Introduction
Among women, breast cancer is the leading cause of
cancer-related mortality and the most common type of cancer
worldwide (1–3). Breast cancer is the second most
common cancer in the world, and its incidence is increasing, with a
total of 1,050,100 cases in 2002 compared to 572,100 in 1980.
Worldwide, the ratio of mortality to incidence is approximately 36%
(1–3). Breast cancer causes 370,000 annual
deaths, representing 13.9% of cancer-related deaths in women. It is
the most prevalent cancer in the world today, with incidence rates
highest in industrialized countries. While researchers are
rigorously searching for the etiology of the disease, a more
sensitive and early detection employing novel biomarkers is
required for breast cancer patients. Presently, there is a growing
enthusiasm for applying proteomic approaches to the identification
of serum biomarkers for the early non-invasive diagnosis of cancer
and the monitoring of tumor progression. In this study, we compared
the sensitivity of the serological level of mutated p53 protein and
the level of anti-p53 antibodies with p53 protein expression in
breast cancer patients.
p53 is a multifunctional transcription factor that
promotes tumor cell death by regulating the expression of genes
involved in cell cycle control and apoptosis, DNA repair and
angiogenesis (4). Mutations or
down-regulation of p53 contribute to cancer development and
progression (4). p53 mutations in
cancer patients are often associated with poor prognosis (4). Mutations in the p53 gene, including
amino acid substitutions, are present in more than 50% of patients
with malignant tumors. These mutations change the conformational
structure of p53, which triggers the inhibition of the DNA repair
mechanisms and induces programmed cell death by apoptosis (5–7). The
accumulation of inactive p53 protein in cells significantly
increases the expression of mutant p53 protein with a longer
half-life (several hours compared to 20 min for wild-type p53).
Therefore, p53 accumulation in tumor tissues is directly related to
the presence of mutation in p53 protein (8,9).
Antibodies to p53 in the sera of cancer patients
have been reported since 1982 (10). However, the reported antibody
frequency in cancer has varied widely, ranging from 2.7 to 31% in
different types of cancers. This is in part due to variations in
the assay systems used (11).
Although the sensitivity of p53 antibodies in diagnosis is not
high, these antibodies are rare in healthy people (12), making anti-p53 antibodies a
dependable marker for cancer.
We previously reported the presence of p53
antibodies in less than 17% of breast cancer patients (13). In the present study, serological
expression of mutant p53 protein was analyzed in 55 cases of human
breast tumors at different stages of progression. The results
revealed that the level of mutant p53 protein in the serum was
directly correlated with p53 protein accumulation in breast tumor
tissues. Serological levels of mutant p53 protein in breast cancer
patients were higher in early-stage and poorly differentiated
tumors. This finding may be important in the detection of breast
cancer at early stages, and may be used as a diagnostic tool for
differentiating benign and malignant breast disease prior to breast
surgery.
Another critical clinical question is whether
anti-p53 antibodies might be used as early markers of incipient
tumors in high risk populations. In the present study, we
demonstrated that the level of anti-p53 antibodies is less
sensitive than mutated p53 protein in serum. Further experiments
are necessary in order to determine whether serological mutant p53
protein may be used as an early marker in breast cancer.
Materials and methods
Patients
Fifty-five patients from Bahía Blanca, Argentina
with mammary pathology were evaluated at local hospitals (Sanatorio
Privado del Sur, Interzonal Dr Jose Penna, Regional Español, Dr
Leonidas Lucero, Hospital de la Asociación Médica). Informed
consent was obtained from each patient prior to enrollment in the
study. Serum and breast tissue from all breast cancer patients were
available for analysis. Serum samples were collected
pre-operatively and stored at −20°C until processing. The median
age of the patients was 55 years (range 28–91 years).
Mutant p53 protein: Serological
analysis
The presence of p53 mutant protein in serum was
quantified employing the p53 ELISA Kit (mutant-selective) from
Oncogene Research Products (Cambridge, MA, USA). Results were
expressed in O.D. units and were categorized as negative or
positive. The ELISA assay was deemed suitable for the quantitative
determination of mutant p53 protein. The specific antibodies
utilized in this assay react with an epitope exclusively expressed
in the recombinant human p53 protein expressed in Escherichia
coli, and are exposed only in human mutant p53 proteins, not in
wild-type p53 forms, making the assay mutant-selective. Eight serum
samples from healthy women without breast disease or a family
history of breast cancer were utilized in the serologic assays as
negative controls.
