Introduction
Endometrial cancer is showing rapid increases in
mortality and incidence in Japan (1). Previous clinicopathological studies
have shown that poor prognosis of endometrial cancer is associated
with the histological grade of the tumour, presence of malignant
cells in ascites or the washing of specimens for cytology, cervical
invasion of malignant cells, deep myometrial invasion of malignant
cells, lymph node metastasis and involvement of malignant cells in
the lymphovascular space (2–4).
Obesity is a well-established risk factor associated
with several types of cancer, including endometrial cancer
(5–8). The factor linking obesity to
endometrial cancer appears to be excessive exposure to various
factors produced by adipose tissue. Adipose tissue is a source of
oestrogen, insulin and insulin-like growth factors, all of which
are considered to be involved in endometrial tumourigenesis
(9,10). In addition to these factors, adipose
tissues produce various bioactive hormones called adipokines, the
most prominent of which are leptin and adiponectin. These may
significantly influence the growth and proliferation of tumours
(11–13).
Leptin, a product of the obese (Ob) gene, is
produced predominantly in adipose tissue and expressed in normal
tissues and malignant breast tissues (14–16).
Expression of leptin and leptin receptor (ObR) is more frequent in
carcinoma than in normal tissue (17,18).
Leptin is involved in a variety of functions, including appetite
regulation, bone formation, reproduction and angiogenesis (19), and may affect processes associated
with cancer initiation and progression, resulting in the
development of metastases (15,17,20,21).
Leptin acts through ObR, which is encoded by the Ob gene. Binding
of leptin to ObR activates the Janus kinase (JAK)/signal transducer
and activator of transcription signalling pathway and induction of
JAK stimulates phosphoinositol-3-kinase (PI3-kinase). Activation of
PI3-kinase increases cell migration and invasion via the Rac/Rho
pathways and stimulates the major growth and survival Akt pathway
(13).
Adiponectin is an additional type of adipocytokine,
predominantly secreted by adipocytes (12). In contrast to other adipocytokines,
adiponectin levels correlate inversely with central fat
accumulation (22). Adiponectin may
exert antineoplastic activity through suppression of tumour
proliferation and neoangiogenesis, and through induction of
apoptosis (23–25). In addition, an inverse correlation
has been found between plasma adiponectin levels and the
histological grade of endometrial cancer (26). However, the precise effects of
adiponectin in endometrial cancer remain unclear. In total, two
adiponectin receptors (AdipoR-1 and AdipoR-2) have been identified
and in vitro studies have shown that the two AdipoR genes
are expressed in human monocytes, macrophages, adipocytes, vascular
smooth muscles, a primary osteoblast cell line, pancreatic cells
and other cell types (27–30). Previous in vivo studies have
shown that AdipoR-1 is abundantly expressed in skeletal muscle and
the liver, whereas AdipoR-2 is predominantly expressed in the
liver. Additionally, AdipoR-1 in the liver activates AMP-activated
protein kinase pathways, while AdipoR-2 activates peroxisome
proliferator-activated receptor pathways (27,31,32).
In addition, expression of AdipoR has previously been documented in
several human cancer cell lines (33,34).
The aim of the present study was to determine
whether the immunohistochemical expression of AdipoR-1, AdipoR-2 or
ObR correlates with the clinicopathological manifestations and
clinical outcomes of endometrial carcinoma patients.
Materials and methods
Clinical samples
Formalin-fixed, paraffin-embedded tumour tissues
were obtained from 77 patients with endometrioid adenocarcinoma of
the endometrium. All patients attended the Gynaecology Clinic at
the Aichi Medical University Hospital (Nagakute, Japan) and were
diagnosed with endometrial endometrioid adenocarcinoma based on
post-surgical assessment. Clinicopathological characteristics of
the patients are shown in Table I.
Normal endometrial tissue was also obtained from 19 patients with
benign uterine disease (uterine leiomyoma, n=12; and uterine
prolapse, n=7). All study protocols were approved by the regional
ethics committee of the Aichi Medical University, School of
Medicine (Nagakute, Japan). Written informed consent was obtained
from all participants prior to study enrolment.
 | Table ICharacteristics of 77 patients with
endometrioid adenocarcinoma of the endometrium. |
Table I
Characteristics of 77 patients with
endometrioid adenocarcinoma of the endometrium.
| Characteristics | n |
|---|
| Stage |
| IA | 30 |
| IB | 23 |
| II | 9 |
| IIIA | 2 |
| IIIC | 13 |
| Grade |
| G1 | 39 |
| G2 | 22 |
| G3 | 16 |
| Myometrial
invasion |
| <1/2 | 38 |
| ≥1/2 | 39 |
| Cervical stromal
invasion |
| Negative | 59 |
| Positive | 18 |
| Adnexal
invasion |
| Negative | 69 |
| Positive | 8 |
| Lymphovascular
space involvement |
| Negative | 52 |
| Positive | 25 |
| Lymph node
metastasis |
| Negative | 65 |
| Positive | 12 |
| Peritoneal
cytology |
| Negative | 61 |
| Positive | 16 |
| Body mass index,
kg/m2 |
| <25 | 45 |
| ≥25 to <30 | 16 |
| ≥30 to <35 | 9 |
| ≥35 | 7 |
| Adjuvant
therapy |
| None | 26 |
| Radiotherapy | 12 |
| Chemotherapy | 39 |
| AP | 9 |
| TJ | 30 |
| Age, years (mean ±
SD) | 56.91±9.98 |
Immunohistochemistry
The prepared 3-μm sections were deparaffinised and
rehydrated. Following microwave processing for 25 min in 10 mM
citrate buffer (pH 6.0), sections were incubated for 30 min in
methanol containing 0.5% H2O2. Following
incubation in normal goat serum for 1 h at room temperature to
block non-specific staining, slides were incubated overnight with
the primary antibodies at 4°C. The primary antibodies used were
rabbit anti-human AdipoR-1 (raised against amino acid residues
357–375) antiserum, rabbit anti-human AdipoR-2 (raised against
amino acid residues 374–386) antiserum (both purchased from Phoenix
Pharmaceuticals, Burlingame, CA, USA) and rabbit anti-human ObR
(raised against amino acid residues 541–840) antiserum (Santa Cruz
Biotechnology, Inc., Santa Cruz, CA, USA), used at dilutions of
1:500, 1:200 and 1:200, respectively. Anti-rabbit antibody-labelled
polymer horseradish peroxidase (ChemMate Envision kit; Dako Japan,
Kyoto, Japan) was used as the secondary antibody, applied for 30
min at room temperature. The horseradish peroxidase reaction was
developed with 3,3′-diaminobenzidine tetrahydrochloride (Katayama
Chemical Industries Co. Ltd., Osaka, Japan)and sections were
counterstained with haematoxylin (Katayama Chemical Industries Co.
