blood oxygen
levels are contingent upon hemoglobin levels, anemia may hinder the
delivery of oxygen. Hemauer et al (43) have shown that lower hemoglobin is
associated with a higher probability of worsening respiratory
dysfunction scores the following day. Anemia is usually associated
with blood transfusion and positive fluid balance. Positive fluid
balance was an independent risk factor associated with 90-day
respiratory mortality in the ICU (44).
FDP is considered one of the markers of fibrin
deposition cleavage (45). Toh
et al (46) suggested that
FDP serves as a risk factor for mortality in patients with toxic
shock. In a prospective observational study conducted in Shanghai,
both indicators of reactive hyperfibrinolysis, D dimer and FDP,
were included. However, only FDP emerged as an independent risk
factor for ICU mortality in the multivariate analysis (47). In the present study,further
substantiates the significance of FDP as an independent risk factor
for ICU mortality in patients admitted following allo-HSCT.
Furthermore, Crone et al (48) suggested that elevated FDP
concentrations have been associated with the development of adult
respiratory distress syndrome. This study confirms that FDP is an
independent risk factor for mortality in respiratory failure.
Patients who undergo allo-HSCT can acquire intense
opportunistic infections pre- and post-treatment that can damage
the myocardium (49). A previous
study showed a 1.7% incidence of heart failure after hematopoietic
stem cell transplantation, which was associated with a poor
prognosis (4). The present study
showed that elevated BNP during ICU admission acts as an
independent risk factor for ICU mortality. Therefore, patients
presenting elevated BNP levels upon ICU admission should receive
close monitoring for myocardial protection and fine volume
management to improve their overall outcomes.
Traditionally, ISDs had been considered the optimal
donors (50,51). However, increasing evidence
suggests that Haplo-SCT should be viewed as a safe and effective
alternative, comparable to an ISD (52-54).
This research reveals that the outcomes of patients with critical
illness undergoing Haplo-SCT were comparable to those of patients
undergoing ISD transplantation.
Based on multivariate analysis, a prognostic model
was proposed, wherein patients with 5-7 risk factors exhibited an
ICU mortality rate of >90%. In the era of widespread allo-HSCT
usage, early identification of patients at a high risk of ICU
mortality can assist ICU healthcare professionals in devising more
effective diagnosis and treatment plans. Additionally, these
findings can play a pivotal role in facilitating communication
between healthcare providers and patients.
In summary, allo-HSCT stands as the primary
treatment approach for a wide range of hematologic conditions.
However, the post-hematopoietic stem cell transplantation landscape
faces significant and potentially severe complications. Risk
factors for mortality in critically ill patients have garnered
substantial attention in recent research endeavors. However, only a
limited number of studies have explored the ICU mortality in
patients undergoing Haplo-SCT and those undergoing ISD
transplantation.
The present research revealed that ICU mortality
rates remain elevated among patients undergoing allo-HSCT. However,
the outcomes of patients undergoing Haplo-SCT were comparable to
those of patients undergoing ISD transplantation. The present study
identified independent risk factors for ICU mortality and proposed
a prognostic model. These findings can provide valuable guidance
for intensive care physicians and hematologists in optimizing
clinical decisions.
Supplementary Material
Multivariable analysis of risk factors
for respiratory failure mortality. All of the variables were
collected on the day of ICU admission. APACHII, acute physiologic
and chronic health assessment II; ICU, intensive care unit; FDP,
fibrinogen degradation products.
Clinical features for post-transplant
patients admitted to the ICU.
Characteristics of patients receiving
HSCT.
Characteristics of clinical tests on
the day of ICU admission and treatments in ICU.
Univariable analyses of prognostic
factors for ICU mortality.
