Introduction
In the late 1990s, a greatly increased standardised
rate of mortality from pleural mesothelioma was highlighted by
epidemiological surveys in the area of Biancavilla, a Sicilian town
on the south west slope of Mount Etna volcano (1,2).
Subsequent studies identified an asbestiform mineral fibre in the
benmoreitic lava from a local stone quarry. The quarry had been
mined from 1950–1998 to extract sand and gravel, which was
routinely used by builders to produce pavements and house plaster
(2,3).
The fibre was identified as fluoro-edenite (4).
Fluoro-edenite
(NaCa2Mg5Si7AlO22F2)
is a new mineral species recognised by the Commission on New
Minerals and Mineral Names (CNMMN; IMA: code 2000–049) in 2001
(5). The fibres are similar in size
and morphology to certain amphibolic asbestos fibres (including
tremolite, actinolite and antophyllite) (4), the inhalation of which may cause chronic
inflammation and pleural mesothelioma (1,2).
Based on previous animal studies, long, thin
asbestos fibers (≥8 µm in length and ≤0.25 µm in width) have been
postulated to be strongly carcinogenic; inducing pleural malignant
mesothelioma, while shorter, thicker fibers are thought to pose a
smaller risk (6). The relationship
between asbestos exposure and respiratory disease has been studied
extensively (7). Occupational
exposure to asbestos is known to be associated with pleural and
lung diseases, including pleural plaques, pleurisy, fibrosis of the
visceral pleura, rounded atelectasis, asbestosis, lung cancer and
malignant mesothelioma (8). These
diseases, termed asbestos-related diseases, are well documented and
approximately 107,000 mortalities are attributable to asbestos
exposure worldwide, annually (9,10). Little
has been established with regard to the effects of human exposure
to fluoro-edenite fibres (11–13),
however, epidemiological studies have indicated that these fibres
may have a causative role in chronic obstructive lung disease
(1,14)
and malignant pleural mesothelioma (2,14).
The aim of the current study was to evaluate the
findings following the assessment of the pleura and lung parenchyma
of a group of construction workers residing and working in the area
of Biancavilla.
Materials and methods
Subjects
Between 2009 and 2013, 52 male construction workers
living and working in the area of Biancavilla were visited within
the framework of periodic occupational surveillance and invited to
participate in this study. A free medical examination, including a
high-resolution computer tomography (HRCT) chest scan, was offered
to participants.
Exclusion criteria were broncho-pulmonary diseases
(e.g. asthma, bronchopneumonia, and tuberculosis), previous
asbestos exposure, and involvement in construction work in the
Biancavilla area for <1 year.
A questionnaire was used to collect information
about the participants with regard to family, medical history,
medication, drinking habits, hobbies, etc. Questions on tobacco
consumption enabled participants to be classified as current
smokers, ex-smokers (those who had not smoked for >1 year) and
non-smokers (those who had never smoked).
The research protocol was approved by the Ethics
Committee of Catania University Hospital (Catania, Italy) and the
written informed consent of all subjects was acquired prior to
their inclusion in the study.
Fluoro-edenite exposure
The questionnaire was used to determine
fluoro-edenite exposure based on each participant's occupational
history. Duration (years) and dates of exposure were recorded. The
intensity of exposure was weighted according to occupation, as
follows: Low (electricians) (passive), 0.01; low intermediate
(tilers, crane operators), 0.1; high intermediate (painter, shovel
operator), 1; high (carpenter, plasterer, plumber), 10. A
cumulative exposure index (CEI) to fluoro-edenite was calculated
for each subject as the sum of all periods of employment in jobs
involving exposure (duration × weighting factor). Due to a lack of
data regarding air-borne fibres, and of detailed information on
exposure frequency (percentage working time), the CEI was expressed
as exposure unit x year rather than as fibres/ml x year. Latency
was defined as the interval from the beginning of the first job
considered to entail fluoro-edenite exposure, to the date of the
HRCT scan performed in the present study.
Clinical parameters
On acquiring a detailed case history, workers were
subjected to: i) Physical examination; ii) blood analysis; iii)
search for uncoated fibres and ferruginous bodies in sputum; iv)
pulmonary function tests and diffusion capacity for carbon monoxide
(TLCO); and v) HRCT chest scanning. Respiratory symptoms
were graded using the American Thoracic Society (ATS) questionnaire
(15).
