Introduction
Solitary fibrous tumors (SFTs) have been reportedly
observed mainly in the pleura but occurrences in urogenital
locations including the kidney, prostate and bladder have also been
been reported in recent years (1–4).
Solitary fibrous tumors arising in the kidney were first described
in 1996 by Gelb et al (2);
however, few cases, particularly those involving malignancy, have
been reported in the worldwide literature to date. We herein
describe a case of two malignant SFTs arising in one kidney and the
diagnosis which was made mainly based on characteristic histologic
findings and immunohistochemical features. We consider that this
study will play a significant role in guiding clinical practice on
the diagnosis and therapy of renal malignant solitary fibrous
tumors.
The study was approved by the ethics committee of
Second Hospital of Tianjin Medical University, Tianjin Institute of
Urology, Tianjin, China. Informed consent was obtained from the
patient prior to the study.
Case report
A 56-year-old man was admitted to the Second
Hospital of Tianjin Medical University complaining of shortness of
breath, weakness, hyperhidrosis and intermittent hypoglycemia of
1-year duration without gross hematuria or lumbago. Physical
examination revealed no obvious tenderness or percussion pain in
the renal regions. Laboratory examinations of routine blood and
urine tests revealed no abnormalities. Blood biochemistry including
renal and liver function tests were normal except for the blood
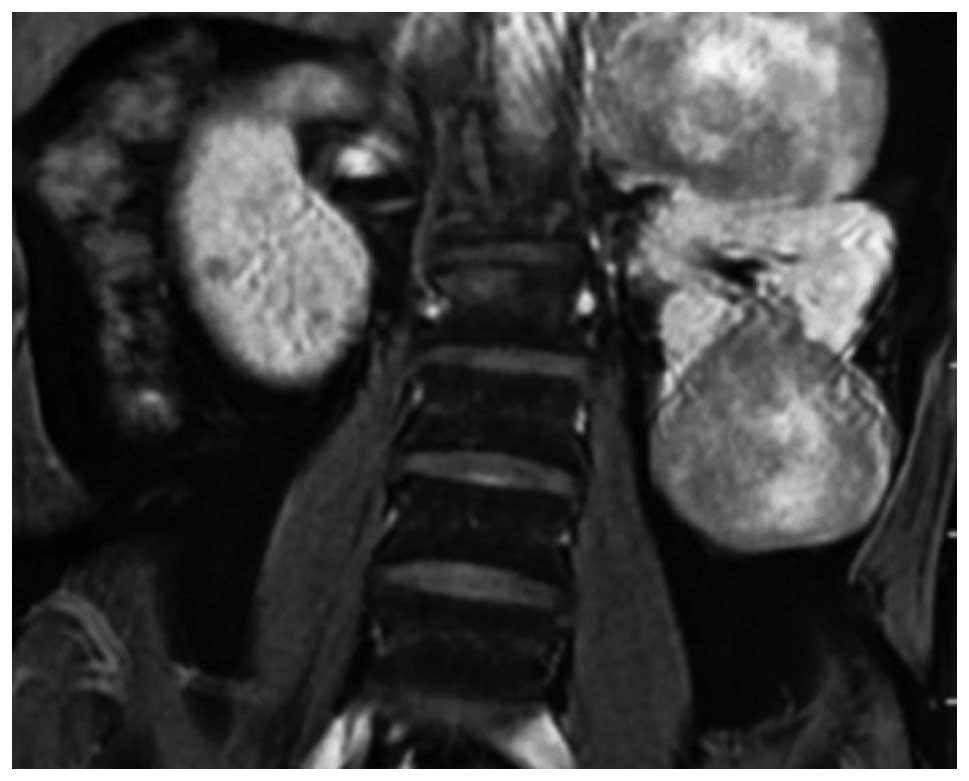
glucose concentration, which was 2.97 mmol/l. A computed tomography
scan revealed the presence of two renal masses presenting as soft
tissues in the upper and lower pole of the left kidney, measuring
10x8x7 cm and 10x7x7 cm, respectively. The lesions presented with
an inhomogeneous density and had no clear boundary, and exhibited
slight peripheral enhancement with contrast medium; however, the
center enhanced unequally. Magnetic resonance imaging also revealed
two renal masses in the upper and lower pole of the left kidney,
which presented as elliptical and inhomogeneous densities (Fig. 1).