Univariable analyses of leading cause
for respiratory failure mortality.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by The National Key Research
and Development Program of China (grant no. 2018YFC2001905).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
PW and HZ conceptualized the study; PW, WH, SL and
JL curated the data; PW performed the formal analysis. PW, WH, and
YA performed the study methodology; PW and YA performed project
administration; PW wrote the original draft of the manuscript. PW,
WH and YA reviewed and edited the manuscript. All authors read and
approved the final version of the manuscript. HZ and JL confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
The study was conducted in accordance with the
Declaration of Helsinki, and the protocol was approved by The
Institutional Review Board of Peking University People's Hospital
(approval no. 2022PHB267-001; Beijing, China). Irrespective of this
analysis, all patients provided informed consent before receiving
treatment.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sant M, Minicozzi P, Mounier M, Anderson
LA, Brenner H, Holleczek B, Marcos-Gragera R, Maynadié M, Monnereau
A, Osca-Gelis G, et al: Survival for haematological malignancies in
Europe between 1997 and 2008 by region and age: Results of
EUROCARE-5, a population-based study. Lancet Oncol. 15:931–942.
2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Gratwohl A, Baldomero H, Aljurf M,
Pasquini MC, Bouzas LF, Yoshimi A, Szer J, Lipton J, Schwendener A,
Gratwohl M, et al: Hematopoietic stem cell transplantation: A
global perspective. JAMA. 303:1617–1624. 2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Gooley TA, Chien JW, Pergam SA, Hingorani
S, Sorror ML, Boeckh M, Martin PJ, Sandmaier BM, Marr KA, Appelbaum
FR, et al: Reduced mortality after allogeneic hematopoietic-cell
transplantation. N Engl J Med. 363:2091–2101. 2010.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mo XD, Xu LP, Liu DH, Zhang XH, Chen H,
Chen YH, Han W, Wang Y, Wang FR, Wang JZ, et al: Heart failure
after allogeneic hematopoietic stem cell transplantation. Int J
Cardiol. 167:2502–2506. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Shen MZ, Li JX, Zhang XH, Xu LP, Wang Y,
Liu KY, Huang XJ, Hong SD and Mo XD: Meta-Analysis of Interleukin-2
Receptor Antagonists as the Treatment for Steroid-Refractory Acute
Graft-Versus-Host Disease. Front Immunol. 12(749266)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Shen MZ, Hong SD, Wang J, Zhang XH, Xu LP,
Wang Y, Yan CH, Chen H, Chen YH, Han W, et al: A predicted model
for refractory/recurrent cytomegalovirus infection in acute
leukemia patients after haploidentical hematopoietic stem cell
transplantation. Front Cell Infect Microbiol.
12(862526)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Liu SN, Zhang XH, Xu LP, Wang Y, Yan CH,
Chen H, Chen YH, Han W, Wang FR, Wang JZ, et al: Prognostic factors
and long-term follow-up of basiliximab for steroid-refractory acute
graft-versus-host disease: Updated experience from a large-scale
study. Am J Hematol. 95:927–936. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Fan S, Huo WX, Yang Y, Shen MZ and Mo XD:
Efficacy and safety of ruxolitinib in steroid-refractory
graft-versus-host disease: A meta-analysis. Front Immunol.
13(954268)2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ferreyro BL, Scales DC, Wunsch H, Cheung
MC, Gupta V, Saskin R, Thyagu S and Munshi L: Critical illness in
patients with hematologic malignancy: A population-based cohort
study. Intensive Care Med. 47:1104–1114. 2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Soubani AO, Kseibi E, Bander JJ, Klein JL,
Khanchandani G, Ahmed HP and Guzman JA: Outcome and prognostic
factors of hematopoietic stem cell transplantation recipients
admitted to a medical ICU. Chest. 126:1604–1611. 2004.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Azoulay E, Mokart D, Pène F, Lambert J,
Kouatchet A, Mayaux J, Vincent F, Nyunga M, Bruneel F, Laisne LM,
et al: Outcomes of critically ill patients with hematologic
malignancies: prospective multicenter data from France and
Belgium-a groupe de recherche respiratoire en réanimation
onco-hématologique study. J Clin Oncol. 31:2810–2818.
2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Grgic Medic M, Gornik I and Gasparovic V:
Hematologic malignancies in the medical intensive care
unit-Outcomes and prognostic factors. Hematology. 20:247–253.
