Introduction
Lung cancer is a malignant tumor responsible for the
highest mortality rate in humans worldwide (1). Non-small cell lung cancer (NSCLC) is
responsible for 80-85% of cases of diagnosed lung cancer (2). The incidence of lung adenocarcinoma
has been increasing in recent years, and despite the application of
various methods for treating lung adenocarcinoma, the mortality
rate remains high (3). Although
targeted drugs can be used in some cases to treat patients with
mutations in genes such as epidermal growth factor receptor and
anaplastic lymphoma kinase, the proportion of such patients is
limited and drug resistance limits the long-term efficacy of
targeted therapy (4). Therefore,
the identification of key genes associated with lung cancer is of
great significance for the development of novel therapeutic
strategies. The classical Wnt/β-catenin pathway serves a critical
role in the multiplication and differentiation of progenitor cells
in various adult epithelia (5). A
strong link has been identified between overactivation of the
Wnt/β-catenin pathway, and the occurrence and progression of
several types of cancer, including colorectal cancer (6). It was been reported that
overactivation of β-catenin in the pulmonary epithelium of
genetically engineered mice could induce epithelial differentiation
defects, promoting cell multiplication, basal cell amplification
and lung tumorigenesis (7). This
previous finding suggested that overactivation of the Wnt/β-catenin
pathway may also lead to lung cancer. It has further been shown
that the Wnt/β-catenin signaling pathway is extensively involved in
NSCLC as a controller of cellular proliferation, apoptosis,
differentiation, cell cycle progression, invasion and migration
(8-10). Epithelial-mesenchymal transition
(EMT) is a critical event, characterized by loss of cellular
polarity and contact, leading to migration of cancer cells and
tumor progression, which is induced by activation of the
Wnt/β-catenin pathway (11-13). Mutations in β-catenin or
adenomatous polyposis coli, which represent the most universal
mechanisms underlying abnormal activation of the Wnt/β-catenin
pathway, are infrequent in NSCLC (14). Therefore, the cause of
overactivation of the Wnt/β-catenin pathway and its effect on EMT
in NSCLC require further exploration.
Replication factor C (RFC) is a component of the
eukaryotic DNA polymerase (15).
In all eukaryotic cell cycles, it is essential for DNA duplication,
DNA injury repair and checkpoint control (16-18). RFC consists of five subunits
(RFC1-5). The interrelationships between RFC2, RFC3 and the c-MYC
oncogene (transcription factor) can induce cell division and
proliferation (19). With the
exception of RFC1, the other four subunits are highly expressed in
various malignant tumors (20-24). It has been reported that RFC3 can
combine with proliferating cell nuclear antigen (PCNA) to form a
complex, and decreased expression of RFC3 can restrict the
multiplication of cancer cells (25). Previous studies have demonstrated
that RFC3 is associated with liver, breast, esophageal and ovarian
cancer, and serves a critical role in cellular proliferation,
invasion and metastasis (25-28). Notably, 9-cis retinoic
acid-activated retinoid X receptor α can inhibit the growth of
retinoid-sensitive breast cancer and embryonic cells, and arrest S
phase entry by disrupting the RFC3-PCNA complex (29). These previous findings suggest
that RFC3 may be an important cancer antigen; however, the effect
of RFC3 on the occurrence and progression of NSCLC remains
unclear.
This study explored the expression of RFC3 in NSCLC
and corresponding paracancerous tissues, and investigated the
association between clinicopathological features and RFC3
expression. Furthermore, MTT, flow cytometry, Boyden chamber and
wound-healing assays were performed to explore the effects of RFC3
on proliferation, invasion and migration of A549 and H1299 cells.
Western blot analysis was finally applied to confirm that RFC3
induces EMT of lung adenocarcinoma H1299 and A549 cells via the
Wnt/β-catenin pathway.
Materials and methods
Tissue specimens, cell lines and culture
conditions
Tissue samples were obtained from patients with lung
adenocarcinoma or squamous cell carcinoma who underwent surgery at
The First Affiliated Hospital of China Medical University between
March 2010 and June 2013. This study was approved by the
Institutional Research Ethics Committee of China Medical University
and written informed consent was obtained from all 165 patients. A
total of 42 patients with lung squamous cell carcinoma and 123
patients with lung adenocarcinoma were included in this study. Each
case comprised cancerous tissue and paracancerous tissue (≥5 cm
from the neoplasm border) samples. All samples had complete
follow-up data and were pathologically diagnosed with lung squamous
cell carcinoma or adenocarcinoma. The NSCLC H460, A549, LK2, H1299,
H3255, H1650, H1975 and H292 cell lines were used in this study,
and normal human bronchial epithelial 135-E6E7 (HBE135-E6E7) cells
were used as a control. The tissue sections were stored in liquid
nitrogen. HBE cells were obtained from the Institute of
Biochemistry and Cell Biology at the Chinese Academy of Sciences.
The NSCLC H460, A549, LK2, H1299, H3255, H1650, H1975 and H292 cell
lines were acquired from the American Type Culture Collection. HBE,
A549 and LK2 cells were cultured in DMEM (cat. no. 10569069; Gibco;
Thermo Fisher Scientific, Inc.) and the remaining cell lines were
cultured in RPMI-1640 (cat. no. 61870044; Gibco; Thermo Fisher
Scientific, Inc.), with all recommended supplements: 10% fetal
bovine serum (cat. no. 10099141C), 100 U/ml penicillin and 100
µg/ml streptomycin (cat. no. 15140122) PBS (cat. no.
70013073) and trypsin (cat. no. R001100) (all from Gibco; Thermo
Fisher Scientific, Inc.). All cells were maintained in a humidified
container with 95% air and 5% CO2 at 37°C.
