Introduction
Poorly differentiated thyroid carcinoma is a
relatively rare disease. At present, it is thought to be an
intermediate entity in the progression of well-differentiated
thyroid carcinoma to anaplastic thyroid carcinoma (1,2). As
patients with poorly differentiated thyroid carcinoma usually have
a fast deterioration and fatal outcome, this carcinoma presents
surgeons with challenging treatment options. Furthermore, when the
carcinoma invades the trachea and results in airway obstruction,
the situation is an emergency and may be complicated. Therefore, an
appropriate treatment strategy is necessary. In the current study,
we present a case of an almost complete airway obstruction
resulting from the invasion of poorly differentiated thyroid
carcinoma. The anesthetist considered intubation to be dangerous as
it had the potential to cause rupture and embolism of the tumor and
lead to asphyxia. With the support of cardiopulmonary bypass
oxygenation, we successfully implanted a tracheal stent under the
guidance of flexible fiber optic bronchoscope. The patient’s
respiratory function improved and no complications occurred.
Furthermore, subsequent concurrent chemoradiotherapy reduced the
size of the tumor and prolonged the survival time of the
patient.
Case report
Patient data
A 48-year-old male presented with dyspnea and
intermittent stridor for three months. He also complained of a
cough and experienced a slight loss of voice. Therefore he attended
a local hospital where the physician misdiagnosed the condition as
asthma and administered the corresponding treatment. Unfortunately,
the dyspnea worsened gradually, and a month later the patient
became hoarse. Thus, the patient was referred to our hospital.
Informed consent was obtained from the patient prior to the study.
The ethics committee of Zhejiang University College of Medicine,
Zheijiang, China approved the study.
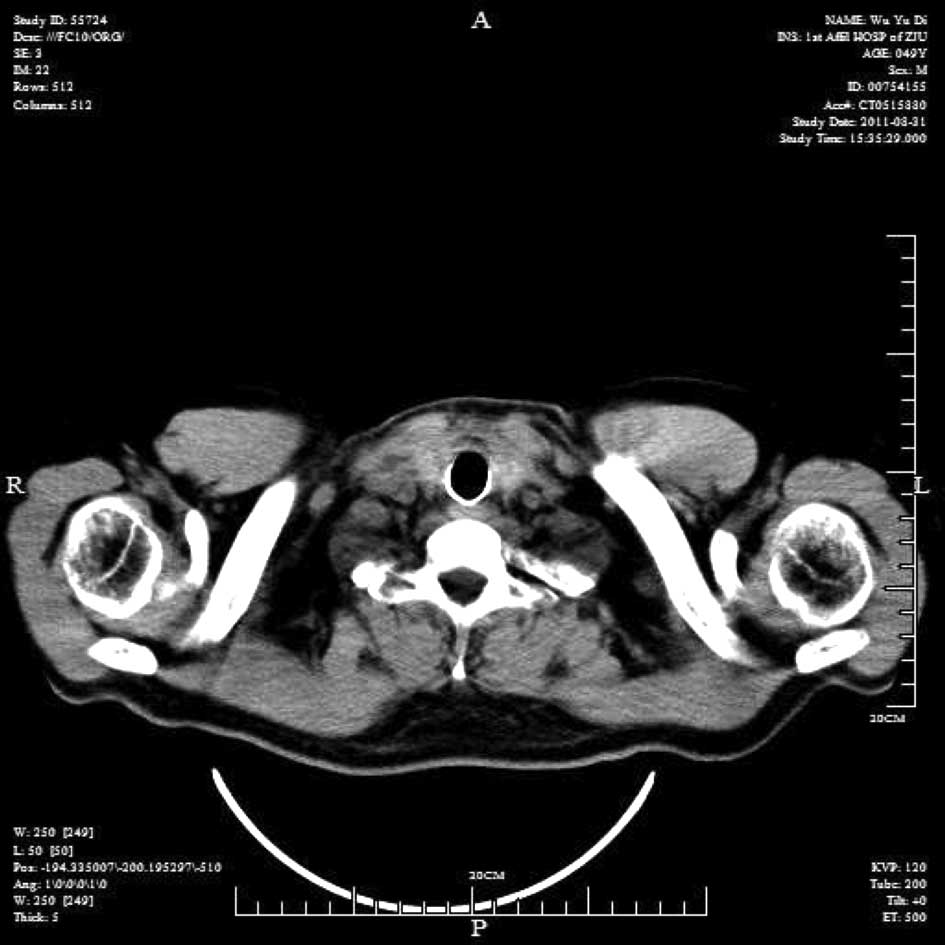
Palpation of the neck revealed a diffuse and firm
goiter without tenderness. Neck and chest computed tomography (CT)
scan showed an approximately 6.5-cm goiter in two lateral lobes of
the thyroid gland, firmly wrapping the trachea. The goiter had
invaded and protruded into the tracheal lumen and the narrowest
internal diameter was 3 mm (Fig.