Ltd.) for microscopic examination (Olympus BX50, Olympus Corp.,
Tokyo, Japan). Sections were defined as showing positive expression
when >50% of tumour cells were intensely stained.
Statistical analysis
The statistical significance of differences among
different categories of expression was analysed using the
χ2 test and two-way analysis of variance.
Progression-free and overall survival were analysed using the
Kaplan-Meier method and log-rank test, and the potential
significance of multiple prognostic factors for progression-free
and overall survival were analysed by the Cox proportional hazard
regression test. P<0.05 was considered to indicate a
statistically significant difference.
Results
AdipoR-1, AdipoR-2 and ObR
localisation
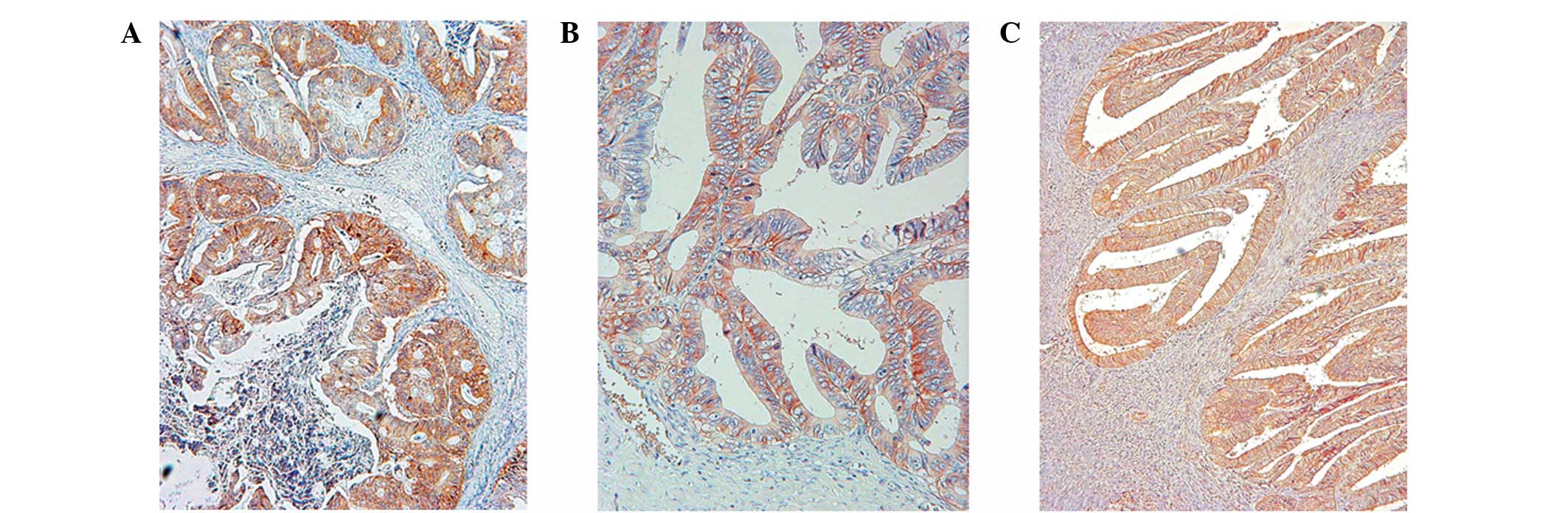
AdipoR-1, AdipoR-2 and ObR were localised
predominantly to the cell membrane and cytoplasm of tumour cells
(Fig. 1). In normal endometrial
tissue, the expression of AdipoR-1, AdipoR-2 and ObR was identified
in endometrial glandular cells, in the proliferative and secretory
phases. Expression of AdipoR-1 was found in nine of the 10
proliferative-phase specimens and in all nine secretory-phase
specimens. In addition, the expression of AdipoR-2 and ObR were
found in all 10 proliferative-phase and nine secretory-phase
specimens.
AdipoR-1, AdipoR-2 and ObR
expression
In the 77 endometrial cancer cases, positive
expression was observed in 46 cases (59.7%) for AdipoR-1, 47 cases
(61.0%) for AdipoR-2 and 33 cases (42.9%) for ObR. Expression of
AdipoR-1 was observed most in stage I cases versus stage II or III
cases, G1 tumours versus G2 or G3 tumours, tumours with shallow
myometrial invasion versus tumours with deep myometrial invasion,
tumours with negative lymphovascular space involvement versus
tumours with positive lymphovascular space involvement, cases with
negative adnexal invasion versus cases with positive adnexal
invasion and cases with negative lymph node metastasis versus cases
with positive lymph node metastasis. Conversely, cervical stromal
invasion, peritoneal cytology and body mass index exhibited no
correlation with AdipoR-1 expression (Table II). However, expression of AdipoR-2
appeared unrelated to any clinicopathological factors and
expression of ObR was unrelated to any factors other than tumour
grade.
| Table IIClinicopathological characteristics
in relation to the immunohistochemical expression of AdipoR-1,
AdipoR-2 and ObR in tumours obtained from 77 patients with
endometrial carcinoma. |
Table II
Clinicopathological characteristics
in relation to the immunohistochemical expression of AdipoR-1,
AdipoR-2 and ObR in tumours obtained from 77 patients with
endometrial carcinoma.