Immunohistochemistry
Immunohistochemistry was performed to investigate
RFC3 expression in cancerous and paracancerous tissues. The tissues
were fixed in 10% formalin for 4 h/mm at room temperature and embed
in paraffin blocks. The 4-µm paraffin-embedded sections of
lung cancer and paracancerous tissues were prepared and
deparaffinized three times in xylene (5 min each time) and were
then dehydrated in graded ethanol solutions. The sections were
washed twice in 100% ethanol (15 min/wash), then twice in 90%
ethanol (15 min/wash). After heat treatment at 95°C for 5 min with
0.01 mol/l citrate buffer (pH 6.0; cat. no. 005000; Thermo Fisher
Scientific, Inc.) for antigen retrieval, immunohistochemical
analysis of paraffin-embedded sections was performed by incubation
with a mouse monoclonal antibody (anti-RFC3; 1:100; cat. no.
sc-390293; Santa Cruz Biotechnology, Inc.) for 2 h at room
temperature, followed by incubation with a secondary antibody
(1:1,000; cat. no. 7076; Cell Signaling Technology, Inc.) for 1 h
at room temperature. Finally, the sections were counterstained with
hematoxylin for 2 min at room temperature. Rabbit IgG (1:100; cat.
no. 3900s; Cell Signaling Technology, Inc.) was employed as a
negative control. Two pathologists who were ignorant of the
clinical data independently analyzed the immunohistochemistry
results. A semi-quantitative method was used to determine the
expression levels of RFC3. The proportion and staining intensity of
positive cells were scored under a light microscope. The proportion
of positive cells was scored as follows: 0, 0; 1, 1-25; 2, 26-50;
3, 51-75; and 4, 76-100%; the positive staining intensity was
scored as follows: 0, no staining; 1, light brown staining; 2,
moderate brown staining; 3, dark brown staining. The final score
was obtained by multiplying the two results for each sample; scores
ranged between 0 and 12. Receiver operating characteristic curve
analysis was performed to determine the cut-off scores for low or
high RFC3 expression. All samples were separated into low
expression (0-4) or high expression (5-12)
groups.
Cell transfection for overexpression and
knockdown of RFC3
A549 cells were treated with 0.25% trypsin and
evenly inoculated in 6-well culture plates at a density of
1.5×105 cells/well. After incubation at constant
temperature (37°C, 5% CO2), cells were transfected once
they adhered to the plates. Cells were starved of serum for 1 h
prior to transfection. The transfection mixture consisted of
serum-free medium, 2.5 µg/ml RFC3 plasmid (cat. no.
RC201655; OriGene Technologies, Inc.) or control plasmid (cat. no.
PS100001; OriGene Technologies, Inc.), and
Lipofectamine® 3000 (cat. no. L3000150; Invitrogen;
Thermo Fisher Scientific, Inc.), and was added to the wells
drop-wise. The culture plate was then gently shaken and incubated
at constant temperature (37°C, 5% CO2) for 5 h. The
transfection media were then discarded, and DMEM containing 10%
fetal calf serum (Gibco; Thermo Fisher Scientific, Inc.) was added
for further culture (37°C, 5% CO2, 24 h).
H1299 cells were digested with 0.25% trypsin and
evenly inoculated into 6-well culture plates at a density of
1×105 cells/well. Following incubation at constant
temperature (37°C, 5% CO2), cells were transfected once
they adhered to the plates. Cells were starved of serum for 1 h
prior to transfection. The transfection mixture consisted of
serum-free medium, 100 nmol RFC3 small interfering (si)RNA (cat.
no. sc-37635; Santa Cruz Biotechnology, Inc.) or control siRNA
(cat. no. sc-37007; Santa Cruz Biotechnology, Inc.), and DHARMAFECT
(cat. no. T-2001-02; GE Healthcare Dharmacon, Inc.), and was added
to the wells dropwise. The culture plate was then gently shaken and
incubated at constant temperature (37°C, 5% CO2) for 5
h. Transfection media were discarded and RPMI-1640 medium
containing 10% fetal calf serum was added for further culture
(37°C, 5% CO2, 48 h).
Western blot analysis
Cells were rinsed with PBS three times. After
removing the buffer, cells were collected in a culture bottle. The
prepared lysis buffer (cat. no. FNN0021; Thermo Fisher Scientific,
Inc.) was added to the culture bottle, and cell lysis was allowed
to occur on ice for 30 min. Protein concentration in the
supernatants was determined using a BCA kit (Pierce; Thermo Fisher
Scientific, Inc.). Proteins (20 µg/lane) were separated by
SDS-PAGE using 10% gels and were transferred to PVDF membranes (EMD
Millipore) for analysis. The PVDF membranes were then transferred
to 0.05% Tween-TBS (TTBS) and rinsed for 5 min; this was repeated
three times. PVDF membranes were blocked with 5% milk in TTBS for 1
h at room temperature, and were probed with primary antibodies
against RFC3 (1:500; cat. no. sc-390293; Santa Cruz Biotechnology,
Inc.), Vimentin (1:1,000, cat. no. 5741S; Cell Signaling
Technology, Inc.), N-cadherin (1:1,000, cat. no. 13116S, Cell
Signaling Technology, Inc.), E-cadherin (1:1,000, cat. no. 14472S;
Cell Signaling Technology, Inc.), phosphorylated (p)-glycogen
synthase kinase 3 (GSK3)-β (Ser9) (1:1,000, cat. no. 5558S; Cell
Signaling Technology, Inc.), β-catenin (1:1,000, cat. no. 8480S,
Cell Signaling Technology, Inc.), GSK3-β (1:1,000, cat. no. 12456S;
Cell Signaling Technology, Inc.), c-MYC (1:1,000, cat. no. 13987S;
Cell Signaling Technology, Inc.), Wnt1 (1:1,000, cat. no.
27935-1-AP; Proteintech Group, Inc.), and GAPDH (1:1,000, cat. no.
5174S; Cell Signaling Technology, Inc.) or actin (1:2,000, cat. no.
3700S; Cell Signaling Technology, Inc.) overnight at 4°C.
Subsequently, the PVDF membranes were rinsed with TTBS three times
prior to incubation with horse anti-mouse IgG-HRP (1:2,000; cat.
no. 7076V; Cell Signaling Technology, Inc.) or goat anti-rabbit
IgG-HRP (1:2,000; cat. no. 7074V; Cell Signaling Technology, Inc.)
secondary antibodies at indoor temperature for 2 h. The PVDF
membranes were finally rinsed three times and observed with an ECL
kit (Thermo Fisher Scientific, Inc.). The intensity of each protein
band was semi-quantified using image analysis software (ImageJ;
National Institutes of Health).
Cell growth curve analysis
The MTT assay was used to observe the effects of
RFC3 upregulation or downregulation on lung adenocarcinoma cell
proliferation. After A549 and H1299 cells were transfected for 48
h, they were transferred to 96-well plates; cell density was
maintained at ~2,000 cells per well. At scheduled times on days
1-5, 5 mg/ml MTT solution was added to each well, and the reaction
was allowed to occur at 37°C for 4 h. Subsequently, DMSO was added
to the wells. The absorbance of each well was calculated using a
microplate reader at a wavelength of 490 nm.
