Introduction
Sinus of Valsalva aneurysm is a rare congenital
cardiovascular malformation, accounting for 0.1-3.5% of congenital
heart disease cases (1). Previous
studies have revealed that 40-70% of patients develop a ruptured
sinus of Valsalva aneurysm (RSVA), which frequently results in a
large left-to-right shunt from the aorta to the cardiac level and
may cause heart failure or sudden mortality (2). According to a previous study, RSVA
was more likely to involve the right coronary sinus (RCS) (70%) and
the non-coronary sinus (NCS; 29%) and less than 1% involved the
left coronary sinus (3). Surgery
used to be the primary treatment for RSVA. However, surgical
procedures may result in a high incidence of aortic regurgitation
and residual leakage due to invasive injury to the sinus of
Valsalva (4). Therefore, Cullen
et al (5) first conducted
transcatheter closure (TCC) of RSVA in 1994, and with the
improvement of interventional techniques and the advances in
interventional devices, there have been an increasing number of
reports on the TCC of RSVA globally (6). Currently, as far as we know, there is
not a specialized occluder for RSVA and the majority of
interventional therapies use the Amplatzer ventricular septal
defect (VSD) or patent ductus arteriosus (PDA) occluders (7-9).
Domestic symmetrical VSD devices are widely used due to their light
weight, complete occlusion and low incidence of severe
atrioventricular block. However, it is rarely reported for the
treatment of RSVA (10). Since
2012, symmetrical VSD closure has been used to treat RSVA through
catheterization at Xijing Hospital (Xi'an, China), and
determination of immediate results and 12-month follow-ups after
treatment were conducted to evaluate its safety and
effectiveness.
Patients and methods
Research subjects
This retrospective study was approved by the ethics
committee of Xijing Hospital, Air Force Medical University (Xi'an,
China; approval no. KY20172078-C-1) and was undertaken in
compliance with the tenets of the Declaration of Helsinki and its
later amendments for research on human subjects. All participants
provided their written informed consent to participate in the
present study. A review of the patients' medical records was
performed and patients aged 18 years or older and had an RSVA
confirmed using thoracic echocardiography were included in the
present study. The exclusion criteria were as follows: RSVA outlet
>8 mm or with aortic regurgitation, hemodynamic instability,
severe pulmonary hypertension due to RSVA, associated with active
infective endocarditis, severe liver and kidney dysfunction and
coagulation dysfunction. Percutaneous intervention was performed
after obtaining written informed consent for the procedure. The
final dataset included 14 consecutive patients treated at Xijing
Hospital (Xi'an, China) between January 2012 and March 2022.
Operation methods and procedures
All patients underwent clinical examination,
including a chest X-ray, electrocardiogram and transthoracic
echocardiography (TTE) with color Doppler interrogation. The
diameter of the inner and outer orifices and blood flow velocity of
RSVA were measured by transthoracic ultrasound at the aortic
terminal and rupture site. Huayi symmetrical VSD device (Beijing
Huayishengjie Technology Co., Ltd; http://www.starwaymedical.com) and Memory VSD device
(Shanghai Shape Memory Co., Ltd.; http://www.shsma.com) were used because these two
types of occluders are widely used in the treatment of ventricular
septal deficiency in China. All patients received 4 mg/kg aspirin
one day prior to the operation. The procedure was conducted under
local anesthesia. The femoral vein and artery were accessed.
Intravenous heparin (100 IU/kg) and cefazolin were administered.