Venous blood (10 ml) was collected in the morning,
following overnight fasting, to determine red blood cell count,
haematocrit, haemoglobin levels, white blood cell count,
erythrocyte sedimentation rate, C-reactive protein levels and liver
enzyme (aspartate aminotransferase and alanine aminotransferase)
levels.
Sampling and fibre search were conducted according
to the protocol by Putzu et al (16). Sputum was classified as negative or
positive for uncoated fibres and ferruginous bodies (detection
limit, 120 ppm).
Respiratory function tests were conducted using a
bell spirometer (Biomedin, Padova, Italy) (17). Equipment, calibration and manoeuvres
met ATS guidelines (15). Forced
vital capacity, forced expiratory volume in 1 s, peak expiratory
flow, maximal expiratory flow rate at 25–75% of the vital capacity,
total lung capacity, and TLCO were measured and
expressed as a proportion of European Coal and Steel Community
reference values adjusted for individual characteristics (age,
weight and height) recorded at the time of testing (18).
Subjects underwent HRCT scanning with the use of an
Optima CT 580W (GE Healthcare, Fairfield, CT, USA), without
contrast enhancement, according to a specifically devised protocol:
The entire chest was screened using spiral acquisition sequences
with the subject in supine position. Interstitial or pleural
abnormalities were recorded in standardised form using the
Fleischner Society glossary of terms (16). Pleural plaques were defined as
circumscribed quadrangular elevations with sharp borders and
density comparable to tissue, with/without signs of calcification.
Thickness was classified, based on the thickest plaque, into four
categories (<2 mm, 2-<5 mm, 5-<10 mm and ≥10 mm). Cut-off
criteria were selected and adapted from the International Labour
Office classification of radiographs of pneumoconiosis (16).
Parenchymal abnormalities (subpleural dependent
opacity, subpleural curvilinear opacities, subpleaural
perpendicular lines, parenchymal nodules, honeycombing and ground
glass opacities) were recorded and classified by three chest
radiologists using a semiquantitative 10-class scale including six
subclasses; 0 (no finding), 1 (normal), 2 (subnormal; one or two
abnormalities located sporadically in the lung periphery, no
honeycombing), 3 (mild fibrosis; at least two abnormalities located
on both sides and in several slices from the lung periphery, no
honeycombing), 4 (moderate fibrosis; several criteria, which extend
deeper into the lung, honeycombing as a general rule), 5 (severe
fibrosis; several abnormalities or associated findings extending
deep into the lung, honeycombing, lung architectural change) and 6
(extreme fibrosis; extremely severe and various fribrotic changes,
little normally aerated lung remaining) as previously described by
Gangemi et al (17).
Statistical analysis
Data analysis was performed using SPSS software
version 20 (IBM, Milan, Italy). The main population
characteristics, respiratory test results and characteristics of
the pleural plaques were expressed as the mean ± standard deviation
(SD) or as the total number of participants with that
characteristic and the percentage represented by that number. The
variables used to determine fluoro-edenite exposure were exposure
duration, CEI, and the interval between earliest exposure and the
HRCT scan conducted during the present study.
A prevalence ratio (PR) with 95% confidence interval
(CI) and two-tailed test P-value were calculated for pleural
plaques using log-binomial regression, measuring plaque size and
thickness, and CEI. Potential confounders were identified from the
literature and included in the analysis; the confounding factors
used in the models were age and smoking status. Age was modeled as
a continuous variable while smoking status was dichotomised as
smoker and ex-smoker versus non-smoker.
Results
Application of the exclusion criteria led to the
exclusion of nine subjects, due to previous exposure to asbestos
(n=5), bronchopneumonia (n=2), tuberculosis (n=1) or allergic
bronchial asthma (n=1), leaving 43 participants, whose
characteristics are reported in Table
I. All 43 workers included in the study had been residing in
Biancavilla for >40 years, and 65% (n=28) were born there.
Additionally, all had been working almost exclusively in and around
Biancavilla. The occupational history recorded from the
participants revealed that 38 (88%) had personally handled and
mixed gravel from the Mount Calvario quarry until 1998.
Furthermore, all had been involved in restoring houses that had
been built in the 1950s, when lava from the quarry had been
extensively used as a building material. Smokers, ex-smokers and
non-smokers did not differ significantly with regard to any study
parameter.
 | Table I.Characteristics of the study
population of exposed workers (n=43). |
Table I.