| Clinicopathological
characteristics | n | AdipoR-1, n
(%) | AdipoR-2, n
(%) | ObR, n (%) |
|---|
| Stage |
| IA | 30 | 23 (76.7) | 18 (60.0) | 10 (33.3) |
| IB | 23 | 14 (60.9) | 14 (60.9) | 13 (56.5) |
| II | 9 | 6 (66.7) | 6 (66.7) | 4 (44.4) |
| IIIA | 2 | 0 (0.0) | 2 (100) | 0 (0.0) |
| IIIC | 13 | 3 (23.1) | 7 (53.8) | 6 (46.2) |
| | P=0.0073 | P=0.7920 | P=0.3507 |
| Grade |
| G1 | 39 | 34 (87.2) | 27 (69.2) | 18 (46.2) |
| G2 | 22 | 10 (45.5) | 14 (63.6) | 13 (59.1) |
| G3 | 16 | 2 (12.5) | 6 (37.5) | 2 (12.5) |
| | P<0.0001 | P=0.0867 | P=0.0138 |
| Myometrial
invasion |
| <1/2 | 38 | 29 (76.3) | 24 (63.2) | 14 (36.8) |
| ≥1/2 | 39 | 17 (43.6) | 23 (59.0) | 19 (48.7) |
| | P=0.0051 | P=0.8162 | P=0.3594 |
| Cervical stromal
invasion |
| Negative | 59 | 38 (64.4) | 35 (59.3) | 25 (42.4) |
| Positive | 18 | 8 (44.4) | 12 (66.7) | 8 (44.4) |
| | P=0.1720 | P=0.7831 | P=0.8765 |
| Adnexal
invasion |
| Negative | 69 | 46 (66.7) | 42 (60.9) | 31 (44.9) |
| Positive | 8 | 0 (0.0) | 5 (62.5) | 2 (25.0) |
| | P=0.0004 | P=0.9287 | P=0.4544 |
| Lymphovascular
space involvement |
| Negative | 52 | 39 (75.0) | 35 (67.3) | 25 (48.1) |
| Positive | 25 | 7 (28.0) | 12 (48.0) | 8 (32.0) |
| | P=0.0001 | P=0.1360 | P=0.2235 |
| Lymph node
metastasis |
| Negative | 65 | 44 (67.7) | 41 (63.1) | 27 (41.5) |
| Positive | 12 | 2 (29.2) | 6 (50.0) | 6 (50.0) |
| | P=0.0024 | P=0.5216 | P=0.7526 |
| Peritoneal
cytology |
| Negative | 61 | 37 (60.7) | 36 (59.0) | 27 (44.3) |
| Positive | 16 | 9 (56.3) | 11 (68.8) | 6 (37.5) |
| | P=0.7805 | P=0.5722 | P=0.7785 |
| BMI,
kg/m2 |
| <25 | 45 | 27 (60) | 29 (64.4) | 20 (44.4) |
| ≥25 | 32 | 19 (59.4) | 18 (56.3) | 13 (40.6) |
| | P=0.9560 | P=0.4872 | P=0.8172 |
| Total | 77 | 46 (59.7) | 47 (61.0) | 33 (42.9) |
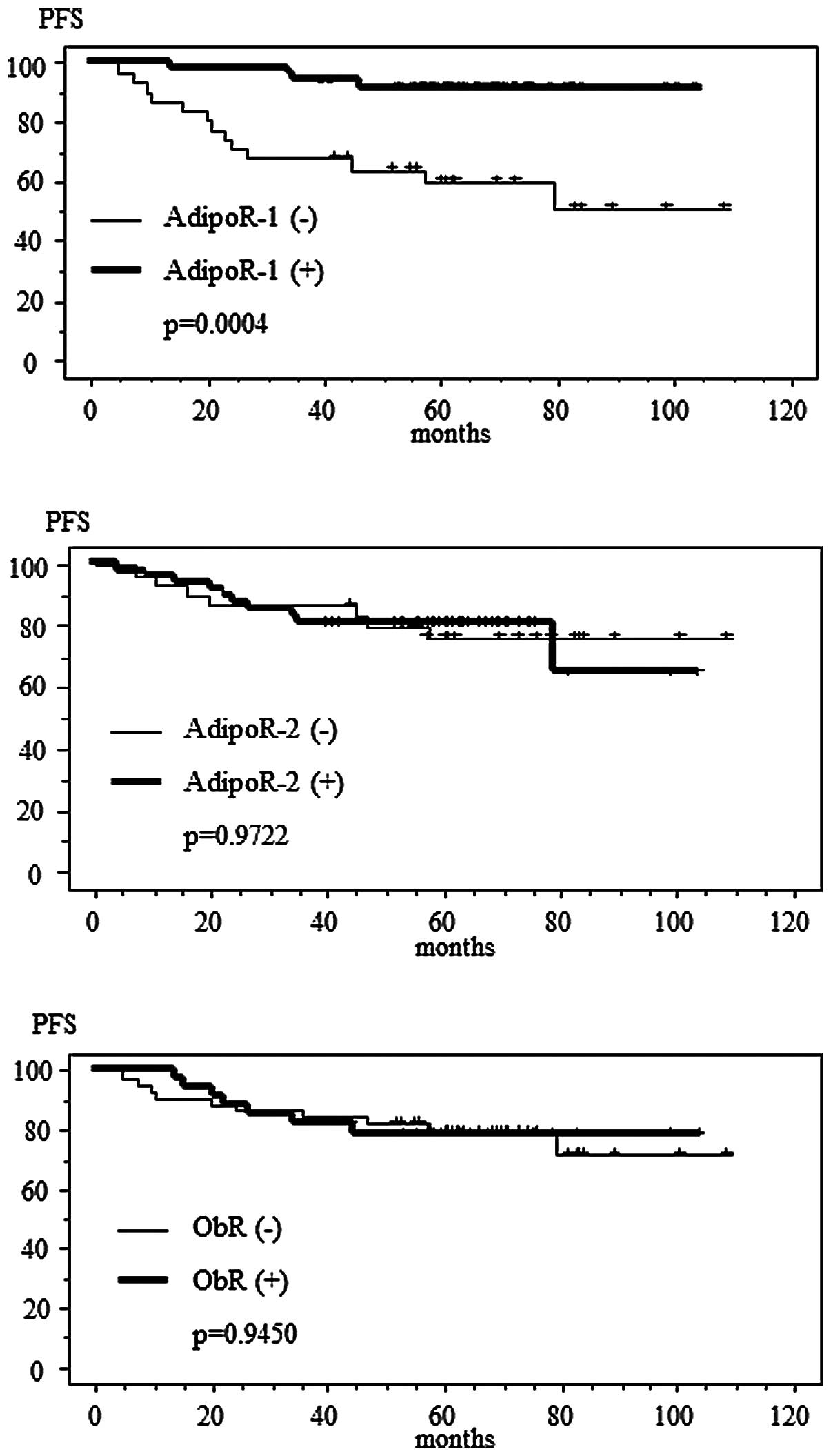
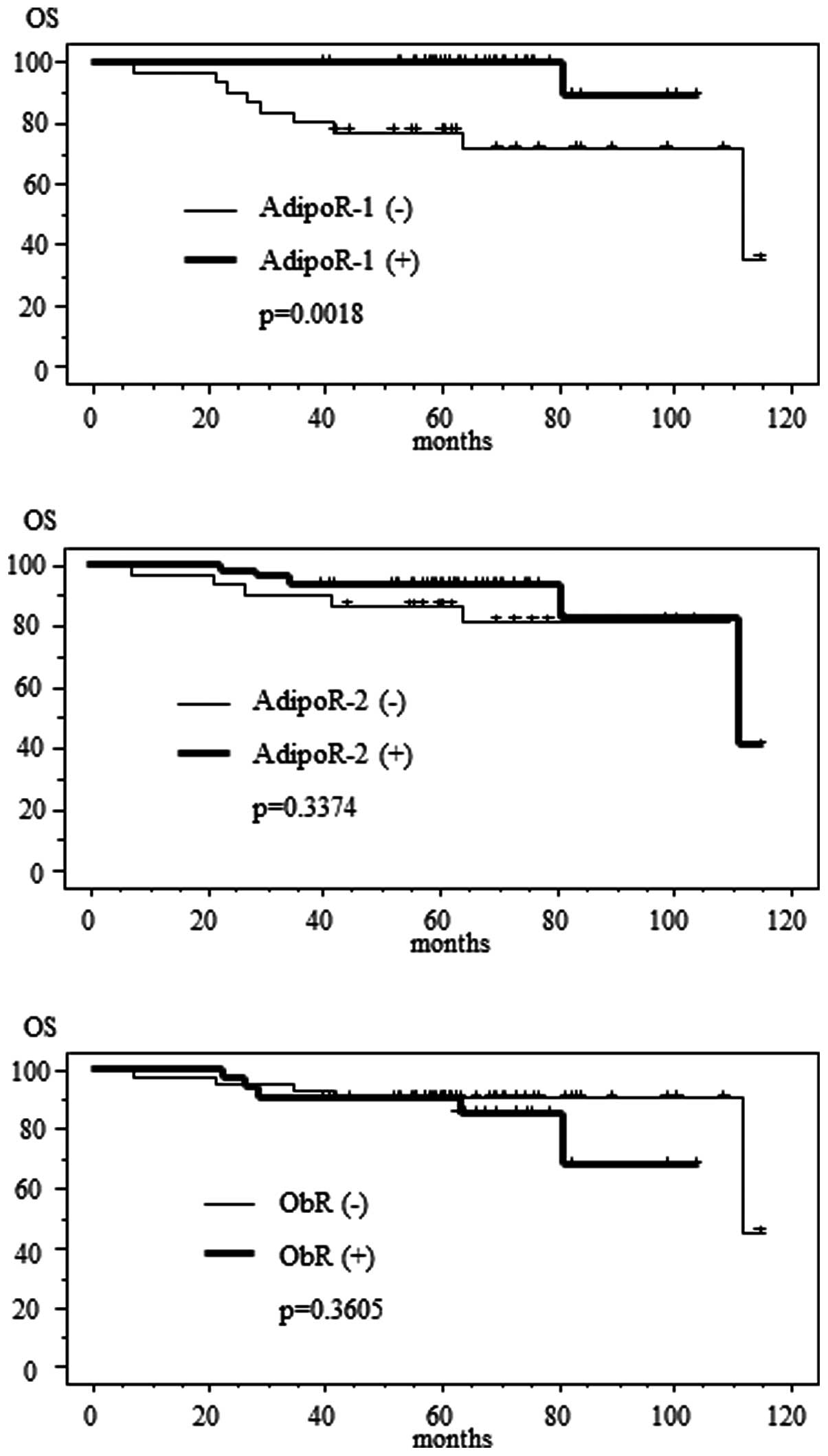
Survival rates
In the Kaplan-Meier analyses, progression-free and
overall survival times were longer in cases with positive AdipoR-1
expression compared with negative AdipoR-1 expression, while
survival time did not show any correlation with AdipoR-2 or ObR
expression (Figs. 2 and 3; Tables
III and IV).
| Table IIIUni- and multivariate analyses of
variables associated with progression-free survival using the
Kaplan-Meier method with log-rank test, logistic regression model
and Cox proportional hazard model. |
Table III
Uni- and multivariate analyses of
variables associated with progression-free survival using the
Kaplan-Meier method with log-rank test, logistic regression model
and Cox proportional hazard model.
| | Kaplan-Meier
method | Univariate
analysis | Multivariate
analysis |
|---|
| |
|
|
|
|---|
| Variables | n | Five-year survival
rate, % | P-value | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Stage | | | | | | | | | |
| I | 53 | 92.10 | <0.0001 | −1.012 | 0.218–0.608 | 0.0001 | −0.554 | 0.130–2.540 | 0.4648 |
| II/III | 24 | 49.20 | | | | | | | |
| Grade | | | | | | | | | |