RSVA was measured at its aortic and rupture site with both TTE and
angiography. The following steps were then performed: i) A femoral
artery-ascending aorta - aortic sinus aneurysm rupture-femoral vein
track was established, and a 9-10 F sheath tube was placed along
the medial femoral vein of the track; ii) VSD occluders 4-6 mm
larger than the rupture site diameter of the RSVA, were generally
selected, and the occluders were placed in the RSVA under the
guidance of echocardiography; and iii) echocardiography and
aortography were performed again to observe the closure effect and
function of the aortic valve. After the sealing effect was
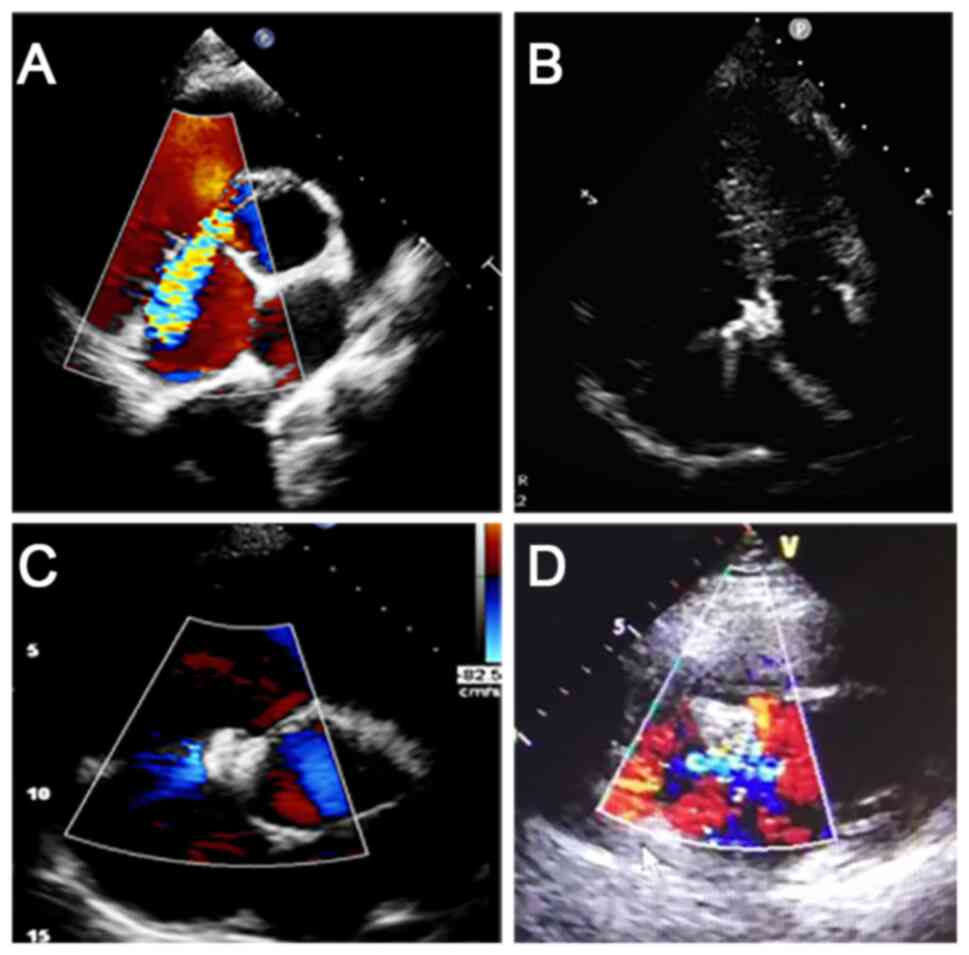
confirmed, the occluder was released. A total of eight Memory and
six Huayi muscular VSD occluders were applied. Representative
examples for Memory devices are provided in Fig. 1.
Follow-up procedure
After TCC, aspirin 4 mg/kg was used to prevent
platelet aggregation for 6 months. Electrocardiogram and TTE were
performed on the first day after closure. Echocardiography was then
performed regularly 1, 6 and 12 months after the procedure
(Fig. 2).
Statistical analysis
Statistical analysis was conducted using SPSS
(version 19.0; IBM Corp.) software. Repeated-measures ANOVA
followed by the Bonferroni test was used for the two sets of heart
size data. An independent-samples unpaired t-test was used to
compare operation time between the two groups. P<0.05 was
considered to indicate a statistically significant difference.