Anti-p53 antibodies using the ELISA
assay
p53 auto-antibodies were quantified in serum
employing the p53 ELISAPlus (Autoantibody) kit (Oncogene Research
Products). The kit was designed to measure circulating antibodies
to p53 in human serum samples. Control serum provided by the
manufacturer was employed. The results were expressed in O.D. units
and were categorized as negative or positive.
Histology
Human breast tumor sections (5 μm) were cut
from formalin-fixed paraffin-embedded tissues and stained with
H&E for histological evaluation. Nuclear grade was defined as
grades I–III according to previously established criteria (14,15).
Histological classification and the nuclear grade were determined
by a medical pathologist. A duplicate of each tissue was cut in
order to analyze the total expression of p53 protein using
immunohistochemistry (IHC).
Immunohistochemistry
Tumor cell staining for p53 protein was performed
using mouse monoclonal DO-1 antibody (Oncogene Research Products).
All sections were de-paraffinized in xylene, dehydrated through a
graded series of alcohols and washed in phosphate-buffered saline.
This buffer was used for all subsequent washes. IHC using the
streptavidin-biotin-peroxidase method was performed on
paraffin-embedded tissues using the anti-p53 mouse monoclonal
antibody DO-1 (diluted 1:100), which recognizes the N-terminus of
the human p53 protein (amino acids 21–23). In addition, the
antibody reacted with wild-type p53 and with numerous mutant p53
proteins. In order to perform a semi-quantitative assessment, the
IHC results were scored. Nuclear staining in >10% of the tumor
cells was interpreted as positive: +, 10–25%; ++, 25–50%; and +++,
50–100% of nuclear staining.
Statistical analysis
The frequency of p53 values at the cut-off and the
frequency of p53 values below the cut-off was compared to the
different parameters by the χ2 test (t-test).
Results
Age-dependent mutated p53 protein
expression
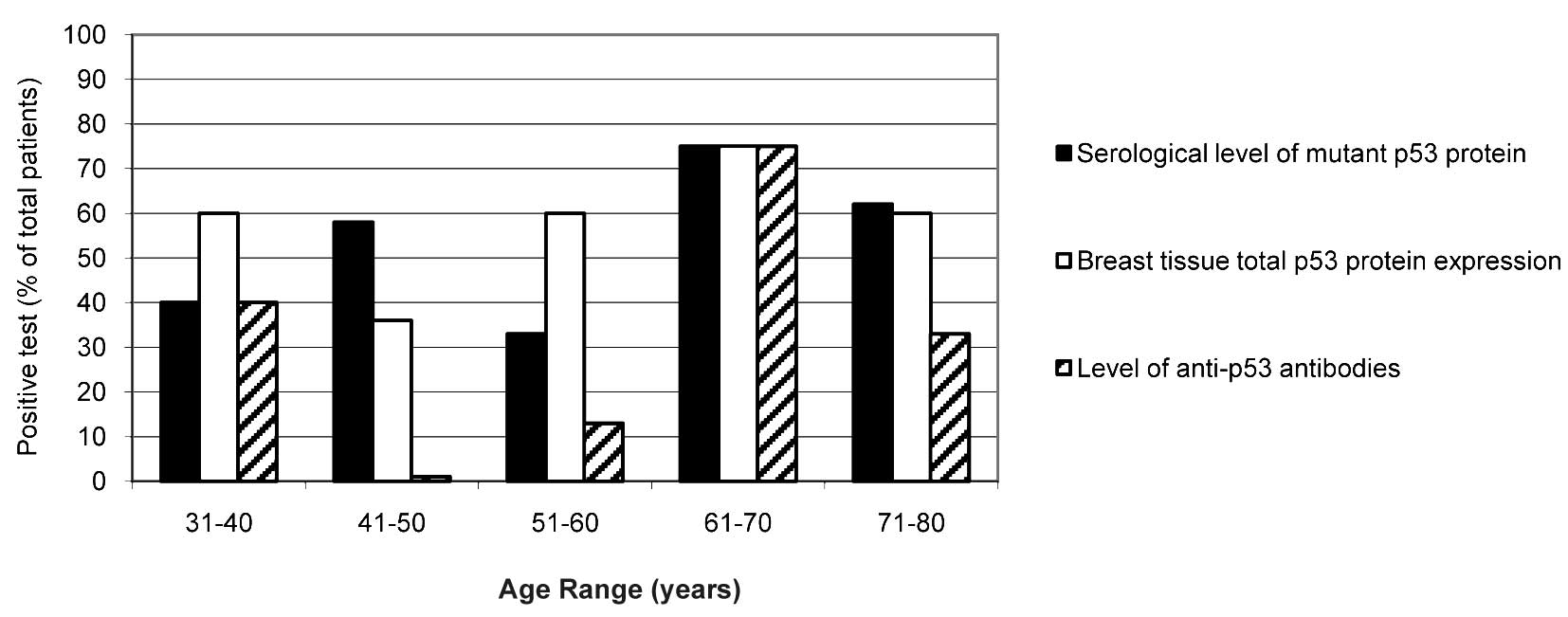
Fig. 1 shows the
ELISA results illustrating the age-dependent correlation of the
serological level of mutant p53 protein (black columns) and
anti-p53 antibodies (hatched columns) in 55 patients with breast
malignancies. The total p53 protein expression in breast tissue
(white columns) determined using IHC is also shown. Mutated p53
protein levels were detected in patients of all ages, but were
highly detected in patients ≥61 years of age (75% positivity at an
age range of 61–70 and 62% at an age range of 71–80 years). A
similar sensitivity (75% at an age range of 61–70 years and 60% at
≥71 years of age) was observed for the total p53 protein expression
in breast tissue by IHC. In addition, the levels of anti-p53