2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cuthbertson BH, Rajalingam Y, Harrison S
and McKirdy F: The outcome of haematological malignancy in scottish
intensive care units. J Intensive Care Soc. 9:135–140. 2008.
|
|
14
|
Yeo CD, Kim JW, Kim SC, Kim YK, Kim KH,
Kim HJ, Lee S and Rhee CK: Prognostic factors in critically ill
patients with hematologic malignancies admitted to the intensive
care unit. J Crit Care. 27:739 e1–e6. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Liu J, Cheng Q, Yang Q, Li X, Shen X,
Zhang L, Liu Z and Khoshnood K: Prognosis-related factors in
intensive care unit (ICU) patients with hematological malignancies:
A retrospective cohort analysis in a Chinese population.
Hematology. 20:494–503. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Irie H, Otake T, Kawai K, Hino M, Namazu
A, Shinjo Y and Yamashita S: Prognostic factors in critically ill
patients with hematological malignancy admitted to the general
intensive care unit: a single-center experience in Japan. J Anesth.
31:736–743. 2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Bird GT, Farquhar-Smith P, Wigmore T,
Potter M and Gruber PC: Outcomes and prognostic factors in patients
with haematological malignancy admitted to a specialist cancer
intensive care unit: A 5 yr study. Br J Anaesth. 108:452–459.
2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Desprez C, Kouatchet A, Marchand T, Mear
JB, Tadié JM, Peterlin P, Chevalier P, Canet E, Couturier MA,
Guillerm G, et al: Outcome of patients with newly diagnosed AML
admitted to the ICU, including preemptive admission-a multi-center
study. Ann Hematol. 102:1383–1393. 2023.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Lueck C, Tzalavras A, Wohlfarth P, Meedt
E, Kiehl M, Turki AT, Hoeper MM, Eder M, Cserna J, Buchtele N, et
al: Impact of chronic graft-versus-host-disease on intensive care
outcome in allogeneic hematopoietic stem cell recipients. Bone
Marrow Transplant. 58:303–310. 2023.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Díaz-Lagares C, Fox L, García-Roche A,
Santafe M, Romera I, Barba P, Pacheco A, Roldán E, Plata-Menchaca
E, Roca O, et al: Sequential organ failure assessment score and the
need for organ support predict mortality in allogeneic stem cell
transplant patients admitted to the intensive care unit. Transplant
Cell Ther. 27:865.e1–865.e7. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mokart D, Granata A, Crocchiolo R, Sannini
A, Chow-Chine L, Brun JP, Bisbal M, Faucher M, Faucher C, Blache
JL, et al: Allogeneic hematopoietic stem cell transplantation after
reduced intensity conditioning regimen: Outcomes of patients
admitted to intensive care unit. J Crit Care. 30:1107–1113.
2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Nassar AP Jr, Archanjo LVF, Ranzani OT,
Zampieri FG, Salluh JIF, Cavalcanti GFR, Moreira CEN, Viana WN,
Costa R, Melo UO, et al: Characteristics and outcomes of autologous
hematopoietic stem cell transplant recipients admitted to intensive
care units: A multicenter study. J Crit Care.
71(154077)2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Gournay V, Dumas G, Lavillegrand JR,
Hariri G, Urbina T, Baudel JL, Ait-Oufella H, Maury E, Brissot E,
Legrand O, et al: Outcome of allogeneic hematopoietic stem cell
transplant recipients admitted to the intensive care unit with a
focus on haploidentical graft and sequential conditioning regimen:
Results of a retrospective study. Ann Hematol. 100:2787–2797.
2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
McDonagh TA, Metra M, Adamo M, Gardner RS,
Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, et
al: 2021 ESC Guidelines for the diagnosis and treatment of acute
and chronic heart failure. Eur Heart J. 42:3599–3726.
2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Rhodes A, Evans LE, Alhazzani W, Levy MM,
Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally
ME, et al: Surviving sepsis campaign: International guidelines for
management of sepsis and septic shock: 2016. Intensive Care Med.
43:304–377. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Palevsky PM, Liu KD, Brophy PD, Chawla LS,
Parikh CR, Thakar CV, Tolwani AJ, Waikar SS and Weisbord SD: KDOQI
US commentary on the 2012 KDIGO clinical practice guideline for
acute kidney injury. Am J Kidney Dis. 61:649–672. 2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Flamm SL, Yang YX, Singh S and Falck-Ytter
YT: AGA Institute Clinical Guidelines Committee. American
gastroenterological association institute guidelines for the
diagnosis and management of acute liver failure. Gastroenterology.