Results
General characteristics of
patients
A total of 14 patients were included in the present
study, comprising 10 males and 4 females, with an age range of
24-66 years (mean, 38±13 years). Among them, 10 patients (71.4%)
had an NCS rupture into the right atrium (RA), 3 patients (21.4%)
had an RCS rupture into the RA and 1 patient (7.2%) had an RCS
rupture into the right ventricle (RV). Furthermore, 1 patient had
atrial fibrillation, 1 patient had patent foramen ovale (PFO) and
VSD, and 1 patient had VSD. The mean diameter of the defect at the
aortic end was 8.56±1.63 mm (median, 9.00 mm) and the mean diameter
at the rupture site measured 5.06±1.18 mm (median, 5.00 mm). The
mean procedure time was 61±17 min. All patients completed a
12-month follow-up. The patient characteristics were summarized in
Table I.
 | Table IClinical, echocardiographic and
baseline variables, procedural variables, and immediate and
mid-term outcomes. |
Table I
Clinical, echocardiographic and
baseline variables, procedural variables, and immediate and
mid-term outcomes.
| Case no. | Age, years/sex | NYHA class | Associated
diseases | Defect location | Defect size by ECHO,
inner/outer opening, mm | Closure device size,
mm | Device supplier | Operation time,
min | Residual shunt at
discharge/follow-up | AR at discharge/
follow-up | NYHA class at
follow-up |
|---|
| 1 | 24/M | II | None | NCS to RA | 9/5 | VSD16 | Memory | 70 | Middle/none | Small/small | I |
| 2 | 50/M | II | VSD | NCS to RA | 8/4 | VSD12 | Memory | 55 | None/none | Small/small | I |
| 3 | 28/F | III | None | NCS to RA | 10/7 | VSD16 | Huayi | 60 | None/none | None/small | I |
| 4 | 27/F | III | None | NCS to RA | 8.7/5.7 | VSD14 | Memory | 90 | None/none | None/none | I |
| 5 | 43/M | IV | AF | NCS to RA | 9/4.5 | VSD16 | Huayi | 85 | None/none | None/small | II |
| 6 | 40/M | II | HTN | NCS to RA | 7/4 | VSD12 | Memory | 40 | None/none | Small/none | I |
| 7 | 35/M | III | None | NCS to RA | 10/4.4 | VSD16 | Memory | 30 | None/none | None/none | I |
| 8 | 48/M | II | None | NCS to RA | 10/4.6 | VSD16 | Memory | 50 | None/none | Middle/small | I |
| 9 | 66/F | II | PFO, VSD | NCS to RV | 5/3 | VSD14 | Memory | 75 | None/none | None/small to
middle | I |
| 10 | 48/F | III | None | RCS to RA | 7.2 | VSD10 | Memory | 65 | None/none | None/small | I |
| 11 | 51/M | II | None | RCS to RA | 10/7 | VSD16 | Huayi | 45 | None/none | None/small | I |
| 12 | 23/M | II | None | RCS to RA | 7/5.6 | VSD16 | Huayi | 80 | None/none | None/none | I |
| 13 | 23/M | II | None | NCS to RA | 8/5 | VSD14 | Huayi | 60 | None/none | None/none | I |
| 14 | 31/M | II | PFO | NCS to RA | 11/6 | VSD16 | Huayi | 45 | None/none | None/none | I |
Deployment success and
complications
All 14 patients were successfully treated with the
domestic symmetrical VSD closure. All of the patients were
implanted once, and after the procedure, there were no instances of
device displacement, the device falling off, device thrombosis or
ineffective endocarditis. Furthermore, the dyspnea of the patients
was reduced, edema disappeared and the grade of the NYHA class was
improved.
Hemolysis and hemoglobinuria occurred in 1 patient
(case 1) 5 h after intervention and a moderate residual shunt was
revealed using thoracic echocardiography. Therefore, dexamethasone
10 mg was administered along with rehydration and alkaline
urination, and the patient recovered on day 10 after conservative
treatment. In the present study, 1 patient (case 5) was transferred
to surgery for aortic regurgitation 1 year after the initial
treatment of RSVA. A total of 5 patients developed
procedure-related aortic regurgitation.