| G1/G2 | 61 | 88.50 | <0.0001 | −1.934 | 0.055–0.381 | <0.0001 | −0.124 | 0.397–1.967 | 0.7615 |
| G3 | 16 | 43.80 | | | | | | | |
| Myometrial
invasion | | | | | | | | | |
| <1/2 | 38 | 92.10 | 0.004 | −1.642 | 0.056–0.675 | 0.0099 | 0.302 | 0.675–2.708 | 0.394 |
| ≤1/2 | 39 | 66.20 | | | | | | | |
| Cervical stromal
invasion | | | | | | | | | |
| Negative | 59 | 87.80 | 0.00001 | −1.724 | 0.066–0.483 | 0.0007 | −0.457 | 0.222–1.808 | 0.3932 |
| Positive | 18 | 48.60 | | | | | | | |
| Adnexal
invasion | | | | | | | | | |
| Negative | 69 | 86.50 | <0.0001 | −2.957 | 0.017–0.154 | <0.0001 | −2.086 | 0.030–0.508 | 0.0037 |
| Positive | 8 | 12.50 | | | | | | | |
| Lymphovascular
space involvement | | | | | | | | | |
| Negative | 52 | 85.90 | 0.0216 | −1.067 | 0.133–0.893 | 0.0283 | −0.005 | 0.495–1.998 | 0.9881 |
| Positive | 25 | 63.80 | | | | | | | |
| Lymph node
metastasis | | | | | | | | | |
| Negative | 65 | 90.40 | <0.0001 | −2.921 | 0.018–0.157 | <0.0001 | −1.953 | 0.040–0.509 | 0.0027 |
| Positive | 12 | 12.50 | | | | | | | |
| Peritoneal
cytology | | | | | | | | | |
| Negative | 61 | 81.60 | 0.237 | −0.623 | 0.188–1.531 | 0.2445 | 0.635 | 0.605–5.886 | 0.2741 |
| Positive | 16 | 67.50 | | | | | | | |
| AdipoR-1
expression | | | | | | | | | |
| Negative | 31 | 59.90 | 0.0004 | 1.780 | 1.928–18.246 | 0.0019 | −0.068 | 0.454–1.921 | 0.8525 |
| Positive | 46 | 91.20 | | | | | | | |
| AdipoR-2
expression | | | | | | | | | |
| Negative | 30 | 75.90 | 0.9722 | 0.017 | 0.384–2.697 | 0.9722 | −0.363 | 0.361–1.340 | 0.2779 |
| Positive | 47 | 80.90 | | | | | | | |
| ObR expression | | | | | | | | | |
| Negative | 44 | 79.20 | 0.945 | 0.034 | 0.393–2.723 | 0.945 | −0.218 | 0.409–1.580 | 0.5273 |
| Positive | 33 | 78.30 | | | | | | | |
| BMI,
kg/m2 | | | | | | | | | |
| <25 | 45 | 82.20 | 0.3527 | 0.126 | 0.716–1.797 | 0.5907 | −0.069 | 0.570–1.529 | 0.7834 |
| ≥25 | 32 | 74.00 | | | | | | | |
| Age, years | | | | | | | | | |
| <60 | 45 | 79.50 | 0.9015 | −0.042 | 0.606–1.516 | 0.8567 | 0.083 | 0.549–2.151 | 0.8121 |
| Table IVUni- and multivariate analyses of
variables associated with overall survival using the Kaplan-Meier
method with log-rank test, logistic regression model and Cox
proportional hazard model. |
Table IV
Uni- and multivariate analyses of
variables associated with overall survival using the Kaplan-Meier
method with log-rank test, logistic regression model and Cox
proportional hazard model.
| | Kaplan-Meier
method | Univariate
analysis | Multivariate
analysis |
|---|
| |
|
|
|
|---|
| Variables | n | Five-year survival
rate, % | P-value | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Stage | | | | | | | | | |
| I | 53 | 100 | <0.0001 | −0.894 | 0.244–0.687 | 0.0007 | −0.871 | 0.097–1.808 | 0.2431 |
| II/III | 24 | 70.80 | | | | | | | |
| Grade | | | | | | | | | |
| G1/G2 | 61 | 95.1 | 0.0101 | −1.575 | 0.055–0.777 | 0.0196 | 0.655 | 0.838–4.422 | 0.1228 |
| G3 | 16 | 75.0 | | | | | | | |
| Myometrial
invasion | | | | | | | | | |
