Introduction
Beginning in December 2022, China entered a new
phase of COVID-19 control policy, with a rapid increase in infected
and critically ill patients. The signs and symptoms of COVID-19
infection include fever, cough, and dyspnoea. COVID-19 can cause
acute respiratory distress syndrome (ARDS); therefore, prompt
non-invasive or invasive ventilation, including intermittent
mandatory ventilation, and prompt improvement of hypoxemia are
vital for improving patient conditions (1).
Acute respiratory distress is life-threatening to
patients. Notably, there are various causes of acute respiratory
distress, such as pulmonary infection or laryngeal edema. Once
acute respiratory distress occurs, prompt initiation of treatment
is essential upon the onset to ensure patient survival (2). One of the most important measures is
to restore air exchange, improve the ventilation status of the
patient and maintain normal blood oxygen saturation (3). Therefore, professional knowledge and
practical experience are needed to address these issues to ensure
patient safety. However, in some cases, medical staff may be faced
with resource-poor conditions and must make use of what is
available. The present study describes two cases of first aid with
a shortage of supplies. The medical staff designed a custom-made
high-flow oxygen nebulization device, which was designed to
increase blood oxygen.
Case report
Case presentation 1
In January 2023, a 95-year-old man (weight, 54 kg)
was admitted to the Department of Infectious Diseases (The First
Affiliated Hospital of Anhui Medical University, Hefei, China) due
to pneumonia. The results of a physical examination at admission
included a temperature of 38.4˚C (normal range, 36-37˚C of axillary
temperature), a pulse of 90 bpm (normal range, 60-100 bpm), a
respiratory rate of 20 breaths/min (normal range, 12-20
breaths/min) and a blood pressure of 128/65 mmHg (normal range,
90-140/60-90 mmHg). The nucleic acid test for SARS-Cov-2 was
positive after admission. The white blood cell count was
2.9x109/l, the percentage of neutrophils was 84.8%, the
percentage of lymphocytes was 9.3%, the absolute value of
lymphocytes was 0.27x109/l, the C-reactive protein level
was 69.8 mg/l and the hemoglobin level was 119 g/l. The initial
computed tomography scan (Fig. 1)
showed bilateral pulmonary pneumonia. The diagnoses at admission
were pneumonia and coronary atherosclerotic heart disease. The
blood oxygen saturation was maintained at 86-92% with a 7 l/min
high-flow mask providing centrally supplied oxygen. The partial
pressures of carbon dioxide and oxygen were monitored using a
transcutaneous partial pressure oxygen/carbon dioxide monitor (TCM
CombiM; Radiometre Medical) on the left forearm (4,5).
Patient transfer to the intensive care unit was not possible owing
to the limited number of beds.
After 3 days in the hospital, the blood oxygen
saturation of the patient was 88% and the oxygen flow rate was 7
l/min. The transcutaneous partial pressure of carbon dioxide
(TcPCO2) was 33 mmHg (normal range, 35-45 mmHg) and the
transcutaneous oxygen pressure (TcPO2) was 47 mmHg
(normal range, 60-100 mmHg). As the patient exited their bed to
urinate while using an oxygen mask, physical exertion and oxygen
consumption occurred, leading to a rapid decline in oxygen levels
and the onset of severe respiratory distress. The oxygen saturation
decreased to 78%, and the patient was short of breath and
irritable. The oxygen flow rate was increased to 10 l/min and the
oxygen saturation rate was increased to 83%. The TCM CombiM monitor
showed a partial pressure of carbon dioxide of 27 mmHg and a
partial pressure of oxygen of 35 mmHg. The use of a custom-made
high-flow rate oxygen nebulization device was subsequently
implemented.