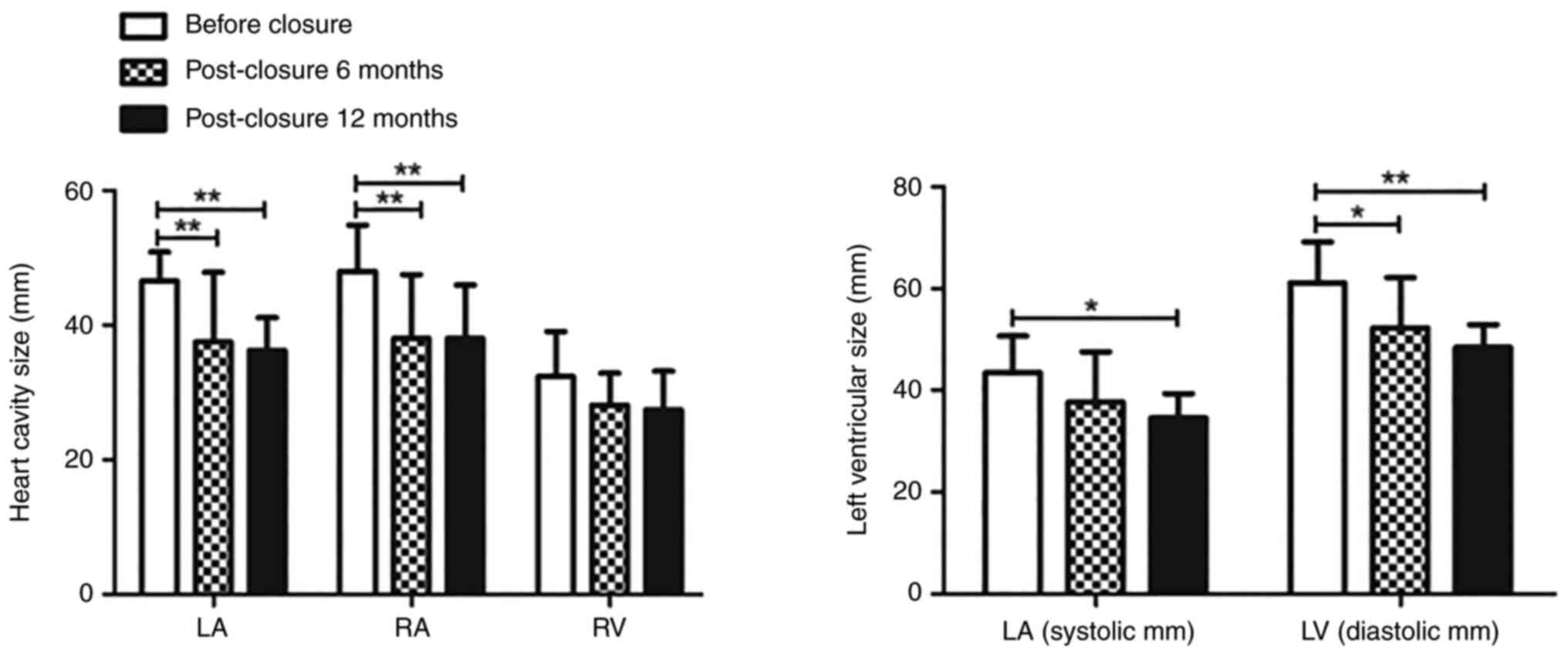
Heart cavity after closure
The results illustrated that the left atrium, RA, LV
(systolic) and LV (diastolic) were significantly reduced 6 and 12
months after the operation compared with that before the TCC
(F=5.66, P=0.02; F=17.80, P<0.001; F=6.72, P=0.01; F=8.95,
P<0.001; respectively). There was no statistically significant
difference in the RV change 6 and 12 months after the operation
compared with that before the TCC (Table II and Fig. 3).
| Table IIHeart cavity after closure. |
Table II
Heart cavity after closure.