1). The goiter extended down the trachea into the chest and
caused narrowing in a 5-cm stretch of the trachea. Laryngoscopy
revealed impaired mobility of the left vocal cords. The results of
the thyroid function test were within normal limits. The day after
admission, the patient presented with a sudden onset of orthopnea
and hemoptysis without an evident cause. After holding group
consultations, we selected emergency treatment with the family’s
consent.
Management procedure
As the intubation was unable to pass through the
narrowest part of the trachea, conventional general anesthesia by
tracheal intubation could not be carried out and it was also
unsafe, as intubation may have resulted in suffocation and
mortality. As the tumor had invaded the trachea and extended to the
substernal area, tracheotomy alone may not have been sufficient to
relieve the breathing difficulties. Suffocation may also have
occurred when undergoing flexible bronchoscopy. Therefore,
extracorporeal oxygenation support was thought to be necessary for
the patient.
The patient was sedated with intravenous diazepam.
Under local anesthesia with lidocaine, a femoro-femoral
cardiopulmonary bypass was started; venous drainage was obtained by
right femoral vein cut-down and arterial inflow was obtained by
right femoral artery cut-down. Through the cardiopulmonary bypass
system, the level of arterial oxygen saturation (SaO2)
was maintained at >90% throughout the procedure. The patient was
intravenously anesthetized and flexible tracheoscopy was performed,
which revealed a severe narrowing of the trachea at 5 cm from the
vocal cords with invasion by tumor tissue, and the narrowest
stenosis was 0.3 cm in diameter. Attempts to traverse the stenosis
with a bronchoscope were unsuccessful. Incisional biopsy was
performed guided by a bronchoscope and tumor tissue was acquired.
Fast-frozen pathology revealed poorly differentiated thyroid
carcinoma. Therefore, it was decided to insert a tracheal stent to
treat the compromised airway instead of performing a surgical tumor
resection. A guide-wire was inserted through the fiber optic
bronchoscope into the trachea stenosis. Then the bronchoscope was
moved away, and an 18×60-mm stent was inserted into the trachea
under fluoroscopic control. Finally, the distal end of the stent
was located across the stricture to normal trachea tissue. The
patient experienced neither dyspnea nor stridor, the respiratory
function was significantly improved and there were no complications
following stent insertion (e.g., migration, retention of
secretions). Furthermore, a chest radiograph scan revealed that the
stent was successfully implanted in the trachea (Fig. 2).
Subsequently, the patient was scheduled for three
cycles of concurrent chemoradiotherapy and three cycles of
chemotherapy alone.
Results
Immunohistochemical analyses revealed that the tumor
was a poorly differentiated carcinoma with positive expression of
CK14 and P63 and negative expression of TTF-1 (thyroid
transcription factor-1) and SP-A (surfactant protein-A).
Subsequently, the patient was scheduled for concurrent
chemoradiotherapy. After two cycles of concurrent
chemoradiotherapy, a cervical CT scan revealed that the size of the
tumor was significantly reduced, the stent was open to maintain
patency of the lumen and there was no granulation tissue or other
abnormal lesions in the tracheal lumen (Fig. 3). Six months after surgery, a CT
scan showed that there were no tumor recurrences in the trachea
(Fig. 4).