Flow cytometry
To detect the proportion of cells in different
stages of the cell cycle and apoptotic cells, flow cytometry
(FACSCalibur; BD Biosciences) was conducted. A total of 3 days
post-transfection, the A549 and H1299 cells were collected, rinsed
with PBS and treated with 75% ethanol at 4°C for 2 h. After washing
with PBS, the cells were incubated with 200 µg/ml RNAse
(cat. no. 10109134001; Sigma-Aldrich; Merck KGaA) for 20 min at
room temperature and stained with 1 µg/ml propidium iodide
(PI; BD Biosciences) in 1 ml PBS at 4°C for 30 min. Subsequently,
the cell cycle was measured by flow cytometry. Cell apoptosis was
detected after washing with 500 µl PBS. Briefly, 10% Annexin
V-FITC (BD Biosciences) and 50 µg/ml PI staining was
performed for 15 min in the dark at room temperature. To promote
apoptosis, A549 cells were treated with paclitaxel (Shanghai YuanYe
Bio-Technology Co. Ltd.) at a final concentration of 50 nM,
followed by incubation for 18 h at 37°C. In addition, H1299 cells
were treated with erlotinib (MAYA Reagent) at a final concentration
of 2 µM and were incubated for 18 h at 37°C. Apoptosis was
measured by flow cytometry using a FACSCalibur analysis system (BD
Biosciences). Data were analyzed with Modfit 2.0 (Verity Software
House, Inc.).
Boyden chamber assay
Cell invasion and migration were analyzed using
Transwell assays. For the migration analysis, 1×105
cells were added to the upper Boyden chamber. After 24 h,
non-migrating cells were removed from the upper chamber with a soft
cotton swab and the cells that had migrated to the lower chamber
were stained with hematoxylin for 15 min at room temperature and
counted under light microscopy. For the invasion analysis, the
upper Boyden chamber was precoated with 50 mg/l Matrigel (BD
Biosciences) prior to the addition of 1×105/ml cells to
the upper chamber. The other steps remained almost the same as for
the migration analysis. Finally, the cells that had invaded into
the lower chamber through the membranes were stained with
hematoxylin for 15 min at room temperature and counted under light
microscopy.
Wound-healing assay
Cells were transferred to 6-well plates at
5×105 cells/well and allowed to reach 90% confluence. A
single layer of cells was scratched in a straight line using a
10-µl pipette tip and was washed with PBS. Subsequently, the
plates were cultured in serum-free medium at 37°C for 48 h. The
width of the healing monolayer wound was recorded after 0 and 48 h.
Quantitative analysis of the wound area from three independent
experiments was performed using ImageJ software with the macro MRI
Wound Healing Tool. Migration rate was presented as a percentage of
the initial wound area: Wound area (%)=(wound area at 0 h-wound
area at 48 h)/wound area at 0 hx100. 0 h is the time when the
scratch was initially created; 48 is 48 h after scratch
creation.
Statistical analysis
Each experiment was repeated at least three times.
The immunohistochemistry results were assessed using χ2
test, whereas the other results were assessed using Student's
t-test or one-way ANOVA, in order to examine the differences
between groups, and data were expressed as the mean ± SD. Multiple
comparisons between the groups were performed using the S-N-K
method. Repeated-measures two-way ANOVA was used to determine
whether there were statistical differences between the growth
curves. Cox regression was employed for univariate and multivariate
analyses. The overall survival rate was assessed by Kaplan-Meier
survival analysis and compared with the log-rank test. SPSS 23.0
(SPSS, Inc.) was employed for statistical analysis, and P<0.05
was considered to indicate a statistically significant
difference.
Results
RFC3 expression in lung cancer
specimens
RFC3 exhibited high expression in lung
adenocarcinoma and RFC3 expression was associated with
clinicopathological characteristics; this was not observed in lung
squamous cell carcinoma. RFC3 expression was measured in various
tissues, as shown in Figs. 1 and
2; and Table I. RFC3 expression in 123 lung
adenocarcinoma specimens was significantly higher than in the
corresponding non-neoplastic lung tissues (P<0.0001). However,
no significant differences were found in 42 cases of lung squamous
cell carcinoma (P=0.533). The association between RFC3 expression
and the clinicopathological characteristics of 123 patients with
lung adenocarcinoma, including sex, age, smoking history, TNM
classification (30),
differentiation, tumor size and node status, is presented in
Table II. RFC3 expression was
markedly associated with TNM classification, differentiation and
node status. Univariate analysis revealed that RFC3 expression, TNM
classification, differentiation, tumor size and node status had
significant effects on overall survival in patients with lung
adenocarcinoma. The expression of RFC3, differentiation and node
status were confirmed as critical independent risk factors by
multivariate analysis (Table
III). Kaplan-Meier analysis indicated that high RFC3 expression
could lead to a poor prognosis in cases of lung adenocarcinoma;
similar results were determined in analysis of disease-free
survival (Fig. 3; P<0.05). In
42 cases of lung squamous cell carcinoma, univariate analysis
revealed that RFC3 expression had no significant effect on
prognosis (P=0.57; data not shown). The expression of RFC3 in three
cases of lung adenocarcinoma and corresponding normal lung tissues
was evaluated by western blotting. The protein expression levels of
RFC3 in cancer tissues were higher than in normal lung tissues;
these findings were consistent with the immunohisto-chemistry
results (Fig. 4A). RFC expression
in NSCLC cell lines and the HBE cell line was evaluated by western
blotting (Fig. 4B). RFC3
expression in the lung adenocarcinoma A549 cell line was slightly
lower than that in HBE, but no significant difference was found
(P=0.1049). RFC3 expression in the lung squamous cell carcinoma LK2
cell line was slightly higher than that in HBE, but no significant
difference was found (P=0.7724). RFC3 expression in the other NSCLC
cell lines was significantly higher than that in HBE cells
(P<0.05).
 | Table IExpression of RFC3 in different
tissues. |
Table I
Expression of RFC3 in different
tissues.
| Tissue type | n | RFC3 expression
| χ2 | P-value |
|---|
| Low expression
(%) | High expression
(%) |
|---|
| Lung
adenocarcinoma | 123 | 66 (53.66) | 57 (46.34) | 18.732 | <0.0001a |
| Non-tumor lung
tissue | 123 | 98 (79.67) | 25 (20.33) | | |
| Lung squamous
carcinoma | 42 | 35 (83.33) | 7 (16.67) | 0.389 | 0.533 |
| Non-tumor lung
tissue | 42 | 37 (88.10) | 5 (11.90) | | |
| Table IIAssociation between RFC3 expression
and clinicopathological characteristics of 123 patients with lung
adenocarcinoma. |
Table II
Association between RFC3 expression
and clinicopathological characteristics of 123 patients with lung
adenocarcinoma.