The pressure safety valve of a sterile adult bag
valve mask (BVM; ShineBall Enterprise) was removed (Fig. 2A) and the outer diameter of the
mask was wrapped with adhesive tape (Fig. 2B). A nebulizer (Emedical)
containing nebulization solution that could provide relief from
symptoms and promote better respiratory function was connected to
the BVM (Fig. 2C), and the
duckbill valve outlet was connected to a catheter mount connected
to a mask (Fig. 2D). Two breathing
tubes were connected to the nebulizer and the inlet of the BVM
(Fig. 2E). Oxygen was used to
drive the nebulizer at an oxygen flow rate of 7 l/min. Similarly,
in the BVM, wall-based central oxygen was used to regulate the flow
of oxygen to 7 l/min. Head straps were used to fix the mask to the
mouth and nose of the patient. After 5 min, the blood oxygen
saturation gradually increased from 83 to 97%. The patient was
conscious and oriented, and their shortness of breath improved
slightly. The TCM CombiM monitor showed a partial pressure of
carbon dioxide of 36 mmHg and a partial pressure of oxygen of 87
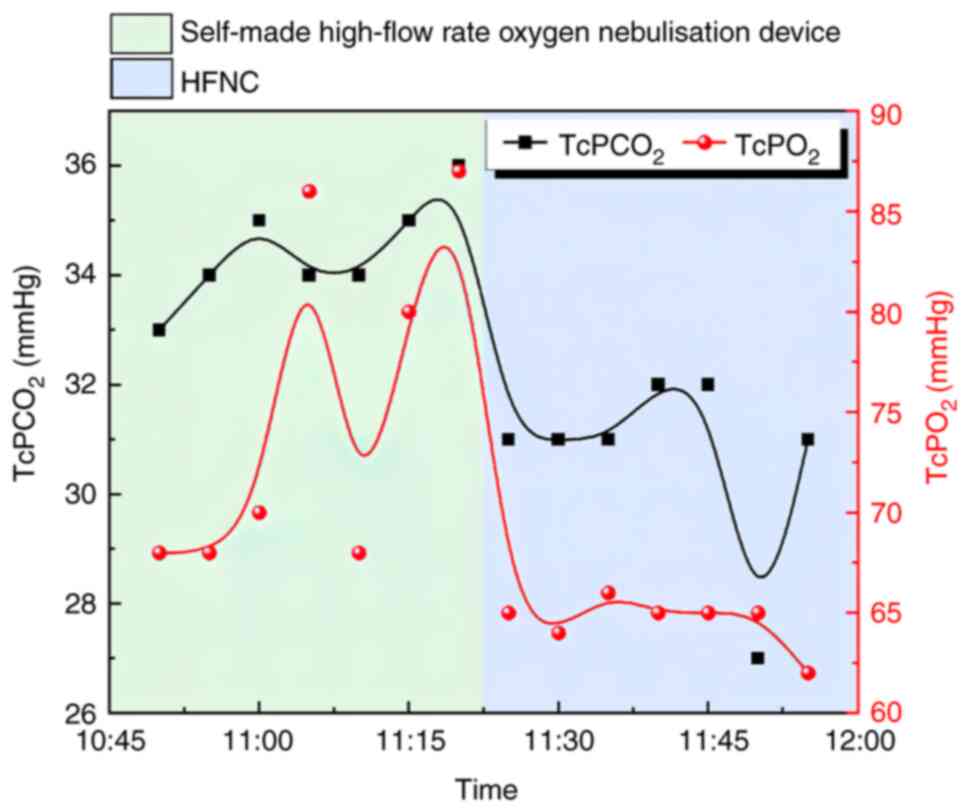
mmHg. After 4 h, a high-flow nasal cannula (HFNC) was applied, and
the parameters were as follows: Oxygen flow rate, 45 l/min; oxygen
concentration, 49%; temperature, 36˚C; pulse oximetry oxygen
saturation, 92%; TcPCO2, 31 mmHg; and TcPO2,
65 mmHg. There was a slight decrease in oxygen saturation in the
early stages of using HFNC, as the patient experienced a temporary
discomfort with high flow (Fig.
3). After 2 h, the blood oxygen saturation was maintained at
98%, the transcutaneous partial pressure of carbon dioxide was 34
mmHg and the partial pressure of oxygen was 69 mmHg. The vital
signs of the patient were stable and they slept peacefully.
Case presentation 2
A 58-year-old male patient was admitted to the
Ambulatory Surgery Center (The First Affiliated Hospital of Anhui
Medical University) in May 2023 due to experiencing hoarseness for
1 year. Vocal cord polypectomy under general anesthesia was
performed the next day. After the operation, the patient was
transferred to the recovery room to assist in breathing via an
endotracheal tube. After 25 min, the patient's spontaneous
breathing recovered and the catheter was removed after the patient
regained consciousness. Due to a lack of assessment of muscle
strength during extubation, the extubation was performed under
light anesthesia, leading to laryngospasm. The patient subsequently
exhibited wheezing and labored breathing, and the three concave
sign was obvious. The blood oxygen saturation gradually decreased
to 87%. Oxygen was administered via the same mask on the anesthesia
machine and the patient was sedated via an intravenous injection of
30 mg propofol (6). The blood
oxygen saturation increased to 99% but the laryngeal wheezing did
not improve. Since the department was not equipped with an
anesthetic machine nebulizer (Fig.
4A, special atomizer for the anesthesia machine), the following
procedure was performed: The balloon of the BVM was removed from
the custom-made high-flow nebulizer used in case 1, the duckbill
valve head was inserted into the intake end of the anesthesia
machine, and 2 ml budesonide suspension was added into the
nebulizer for atomization to reduce airway edema and inflammation
(Fig. 4B) (7). After 5 min, the laryngeal sounds
completely disappeared and the treatment effect was
satisfactory.
Discussion
In the present case report, a custom-made
high-flow-rate oxygen nebulization device was able to supply
high-flow oxygen therapy and airway humidification, and may be used
to provide respiratory support for patients to maintain blood
oxygen saturation and ensure safety while they are waiting for
respiratory equipment.