| Heart cavity | Before closure | Post-closure 6
months | Post-closure 12
months | F-value | P-value |
|---|
| LA, mm | 46.57±4.31 | 37.53±10.36 | 36.28±4.86 | 5.66 | 0.02 |
| RA, mm | 48.00±6.88 | 38.00±9.55 | 38.00±7.98 | 17.80 | <0.001 |
| RV, mm | 32.36±6.73 | 28.15±4.72 | 27.43±5.74 | 1.44 | 0.27 |
| Systolic LV,
mm | 43.50±7.23 | 37.70±9.86 | 34.57±4.79 | 6.72 | 0.01 |
| Diastolic LV,
mm | 61.07±8.12 | 52.31±9.84 | 48.43±4.50 | 8.95 | <0.001 |
Effects of the two types of
devices
In the present study, two domestic symmetrical VSD
devices were used and there were no significant differences in the
operation time (F=0.31; P=0.76) (Table III).
| Table IIIEffect comparison of the two types of
device. |
Table III
Effect comparison of the two types of
device.
| Device
supplier | Number of times
used in operation | Operation time,
min | Residual shunt | Aortic
regurgitation | F-value | P-value |
|---|
| Memory | 8 | 59±20 | 1 | 2 | 0.31 | 0.76 |
| Huayi | 6 | 63±17 | 0 | 3 | | |
Concomitant congenital heart
disease
In the present study, there were 2 cases with VSD.
Due to the defect being small (1.3 mm), 1 case was not treated. In
the other case, the patient had PFO and VSD, and the sinus aneurysm
of the aorta ruptured into the right ventricle; therefore, the VSD
occluder blocked both the rupture and the VSD. Angiography revealed
the disappearance of residual shunt and auscultation of cardiac
murmur. Echocardiographic re-examination revealed that the position
of the occluder was normaland no residual shunt was revealed in the
VSD.
Discussion
RSVA is mainly caused by congenital dysplasia of
elastic fibers in the middle of the aortic root and is more common
in males compared with females (ratio, ~4:1) (11). Aortic sinus aneurysm mainly
involves the RCS (~70%), followed by the NCS (~29%) and rarely
involves the left coronary sinus (3). The occurrence of these aneurysms may
be secondary due to events and conditions (including trauma,
bacterial endocarditis, syphilis, cystic medial necrosis and
atherosclerosis) that weaken the juncture between the media and the
annulus fibrosus of the aorta (12). Most frequently, it is congenital in
origin (13) due to either a
congenital absence of continuity between the aortic media and the
annulus fibrosis, or a developmental structural defect in the
aortic annulus itself, which may gradually give way under aortic
pressure to form an aneurysm. Aortic sinus aneurysm may rupture
into the RA, RV, pulmonary artery, left ventricle or pericardial
cavity, and usually manifest as a sudden chest pain or acute heart
failure (14). The disease process
of either ruptured or non-ruptured supraventricular arrhythmias
(SVAs) is difficult to determine due to the rarity of these
lesions. Adams et al (15)
revealed that the mean survival of patients with untreated ruptured
SVA was 3.9 years. Therefore, early intervention is required in
these patients (16).
Since 1994, when Cullen et al first carried
out transcatheter intervention to block RSVA, transcatheter closure
has been widely applied for its clinical advantages and economic
benefits (5,17). However, due to the low incidence of
aortic sinus aneurysm, there is no specialized device to block
RSVA. According to related reports, the Amplatzer occluder has been
the most widely used device in the world (7-9).
There are few studies on the device made in China to treat RSVA.
Chen et al (2) evaluated
the safety and effectiveness of a domestic small lumbar VSD closure
device for the treatment of ruptured aneurysm of valsalva sinus
(RSVA). From 2005 to 2010, Chen et al (2) treated 7 patients with RSVAusing a
domestic small lumbar VSD device, and during the 12-month
follow-up, there were no cases of hemolysis, arrhythmia, device
embolism, infective endocarditis, heart failure or mortality. This
demonstrates that the domestic small lumbar VSD device was safe and
effective as a therapy for RSVA Xiao et al (18) retrospectively analyzed 35 patients
after treatment of RSVA using a domestic small lumbar VSD occluder
and PDA device. The study revealed that 1 patient developed severe
obstructive aortic insufficiency and 2 cases failed. However, 32 of
the patients successfully completed transcatheter closure, and
there were no cases of infective endocarditis, residual shunt,
thrombosis, device displacement, severe aortic regurgitation,
severe arrhythmia or mortality after an average follow-up of 73.5
months (18).