An initial diagnosis of space-occupying lesions of
the left kidney was given (with suspicions of renal cell carcinoma)
and subsequently, the patient underwent left radical nephrectomy.
Surgery revealed two masses in the upper and lower pole, with the
lower mass showing no clear boundary with the kidney. The cut
surface of the tumors was grey to white and crisp in texture with
local hemorrhage and necrosis.
Microscopically, both tumors had a similar
histological appearance, consisting of ovoid or spindle cells
arranged as bundles, swirls or irregularities. Partial focal areas
containing vessels were present, which had a
hemangiopericytoma-like pattern. Certain areas in the tumors
(particularly the lower one) demonstrated increased cells and
cellular atypia and mitotic figures were also focally observed
(more than 4 per 10 high-power fields). The edge of the mass
demonstrated infiltrating growth, and certain areas revealed
hemorrhage and/or necrosis (Fig.
2). Immunohistochemically, the tumor cells were positive for
CD34, vimentin and CD99 (Fig. 3).
Staining for cytokeratin, α-smooth muscle actin (α-SMA) and S-100
was negative.
Accordingly, a pathological diagnosis of malignant
solitary fibrous tumor of the left kidney (low-grade malignancy)
was established based on the microscopic features and the
immunohistochemical findings.
A postoperative follow-up of 10 months revealed no
signs of tumor recurrence or metastasis and the hypoglycemia was
resolved with the removal of the tumors.
Discussion
Solitary fibrous tumors arising in the kidney were
first described in 1996 by Gelb et al (2). The majority of renal SFTs are observed
in adults in a wide age range (18–85); however, one pediatric case
has been reported in a 4-year-old boy (5). In general, SFTs are slow-growing
tumors with a favorable prognosis, although there have been some
malignant cases (6).
Symptoms of SFTs usually do not differ from those
reported by patients with renal cell carcinoma, which include flank
or abdominal pain and/or gross hematuria. In certain patients, the
tumor is found incidentally and in others the mass is palpable
(2,6). Non islet-cell hypoglycemia (Doege
Potter syndrome) arises due to the production of high molecular
weight insulin-like growth factors and is a frequently associated
paraneoplastic syndrome, which may have malignant behavior or poor
survival from diagnosis (7). In our
case, the patient had symptoms of hypoglycemia; however, it was
resolved with the removal of the neoplasm suggesting it was the
result of a paraneoplastic syndrome.
Macroscopically, renal SFTs are usually single;
however, this was not observed in the present case. Occasionally,
myxoid and pseudocapsules are also present. The size of the tumors
is usually between 2.0 and 25.0 cm. The majority of cases are
without cystic, hemorrhagic or necrotic changes which may be
malignant (6). Microscopically,
SFTs of the kidney are pathologically characterized by spindle cell
proliferation showing a patternless architecture with a combination
of alternating hypocellular and hypercellular areas. Furthermore,
SFTs are tumors with variable cellularity and are composed of a
mixture of haphazard, storiform, short fascicular arrangements of
bland spindle cells and collagenous bands. They are highly vascular
tumors, with hemangiopericytoma-like patterns observed in certain
areas. Myxoid changes and fibrosis may also be observed (6,8,9).
Immunohistochemical study is key to diagnosis.
Although it is not specific to SFTs, CD34 immunoreactivity has been
reported to be diffusely expressed in many cases of SFTs, thus
strong CD34 reactivity is currently regarded as the most prominent
characteristic and indispensable finding to aid diagnosis (2–4,8–10).
In addition, a positive expression of bcl-2, vimentin and CD99 is
also present in the majority of SFTs; however, cytokeratin,
α-smooth muscle actin (α-SMA) and S-100 are usually absent
(2–4,8–10).