| Variables | RFC3 expression
| Total | χ2 | P-value |
|---|
| Low expression | High
expression |
|---|
| Total cases | 66 | 57 | | | |
| Sex | | | | 0.012 | 0.914 |
| Male | 26 | 23 | 49 | | |
| Female | 40 | 34 | 74 | | |
| Age | | | | 0.879 | 0.349 |
| ≤60 years | 38 | 28 | 66 | | |
| >60 years | 28 | 29 | 57 | | |
| Smoking
history | | | | 2.897 | 0.089 |
| Yes | 27 | 15 | 42 | | |
| No | 39 | 42 | 81 | | |
| TNM stage | | | | 6.409 | 0.011a |
| Stage I-II | 60 | 42 | 102 | | |
| Stage III-IV | 6 | 15 | 21 | | |
|
Differentiation | | | | 5.139 | 0.023a |
| Well | 39 | 22 | 61 | | |
| Moderate/poor | 27 | 35 | 62 | | |
| Size | | | | 2.328 | 0.127 |
| ≤3 cm | 49 | 35 | 84 | | |
| >3 cm | 17 | 22 | 39 | | |
| Node status | | | | 5.747 | 0.017a |
| Positive | 9 | 18 | 27 | | |
| Negative | 57 | 39 | 96 | | |
| Table IIIUnivariate and multivariate analyses
of the factors associated with overall survival of patients with
lung adenocarcinoma. |
Table III
Univariate and multivariate analyses
of the factors associated with overall survival of patients with
lung adenocarcinoma.
| Variables | Univariate analysis
| Multivariate
analysis
|
|---|
| Hazard ratio | 95% CI | P-value | Hazard ratio | 95% CI | P-value |
|---|
| RFC3
expression | 3.46 | 1.660-7.209 | 0.001a | 2.339 | 1.103-4.959 | 0.027a |
| Sex | 1.812 | 0.933-3.517 | 0.079 | | | |
| Age | 1.927 | 0.980-3.792 | 0.057 | | | |
| Smoking
history | 1.504 | 0.770-2.938 | 0.233 | | | |
| TNM stage | 4.088 | 2.051-8.148 | <0.0001a | 0.588 | 0.211-1.636 | 0.309 |
|
Differentiation | 4.907 | 2.141-11.249 | <0.0001a | 3.143 | 1.321-7.478 | 0.010a |
| Size | 2.78 | 1.431-5.401 | 0.003a | 1.558 | 0.747-3.248 | 0.237 |
| Node status | 5.578 | 2.859-10.882 | <0.0001a | 4.922 | 1.913-12.665 | 0.001a |
Role of RFC3 in cell proliferation, cell
cycle progression and apoptosis
Based on the aforementioned results, a plasmid
containing cloned RFC3 cDNA was transfected into the A549 cell line
to induce overexpression of RFC3. In addition, a RFC3 siRNA was
transfected into the H1299 cell line to knock down RFC3. Western
blotting was employed to verify the effects (Fig. 5). As shown in Fig. S1, the proliferative ability of
H1299 and A549 cells was not significantly affected by
overexpression or knockdown of RFC3 compared with in the control
groups (P>0.05). Flow cytometry revealed that the percentage of
A549 cells in G0/G1 stage was decreased when
RFC3 was overexpressed, whereas the percentage of S stage cells was
increased, indicating that RFC3 overexpression induced more cells
to enter S stage from G1 stage (P<0.05). The
proportion of H1299 cells in G0/G1 stage was
increased when RFC3 was knocked down, whereas the proportion of S
stage cells was decreased, indicating that more cells were arrested
at G0/G1 stage after RFC3 was knocked down
(P<0.05; Fig. S2). Although
fewer apoptotic cells were detected in the A549 cell line when RFC3
was overexpressed, the difference was not significant compared with
in the control group (P=0.2666). In addition, more apoptotic cells
were detected in the H1299 cell line when RFC3 was knocked down in
comparison with the control group (P<0.01; Fig. S3). When paclitaxel was added to
the A549 cell line to induce apoptosis, fewer apoptotic cells were
detected in the A549 cell line when RFC3 was overexpressed in
comparison with the control group (P<0.01). Conversely, when
erlotinib was added to the H1299 cell line to induce apoptosis,
more apoptotic cells were detected in the H1299 cell line when RFC3
was knocked down in comparison with the control group (P<0.05;
Fig. S4).
Effects of RFC3 on cell invasion and
migration
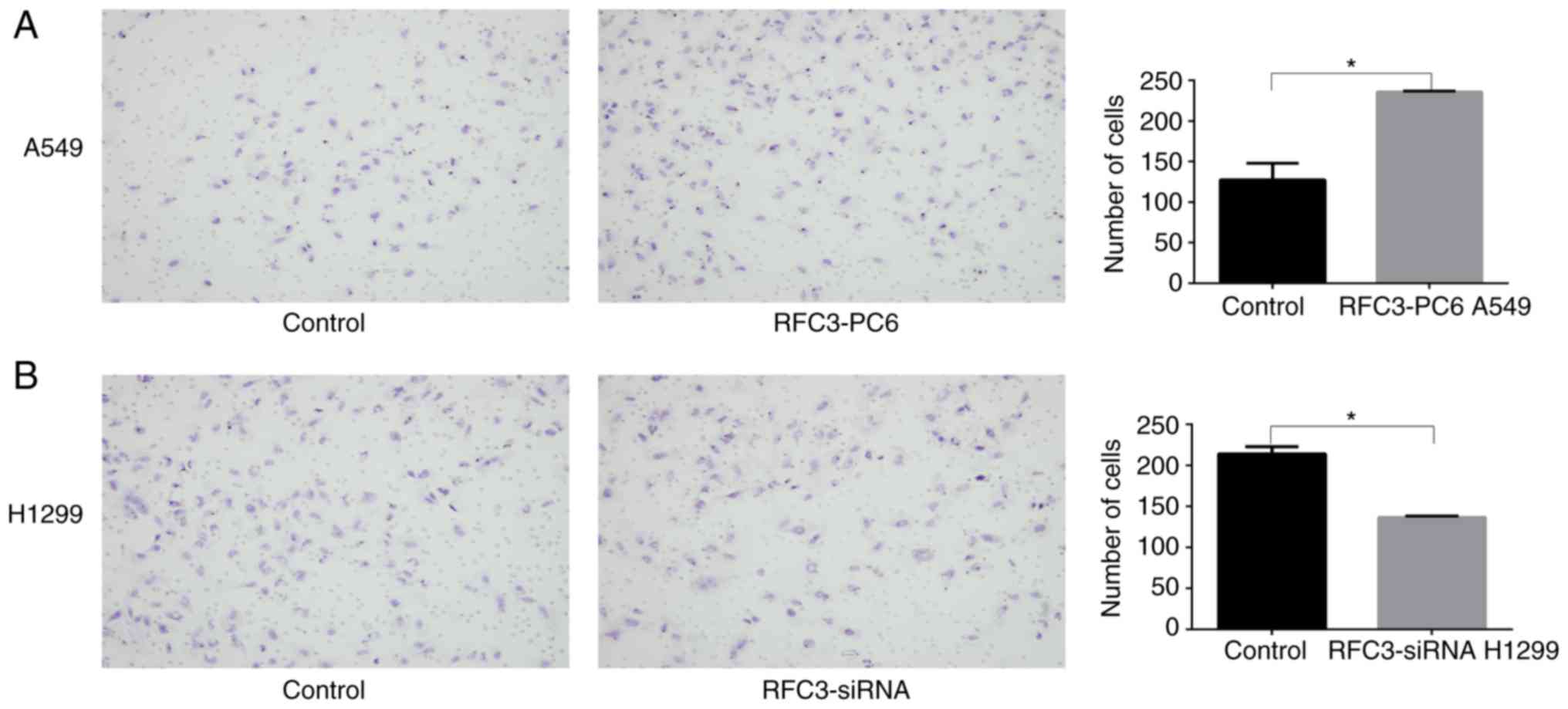
The Boyden chamber assay indicated that the invasion
and migration of A549 cells was significantly increased following
overexpression of RFC3 (P<0.05), whereas the invasion and
migration of H1299 cells was significantly decreased after RFC3
downregulation (P<0.05; Figs.