Characteristics of the study
population of exposed workers (n=43).
| Patient
characteristics | Participants |
|---|
| Age, mean ± SD,
years | 49.3±6.7 |
| Occupation, n
(%) |
|
|
Unskilled construction
worker | 16 (37) |
|
Specialised construction
worker | 14 (33) |
|
Carpenters | 13 (30) |
| Duration of
residence in Biancavilla, mean ± SD, years | 44.7±10.3 |
| Smoking habits, n
(%) |
|
| Current
smokersa | 13 (30) |
|
Ex-smokersa | 16 (37) |
|
Non-smokersa | 14 (33) |
| CEI to
fluoro-edenite (exposure unit × years), n (%) |
|
|
1–9 | 3 (5) |
|
10–19 | 11 (25) |
|
20–29 | 19 (44) |
|
30–39 | 7 (19) |
|
≥40 | 3 (7) |
A CEI ranging from 10–29 was determined in the
majority of participants (n=30; 70%). Respiratory symptoms were
identified in six (14%) workers: Four (10%) had a cough and two
(5%) had mild (grade I) dyspnoea. Other identified conditions not
involving the respiratory apparatus were: Arterial hypertension
(n=5; 12%), type II diabetes mellitus (n=2; 5%), dyslipidaemia
(n=4; 10%), dysthyroidism (n=3; 7%) and prostatic hypertrophy (n=1;
2%). All conditions were being treated. Blood examination to
determine red blood cell count, haematocrit, haemoglobin levels,
white blood cell count, erythrocyte sedimentation rate, C-reactive
protein levels and liver enzyme (aspartate aminotransferase and
alanine aminotransferase) levels revealed that two participants
(the two diabetic subjects) had hyperglycaemia (blood glucose
level, >125 mg/dl); the parameters of the other workers were
within the normal range.
The results from the respiratory tests and the
search for uncoated fibres and ferruginous bodies in sputum are
reported in Table II. The mean
values (% predicted) of the functional respiratory tests were
within the normal range for all participants. A restrictive
ventilatory defect was discovered in two (5%) subjects and an
obstructive ventilatory defect observed in three (7%).
TLCO was reduced in two additional participants.
Overall, a slight non-significant reduction in predictive values
(%) was noted with rising CEI (range, 30-≥40). Fluoro-edenite
fibres, but not fibre bundles, were recovered from the sputum of 19
(44%) workers. The length of the fibres ranged from 10–35 µm, with
a diameter of <0.5 µm. Ferruginous bodies were not identified in
any of the samples.
| Table II.Results of respiratory tests
(expressed as % predicted mean ± SD) and sputum examination
(expressed as n and %) of participants, subdivided by occupational
CEI values. |
Table II.
Results of respiratory tests
(expressed as % predicted mean ± SD) and sputum examination
(expressed as n and %) of participants, subdivided by occupational
CEI values.
| CEI | 1–9 | 10–19 | 20–29 | 30–39 | ≥40 |
|---|
| Subjects, n
(%a) | 2 (5) | 9 (21) | 23 (53) | 7 (16) | 2 (5) |
| Smokers, n