152:644–647. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Bajaj JS, O'Leary JG, Lai JC, Wong F, Long
MD, Wong RJ and Kamath PS: Acute-on-Chronic liver failure clinical
guidelines. Am J Gastroenterol. 117:225–252. 2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Murugan R, Hoste E, Mehta RL, Samoni S,
Ding X, Rosner MH, Kellum JA and Ronco C: Acute Disease Quality
Initiative (ADQI) Consensus Group. Precision fluid management in
continuous renal replacement therapy. Blood Purif. 42:266–278.
2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Abe T, Matsuo H, Abe R, Abe S, Asada H,
Ashida A, Baba A, Eguchi K, Eguchi Y, Endo Y, et al: The Japanese
Society for Apheresis clinical practice guideline for therapeutic
apheresis. Ther Apher Dial. 25:728–876. 2021.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Nava S and Hill N: Non-invasive
ventilation in acute respiratory failure. Lancet. 374:250–259.
2009.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Rochwerg B, Brochard L, Elliott MW, Hess
D, Hill NS, Nava S and Navalesi P: Members Of The Steering
Committee. Antonelli M, Brozek J, et al: Official ERS/ATS clinical
practice guidelines: Noninvasive ventilation for acute respiratory
failure. Eur Respir J. 50(1602426)2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Baden LR, Swaminathan S, Angarone M,
Blouin G, Camins BC, Casper C, Cooper B, Dubberke ER, Engemann AM,
Freifeld AG, et al: Prevention and treatment of cancer-related
infections, version 2.2016, NCCN clinical practice guidelines in
oncology. J Natl Compr Canc Netw. 14:882–913. 2016.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Gauzit R, Castan B, Bonnet E, Bru JP,
Cohen R, Diamantis S, Faye A, Hitoto H, Issa N, Lebeaux D, et al:
Anti-infectious treatment duration: The SPILF and GPIP French
guidelines and recommendations. Infect Dis Now. 51:114–139.
2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Azoulay E, Schellongowski P, Darmon M,
Bauer PR, Benoit D, Depuydt P, Divatia JV, Lemiale V, van Vliet M,
Meert AP, et al: The Intensive Care Medicine research agenda on
critically ill oncology and hematology patients. Intensive Care
Med. 43:1366–1382. 2017.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Hill QA: Intensify, resuscitate or
palliate: Decision making in the critically ill patient with
haematological malignancy. Blood Rev. 24:17–25. 2010.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Blot F, Guiguet M, Nitenberg G, Leclercq
B, Gachot B and Escudier B: Prognostic factors for neutropenic
patients in an intensive care unit: respective roles of underlying
malignancies and acute organ failures. Eur J Cancer. 33:1031–1037.
1997.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Benoit DD, Vandewoude KH, Decruyenaere JM,
Hoste EA and Colardyn FA: Outcome and early prognostic indicators
in patients with a hematologic malignancy admitted to the intensive
care unit for a life-threatening complication. Crit Care Med.
31:104–112. 2003.PubMed/NCBI View Article : Google Scholar
|
|
39
|
van der Heiden PLJ, Arbous MS, van Beers
EJ, van den Bergh WM, le Cessie S, Demandt AMP, Eefting M, Hess C,
Kusadasi N, Marijt WAF, et al: Predictors of short-term and
long-term mortality in critically ill patients admitted to the
intensive care unit following allogeneic stem cell transplantation.
Bone Marrow Transplant. 54:418–424. 2019.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Pène F, Aubron C, Azoulay E, Blot F,
Thiéry G, Raynard B, Schlemmer B, Nitenberg G, Buzyn A, Arnaud P,
et al: Outcome of critically ill allogeneic hematopoietic stem-cell
transplantation recipients: A reappraisal of indications for organ
failure supports. J Clin Oncol. 24:643–649. 2006.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Akahoshi Y, Kanda J, Gomyo A, Hayakawa J,
Komiya Y, Harada N, Kameda K, Ugai T, Wada H, Ishihara Y, et al:
Risk factors and impact of secondary failure of platelet recovery
after allogeneic stem cell transplantation. Biol Blood Marrow
Transplant. 22:1678–1683. 2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Ivanov V, Faucher C, Mohty M, Bilger K,
Ladaique P, Sainty D, Arnoulet C, Chabannon C, Vey N, Camerlo J, et
al: Early administration of recombinant erythropoietin improves
hemoglobin recovery after reduced intensity conditioned allogeneic
stem cell transplantation. Bone Marrow Transplant. 36:901–906.