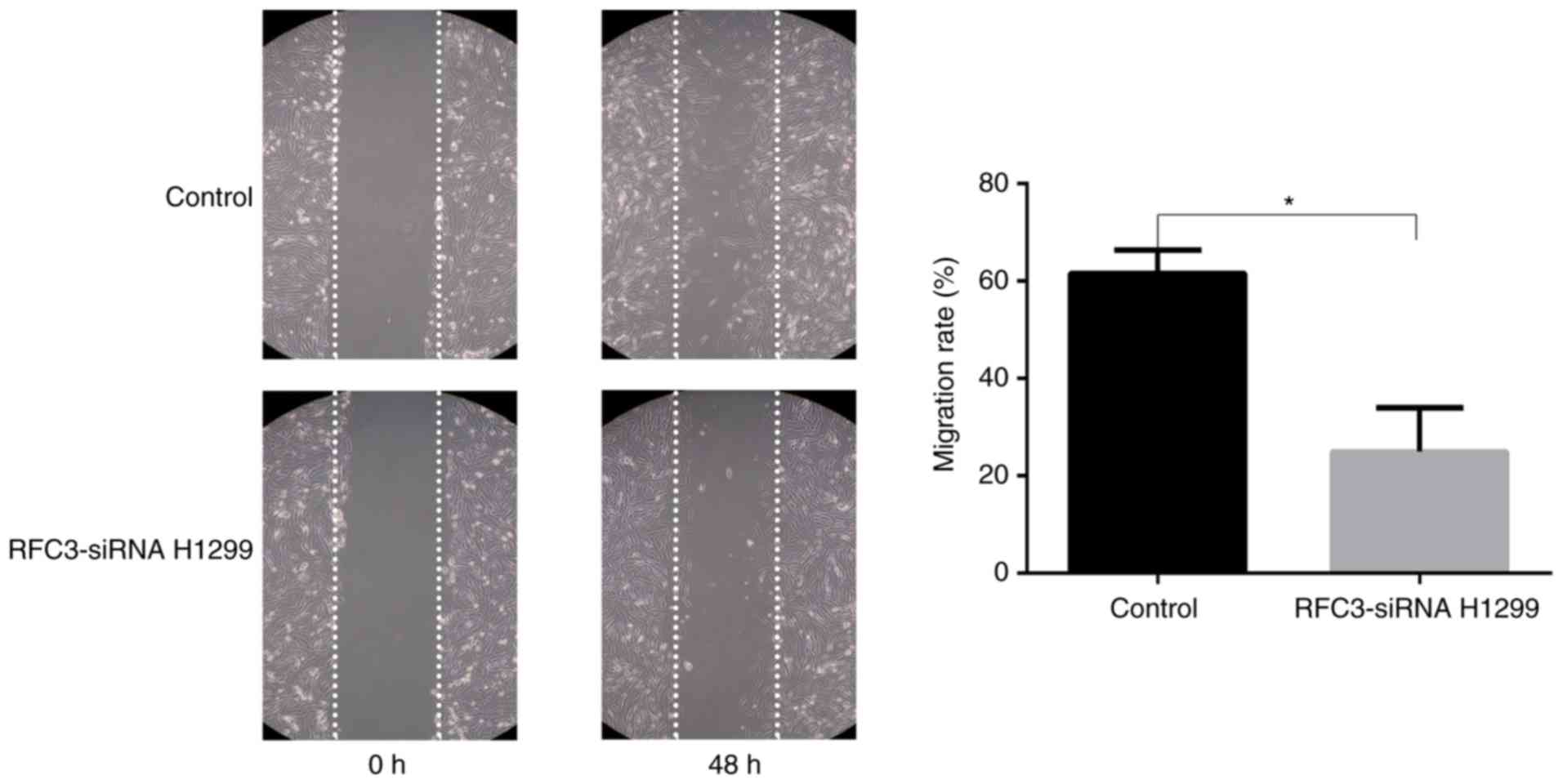
6 and 7). The wound-healing
assay demonstrated that the migration rate of A549 cells following
overexpression of RFC3 was markedly higher than that in the control
group (P<0.05), indicating that the migratory ability of A549
cells was increased (Fig. 8).
Conversely, after the knockdown of RFC3, the opposite result was
observed in H1299 cells (P<0.05; Fig. 9).
RFC3 induces EMT in lung adenocarcinoma
cells via the Wnt/β-catenin pathway
Western blotting was employed to detect alterations
in the expression of proteins associated with the Wnt/β-catenin
signaling pathway and EMT in A549 cells transfected with the RFC3
overexpression plasmid and H1299 cells transfected with the RFC3
siRNA. After the overexpression of RFC3 in A549 cells, the
expression levels of Wnt1, β-catenin, c-MYC, N-cadherin, Vimentin
and the ratio of p-GSK3-β (Ser9)/GSK3-β were increased, whereas
E-cadherin expression was decreased. However, following RFC3
knockdown in H1299 cells, the expression levels of Wnt1,
N-cadherin, β-catenin, Vimentin, c-MYC and the ratio of p-GSK3-β
(Ser9)/GSK3-β were decreased, whereas E-cadherin expression was
increased. These results suggested that RFC3 may trigger the
Wnt/β-catenin signaling pathway in A549 and H1299 cells and promote
lung adenocarcinoma migration and invasion through EMT (Fig. 10).
 | Figure 10Effects of RFC3 on the regulation of
proteins associated with epithelial-mesenchymal transition and the
Wnt/β-catenin signaling pathway. (A) RFC3 overexpression plasmid
and empty vector were transfected into the lung cancer A549 cell
line. (B) RFC3-specific siRNA and non-specific control siRNA were
transfected into the lung cancer H1299 cell line. Total protein was
extracted and subjected to immunoblotting of Wnt1, p-GSK3-β (Ser9),
GSK3-β, β-catenin, c-MYC, E-cadherin, N-cadherin and Vimentin.