(%b) | 3 (23) | 4 (31) | 3 (23) | 2 (15) | 1 (8) |
| FVC, % | 98.2±5.7 | 97.7±1.1 | 96.9±1.6 | 92.9±6.7 | 90.8±8.6 |
| FEV1,
% | 98.8±7.8 | 95.5±1.3 | 93.6±1.4 | 87.6±6.5 | 83.3±9.1 |
| PEF, % | 97.6±7.9 | 95.2±6.4 | 92.3±5.7 | 90.7±6.9 | 86.9±9.6 |
|
MEF25–75, % | 94.5±8.6 | 94.3±9.1 | 89.5±6.3 | 85.2±6.1 | 82.5±8.7 |
| TLC, % | 96.6±5.6 | 95.5±3.3 | 90.3±7.2 | 88.9±5.1 | 87.7±5.4 |
| TLCO,
% | 96.9±6.4 | 95.4±6.6 | 90.2±4.1 | 81.5±5.7 | 79.3±6.4 |
| Fibres present in
sputum, n (%c) | 0 (0) | 4 (21) | 12 (63) | 2 (11) | 1 (5) |
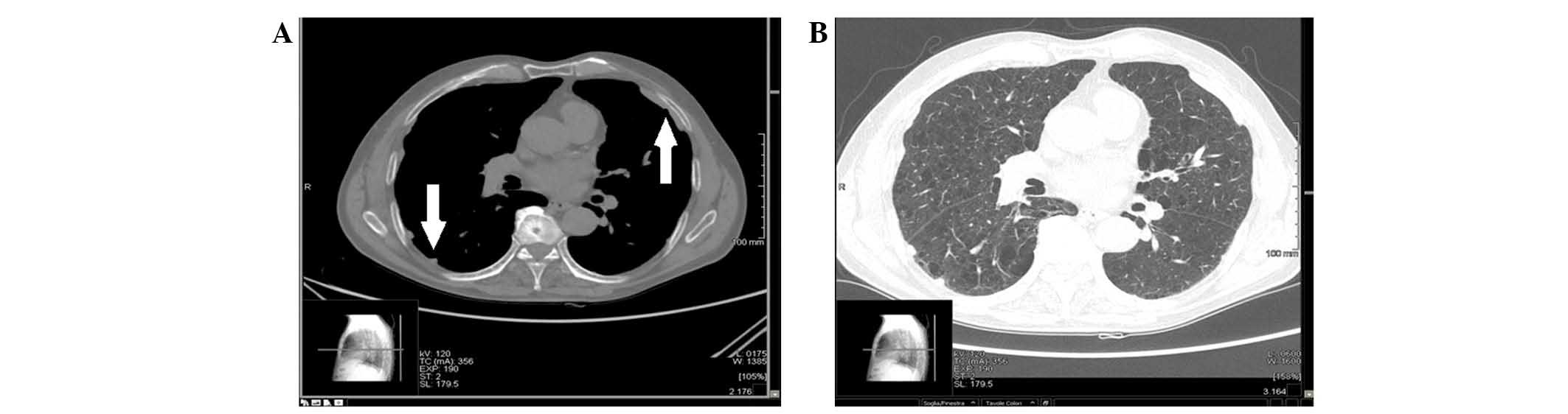
The HRCT findings in lung parenchyma are reported in
Table III. HRCT scans revealed
low-grade fibrosis in seven workers (two unilateral and five
bilateral) and unilateral rounded atelectasis in two workers.
Pleural involvement was documented in 39 (91%) subjects, of whom 31
(72%) had bilateral plaques. Calcifications were detected in 25
(58%) participants (Table IV).
Examples of HRCT scans acquired from these participants are shown
in Figs. 1 and 2. Calculation of plaque PR with 95% CI, and
the P-value from the two-tailed test by log-binomial regression,
demonstrated a progressive increase in the risk of developing
pleural lesions with rising CEI, i.e. length of exposure (Table V).
| Table III.High-resolution computed tomography
findings in the lung parenchyma of 43 workers. |
Table III.
High-resolution computed tomography
findings in the lung parenchyma of 43 workers.
|
| Subjects with
unilateral abnormalities, n (%; mean score ± SD) | Subjects with
bilateral abnormalities, n (%; mean score ± SD) |
|---|
| Rounded
atelectasis | 2 (5%;
1.12±0.23) | 0 |
| Emphysema | 0 | 0 |
| Thickness | 0 | 0 |
| Bronchiectasis | 0 | 0 |
| Fibrosis | 2 (5%;
1.43±0.32) | 5 (12%;
2.07±0.65) |
| Table IV.Characteristics of the pleural
plaques detected by high-resolution computed tomography in 39
participants. |
Table IV.
Characteristics of the pleural
plaques detected by high-resolution computed tomography in 39
participants.
| Plaque
features | Unilateral plaques,
n (%a) | Bilateral plaques,
n (%b) | Total, n
(%c) |
|---|
| Thickness, mm |
|
|
|
|
<2 | 0 (0%) | 5 (16%) | 5 (13%) |
|
2–4.9 | 5 (62%) | 10 (32%) | 15 (38%) |
|
5–9.9 | 3 (38%) | 9 (29%) | 12 (31%) |
|
≥10 | 0 (0%) | 7 (23%) | 7 (18%) |
| Size |
|
|
|
| <1
cm | 0 (0%) | 4 (15%) | 4 (10%) |
| 1
cm-24% of lateral chest wall | 4 (50%) | 15 (48%) | 22 (49%) |
| 24–49%
of lateral chest wall | 4 (50%) | 9 (29%) | 14 (33%) |
| ≥0% of
lateral chest wall | 0 (0%) | 3 (10%) | 3
(8%) |
| Calcification | 4 (50%) | 21 (54%) | 25 (58%) |
| Table V.PR with 95% CI and two-tailed test
P-value were calculated for the pleural plaques in the 39 (91%)
participants using log-binomial regression taking into
consideration plaque size and thickness and CEI. |
Table V.