antibodies were higher in patients in the age range of 61–70 years
(75% of positivity). This sensitivity decreased (33%) in patients
≥71 years of age, probably due to immune system depression and the
lower level of antibody synthesis at this age.
Notably, at the age range of 41–50 years, the
sensitivity of mutant protein detection in serum was higher
compared to the total p53 protein expression in breast tissues (58
and 36%, respectively). However, anti-p53 antibodies were
practically not detected at that age range (only 1% of the total
number of patients). It is now important to ascertain why the
immune system did not respond to the increased level of serological
mutant p53 protein. There are several explanations for this
discrepancy, including one which suggests that mutant p53 protein
conformational structures are ‘hidden’ to the immune system, which
does not recognize the foreign epitopes in the new p53 mutated
protein. Further molecular and genetic analysis is necessary to
prove this hypothesis.
In the age range of 51–60 years, the sensitivity of
serological mutant p53 detection was lower in comparison with the
total p53 protein expression in breast tissues (33 and 60%,
respectively). Anti-p53 antibody sensitivity was again low (13%) in
this age range. The ELISA kit for the detection of mutant p53
protein in serum is designed specifically against an epitope
present in the mutant p53 protein, and did not recognize the
wild-type form. However, the antibody employed in the IHC
recognized both forms of p53 protein, mutated and wild-type. This
is likely the reason for the observed higher levels of p53 protein
in breast tissues compared to the level of mutated p53 protein in
serum. The wild-type p53 form has a shorter half-life compared to
the mutated form. It is believed that menopausal breast cancer
patients (51–60 years) have accumulated a higher level of the
wild-type p53 form. In order to demonstrate this hypothesis,
mutational analysis by sequencing of the whole p53 gene and a
correlation of the presence of point mutations with hormonal
changes during the menopausal period must be carried out. Similar
results were observed in patients <40 years of age. In the age
range of 31–40 years, IHC was the most sensitive technique for the
detection of the accumulation of p53 protein, followed by mutant
p53 protein in serum (60 and 40%, respectively). Notably, the
levels of anti-p53 antibodies were high (40%) in this age range.
One possible explanation for this observation is possibly that the
immunological system of patients <40 years of age is more
sensitive to the presence of foreign or mutated proteins, thus
stimulating antibody synthesis, compared to patients >70 years
of age, who are less susceptible.