The symmetrical VSD occluder is a device developed
in China. It is made of superelastic nickel-titanium alloy wire and
has a self-expanding double-disc structure with a connection in the
middle. The middle part, which is called the waist, is also made of
nickel-titanium alloy. The diameter of both sides of the plates is
the same and the waist height is 2.5-4 mm. The new domestic Nitinol
VSD blocker has the advantages of being easily operated and
recyclable, a reliable curative effect and low cost, which has
resulted in it being rapidly popularized and applied in clinical
practice. Animal experiments have demonstrated that with the memory
VSD occluder, endothelialization began on the 7th day after
implantation, and endothelialization was completed on the 30th day
after the operation, which is superior to the VSD occluder that has
been marketed (19). Clinical
studies have indicated that the memory VSD occluder may be used for
membranous or muscular ventricular septal defects (20,21).
Furthermore, a multi-center clinical study demonstrated that the
incidence of complete atrioventricular block is significantly
reduced (20,22). However, as far as we know, it is
rarely reported for the treatment of RSVA.
The present study reported the effect of a domestic
made symmetrical occluder treatment RSVA for the first time. All of
the 14 patients were successfully treated with the closure and
immediate results indicated that the heart function of the patients
improved, dyspnea was alleviated and motor capacity increased. At
the 12-month follow-up, it was revealed that there were no cases of
infective endocarditis, device thrombosis, severe aortic
regurgitation, severe arrhythmia or mortality, with the exception
that 1 patient underwent surgery 1 year after initial RSVA
treatment. These results demonstrated that domestic symmetrical
occluders were safe and effective in the treatment of RSVA. Two
types of devices were used in the present study. There was no
significant difference in the therapeutic effect and safety between
the two types of occluder.
The RSVA is similar to PDA in morphology, but the
structure of RSVA is different from PDA. PDA is muscular fibrous
tissue with a strong supporting force. The muscular layer of aortic
sinus aneurysms has degenerated and lacks supporting force
(13), so the PDA occluder is not
selected for occlusion. However, PDA occluders have also been
reported to treat RSVA (23).
Therefore, more clinical trials are required to determine which
occluders are more effective.
Aneurysms of the sinus of Valsalva are rare, and
thus, the number of treatment options are limited. At present,
there are no consensus guidelines for transcatheter closure. The
present study hypothesized that the successful operations were due
to the size and location of the RSVA. The majority of cases that
failed were due to large defects. Previous studies suggested that
the defects of RSVA <10 mm are more likely to be closed using
TCC, while surgery is preferred for defects >10 mm. According to
the literature, the biggest defect of RSVA via TCC was 17 mm and
the largest occluder was 22 mm (24). The occluder selected is generally
2-4 mm larger compared with the defect. The second factor that
affected intervention was the relationship between the device and
the surrounding tissue. The most common complications after
occlusion were aortic regurgitation and residual shunt, and often
due to these complications, a number of patients had to transfer to
surgery.
The RSVA has been frequently associated with other
congenital heart diseases, such as VSD or atrial septal defect
(ASD). In the past, surgery was the first choice for these cases. A
number of studies have attempted to plug both RSVA and VSD using a
catheter. The study by Mahimarangariah et al (25) reported on a 14-year-old male
patient with RSVA and VSD, in whom the RSVA and VSD was closed
using TCC at the same time. Mehta et al (26) illustrated a case of RSVA with ASD.
After transcatheter closure of the RSVA, echocardiography revealed
that the ASD was smaller compared with the ASD before (from 22 to
18 mm) and 6 months after the ASD was occluded using interventional
closure.
Interventional complications were also the focus of
attention for the present study, mainly to observe the effect of
the occluder on the structures of adjacent tissues such as the
aortic valve, tricuspid valve and coronary arteries. In the present
study, one patient had surgery for severe aortic regurgitation.
Mild aortic regurgitation occurred in 5 patients, but it had no
effect on heart size or function. Whether moderate aortic
regurgitation requires additional surgery may depend primarily on
whether the regurgitation continues to increase, whether cardiac
insufficiency occurs and whether hemodynamics were affected. Kerkar
et al (27) also observed a
similar phenomenon with Amplatzer duct occluder for RSVA.