PR with 95% CI and two-tailed test
P-value were calculated for the pleural plaques in the 39 (91%)
participants using log-binomial regression taking into
consideration plaque size and thickness and CEI.
|
| Risk
indicators |
|---|
|
|
|
|---|
| CEI to
fluoro-edenitea | PR | CI | P-value |
|---|
| 1–9 | 1.00 |
|
|
| 10–19 | 1.45 | 1.12–1.78 | >0.05 |
| 20–29 | 1.98 | 1.84–2.12 | >0.001 |
| 30–39 | 2.36 | 2.01–2.58 | >0.001 |
| ≥40 | 3.32 | 3.24–3.48 | >0.001 |
Discussion
Exposure to asbestiform fibres similar to that
described in Biancavilla has been reported for erionite in the
central Anatolian villages of Karain and Tuzkoy (21–23).
Erionite is a fibrous zeolite found in the natural rock material
used locally for building (24,25). As in
Biancavilla, a high mortality rate from pleural carcinoma (sentinel
event) allowed for the recognition of population exposure and,
consequently, occupational exposure, particularly for construction
workers.
For decades, fluoro-edenite has been considered
predominantly as a synthetic fibre (26–28). The
natural environments from which it had previously been discovered
include the Pargas region in Finland (29), the Utah Rocky Mountains (30) and the Orange area in New Jersey
(31). However, Biancavilla is the
first and sole instance involving human exposure (2,3).
Additionally, the fibres recovered from the lava of the Kimpo
volcano in Kumamoto Prefecture (Japan) are structurally similar to
Biancavilla's fluoro-edenite (32),
however, they have never been submitted to the CNMMN, nor has human
exposure been described.
The type of environmental contamination discovered
in Biancavilla (22,33,34)
suggests that the entire population is exposed to fluoro-edenite
(1). Construction workers are at
increased risk due to additional exposure to fibres present in the
cement and plaster made with contaminated material from the Mount
Calvario quarry (2,3).
The respiratory function tests and HRCT imaging
conducted in the present study enabled the evaluation of the
effects of fluoro-edenite fibres on subjects who are both residents
and occupationally exposed subjects. The results document a broad
involvement of the respiratory apparatus, and a greater involvement
of the pleura (39/43) compared with the lung. However, these
lesions have a limited effect on respiratory function, as has been
demonstrated from the results of the spirometry. The respiratory
function data collected in the present study are consistent with
those of other studies conducted on construction workers with
pleural plaques related to occupational asbestos exposure (35–38).
Pleural plaques are circumscribed, thickened areas,
consisting of avascular connective tissue, localised to the
parietal and/or diaphragmatic pleura of asbestos-exposed subjects
(38). They may reflect a local
(pleural) response to asbestos fibre accumulation, and are
typically detected in exposed construction workers (39). Plaques indicate consistent exposure to
low fibre concentrations (0.19 fibre-years/ml) (40). Other potential pleural responses
include lymph node calcification and carcinogenesis (41,42). The
results of the current study are consistent with those of other
studies, which reported that, in cases of chest wall pleural
plaques detected in asbestos-exposed construction workers, ~70%
exhibit lesions on both sides of the chest (20,39,43), and
~30% also exhibit calcifications (25% in the current sample)
(20,39).
Subjects with pleural plaques are at greater risk of
lung cancer and malignant pleural mesothelioma, compared with the
general population (38,41,42,44).
Inhalation of asbestos fibres may induce two types of
interconnected pathogenic processes involving the respiratory
apparatus: Chronic inflammation or carcinogenesis. These effects
are related to the ability of fibres to disrupt mitotic mechanisms,
stimulate host cell proliferation, induce release of free radicals
(resulting in DNA damage), and prolong the release of cytokines and
growth factors (45,46). In vivo and in vitro
analysis of the biological reactivity of fluoro-edenite fibres has
also demonstrated that they are able to cause the production of
reactive oxygen species, stimulation of the intrinsic and extrinsic
apoptosis pathways, and induction of inflammatory processes through
the activation of specific cytokines (47–51).
With regard to the recovery of fibres from sputum,
the current data are consistent with those of Putzu et al
(16), who described fibres similar
to those found in the present study in 50% (6/12) of their sample
of Biancavilla residents (vs. 44%, or 19/43, in the current study).