| <1/2 | 38 | 100 | 0.0177 | −2.106 | 0.015–0.974 | 0.0472 | 0.208 | 0.616–2.461 | 0.5566 |
| ≥1/2 | 39 | 82.10 | | | | | | | |
| Cervical stromal
invasion | | | | | | | | | |
| Negative | 59 | 94.90 | 0.0078 | −1.653 | 0.049–0.741 | 0.0166 | 0.837 | 0.748–7.123 | 0.1454 |
| Positive | 18 | 77.80 | | | | | | | |
| Adnexal
invasion | | | | | | | | | |
| Negative | 69 | 98.60 | <0.0001 | −3.867 | 0.004–0.108 | <0.0001 | −2.266 | 0.032–0.340 | 0.0002 |
| Positive | 8 | 25.0 | | | | | | | |
| Lymphovascular
space involvement | | | | | | | | | |
| Negative | 52 | 96.20 | 0.0607 | −1.156 | 0.088–1.125 | 0.0752 | 0.192 | 0.577–2.545 | 0.6125 |
| Positive | 25 | 80.0 | | | | | | | |
| Lymph node
metastasis | | | | | | | | | |
| Negative | 65 | 100 | <0.0001 | −4.510 | 0.001–0.093 | <0.0001 | −1.193 | 0.107–0.860 | 0.0248 |
| Positive | 12 | 41.70 | | | | | | | |
| Peritoneal
cytology | | | | | | | | | |
| Negative | 61 | 93.40 | 0.0368 | −1.313 | 0.072–1.009 | 0.0515 | −0.109 | 0.332–2.425 | 0.8306 |
| Positive | 16 | 81.30 | | | | | | | |
| AdipoR-1
expression | | | | | | | | | |
| Negative | 31 | 77.40 | 0.0018 | 2.565 | 1.620–10.427 | 0.0158 | 0.026 | 0.478–2.202 | 0.947 |
| Positive | 46 | 100 | | | | | | | |
| AdipoR-2
expression | | | | | | | | | |
| Negative | 30 | 86.70 | 0.3374 | 0.637 | 0.504–7.092 | 0.3453 | 0.387 | 0.796–2.726 | 0.2176 |
| Positive | 47 | 93.60 | | | | | | | |
| ObR expression | | | | | | | | | |
| Negative | 44 | 90.90 | 0.3605 | −0.608 | 0.145–2.043 | 0.3676 | −0.432 | 0.321–1.312 | 0.2284 |
| Positive | 33 | 90.90 | | | | | | | |
| BMI,
kg/m2 | | | | | | | | | |
| <25 | 45 | 91.10 | 0.2739 | 0.095 | 0.696–1.737 | 0.685 | 0.034 | 0.610–1.754 | 0.8988 |
| ≥25 | 32 | 90.60 | | | | | | | |
| Age, years | | | | | | | | | |
| <60 | 45 | 91.10 | 0.9348 | −0.024 | 0.617–1.546 | 0.9186 | −0.192 | 0.417–1.636 | 0.5828 |
| ≥60 | 32 | 90.60 | | | | | | | |
Univariate and multivariate analyses
Univariate logistic regression analysis revealed
that advanced-stage disease, high tumour grade, deeper myometrial
invasion, cervical stromal invasion, adnexal invasion, involvement
of the lymphovascular space, lymph node metastasis and negative
AdipoR-1 expression were all significantly associated with poor
progression-free survival. Similarly, multivariate Cox proportional
hazard regression analysis revealed adnexal invasion and lymph node
metastasis as independent variables associated with shorter
progression-free survival (Table
III). Univariate logistic regression analysis revealed that
advanced-stage disease, high tumour grade, deeper myometrial
invasion, cervical stromal invasion, adnexal invasion, lymph node
metastasis and negative AdipoR-1 expression were significantly
associated with poor overall survival, while multivariate Cox
proportional hazard regression analysis revealed that adnexal
invasion and lymph node metastasis were also identified as
independent variables associated with shorter overall survival
(Table IV).