Histology-dependent curve and p53 protein
expression
Fig. 2 shows the
number of cases (% with respect to the total number of patients)
positive for the presence of mutant p53 protein in serum (black
column) or for total p53 protein expression by IHC (white column)
as well as anti-p53 antibody levels (hatched column) in samples
from 55 patients with different stages of breast carcinoma and in 8
serum samples from healthy women, used as negative controls. In
this study, we analyzed 6 patients with benign disease, 2 patients
with ductal carcinoma in situ (DCIS), 19 patients with
invasive ductal carcinoma (IDC) stage I, 7 patients with IDC stage
II, 17 patients with IDC stage III, 1 patient with phylloides tumor
and 3 patients still undiagnosed at the time of publishing.
In patients with benign disease, mutant p53 protein
was not detected in serum (Fig.
2). Detection of anti-p53 antibodies and p53 protein expression
in breast tissue was also negative in these patients. Total p53
protein expression was detected in 1 of 2 patients with DCIS
(Fig. 2), indicating that 50% of
DCIS patients showed positive expression of p53 by IHC, but none
were positive for the presence of mutant p53 protein in their serum
(Fig. 2). Further analysis
employing a higher number of patients with DCIS is needed to reach
a conclusion concerning the expression of p53 mutations.
Among the breast cancer patients with IDC stage I,
12 of 19 patients (63%) were positive for the mutant p53 protein in
serum. Similar results were obtained from the IHC (11/19, 58% of
patients). However, the presence of anti-p53 antibodies was lower
(6/19, 32% of patients) (Fig. 2).
Among the breast cancer patients with IDC stage II, 5 of 7 patients
(71%) were positive for mutant p53 in serum. The same results were
obtained using IHC (5/7, 71% of patients). Nonetheless, a very low
sensitivity was found for the detection of anti-p53 antibodies
(1/7, 14% of patients). Among breast cancer patients with IDC stage
III, 9 of 17 patients (53%) were positive for mutant p53 protein in
serum, 11 of 17 (65%) were positive for total p53 protein
expression in breast tissues by IHC, and 8 of 17 (47%) exhibited
high levels of anti-p53 antibodies in their serum samples.
The present data clearly demonstrate that mutant p53
protein expression in breast cancer is stage-dependent. Agreement
was found in the results upon comparing the three molecular biology
techniques employed in this study. All techniques detected
mutations in p53 in IDC from stage I to III, but at a different
sensitivity. Anti-p53 antibodies were highest in patients with IDC
stage III; however they were also detected during the early stages
of the disease. These results suggest that serological expression
of mutant p53 protein is a more sensitive technique than anti-p53
antibodies for detecting p53 alterations in breast cancer,
particularly during the early stages of the disease.
Grade of tumor differentiation and
expression of p53 mutations in breast cancer patients
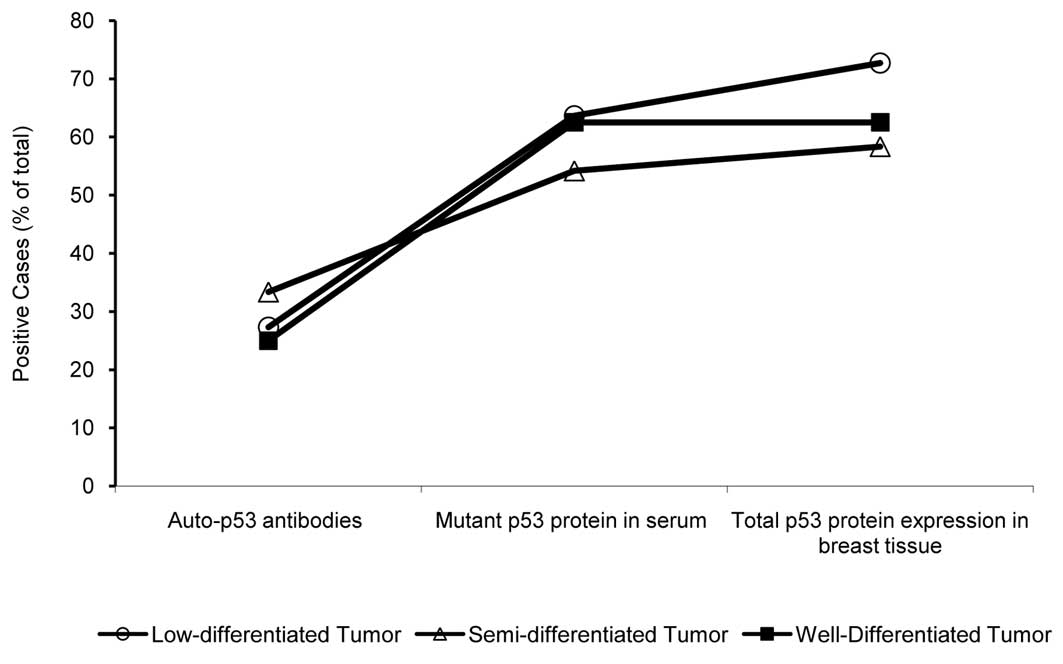
To determine whether the grade of tumor
differentiation affects the detection of p53 mutations, we analyzed
55 patients with poor, semi- and well-differentiated breast
carcinomas (Fig. 3). In patients
with poorly differentiated breast carcinomas, we found mutated p53
protein in serum in 7 of 13 patients (63.64%), while 8 of 13
(72.73%) exhibited total p53 protein expression using IHC. At the
semi-differentiated level, 8 of 24 patients (33.33%) showed the
presence of p53-auto-antibodies, 13 of 24 (54.17%) showed mutant