Of note, the present study had limitations. The
patients were included from a single center, which limits the
generalizability of the results. Therefore, a well-designed
multicenter study with a larger sample size is required. Although
immediate and mid-term effects were demonstrated to be favorable in
the present study, attention should be given to possible residual
shunt as well as aortic regurgitation and the long-term effects
should be observed.
Acknowledgements
Not applicable.
Funding
Funding: The present study was funded by the Key Research and
Development Program of Shaanxi Province (grant no.
2017ZDXM-SF-049).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HL and WC confirm the authenticity of all the raw
data. HL and TL contributed to the conception and design of the
study. WC completed the implementation of the study and drafted the
manuscript and revised it critically for important intellectual
content. WC and XL completed the collection, analysis and
interpretation of data. HL and TL agreed to be accountable for all
aspects of the work and ensured that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved. All authors have read and approved the
final manuscript.
Ethics approval and consent to
participate
The Ethics committee of Xijing Hospital (Xi'an,
China) approved the study (approval no. KY20172078-C-1). All
participants provided their written informed consent to participate
in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Goldberg N and Krasnow N: Sinus of
Valsalva aneurysms. Clin Cardiol. 13:831–836. 1990.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Chen SP, Bai Y, Zhao XX and Qin YW: Safety
and efficacy of a domestic made small-waist ventricular septal
defect occluder for transcatheter closure of ruptured aneurysm of
the sinus of Valsalva. Zhonghua Xin Xue Guan Bing Za Zhi.
40:298–301. 2012.PubMed/NCBI(In Chinese).
|
|
3
|
Sakakibara S and Konno S: Congenital
aneurysm of the sinus of Valsalva. Anatomy and classification. Am
Heart J. 63:405–424. 1962.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Murashita T, Kubota T, Kamikubo Y, Shiiya
N and Yasuda K: Long-term results of aortic valve regurgitation
after repair of ruptured sinus of valsalva aneurysm. Ann Thorac
Surg. 73:1466–1471. 2002.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Cullen S, Somerville J and Redington A:
Transcatheter closure of a ruptured aneurysm of the sinus of
Valsalva. Br Heart J. 71:479–480. 1994.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Mao Y, Wang C, Li Y, Guan X, Zhang X and
Wu X: Percutaneous closure versus surgical repair for ruptured
sinus of valsalva aneurysm: A systematic review and meta-analysis.
Front Cardiovasc Med. 10(1158906)2023.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kerkar P, Suvarna T, Burkule N and Panda
R: Transcatheter closure of ruptured sinus of Valsalva aneurysm
using the Amplatzer duct occluder in a critically ill post-CABG
patient. J Invasive Cardiol. 19:E169–E171. 2007.PubMed/NCBI
|
|
8
|
Szkutnik M, Kusa J, Glowacki J, Fiszer R
and Bialkowski J: Transcatheter closure of ruptured sinus of
valsalva aneurysms with an Amplatzer occluder. Rev Esp Cardiol.
62:1317–1321. 2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Agrawal G, Agarwal M and Chintala K:
Transcatheter closure of ruptured sinus of Valsalva aneurysm in a
pregnant woman. J Cardiol Cases. 12:183–187. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Liu S, Xu X, Zhao X, Chen F, Bai Y, Li W,
Zhang Y, Wang C, Xiang J, Wu G, et al: Percutaneous closure of
ruptured sinus of Valsalva aneurysm: Results from a multicentre
experience. EuroIntervention. 10:505–512. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Henze A, Huttunen H and Bjork VO: Ruptured
sinus of valsalva aneurysms. Scand J Thorac Cardiovasc Surg.
17:249–253. 1983.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Sarikaya S, Adademir T, Elibol A,
Buyukbayrak F, Onk A and Kirali K: Surgery for ruptured sinus of
Valsalva aneurysm: 25-year experience with 55 patients. Eur J
Cardiothorac Surg. 43:591–596. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ott DA: Aneurysm of the sinus of valsalva.
Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 165–176.
2006.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kumar GA, Parimala PS, Jayaranganath M and
Jagadeesh AM: Three-dimensional transesophageal
echocardiography-guided transcathetar closure of ruptured
noncoronary sinus of valsalva aneurysm. Ann Card Anaesth.
20(Suppl):S73–S75. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Adams JE, Sawyers JL and Scott HW Jr:
Surgical treatment of aneurysms of the aortic sinuses with
aorticoatrial fistula; experimental and clinical study. Surgery.
41:26–42. 1957.PubMed/NCBI
|
|
16
|
Sawyers JL, Adams JE and Scott HW Jr: A
method of surgical repair for ruptured aortic sinus aneurysms with
aorticoatrial fistula. South Med J. 50:1075–1078. 1957.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Liu S, Xu X, Ding X, Liu G, Zhao Z, Zhao X
and Qin Y: Comparison of immediate results and mid-term follow-up
of surgical and percutaneous closure of ruptured sinus of Valsalva
aneurysm. J Cardiol. 63:239–243. 2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Xiao JW, Niu MN, Wang QG, Zhang DZ, Han
XM, Zhang P, Cui CS and Zhu XY: Safety and efficacy of
transcatheter closure of ruptured sinus of Valsalva aneurysm.
Zhonghua Xin Xue Guan Bing Za Zhi. 46:799–803. 2018.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
19
|
Zhou Y, Chen F, Huang X, Zhao X, Wu H, Bai
Y and Qin Y: A new coated nitinol occluder for transcatheter
closure of ventricular septal defects in a canine model. Biomed Res
Int. 2013(507919)2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Chen F, Li P, Liu S, Du H, Zhang B, Jin X,
Zheng X, Wu H, Chen S, Han L, et al: Transcatheter closure of
intracristal ventricular septal defect with mild aortic cusp
prolapse using zero eccentricity ventricular septal defect
occluder. Circ J. 79:2162–2168. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Zhu D, Tao K, An Q, Luo S, Gan C and Lin
K: Perventricular device closure of residual muscular ventricular
septal defects after repair of complex congenital heart defects in
pediatric patients. Tex Heart Inst J. 40:534–540. 2013.PubMed/NCBI
|
|
22
|
Zhou D, Pan W, Guan L and Ge J:
Transcatheter closure of perimembranous and intracristal
ventricular septal defects with the SHSMA occluder. Catheter
Cardiovasc Interv. 79:666–674. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Guan L, Zhou D, Zhang F, Pan W, Dong L,
Chen H and Ge J: Percutaneous device closure of ruptured sinus of
valsalva aneurysm: A preliminary experience. J Invasive Cardiol.
25:492–496. 2013.PubMed/NCBI
|
|
24
|
Sinha SK, Khanna NN, Razi M, Krishna V,
Jha MJ, Mishra V, Aggarwal P, Goel A, Singh K, Thakur R, et al:
Safety and feasibility of transcatheter interruption of ruptured
sinus of valsalva aneurysm using the cocoon duct occluder:
Immediate results and mid-term follow-up. Cardiol Res. 8:154–160.
2017.PubMed/NCBI View
Article : Google Scholar
|
|
25
|
Mahimarangariah J, Kikkeri HS, Rai KM and
Nanjappa MC: Combined transcatheter device closure of ruptured
sinus of valsalva and a post-surgical residual ventricular septal
defect. Catheter Cardiovasc Interv. 82:E803–E808. 2013.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Mehta NK, Mishra N and Kerkar P:
Percutaneous closure of ruptured sinus of valsalva aneurysm and
atrial septal defect. J Invasive Cardiol. 22:E82–E85.
2010.PubMed/NCBI
|
|
27
|
Kerkar PG, Lanjewar CP, Mishra N,
Nyayadhish P and Mammen I: Transcatheter closure of ruptured sinus
of Valsalva aneurysm using the Amplatzer duct occluder: Immediate
results and mid-term follow-up. Eur Heart J. 31:2881–2887.
2010.PubMed/NCBI View Article : Google Scholar
|