To date, the patient has survived for ten months and
finished chemoradiotherapy. A CT scan showed that the thyroid tumor
appeared to be more localized and reduced, compared with the
previous CT scan (Fig. 5).
Bronchoscopic examination showed that the airway was smooth around
the endobronchial stent (Fig.
6).
Discussion
Poorly differentiated thyroid carcinoma is a group
of carcinomas that ranks between well-differentiated and anaplastic
thyroid carcinoma in terms of both morphological appearance and
biological behavior (1,2). An international panel of 12 thyroid
pathologists recommended a diagnostic algorithm (‘Turin Proposal
criteria’) on the basis of the interpretation of the WHO
classification and suggested a uniform approach to classify these
tumors. The Turin proposal algorithm defines poorly differentiated
carcinomas by the presence of a solid/trabecular/insular growth
pattern, absence of conventional nuclear features of papillary
carcinoma and the presence of at least one of the following
features: convoluted nuclei, mitotic activity greater than or equal
to 3/10 HPF or tumor necrosis (3).
Airway obstruction usually occurs secondary to
malignant cervical disease. In the case of an almost completely
occluded trachea, endotracheal intubation may be unexpectedly
difficult, which may result in catastrophic outcomes, including
cerebral anoxia and mortality. In the present study, due to the
massive tracheal invasion, the narrowest stenosis was 0.3 cm in
diameter and extended to the substernal area, so tracheotomy alone
may have been unable to relieve the breathing difficulties.
Suffocation may also have occurred when undergoing flexible
bronchoscopy. Therefore, proper evaluation and timely intervention
are decisive for such patients. Cardiopulmonary bypass has been
applied in cardiac and respiratory failure for a number of years.
Venous blood is removed from the body, oxygenated and then returned
to the body. In the field of malignant airway obstruction,
cardiopulmonary bypass has been used for the management of airway
in a few case reports. Sendasgupta et al (4) reported the successful management of a
patient with a large anterior mediastinal mass which compressed and
distorted the trachea through a femoro-femoral cardiopulmonary
procedure. In a patient with an aggressive thyroid papillary
carcinoma invading the trachea, curative surgery and reconstruction
were performed by cardiopulmonary bypass oxygenation (5). Tyagi et al reported that two
patients who presented with respiratory distress with cyanosis had
a pedunculated mass in the lower trachea above the carina, with
approximately 90% tracheal lumen obstruction. The two patients were
successfully managed with femoro-femoral cardiopulmonary bypass and
the airways were restored (5). As
described in the present study, cardiopulmonary bypass provides
adequate oxygen support to facilitate further appropriate treatment
in patients with massive tracheal invasion.
Tracheal resection and reconstruction with primary
anastomosis is considered to be the curative treatment for gross
intraluminal involvement of malignant tumors. However, the
indications are rigid: the glottis must be functional and patients
should not have severe pulmonary pathology (6). To avoid circumferential mobilization
of the trachea or larynx, a total of 5 to 6 cm of trahea may be
resected and primary reanastomosis performed (7). In the present study, as the tumor had
invaded a 5-cm stretch of the trachea and extended to the
substernal area, tracheal resection and reconstruction was not only
difficult but also dangerous. Tracheal stent implantation is an
effective palliative treatment for patients with malignant tracheal
obstruction, especially for inoperable patients (8–10). It
significantly relieves acute dyspnea caused by local tumor
compression or invasion and improves the quality of life of
patients. The stent may also function as a bridge until further
curative treatment may be administered. As expected, this patient’s
symptoms, including dyspnea and stridor, were significantly
relieved through the placing of a self-expanding metallic stent. At
present, the application of the non-membrane coated metallic stent
is somewhat controversial in malignant airway obstruction. Certain
experts consider that, unlike a covered stent, non-membrane coated
metallic stents are unable to hinder the overgrowth of granulation
tissue, leading to difficulties with intubation or ventilation
(11). However, others have
reported (8) that tumors do not
grow into the non-membrane coated metallic stent as easily as
expected, as, unlike the uncoated stent, the covered stent does not
compress the tumor. On the contrary, the non-membrane coated stent
results in the avascular necrosis of the tumor.