Discussion
Obesity is a known risk factor for endometrial
cancer (8). Adipose tissues produce
various bioactive substances called adipokines, the most prominent
of which are leptin and adiponectin. Leptin has been found to
positively correlate with obesity and is a well-known regulator of
food intake and energy balance. By reducing tissue sensitivity to
insulin, leptin is responsible for hyperinsulinaemia (35). Adiponectin has been found to
negatively correlate with obesity, and low levels of adiponectin
have been shown to have a high correlation with hyperinsulinaemia
and the degree of insulin resistance independent of adiposity
(36). These adipokines are
reportedly associated with carcinogenesis and tumour growth in
several types of cancer, including breast, colon, stomach and
endometrial cancer (5–8). Serum concentrations of leptin are
reportedly higher, and those of adiponectin lower, in patients with
endometrial cancer compared with the control subjects (26,37–40).
The balance of leptin and adiponectin levels in individuals, rather
than leptin or adiponectin levels alone, may indicate such
physiological changes as the development of endometrial cancer
(41).
Previously, adiponectin has been shown to exert
suppressive effects on tumour development (42). Low adiponectin serum concentrations
have been identified in patients affected by cancer (38,42–44),
including endometrial cancer. Serum adiponectin levels have been
found to be inversely and independently associated with endometrial
cancer (39).
The actions of adiponectin are mediated by binding
to two receptors, AdipoR-1 and AdipoR-2 (31), and leptin actions are also mediated
by binding to ObR.
Adiponectin has been previously reported to suppress
endometrial cancer proliferation through AdipoRs and also increase
the expression of the adaptor molecule, LKB1, which is
required for adiponectin-mediated activation of the AMPK/S6 axis
and modulation of cell proliferation, colony formation, adhesion
and invasion of endometrial carcinoma cell lines in vitro
(34,45). In addition, adiponectin reportedly
acts to potently inhibit endothelial cell proliferation and
migration in vitro and, in chick chorioallantoic membrane
and mouse corneal angiogenesis assays, adiponectin shows marked
activity in preventing new blood vessel growth. Furthermore, the
antiendothelial mechanisms have been demonstrated to involve the
activation of caspase-mediated endothelial cell apoptosis.
Adiponectin induces the cascade activation of caspase-8, -9 and -3,
leading to cell death. In a previous mouse tumour model,
adiponectin significantly inhibited primary tumour growth (23). Impaired tumour growth appeared to be
associated with decreased neovascularisation, leading to
significantly increased tumour cell apoptosis. These results
demonstrated the induction of endothelial apoptosis as an unique
mechanism for adiponectin-induced antiangiogenesis. Adiponectin, as
a direct endogenous angiogenesis inhibitor, may have therapeutic
implications in the treatment of angiogenesis-dependent diseases,
including endometrial cancer (23).
The expression of these receptors has previously
been documented in normal endometrium (46) and endometrial cancer tissues
(47), but the role of AdipoR-1,
AdipoR-2 and ObR in endometrial carcinoma has not been fully
determined.
The present study demonstrated that AdipoR-1,
AdipoR-2 and ObR are expressed in endometrial carcinoma tissue, and
that AdipoR-1 expression inversely correlates with high
histological grade, deep myometrial invasion, involvement of the
lymphovascular space, adnexal invasion and lymph node metastasis,
and is associated with improved progression-free and overall
survival. However, AdipoR-2 and ObR expression was not found to
correlate with any clinicopathological factors or survival in
patients with endometrial carcinoma. Immunohistochemical expression
of adiponectin in paired samples of endometrial carcinoma was also
examined, but failed to observe any adiponectin expression in
tumour cells or stromal elements (data not shown). Thus, the
present results suggested that autocrine and paracrine stimulations
of AdipoRs are unsuitable for endometrial carcinoma.
Previously, Yamauchi et al (47) reported that decreased AdipoR-1
expression significantly correlates with higher histological grade,
myometrial invasion and lymph node metastasis of endometrioid
adenocarcinoma. These results raised the possibility that the
decreased expression of AdipoRs is implicated in the development,
invasion and metastasis of human endometrioid adenocarcinoma. Thus,
AdipoRs may be considered as therapeutic targets for endometrioid
adenocarcinoma. In AdipoR-positive endometrioid adenocarcinoma,
adiponectin-based anticancer therapy may prove useful. In addition,
Yamauchi et al (47)
commented that AdipoR-1 and AdipoR-2 may be considered as
therapeutic targets for endometrioid adenocarcinomas. Methods
leading to the upregulation of AdipoRs or development of specific
AdipoR agonists (such as osmotin) may prove beneficial in the
treatment of endometrioid adenocarcinomas, and the results of the
current study appear to support this perspective.
Several limitations must be considered when
interpreting the results of the present study. Firstly, the
immunohistochemical expression of AdipoR-1, AdipoR-2 and ObR were
analysed, but gene and protein expression levels were not revealed
in endometrial carcinoma. Secondly, the present study was unable to
assume that correlations exist between serum adiponectin or leptin
levels and the expression of AdipoRs and ObR in patients with
endometrial carcinoma. Despite these limitations, we considered the
present observations to be meaningful, since they provide evidence
that AdipoR-1 levels are inversely correlated with the biologically
malignant phenotypes of endometrial carcinoma, and that endometrial
cancer patients with positive expression of AdipoR-1 experience an
improved prognosis in terms of progression-free and overall
survival.
In conclusion, the present study demonstrated the
expression of AdipoR-1, AdipoR-2 and ObR in human endometrioid
adenocarcinoma of the uterine corpus. In addition, the decreased
expression of AdipoR-1 molecules was associated with tumour growth,
invasion and metastasis, representing factors predictive of poor
prognosis in patients with endometrial carcinoma. Furthermore,
adiponectin-based anticancer therapies may prove useful for
treating endometrial cancer.
References
|
1
|
Matsuda T, Marugame T, Kamo K, Katanoda K,
Ajiki W and Sobue T; Japan Cancer Surveillance Research Group.