p53 protein, and 14 of 24 (58.33%) were positive for the presence
of p53 protein by IHC (Fig. 3). In
well-differentiated tumors, 5 of 8 patients (62.50%) showed mutant
p53 protein expression in serum by ELISA and in breast tumor
tissues by IHC (Fig. 3). These
results indicate that poorly differentiated breast tumors can be
identified by detecting p53 protein expression using IHC. No
statistically significant differences were found in the detection
of mutant p53 in serum among the poor, semi- or well-differentiated
breast carcinomas. However, the sensitivity of anti-p53 antibody
detection was lower than that of mutant p53 protein in serum.
Discussion
The development of molecular markers is required to
improve the diagnosis and assessment of tumor progression in breast
cancer patients. Mutations in the p53 tumor suppressor gene, as
well as overexpression of serum p53 antibodies and p53 protein in
tumor tissues, have been encountered in a variety of human
malignancies (16). The p53
antibody was originally described in 1982 by Crawford et al
(17) in the serum of 9% of breast
cancer patients using Western blot analysis. More than 15 studies
were performed by Soussi et al using ELISA in breast cancer
(16). The frequency of the p53
antibody in breast cancer ranged from 15 to 20%. However, the
majority of these studies were performed in European countries or
in the US. No studies have been performed in South America or in
Argentina, where the frequency of breast cancer is similar or
slightly lower than that observed in the studies conducted.
Overexpression of mutant p53 protein in breast
cancer patients has usually been evaluated in tumor tissue with
immunohistochemical staining; however, a serum assay for p53
oncoproteins using ELISA can be performed easily and repeatedly due
to its minimal invasiveness compared with assays using tissue
materials (18,19). In the present study, the median
serum level of mutant p53 protein in patients with IDC was
significantly different (26 of 43, 60.45%) (p<0.001) compared to
the controls.
Our results are well correlated with those of
studies performed in cervical carcinomas by Sobti et al
(20), who detected p53 mutant
protein in serum from 61.5% patients with invasive cervical
carcinoma (20). In addition, Oh
et al (21) recently
demonstrated similar results. However, there have been few results
involving breast cancer. Micelli et al (22) demonstrated the presence of mutant
p53 protein in serum in 23% of breast cancer patients, and showed a
100% mutant p53 specificity employing 20 healthy controls (22).
In the present study, mutant p53 protein was
predominantly detected in serum from IDC patients with the early
stages of the disease: 12/19 (63.15%) in stage I (p<0.0001), and
5/6 (83.33%) in stage II (p<0.0001). It was maintained at a high
level in late stages: 8/16 (50%) of patients in stage III. The
specificity of mutant p53 protein detection was 100%, since it was
found to be negative in the serum of normal control patients, and
was also negative in patients with benign diseases (0/6, 0%). In
this study, we observed the expression of p53 protein using IHC in
1 of 2 patients with DCIS. Further analyses are needed to
demonstrate the sensitivity of p53 mutation detection in the serum
of patients with DCIS.
The presence of mutant p53 protein in serum and p53
accumulation in tissue was correlated with poorly differentiated
tumors in patients with IDC (63.64 and 72.73%, respectively;
p<0.005) compared to those with well-differentiated tumors.