As the stent implantation keeps the respiratory
tract open, this provides time to undergo further management of the
tumor (10,12). Adjuvant therapy and/or chemotherapy
appear to be effective in patients with poorly differentiated
thyroid carcinoma. In particular, endoluminal brachytherapy may
reduce the risk of granulation tissue formation above and below the
mesh stents and neoplastic infiltration through the mesh into the
lumen (13). In the present study,
after two cycles of concurrent chemoradiotherapy, the size of the
tumor was significantly reduced, the stent was open to maintain the
patency of the lumen and there was no granulation tissue or other
abnormal lesions in the tracheal lumen.
In conclusion, for patients with serious tracheal
obstruction secondary to a malignant tumor, femoro-femoral
cardiopulmonary bypass provides adequate oxygen support to
facilitate further management, such as tumor resection or
chemoradiotherapy, so as to reduce or cure the tumor. Tracheal
stent implanting is an effective emergent measure to relieve
tracheal obstruction.
Acknowledgements
We thank Xuefen Wang, Department of
Pulmonary Medicine, and Liping Shi, Department of Extracorporeal
Crculation, The First Affiliated Hospital, Zhejiang University
College of Medicine for providing technological assistance.
References
|
1.
|
KN PatelAR ShahaPoorly differentiated and
anaplastic thyroid cancerCancer Control13119128200616735986
|
|
2.
|
EM Sanders JrVA LiVolsiJ BrierleyAn
evidence-based review of poorly differentiated thyroid cancerWorld
J Surg31934945200710.1007/s00268-007-9033-317431717
|
|
3.
|
M VolanteP ColliniYE NikiforovPoorly
differentiated thyroid carcinoma: the Turin proposal for the use of
uniform diagnostic criteria and an algorithmic diagnostic
approachAm J Surg
Pathol3112561264200710.1097/PAS.0b013e3180309e6a
|
|
4.
|
C SendasguptaG SenguptaK GhoshA MunshiA
GoswamiFemoro-femoral cardiopulmonary bypass for the resection of
an anterior mediastinal massIndian J
Anaesth54565568201010.4103/0019-5049.7264921224977
|
|
5.
|
I TyagiA GoyalR SyalSK AgarwalP
TewariEmergency cardiopulmonary bypass for impassable airwayJ
Laryngol Otol120687690200610.1017/S002221510600174516740200
|
|
6.
|
C PinsonneaultJ FortierF DonatiTracheal
resection and reconstructionCan J
Anaesth46439455199910.1007/BF0301294310349923
|
|
7.
|
DL PriceRJ WongGW RandolphInvasive thyroid
cancer: management of the trachea and esophagusOtolaryngol Clin
North Am4111551168ixx200810.1016/j.otc.2008.08.00219040976
|
|
8.
|
G MaDF WangQG SuTracheal stent
implantation for the treatment of tumor-induced acute airway
stenosisAi Zheng278518552008(In Chinese)
|
|
9.
|
RM MrozK KordeckiMD KozlowskiSevere
respiratory distress caused by central airway obstruction treated
with self-expandable metallic stentsJ Physiol Pharmacol59Suppl
6491497200819218673
|
|
10.
|
JH KimJH ShinHY SongPalliative treatment
of inoperable malignant tracheobronchial obstruction: temporary
stenting combined with radiation therapy and/or chemotherapyAJR Am
J Roentgenol193W3842200910.2214/AJR.08.2037
|
|
11.
|
N DavisBP MaddenA ShethAJ
Crerar-GilbertAirway management of patients with tracheobronchial
stentsBr J Anaesth96132135200610.1093/bja/aei26716257995
|
|
12.
|
A LemaireWR BurfeindE TolozaOutcomes of
tracheobronchial stents in patients with malignant airway
diseaseAnn Thorac Surg80434437discussion
437–438200510.1016/j.athoracsur.2005.02.07116039180
|
|
13.
|
R YerushalmiE FenigD ShitritEndobronchial
stent for malignant airway obstructionsIsr Med Assoc
J8615617200617058411
|