2005.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Hemauer SJ, Kingeter AJ, Han X, Shotwell
MS, Pandharipande PP and Weavind LM: Daily lowest hemoglobin and
risk of organ dysfunctions in critically Ill patients. Crit Care
Med. 45:e479–e484. 2017.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Gündoğan K, Akbudak İH, Hancı P, Halaçlı
B, Temel Ş, Güllü Z, İnci K, Bilir Y, Bozkurt FT, Yıldırım F, et
al: Clinical outcomes and independent risk factors for 90-day
mortality in critically Ill patients with respiratory failure
infected with SARS-CoV-2: A multicenter study in turkish intensive
care units. Balkan Med J. 38:296–303. 2021.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Eisenberg PR, Jaffe AS, Stump DC, Collen D
and Bovill EG: Validity of enzyme-linked immunosorbent assays of
cross-linked fibrin degradation products as a measure of clot
lysis. Circulation. 82:1159–1168. 1990.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Toh JM, Ken-Dror G, Downey C and Abrams
ST: The clinical utility of fibrin-related biomarkers in sepsis.
Blood Coagul Fibrinolysis. 24:839–843. 2013.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Fei A, Lin Q, Liu J, Wang F, Wang H and
Pan S: The relationship between coagulation abnormality and
mortality in ICU patients: A prospective, observational study. Sci
Rep. 5(9391)2015.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Crone KR, Lee KS and Kelly DL Jr:
Correlation of admission fibrin degradation products with outcome
and respiratory failure in patients with severe head injury.
Neurosurgery. 21:532–536. 1987.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Hertenstein B, Stefanic M, Schmeiser T,
Scholz M, Göller V, Clausen M, Bunjes D, Wiesneth M, Novotny J and
Kochs M: Cardiac toxicity of bone marrow transplantation:
Predictive value of cardiologic evaluation before transplant. J
Clin Oncol. 12:998–1004. 1994.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Szydlo R, Goldman JM, Klein JP, Gale RP,
Ash RC, Bach FH, Bradley BA, Casper JT, Flomenberg N, Gajewski JL,
et al: Results of allogeneic bone marrow transplants for leukemia
using donors other than HLA-identical siblings. J Clin Oncol.
15:1767–1777. 1997.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Howard CA, Fernandez-Vina MA, Appelbaum
FR, Confer DL, Devine SM, Horowitz MM, Mendizabal A, Laport GG,
Pasquini MC and Spellman SR: Recommendations for donor human
leukocyte antigen assessment and matching for allogeneic stem cell
transplantation: consensus opinion of the Blood and Marrow
Transplant Clinical Trials Network (BMT CTN). Biol Blood Marrow
Transplant. 21:4–7. 2015.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Yang B, Yu R, Cai L, Bin Guo, Chen H,
Zhang H, He P and Lu X: Haploidentical versus matched donor stem
cell transplantation for patients with hematological malignancies:
A systemic review and meta-analysis. Bone Marrow Transplantation.
54:99–122. 2019.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Rashidi A, Hamadani M, Zhang MJ, Wang HL,
Abdel-Azim H, Aljurf M, Assal A, Bajel A, Bashey A, Battiwalla M,
et al: Outcomes of haploidentical vs matched sibling
transplantation for acute myeloid leukemia in first complete
remission. Blood Adv. 3:1826–1836. 2019.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Ghosh N, Karmali R, Rocha V, Ahn KW,
DiGilio A, Hari PN, Bachanova V, Bacher U, Dahi P, de Lima M, et
al: Reduced-Intensity transplantation for lymphomas using
haploidentical related donors versus HLA-Matched Sibling Donors: A
center for international blood and marrow transplant research
analysis. J Clin Oncol. 34:3141–3149. 2016.PubMed/NCBI View Article : Google Scholar
|