Cancer incidence and incidence rates in Japan in 2006: based on
data from 15 population-based cancer registries in the monitoring
of cancer incidence in Japan (MCIJ) project. Jpn J Clin Oncol.
42:139–147. 2012. View Article : Google Scholar
|
|
2
|
Morrow CP, Bundy BN, Kurman RJ, Creasmann
WT, Heller P, Homesley HD and Graham JE: Relationship between
surgical-pathological risk factors and outcome in clinical stage I
and II carcinoma of the endometrium: A Gynecologic Oncology Group
Study. Gynecol Oncol. 40:55–65. 1991. View Article : Google Scholar
|
|
3
|
Creasman WT, Morrow CP, Bundy BN, Homesley
HD, Graham JE and Heller PB: Surgical pathologic spread patterns of
endometrial cancer. A Gynecologic Oncology Group Study. Cancer.
60(Suppl 8): S2035–S2041. 1987. View Article : Google Scholar
|
|
4
|
DiSaia PJ, Creasmann WT, Boronow RC and
Blessing JA: Risk factors and recurrent patterns in Stage I
endometrial cancer. Am J Obstet Gynecol. 151:1009–1015. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ishikawa M, Kitayama J, Kazama S,
Hiramatsu T, Hatano K and Nagawa H: Plasma adiponectin and gastric
cancer. Clin Cancer Res. 11:466–472. 2005.PubMed/NCBI
|
|
6
|
Wei EK, Giovannucci E, Fuchs CS, Willett
WC and Mantzoros CS: Low plasma adiponectin levels and risk of
colorectal cancer in men: a prospective study. J Natl Cancer Inst.
97:1688–1694. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mantzoros C, Petridou E, Dessypris N,
Chavelas C, Dalagama M, Alexe DM, Papadiamantis Y, Markopoulos C,
Spanos E, Chrousos G and Trichopoulos D: Adiponectin and breast
cancer risk. J Clin Endocrinol Metab. 89:1102–1107. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dal Maso L, Augustin LS, Karalis A,
Talamini R, Franceschi S, Trichopoulos D, Mantzoros CS and La
Vecchia C: Circulating adiponectin and endometrial cancer risk. J
Clin Endocrinol Metab. 89:1160–1163. 2004.PubMed/NCBI
|
|
9
|
Judd HL, Shamonki IM, Frumar AM and
Lagasse LD: Origin of serum estradiol in postmenopausal women.
Obstet Gynecol. 59:680–686. 1982.PubMed/NCBI
|
|
10
|
Berstein LM, Kvatchevskaya JO, Poroshina
TE, Kovalenko IG, Tsyrlina EV, Zimarina TS, Ourmantcheeva AF,
Ashrafian L and Thijssen JH: Insulin resistance, its consequences
for the clinical course of the disease, and possibilities of
correction in endometrial cancer. J Cancer Res Clin Oncol.
130:687–693. 2004. View Article : Google Scholar
|
|
11
|
Vona-Davis L and Rose DP: Angiogenesis,
adipokines and breast cancer. Cytokine Growth Factor Rev.
20:193–201. 2009. View Article : Google Scholar
|
|
12
|
Housa D, Housová J, Vernerová Z and
Haluzík M: Adipocytokines and cancer. Physiol Res. 55:233–244.
2006.
|
|
13
|
Garofalo C and Surmacz E: Leptin and
cancer. J Cell Physiol. 207:12–22. 2006. View Article : Google Scholar
|
|
14
|
Zhang Y, Proenca R, Maffei M, Barone M,
Leopold L and Friedman JM: Positional cloning of the mouse obese
gene and its human homologue. Nature. 372:425–432. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hu X, Juneja SC, Maihle NJ and Cleary MP:
Leptin - a growth factor in normal and malignant breast cells and
for normal mammary gland development. J Natl Cancer Inst.
94:1704–1711. 2002. View Article : Google Scholar
|
|
16
|
Jardé T, Caldefie-Chézet F, Damez M,
Mishellany F, Perrone D, Penault-Llorca F, Guillot J and Vasson MP:
Adiponectin and leptin expression in primary ductal breast cancer
and in adjacent healthy epithelial and myoepithelial tissue.
Histopathology. 53:484–487. 2008.PubMed/NCBI
|
|
17
|
Ishikawa M, Kitayama J and Nagawa H:
Enhanced expression of leptin and leptin receptor (OB-R) in human
breast cancer. Clin Cancer Res. 10:4325–4331. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tessitore L, Vizio B, Jenkins O, De
Stefano I, Ritossa C, Argiles JM, Benedetto C and Mussa A: Leptin
expression in colorectal and breast cancer patients. Int J Mol Med.
5:421–426. 2000.PubMed/NCBI
|
|
19
|
Huang L and Li C: Leptin: a
multifunctional hormone. Cell Res. 10:81–92. 2000. View Article : Google Scholar
|
|
20
|
Saxena NK, Taliaferro-Smith L, Knight BB,
Merlin D, Anania FA, O’Regan RM and Sharma D: Bidirectional
crosstalk between leptin and insulin-like growth factor-I signaling
promotes invasion and migration of breast cancer cells via
transactivation of epidermal growth factor receptor. Cancer Res.
68:9712–9722. 2008. View Article : Google Scholar
|
|
21
|
Garofalo C, Koda M, Cascio S, Sulkowska M,
Kanczuga-Koda L, Golaszewska J, Russo A, Sulkowski S and Suemacz E:
Increased expression of leptin and the leptin receptor as a marker
of breast cancer progression: possible role of obesity-related
stimuli. Clin Cancer Res. 12:1447–1453. 2006. View Article : Google Scholar
|
|
22
|
Arita Y, Kihara S, Ouchi N, Takahashi M,
Maeda K, Miyagawa J, Hotta K, Shimomura I, Nakamura T, Miyaoka K,
et al: Paradoxical decrease of an adipose-specific protein,
adiponectin, in obesity. 1999. Biochem Biophys Res Commun.
425:560–564. 2012.PubMed/NCBI
|
|
23
|
Bråkenhielm E, Veitonmäki N, Cao R, Kihara
S, Matsuzawa Y, Zhivotovsky B, Funahashi T and Cao Y:
Adiponectin-induced antiangiogenesis and antitumor activity involve
caspase-mediated endothelial cell apoptosis. Proc Natl Acad Sci
USA. 101:2476–2481. 2004.PubMed/NCBI
|
|
24
|
Ogunwobi OO and Beales IL: Globular
adiponectin, acting via adiponectin receptor-1, inhibits
leptin-stimulated oesophageal adenocarcinoma cell proliferation.