Several studies have demonstrated the presence of p53-accumulated
protein in breast cancer by IHC. Al-Moundhri et al (23) found p53 overexpression in 41.7% of
breast tumors. They also reported that the p53 accumulation was
related to poor differentiation in human breast cancer (23).
Expression of conformational altered protein induces
an immune response, thus leading to the presence of circulating
anti-p53 antibodies in cancer patients (24). Trivers et al (25) used an anti-p53 antibody as a
molecular marker and found a great level of anti-p53 antibody among
five workers occupationally exposed to vinyl chloride, who later
developed angiosarcoma of the liver (25).
However, in the present study, the level of anti-p53
antibodies demonstrated low sensitivity in breast cancer patients.
Its level was higher (47%) in advanced breast disease in patients
with IDC stage III. No statistically significant differences have
been found in the expression of p53 antibodies and the grade of
tumor differentiation. We found a high reactivity in patients ≤40
and ≥61 years of age, reaching similar levels of serological mutant
p53 protein in patients at those ages.
Recently, it was reported that TP53 and KRAS
mutation detection in the plasma of healthy subjects was associated
with environmental exposure to carcinogenic agents (26). These observations have implications
for monitoring the early stages of bladder cancer development. In
another report, analyses were performed to calculate the
association between the prevalence of positivity for the p53
antibody or mutant-p53 antigen with accumulative vinyl chloride
exposure in a population of healthy workers (27). The results from these studies
demonstrate the utility of the TP53 mutation in a simple blood
sample as a molecular marker to determine a minimum threshold for
the effects of exposure to carcinogens.
In conclusion, mutant p53 protein from serum was
elevated in invasive breast carcinomas, with a strong correlation
with p53-accumulation detected by IHC. These data strongly indicate
that the detection of mutant p53 in serum and p53 accumulation in
breast tissue are well correlated, and both tests are sensitive and
specific for invasive ductal breast carcinomas. A prospective study
with a large sample size is warranted, as the presence of mutant
p53 protein in serum is potentially useful as a biological marker
of breast carcinoma, particularly for the prediction of prognosis
and in follow-up after treatment.
Our findings indicate that mutant p53 in serum is a
promising novel parameter for the evaluation of cellular biology
and the prognosis of breast cancer using blood samples, thus
avoiding surgery. The presence of mutant p53 protein in serum is
potentially an important tool for discerning benign disease prior
to performing breast surgery.
Acknowledgements
This work was supported by the
Instituto de Análisis Clinicos Asociados (IACA Laboratory), Bahía
Blanca, Argentina. Special thanks to all the doctors of gynecology
from Sanatorio Privado del Sur, Interzonal Dr Jose Penna, Regional
Español, Dr Leonidas Lucero, Hospital de la Asociación Médica from
Bahía Blanca, Argentina, for their support.
References
|
1.
|
Ries L, Eisner M, Kosary C, et al: SEER.
Cancer Statistics Review. National Cancer Institute; Bethesda, MD:
pp. 1973–1999. 2002
|
|
2.
|
Greenie RT, Murray T, Boldin S and Wingo
P: Cancer statistics 2000. Cancer J Clin. 50:7–23. 2000. View Article : Google Scholar
|
|
3.
|
Stewart BW and Kleihues P: World Cancer
Report. IARC Press; France: 2003
|
|
4.
|
Oliveira AM, Ross JS and Fletcher JA:
Tumor suppressor genes in breast cancer: the gatekeepers and the
caretakers. Am J Clin Pathol. 124:S16–S28. 2005.PubMed/NCBI
|
|
5.
|
Bourdon JC, Laurenzi VD, Melino G and Lane
D: p53: 25 years of research and more questions to answer. Cell
Death Differ. 10:397–399. 2003.PubMed/NCBI
|
|
6.
|
Bourdon JC: p53 and its isoforms in
cancer. Br J Cancer. 97:277–282. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Soussi T: The p53 pathway and human
cancer. Br J Surg. 92:1331–1332. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Casey G, Lopez ME, Ramos JC, Plummer SJ,
Arboleda MJ, Shaughnessy M, Karlan B and Slamon DJ: DNA sequence
analysis of exons 2 through 11 and immunohistochemical staining are
required to detect all known p53 alterations in human malignancies.