Before emergency intervention, the first patient
mentioned used a standard oxygen mask with a flow rate of 7 l/min,
and their blood oxygen saturation was maintained at 86-92%. When
there was a change in their condition, the flow rate was increased
to 10 l/min, but the blood oxygen saturation was maintained at only
83%. The use of an oxygen mask failed to sustain a normal oxygen
saturation level in the patient. In the context of limited medical
resources at that time, the custom-made device, equipped with an
oxygen reservoir bag, features two oxygen supply channels, each
with a flow rate of 7 l/min; this allows for the provision of
oxygen support at a combined flow rate of 14 l/min, which can
provide 100% oxygen concentration (8). The patient in case one experienced a
quick recovery of oxygen saturation using this device.
Additionally, a high-flow humidifier is effective at improving
patient blood oxygen saturation. The patient experienced a
temporary drop in blood oxygen saturation, due to the initial
discomfort of the patient with the high flow, there was a slight
decrease in oxygen saturation in the early stages (9). However, after a 2-h adaptation
period, the oxygen saturation reached 98%. Furthermore, the mask of
the custom-made device has gaps on both sides of the cheeks in
order to prevent suffocation, while continuous dynamic monitoring
of TcPO2 and TcPCO2 is conducted using a TCM
CombiM monitor. The patient did not experience complications within
the 4-h usage period.
In addition, the custom-made device can be used for
simultaneous nebulization, as indicated in the second patient, and
it did not cause hypoxia or interfere with positive pressure
ventilation. As in the case of assisting positive pressure
ventilation with a simple breathing bag during assisted positive
pressure ventilation, oxygen and nebulized particles enter the
patient's airway through the oxygen outlet. Additionally, the
device's duckbill valve, along with appropriately applied sterile
tape, ensures a secure seal without causing air leakage.
In conclusion, the custom-made device described in
the present study can be used as a temporary anesthesia machine for
nebulization of patients with acute laryngeal oedema or
laryngospasm, or in airway surface anesthesia in resource-poor
settings. The materials for this device are easy to obtain, and
adult or pediatric BVMs can be used until respirators become
available in resource-poor settings. Hence, this approach is worth
promoting in clinical practice.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
TW and YH are co-first authors of this paper, they
collected and analyzed the data, and drafted the manuscript. YY and
BM collated and analyzed the data, TW and SC confirm the
authenticity of all the raw data. XL and YL analyzed and
interpreted the data. SC designed the study, is the corresponding
author of this paper and revised the final manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Both patients' families consented to participate in
the treatment using the custom-made device.
Patient consent for publication
Both patients and their families provided written
consent for this report, including the figures, to be
published.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lavorini F, Usmani OS and Dhand R: Aerosol
delivery systems for treating obstructive airway diseases during
the SARS-CoV-2 pandemic. Intern Emerg Med. 16:2035–2039.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Saguil A and Fargo M: Acute respiratory
distress syndrome: Diagnosis management. Am Fam Physician.
85:352–358. 2012.PubMed/NCBI
|
|
3
|
Rutt AL, Bojaxhi E and Torp KD: Management
of refractory laryngospasm. J Voice. 35:633–635. 2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zhu XW, Shi Y, Shi LP, Liu L, Xue J and
Ramanathan R: NHFOV Study Group. Non-invasive high-frequency
oscillatory ventilation versus nasal continuous positive airway
pressure in preterm infants with respiratory distress syndrome:
Study protocol for a multi-center prospective randomized controlled
trial. Trials. 19(319)2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Janssens JP, Borel JC, Pépin JL and
SomnoNIV Group: Nocturnal monitoring of home non-invasive
ventilation: The contribution of simple tools such as pulse
oximetry, capnography, built-in ventilator software and autonomic
markers of sleep fragmentation. Thorax. 66:438–445. 2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Afshan G, Chohan U, Qamar-Ul-Hoda M and
Kamal RS: Is there a role of a small dose of propofol in the
treatment of laryngeal spasm? Paediatr Anaesth. 12:625–628.
2002.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Huang C, Yang M and Jiang R: The effect of
premedication with budesonide aerosol inhalation on the incidence
of respiratory adverse events during anesthesia recovery period in
pediatric patients. Bio Res. 29:437–441. 2018.
|
|
8
|
Kabak M and Çil B: Feasibility of
non-rebreather masks and nasal cannula as a substitute for high
flow nasal oxygen in patients with severe COVID-19 infection. Acta
Medica Mediterr. 37:949–954. 2021.
|
|
9
|
Chanques G, Constantin JM, Sauter M, Jung
B, Sebbane M, Verzilli D, Lefrant JY and Jaber S: Discomfort
associated with underhumidified high-flow oxygen therapy in
critically ill patients. Intensive Care Med. 35:996–1003.
2009.PubMed/NCBI View Article : Google Scholar
|