The majority of SFTs are benign; however, a few have
revealed histologically malignant features. The criteria for
malignant SFTs, first proposed by England et al (10) in 1989, include increased cellularity
with crowded/overlapping nuclei, cellular pleomorphism and a
mitotic count of more than 4 per 10 high-power fields. However, in
spite of cytologic malignancy in SFTs, the clinical outcome is not
always poor (10). In the present
case, the majority of areas in the tumors (particularly the lower
one) demonstrated increase cell density and cellular atypia, and
mitotic figures were more than 4 per 10 high-power fields. The edge
of the masses showed infiltrating growth and certain areas revealed
hemorrhage or necrosis. Accordingly, the diagnosis was confirmed as
malignant.
Solitary fibrous tumors should be distinguished from
benign and malignant spindle cell tumors of the kidney.
Inflammatory myofibroblastic tumors are characterized by spindle
cells in an edematous background with blood vessels and
inflammation consisting of lymphocytes and plasma cells.
Furthermore, a mixture of spindle cells and collagenization with
CD34 reactivity differentiates SFTs from inflammatory
myofibroblastic tumors. Fibromas are small tumors that do not react
with CD34. Leiomyoma can be excluded by the lack of expression of
muscle markers. The absence of smooth muscle and adipose tissue
components, with the aid of HMB-45 immunonegativity, distinguishes
SFT from angiomyolipoma. It is occasionally difficult to
differentiate hemangiopericytoma from SFT; however, the presence of
spindle cell cytological features, various growth patterns with
alternating hypocellular and hypercellular areas and abundant
collagenization favors a diagnosis of SFTs. Solitary fibrous tumors
may also be differentiated from leiomyosarcoma, malignant nerve
sheath tumors, sarcomatoid renal and transitional cell carcinoma by
the absence of dense cellularity, severe atypia, high mitotic rates
and with the help of immunohistochemical staining of these tumors
for α-smooth muscle actin, S-100 and cytokeratin (8).
Surgery is considered the first choice of treatment
if possible. The use of chemotherapy is reserved for metastatic or
symptomatic non-resectable SFTs; however, there are still no
standard chemotherapeutic indications or regimens. The relatively
effective drugs appear to be those which are commonly used in soft
tissue sarcomas even though SFTs are considered chemoresistant
(11,12). Radiation therapy is of some benefit,
when applicable, given in combination with chemotherapy (13). The novel targeted drug imatinib
mesilate, which exerts some activity on SFTs expressing the
wild-type PDGFR-β, has recently been reported (14,15).
The prognosis is generally good for SFTs and the
majority are non-recurring and non-metastazing tumors. It is
estimated that 10 to 15% of intrathoracic SFTs and 10% of
extrathoracic SFTs will recur and/or metastasize (16,17),
therefore SFT is regarded as an ‘intermediate malignant, rarely
metastasizing neoplasm’ (18). Poor
prognosis of SFTs may occur when there is incomplete resection, a
large size (>10 cm), presence of malignant cellularity or they
are located outside the thoracic cavity. An additional factor
conferring a worse prognosis in SFTs is dedifferentiation or
sarcomatous overgrowth, which represents an abrupt transition to a
morphologically anaplastic component (19). In the present case, a postoperative
follow-up of 10 months revealed no recurrence or metastasis.
Nevertheless, long-term follow-up is indispensable since metastases
may still occur after several years.
To summarize, we presented a case of two malignant
SFTs in one kidney with characteristic clinicopathological
features. Although malignant SFTs in extrapleural sites remain
extremely uncommon, it is indispensable to consider this
possibility when renal spindle cell tumors are encountered. In view
of characteristic findings which are often not observed in imaging
studies including CT and MRI, the histologic features and
immunohistochemical staining for CD34, CD99, bcl-2 and vimentin may
be helpful in confirming the diagnosis of malignant SFTs of the
kidney.
References
|
1.
|
L RobinsonSolitary fibrous tumor of
pleuraCancer Control13264269200617075563
|
|
2.
|
A GelbM SimmonsN WeidnerSolitary fibrous
tumor involving the renal capsuleAm J Surg
Pathol2012881295199610.1097/00000478-199610000-000168827037
|
|
3.
|
M MarziP PiraM D’AlpaosA PaiuscoS
CanessaMS MinerviniP Di ZittiThe solitary fibrous malignant tumor
of the kidney: clinical and pathological considerations on a case
revisiting the literatureMinerva Urol
Nefrol63109113201121336250
|
|
4.