Oncogene. 13:1971–1981. 1997.PubMed/NCBI
|
|
9.
|
Dowell SP, Wilson PO, Derias NW, Lane DP
and Hall PA: Clinical utility of the immunocytochemical detection
of p53 protein in cytological specimens. Cancer Res. 54:2914–2918.
1994.PubMed/NCBI
|
|
10.
|
Crawford LV, Pim DC and Bulbrook RD:
Detection of antibodies against the cellular protein p53 in sera
from patients with breast cancer. Int J Cancer. 30:403–408. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Soussi T: Antibodies in the sera of
patients with various types of cancer: a review. Cancer Res.
60:1777–1788. 2000.PubMed/NCBI
|
|
12.
|
Vogl FD, Frey M, Kreienberg R and
Runnebaum IB: Autoimmunity against p53 predicts invasive cancer
with poor survival in patients with an ovarian mass. Br J Cancer.
83:1338–1343. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Balogh GA, Corte MM, Nardi H, et al:
Mutant p53 protein in serum could be used as a molecular marker in
human breast cancer. Int J Oncol. 8:995–1002. 2006.PubMed/NCBI
|
|
14.
|
Lagios MD: Pathologic practice standards
for breast carcinoma: tumor size, reliable data, or miscues? J Am
Coll Surg. 196:91–92. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Silverstein MJ and Lagios MD: Pathologic
findings from the National Surgical Adjuvant Breast Project (NSABP)
eight-year update of Protocol B-17. Cancer. 88:242–244. 2000.
|
|
16.
|
Soussi T: p53 antibodies in the sera of
patients with various types of cancer: a review. Cancer Res.
60:1777–1788. 2000.PubMed/NCBI
|
|
17.
|
Crawford LV, Pimand DC and Bulbrook RD:
Detection of antibodies against the cellular protein p53 in sera
from patients with breast cancer. Int J Cancer. 30:403–408. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Choi JH, Oh JY, Ryu SK, et al: Detection
of epidermal growth factor receptor in the serum of gastric
carcinoma patients. Cancer. 79:1879–1883. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Oh MJ, Choi JH, Kim IH, et al: Detection
of epidermal growth factor receptor in the serum of patients with
cervical carcinoma. Clin Cancer Res. 6:4760–4763. 2000.PubMed/NCBI
|
|
20.
|
Sobti RC, Parashar K, Kaurand R and
Capalash N: Detection of human papillomavirus DNA, serum p53 and
p53 antibodies in patients with cervical cancer. J Environ Pathol
Toxicol Oncol. 21:79–85. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Oh MJ, Choi JH, Lee YH, Lee JK, Hur JY,
Park YK, Lee KW, Chough SY and Saw HS: Mutant p53 protein in the
serum of patients with cervical carcinoma: correlation with the
level of serum epidermal growth factor receptor and prognostic
significance. Cancer Lett. 203:107–112. 2004. View Article : Google Scholar
|
|
22.
|
Micelli G, Donadeo A and Quaranta M: The
p53 tumor suppressor gene. A preliminary clinical study in breast
cancer patients. Cell Biophys. 21:25–31. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Al-Moundhri M, Nirmala V, Al-Mawaly K,
Ganguly S, Burney I, Rizvi A and Grant C: Significance of p53,
Bcl-2 and HER-2/neu protein expression in Omani Arab females with
breast cancer. Pathol Oncol Res. 9:226–231. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Labrecque S, Naor N, Thomson D and
Matlashewski G: Analysis of the anti-p53 antibody response in
cancer patients. Cancer Res. 53:3468–3471. 1993.PubMed/NCBI
|
|
25.
|
Trivers GE, Cawley HL, De Benedetti VM,
Hollstein M, Marion MJ, Bennett WP, Hoover ML, Prives CC, Tamburro
CC and Harris CC: Anti-p53 antibodies in sera of workers
occupationally exposed to vinyl chloride. J Natl Cancer Inst.
87:1400–1407. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Gormally E, Vineis P, Matullo G, et al:
TP53 and KRAS2 mutations in plasma DNA of healthy subjects and
subsequent cancer occurrence: a prospective study. Cancer Res.
66:6871–6876. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Mocci F and Nettuno M: Plasma mutant-p53
protein and anti-p53 antibody as a marker: an experience in vinyl
chloride workers in Italy. J Occup Environ Med. 48:158–164. 2006.
View Article : Google Scholar : PubMed/NCBI
|