Actin was used as a loading control. (A and B) Representative image
data of immunoblotting, semi-quantitative representation of protein
expression and ratios of p-GSK3-β/GSK3-β from three separate
experiments. *P<0.05, **P<0.01. GSK3,
glycogen synthase kinase 3; p-, phosphorylated; RFC3, replication
factor C subunit 3; siRNA, small interfering RNA. |
Discussion
NSCLC is the main cause of malignant
tumor-associated mortality in humans and adenocarcinoma is the main
subtype worldwide (1). Novel
diagnostic and therapeutic technologies have been developed;
however, overall survival and prognosis are still poor (2,3).
Therefore, it is important to identify new biomarkers and pathways
for the treatment of lung adenocarcinoma. In several types of
malignant tumor, RFC3 is overexpressed and is associated with the
regulation of tumor development through various mechanisms, as
observed in triple-negative breast cancer, ovarian cancer,
esophageal cancer and liver cancer (25-28). However, it has also been reported
that RFC3 mutations in gastric and colorectal cancer result in
downregulation of expression or loss of function (31). These findings indicated that RFC3
might serve different roles in different types of cancer.
Therefore, the mechanism and function of RFC3 in NSCLC remains to
be elucidated.
Through immunohistochemistry, this study revealed
that RFC3 expression was markedly higher in lung adenocarcinoma
tissue compared with in corresponding paracancerous lung tissue,
and RFC3 expression was significantly associated with
clinicopathological characteristics; these findings were not
observed in lung squamous cell carcinoma. Notably, RFC3 expression
was markedly associated with TNM classification, differentiation
and node status in lung adenocarcinoma. Furthermore, RFC3
expression was determined to be a critical independent risk factor
through multivariate analysis. Kaplan-Meier analysis indicated that
RFC3 overexpression could lead to a poor prognosis in patients with
lung adenocarcinoma, and similar results were obtained in analysis
of disease-free survival. These results demonstrated that RFC3 may
present prognostic value in human lung adenocarcinoma. The outcomes
of this research were highly similar to findings obtained in
triple-negative breast cancer, esophageal cancer, ovarian cancer
and liver cancer (25-28). However, to the best of our
knowledge, RFC3 has not been reported as an independent risk factor
in lung adenocarcinoma. Unlike triple-negative breast cancer, RFC3
expression was not related to the size of lung adenocarcinoma
(P=0.127) (25), which suggests
that RFC3 may not be associated with the proliferation of lung
adenocarcinoma cells.
In the present cell line experiments, the highest
expression of RFC3 was detected in H292 cells and the second
highest in H460 cells. However, H292 and H460 cells are a
mucoepidermoid carcinoma of the bronchus cell line and a large-cell
lung cancer cell line, respectively. The incidence of these cancers
is much lower than that of lung adenocarcinoma; therefore, their
value for further clinical research is limited. Finally, the lung
adenocarcinoma H1299 cell line was selected for use in the present
study for the RFC3 knockdown experiment; this cell line exhibited
the third highest expression of RFC3. Previous studies have
observed changes in cell biological behavior after knocking down
RFC3 (25-28). In addition, RFC3 overexpression
was induced in A549 cells with low basal expression, in order to
observe changes in their biological behavior. The proliferative
abilities of A549 and H1299 cells were not significantly affected
by overexpression or knockdown of RFC3 compared with in the control
groups. These findings confirmed that RFC3 may not be associated
with the proliferation of lung adenocarcinoma cells. However,
previous studies have reported that the proliferation curve is
significantly decreased when RFC3 is knocked down (25-28) in the following cell lines: Liver
cancer SMMC-7721, ovarian cancer OVCAR-3, breast cancer MDA-MB-231
and MDA-MB-468, and esophageal cancer, OE33 and OE19. The
difference in these findings might suggest that RFC3 serves
different roles in cancer cell proliferation in different types of
cancer.
Flow cytometry suggested that upregulation of RFC3
resulted in a greater number of cells entering S phase from
G1 phase in A549 cells, whereas downregulation of RFC3
resulted in a greater number of cells arrested at
G0/G1 phase in H1299 cells; however, no
significant change in the ratio of cells in G2/M stage
was found. The proportion of G0/G1 and S
phase cells was altered by only ~4%; therefore, it was hypothesized
that RFC3 may exert a certain effect on the cell cycle progression
of lung adenocarcinoma, but this effect is weaker than that on
liver cancer and ovarian cancer. Notably, hepatocellular and
ovarian cancer cell lines were arrested in S phase after RFC3
knockdown (26,27). Changes in some cell cycle
regulatory proteins have been detected after RFC3 knockdown in
hepatocellular carcinoma cell lines, which explains why the
hepatocellular carcinoma cell cycle was arrested in S stage after
RFC3 knockdown in this previous study (26). The present study demonstrated that
upregulation of RFC3 or knockdown of RFC3 could result in
corresponding changes in the downstream protein c-MYC in the
Wnt/β-catenin pathway. Notably, c-MYC can promote cell cycle
G1-S progression (32-34). Unlike the effects on
hepatocellular carcinoma cells (26), in this study, the effects of RFC3
on the cell cycle progression of lung adenocarcinoma resulted in
G1-S progression, not S-G2 progression. Why
RFC3 has different effects on the cell cycle progression of
hepatocellular carcinoma and lung adenocarcinoma cells requires
further study.
Upregulation of RFC3 reduced apoptosis in the A549
cell line; however, the difference was not significant when
compared with the control group. When paclitaxel was added to the
A549 cell line to induce apoptosis, overexpression of RFC3 more
obviously reduced apoptosis in the A549 cell line; this finding was
statistically significant. Whether or not erlotinib was added to
H1299 cells to induce apoptosis, knockdown of RFC3 resulted in a
significant increase in apoptosis. However, the percentage of
apoptotic cells changed very little, all <2%. Furthermore, after
72 h of incubation, it was observed that the apoptotic cells were
almost all early apoptotic cells. Unlike these results,
downregulation of RFC3 in ovarian cancer has been shown to induce a
higher proportion of apoptotic cells, and after 24 h incubation,
late apoptotic cells were revealed to account for the majority of
apoptotic cells (27). In
summary, RFC3 has a weaker effect on cell cycle progression and
apoptosis in lung adenocarcinoma cells than in other cancer
cells.