|
H TalvitieK AströmO LarssonSolitary
fibrous tumor of the prostate: A report of two casesPathol
Int61536538201110.1111/j.1440-1827.2011.02696.x21884303
|
|
5.
|
N FerrariL NieldFinal diagnosis: solitary
fibrous tumor of the kidneyClin Pediatr
(Phila)45871873200617080561
|
|
6.
|
SW FineDM McCarthyTY ChanMalignant
solitary fibrous tumor of the kidney: report of a case and
comprehensive review of the literatureArch Pathol Lab
Med130857861200616740040
|
|
7.
|
B HerrmannB SallerW KiessK MorgenrothK
DrochnerT SchröderPrimary malignant fibrous histiocytoma of the
lung: IGF-II producing tumor induces fasting hypoglycaemiaExp Clin
Endocr Diab108515518200010.1055/s-2000-1100711149628
|
|
8.
|
G MagroV CavallaroA TorrisiM LopesM
Dell’AlbaniS LanzafameIntrarenal solitary fibrous tumor of the
kidney report of a case with emphasis on the differential diagnosis
in the wide spectrum of monomorphous spindle cell tumors of the
kidneyPathol Res
Pract1983743200210.1016/S0344-0338(04)70182-X11866209
|
|
9.
|
T YazakiS SatohT IizumiT UmedaY
YamaguchiSolitary fibrous tumor of renal pelvisInt J
Urol8504508200110.1046/j.1442-2042.2001.00360.x11683972
|
|
10.
|
D EnglandL HochholzerM McCarthyLocalized
benign and malignant fibrous tumors of the pleura: a
clinicopathologic review of 223 casesAm J Surg
Pathol13640658198910.1097/00000478-198908000-000032665534
|
|
11.
|
SR GrobmyerRG MakiGD DemetriM MazumdarE
RiedelMF BrennanNeo-adjuvant chemotherapy for primary high-grade
extremity soft tissue sarcomaAnn
Oncol1516671672200410.1093/annonc/mdh43115520069
|
|
12.
|
GD DemetriS AntoniaRS BenjaminNCCN
Clinical Practice Guidelines in Oncology: Soft Tissue Sarcoma-V.
22009
|
|
13.
|
J De BoerPL JagerT WiggersP NieboerWAN
MachteldE PrasThe therapeutic challenge of a nonresectable solitary
fibrous tumor in a hypoglycemic patientInt J Clin
Oncol11478481200617180519
|
|
14.
|
M PrunottoM BoscoL DanieleL Macri’L
BonelloL SchirosiImatinib inhibits in vitro proliferation of cells
derived from a pleural solitary fibrous tumor expressing
platelet-derived growth factor receptor-betaLung
Cancer64244246200910.1016/j.lungcan.2008.10.013
|
|
15.
|
T De PasF ToffalorioP ColomboG TrifiròG
PelosiPD VignaBrief report: activity of imatinib in a patient with
platelet-derived-growth-factor receptor positive malignant solitary
fibrous tumor of the pleuraJ Thorac Oncol3938941200818670317
|
|
16.
|
SW WeissJR GoldblumSoft tissue tumors of
intermediate malignancy of uncertain typeSoft Tissue Tumor5th
editionMosby ElsevierPhiladephia109311602008
|
|
17.
|
AV Vallat-DecouvelaereSM DryCD
FletcherAtypical and malignant solitary fibrous tumors in
extrathoracic locations: evidence of their comparability to
intra-thoracic tumorsAm J Surg
Pathol2215011511199810.1097/00000478-199812000-00007
|
|
18.
|
LFJ GuillouCDM FletcherN
MandahiExtrapleural solitary fibrous tumour and
hemangiopericytomaWorld Health Organization Classification of
Tumours: Pathology and Genetics of Tumours of Soft Tissue and Bone.
Fletcher. CDMKK UnniF MertensIARC PressLyon86902002
|
|
19.
|
JM MosqueraCD FletcherExpanding the
spectrum of malignant progression in solitary fibrous tumors: a
study of 8 cases with a discrete anaplastic component - is this
dedifferentiated SFT?Am J Surg
Pathol3313141321200910.1097/PAS.0b013e3181a6cd3319718788
|