Mol Cell Endocrinol. 285:43–50. 2008. View Article : Google Scholar
|
|
25
|
Ishikawa M, Kitayama J, Yamauchi T,
Kadowaki T, Maki T, Miyato H, Yamashita H and Nagawa H: Adiponectin
Inhibits the growth and peritoneal metastasis of gastric cancer
through its specific membrane receptors AdipoR1 and AdipoR2. Cancer
Sci. 98:1120–1127. 2007. View Article : Google Scholar
|
|
26
|
Rzepka-Górska I, Bedner R, Cymbaluk-Płoska
A and Chudecka-Głaz A: Serum adiponectin in relation to endometrial
cancer and endometrial hyperplasia with atypia in obese women. Eur
J Gynaecol Oncol. 29:594–597. 2008.PubMed/NCBI
|
|
27
|
Yamauchi T, Kamon J, Ito Y, Tsuchida A,
Yokomizo T, Kita S, Sugiyama T, Miyagishi M, Hara K, Tsunoda M, et
al: Cloning of adiponectin receptors that mediate antidiabetic
metabolic effects. Nature. 423:762–769. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Luo XH, Guo LJ, Yuan LQ, Xie H, Zhou HD,
Wu XP and Liao EY: Adiponectin stimulates human osteoblasts
proliferation and differentiation via the MAPK signaling pathway.
Exp Cell Res. 309:99–109. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fasshauer M, Klein J, Kralisch S, Klier M,
Lössner U, Blüher M and Paschke R: Growth hormone is a positive
regulator of adiponectin receptor 2 in 3T3-L1 adipocytes. FEBS
Lett. 558:27–32. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kharroubi I, Rasschaert J, Eizirik DL and
Cnop M: Expression of adiponectin receptors in pancreatic beta
cells. Biochem Biophys Res Commun. 312:1118–1122. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kadowaki T and Yamauchi T: Adiponectin and
adiponectin receptors. Endocrine Rev. 26:439–451. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kadowaki T, Yamauchi T, Kubota N, Hara K,
Ueki K and Tobe K: Adiponectin and adiponectin receptors in insulin
resistance, diabetes, and the metabolic syndrome. J Clin Invest.
116:1784–1792. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
33
|
Takahata C, Miyoshi Y, Irahara N, Taguchi
T, Tamaki Y and Noguchi S: Demonstration of adiponectin receptors 1
and 2 mRNA expression in human breast cancer cells. Cancer Lett.
250:229–236. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cong L, Gasser J, Zhao J, Yang B, Li F and
Zhao AZ: Human adiponectin inhibits cell growth and induces
apoptosis in human endometrial carcinoma cells, HEC-1-A and RL95-2.
Endocrine Relat Cancer. 14:713–720. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Gnacińska M, Małgorzewicz S, Stojek M,
Łysiak-Szydłowska W and Sworczak K: Role of adipokines in
complications related to obesity: a review. Adv Med Sci.
54:150–157. 2009.PubMed/NCBI
|
|
36
|
Hanley AJ, Bowden D, Wagenknecht LE,
Balasubramanyam A, Langfeld C, Saad MF, Rotter JI, Guo X, Chen YD,
Bryer-Ash M, et al: Associations of adiponectin with body fat
distribution and insulin sensitivity in nondiabetic Hispanics and
African-Americans. J Clin Endocrinol Metab. 92:2665–2671. 2007.
View Article : Google Scholar
|
|
37
|
Petridou E, Mantzoros C, Dessypris N,
Koukoulomatis P, Addy C, Voulgaris Z, Chrousos G and Trichopoulos
D: Plasma adiponectin concentrations in relation to endometrial
cancer: a case-control study in Greece. J Clin Endocrinol Metab.
88:993–997. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Cymbaluk A, Chudecka-Głaz A and
Rzepka-Górska I: Leptin levels in serum depending on Body Mass
Index in patients with endometrial hyperplasia and cancer. Eur J
Obstet Gynecol Reprod Biol. 136:74–77. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Soliman PT, Wu D, Tortolero-Luna G,
Schmeler KM, Slomovitz BM, Bray MS, Gershenson DM and Lu KH:
Association between adiponectin, insulin resistance, and
endometrial cancer. Cancer. 106:2376–2381. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cust AE, Kaaks R, Friedenreich C, Bonnet
F, Laville M, Lukanova A, Rinaldi S, Dossus L, Slimani N, Lundin E,
et al: Plasma adiponectin levels and endometrial cancer risk in
pre- and postmenopausal women. J Clin Endocrinol Metab. 92:255–263.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ashizawa N, Yahata T, Quan J, Adachi S,
Yoshihara K and Tanaka K: Serum leptin-adiponectin ratio and
endometrial cancer risk in postmenopausal female subjects. Gynecol
Oncol. 119:65–69. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kelesidis I, Kelesidis T and Mantzoros CS:
Adiponectin and cancer: a systemic review. Br J Cancer.
94:1221–1225. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Petridou E, Mantzoros C, Dessypris N,
Dikalioti SK and Trichopoulos D: Adiponectin in relation to
childhood myeloblastic leukaemia. Br J Cancer. 94:156–160. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Goktas S, Yilmaz MI, Caglar K, Sonmez Z,
Kilic S and Bedir S: Prostate cancer and adiponectin. Urology.
65:1168–1172. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Moon HS, Chamberland J, Aronis K,
Tseleni-Balafonta S and Mantzoros C: Direct role of adiponectin and
adiponectin receptors in endometrial cancer: in vitro and ex vivo
studies in humans. Mol Cancer Ther. 10:2234–2243. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Takemura Y, Osuga J, Yamauchi T, Kobayashi
M, Harada M, Hirata T, Morimoto C, Hirota Y, Yoshino O, Koga K, et
al: Expression of adiponectin receptors and its possible
implication in the human endometrium. Endocrinology. 147:3203–3210.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Yamauchi N, Takazawa Y, Maeda D, Hibiya T,
Tanaka M, Iwabu M, Okada-Iwabu M, Yamauchi T, Kadowaki T and
Fukayama M: Expression levels of adiponectin receptors are
decreased in human endometrial adenocarcinoma tissues. Int J
Gynecol Pathol. 31:352–357. 2012. View Article : Google Scholar
|