In this study, the results of Boyden chamber and
wound-healing assays suggested that RFC3 may increase lung cancer
cell invasion and migration. The expression levels of Wnt1 and the
ratio of p-GSK3-β (Ser9)/GSK3-β were upregulated by overexpression
of RFC3, which together may result in activation of the
Wnt/β-catenin signaling pathway. The upregulation of p-GSK3-β
(Ser9)/GSK3-β can lead to a decrease in the ability of GSK3-β to
phosphorylate and degrade β-catenin (35). β-catenin is a prime downstream
protein of the classical Wnt signaling pathway, which has a
critical function in EMT. The accumulation of β-catenin leads to
upregulation of the expression of the downstream protein c-MYC and
affects EMT-related proteins (increases Vimentin and N-cadherin,
and decreases E-cadherin) (36,37). When RFC3 was knocked down, the
aforementioned effects of RFC3 overexpression were reversed. In a
previous study, microarray analysis and Ingenuity Pathway Analysis
software were employed to explore the biological pathways and gene
networks of RFC3 in esophageal adenocarcinoma (28). Pathway analysis of genes related
to RFC3 expression indicated that the Wnt/β-catenin signaling
pathway was enriched, but this prediction has not been further
confirmed (28). RFC3 has been
reported to promote EMT in triple-negative breast cancer cell
lines; however, there is no evidence that RFC3 promotes EMT in
triple-negative breast cancer cells by affecting the Wnt/β-catenin
signaling pathway (25). This
study indicated that RFC3 may induce EMT in lung adenocarcinoma
cells via the Wnt/β-catenin pathway.
This research had some limitations. A relatively
small number of cases was included in the study, and the TNM
classifications were mainly stages I and II. To address this
problem, extensive identification of cases with different TNM
classifications and complete case follow-up data are required.
Secondly, in vivo experiments and improved exploration of
the RFC3 mechanism are required in the future. STRING database
(38) and WebGestalt database
(39) were used for
bioinformatics analysis, however, the target protein through which
RFC3 can affect the Wnt pathway has not yet been identified (data
not shown). When the target protein has been identified, we aim to
study its association with RFC3 in vivo. Thirdly, the study
is retrospective; therefore, prospective studies and double-blind
control studies are required to further verify the current
outcomes. Finally, RFC3 expression in "normal" lung tissue was
compared and analyzed by immunohistochemistry. The 'normal' lung
tissues came from the paracancerous tissues of the same patients,
which might not truly represent normal tissue.
In conclusion, these data indicated that reduction
or over-expression of RFC3 could attenuate or increase the invasion
and migration of lung adenocarcinoma cells, respectively. In
addition, this study revealed that RFC3 regulated lung
adenocarcinoma biological behavior potentially by inducing EMT via
the Wnt/β-catenin pathway, and RFC3 expression was closely
associated with the clinical outcome of patients with lung
adenocarcinoma. These findings suggested that RFC3 may provide a
potential anticancer strategy for the treatment of metastasis of
advanced lung adenocarcinoma.
Supplementary Data
Acknowledgments
Not applicable.
Funding
This study was funded by the PhD Research Fund of
China Medical University.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SG and QZ designed the experiments. SG, XQ, SY, SZ
and PL performed the experiments, and SG, SY and PL analyzed the
data. SG and SZ wrote the manuscript. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
All experimental procedures involving human tissue
conformed to the ethical standards of The First Affiliated Hospital
of China Medical University. This study was approved by the
Institutional Research Ethics Committee of China Medical University
and written informed consent was obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ettinger DS, Wood DE, Akerley W, Bazhenova
LA, Borghaei H, Camidge DR, Cheney RT, Chirieac LR, D'Amico TA,
Demmy TL, et al: Non-small cell lung cancer, version 6.2015. J Natl
Compr Canc Netw. 13:515–524. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rotow J and Bivona TG: Understanding and
targeting resistance mechanisms in NSCLC. Nat Rev Cancer.
17:637–658. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Clevers H: Wnt/beta-catenin signaling in
development and disease. Cell. 127:469–480. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Klaus A and Birchmeier W: Wnt signalling
and its impact on development and cancer. Nat Rev Cancer.
8:387–398. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang Y, Goss AM, Cohen ED, Kadzik R,
Lepore JJ, Muthukumaraswamy K, Yang J, DeMayo FJ, Whitsett JA,
Parmacek MS and Morrisey EE: A Gata6-Wnt pathway required for
epithelial stem cell development and airway regeneration. Nat
Genet. 40:862–870. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Guo YZ, Xie XL, Fu J and Xing GL: SOX9
regulated proliferation and apoptosis of human lung carcinoma cells
by the Wnt/β-catenin signaling pathway. Eur Rev Med Pharmacol Sci.
22:4898–4907. 2018.PubMed/NCBI
|
|
9
|
Ding L, Yao W, Lu J, Gong J and Zhang X:
Upregulation of circ_001569 predicts poor prognosis and promotes
cell proliferation in non-small cell lung cancer by regulating the
Wnt/β-catenin pathway. Oncol Lett. 16:453–458. 2018.PubMed/NCBI
|
|
10
|
Zhang B, Li N and Zhang H: Knockdown of
homeobox B5 (HOXB5) inhibits cell proliferation, migration, and
invasion in non-small cell lung cancer cells through inactivation
of the Wnt/β-catenin pathway. Oncol Res. 26:37–44. 2018. View Article : Google Scholar
|
|
11
|
Weinberg RA: Mechanisms of malignant
progression. Carcinogenesis. 29:1092–1095. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen Z, He J, Xing X, Li P, Zhang W, Tong
Z, Jing X, Li L, Liu D, Wu Q and Ju H: Mn12Ac inhibits the
migration, invasion and epithelial-mesenchymal transition of lung
cancer cells by downregulating the Wnt/β-catenin and PI3K/AKT
signaling pathways. Oncol Lett. 16:3943–3948. 2018.PubMed/NCBI
|
|
13
|
Wang B, Sun L, Li J and Jiang R: miR-577
suppresses cell proliferation and epithelial-mesenchymal transition
by regulating the WNT2B mediated Wnt/β-catenin pathway in non-small
cell lung cancer. Mol Med Rep. 18:2753–2761. 2018.PubMed/NCBI
|
|
14
|
Akiri G, Cherian MM, Vijayakumar S, Liu G,
Bafico A and Aaronson SA: Wnt pathway aberrations including
autocrine Wnt activation occur at high frequency in human
non-small-cell lung carcinoma. Oncogene. 28:2163–2172. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Uhlmann F, Cai J, Flores-Rozas H, Dean FB,
Finkelstein J, O'Donnell M and Hurwitz J: In vitro reconstitution
of human replication factor C from its five subunits. Proc Natl
Acad Sci USA. 93:6521–6526. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Venclovas C, Colvin ME and Thelen MP:
Molecular modeling-based analysis of interactions in the
RFC-dependent clamp-loading process. Protein Sci. 11:2403–2416.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sancar A, Lindsey-Boltz LA, Unsal-Kacmaz K
and Linn S: Molecular mechanisms of mammalian DNA repair and the
DNA damage checkpoints. Annu Rev Biochem. 73:39–85. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shen H, Cai M, Zhao S, Wang H, Li M, Yao S
and Jiang N: Overexpression of RFC3 is correlated with ovarian
tumor development and poor prognosis. Tumour Biol. 35:10259–10266.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Koch HB, Zhang R, Verdoodt B, Bailey A,
Zhang CD, Yates JR III, Menssen A and Hermeking H: Large-scale
identification of c-MYC-associated proteins using a combined
TAP/MudPIT approach. Cell Cycle. 6:205–217. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xiong S, Wang Q, Zheng L, Gao F and Li J:
Identification of candidate molecular markers of nasopharyngeal
carcinoma by tissue microarray and in situ hybridization. Med
Oncol. 28(Suppl 1): S341–S348. 2011. View Article : Google Scholar
|
|
21
|
Arai M, Kondoh N, Imazeki N, Hada A,
Hatsuse K, Matsubara O and Yamamoto M: The knockdown of endogenous
replication factor C4 decreases the growth and enhances the
chemosensi-tivity of hepatocellular carcinoma cells. Liver Int.
29:55–62. 2009. View Article : Google Scholar
|
|
22
|
Niu G, Wang D, Pei Y and Sun L: Systematic
identification of key genes and pathways in the development of
invasive cervical cancer. Gene. 618:28–41. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Srihari S, Kalimutho M, Lal S, Singla J,
Patel D, Simpson PT, Khanna KK and Ragan MA: Understanding the
functional impact of copy number alterations in breast cancer using
a network modeling approach. Mol Biosyst. 12:963–972. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Martinez I, Wang J, Hobson KF, Ferris RL
and Khan SA: Identification of differentially expressed genes in
HPV-positive and HPV-negative oropharyngeal squamous cell
carcinomas. Eur J Cancer. 43:415–432. 2007. View Article : Google Scholar :
|
|
25
|
He ZY, Wu SG, Peng F, Zhang Q, Luo Y, Chen
M and Bao Y: Up-regulation of RFC3 promotes triple negative breast
cancer metastasis and is associated with poor prognosis Via EMT.
Transl Oncol. 10:1–9. 2017. View Article : Google Scholar
|
|
26
|
Yao Z, Hu K, Huang H, Xu S, Wang Q, Zhang
P, Yang P and Liu B: shRNA-mediated silencing of the RFC3 gene
suppresses hepatocellular carcinoma cell proliferation. Int J Mol
Med. 36:1393–1399. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Shen H, Xu J, Zhao S, Shi H, Yao S and
Jiang N: ShRNA-mediated silencing of the RFC3 gene suppress ovarian
tumor cells proliferation. Int J Clin Exp Pathol. 8:8968–8975.
2015.PubMed/NCBI
|
|
28
|
Lockwood WW, Thu KL, Lin L, Pikor LA,
Chari R, Lam WL and Beer DG: Integrative genomics identified RFC3
as an amplified candidate oncogene in esophageal adenocarcinoma.
Clin Cancer Res. 18:1936–1946. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Maeng S, Kim GJ, Choi EJ, Yang HO, Lee DS
and Sohn YC: 9-Cis-retinoic acid induces growth inhibition in
retinoid-sensitive breast cancer and sea urchin embryonic cells via
retinoid X receptor α and replication factor C3. Mol Endocrinol.
26:1821–1835. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sobin LH, Gospodarowicz MK and Wittekind
C: International Union Against Cancer (UICC): TNM Classification of
Malignant Tumours. 8th edition. Wiley-Blackwell; Oxford: 2017
|
|
31
|
Kim YR, Song SY, Kim SS, An CH, Lee SH and
Yoo NJ: Mutational and expressional analysis of RFC3, a clamp
loader in DNA replication, in gastric and colorectal cancers. Hum
Pathol. 41:1431–1437. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Pelengaris S and Khan M: The many faces of
c-MYC. Arch Biochem Biophys. 416:129–136. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Steiner P, Philipp A, Lukas J, Godden-Kent
D, Pagano M, Mittnacht S, Bartek J and Eilers M: Identification of
a Myc-dependent step during the formation of active G1 cyclin-cdk
complexes. EMBO J. 14:4814–4826. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Berns K, Hijmans EM and Bernards R:
Repression of c-Myc responsive genes in cycling cells causes G1
arrest through reduction of cyclin E/CDK2 kinase activity.
Oncogene. 15:1347–1356. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nusse R: Wnt signaling. Cold Spring Harb
Perspect Biol. 4:pii: a011163. 2012. View Article : Google Scholar
|
|
36
|
Ghahhari NM and Babashah S: Interplay
between microRNAs and WNT/β-catenin signalling pathway regulates
epithelial-mesenchymal transition in cancer. Eur J Cancer.
51:1638–1649. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
He W, He S, Wang Z, Shen H, Fang W, Zhang
Y, Qian W, Lin M, Yuan J, Wang J, et al: Astrocyte elevated
gene-1(AEG-1) induces epithelial-mesenchymal transition in lung
cancer through activating Wnt/β-catenin signaling. BMC Cancer.
15:1072015. View Article : Google Scholar
|
|
38
|
Szklarczyk D, Franceschini A, Wyder S,
Forslund K, Heller D, Huerta-Cepas J, Simonovic M, Roth A, Santos
A, Tsafou KP, et al: STRING v10: Protein-protein interaction
networks, integrated over the tree of life. Nucleic Acids Res.
43(Database Issue): D447–D452. 2015. View Article : Google Scholar
|
|
39
|
Wang J, Duncan D, Shi Z and Zhang B:
WEB-based GEne SeT AnaLysis toolkit (WebGestalt): Update 2013.
Nucleic Acids Res. 41(Web Server Issue): W77–W83. 2013. View Article : Google Scholar : PubMed/NCBI
|