That these subjects were four housewives, a farmer and a mason,
with no history of exposure to fluoro-edenite fibres, indicates a
predominantly environmental exposure.
Environmental contamination had previously been
demonstrated by examination of the lungs and lymph nodes of sheep
whose pastures lay a few kilometres from Biancavilla (33,34).
Therefore the risk of inhalation of dust particles, particularly
fluoro-edenite fibres, from Mount Calvario quarry is high even in
open, non-urban areas located a short distance away from this
region (33,34). Such contamination is likely to be the
cause of the pleural plaques detected in the lungs of the
construction workers in the current study with a relatively short
occupational exposure (low CEI). The significantly greater plaque
size and thickness observed in workers with a higher CEI may
indicate a combination of environmental and occupational exposure,
thus increasing the risk of development of respiratory conditions
in these individuals (52).
A form of biphasic pollution may be hypothesised for
fluoro-edenite, as proposed for asbestos fibres (53). As sand from the Mount Calvario quarry
is commonly used locally in the production of building materials,
the maintenance, repair and restructuring work conducted over the
years may have induced the fragmentation of larger particles and
fibres into smaller particles and fibres, capable of remaining
airborne for a long period, and of disseminating over considerable
distances.
The present findings demonstrate for the first time
pleural plaques in the lungs of subjects not exposed to asbestos,
but to fluoro-edenite fibres, through living and working in
Biancavilla. The data indicate the requirement to establish a
population screening programme for conditions associated with fibre
exposure. All sources of occupational exposure to fluoro-edenite
fibres must be identified and measures should be taken to minimise
this exposure, including periodic environmental fibre monitoring
and adaptation of a surveillance protocol to consider the health
effects of fibres, assess risks and calculate the cost-benefit
ratio of the monitoring programme.
The present, preliminary study is of value as it
describes pleural plaques that may be ascribed to exposure to
fluoro-edenite fibres. Investigation of the resident population and
of larger cohorts of exposed workers is required to gain further
insights.
Acknowledgements
The authors would like to thank Dr Marine Castaing
(Cancer Registry of Catania-Messina-Siracusa-Enna; University of
Catania, Catania, Italy) for her assistance and support.
References
|
1
|
Di Paola M, Mastrantonio M and Carboni M:
Mortality from malignant pleural neoplasms in Italy in the years
1988–1992Rapporti ISTISAN 96/40. Rome, Italy: pp. 1–30. 1996
|
|
2
|
Paoletti L, Batisti D, Bruno C, et al:
Unusually high incidence of malignant pleural mesothelioma in a
town of eastern Sicily: an epidemiological and environmental study.
Arch Environ Health. 55:392–398. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rapisarda V, Amati M, Coloccini S, et al:
The in vitro release of hydroxyl radicals from dust containing
fluoro-edenite fibers identified in the volcanic rocks of
Biancavilla (eastern Sicily). Med Lav. 94:200–206. 2003.[(In
Italian)]. PubMed/NCBI
|
|
4
|
Comba P, Gianfagna A and Paoletti L:
Pleural mesothelioma cases in Biancavilla are related to a new
fluoro-edenite fibrous amphibole. Arch Environ Health. 58:229–232.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gianfagna A and Oberti R: Fluoro-edenite
from Biancavilla (Catania, Sicily, Italy): Crystal chemistry of a
new amphibole end-member. Am Mineral. 86:1489–1493. 2001.
|
|
6
|
Stanton MF, Layard M, Tegeris A, et al:
Relation of particles dimension to carcinogenicity in amphibole
asbestoses and fibrous minerals. J Natl Cancer Inst. 67:965–975.
1981.PubMed/NCBI
|
|
7
|
Bernstein D, Dunnigan J, Hesterberg T, et
al: Health risk of chrysotile revisited. Crit Rev Toxicol.
43:154–183. 2003. View Article : Google Scholar
|
|
8
|
Becklake MR, Bagatin E and Neder JA:
Asbestos-related diseases of the lungs and pleura: uses, trends and
management over the last century. Int J Tuberc Lung Dis. 11:356–69.
2007.PubMed/NCBI
|
|
9
|
Robinson BW and Lake RA: Advances in
malignant mesothelioma. N Engl J Med. 353:1591–1603. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
World Health Organization: Asbestos:
elimination of asbestos-related diseases. http://www.who.int/mediacentre/factsheets/fs343/en/Accessed.
January 20–2015
|
|
11
|
Fazzo L, Minelli G, De Santis M, et al:
Mesothelioma mortality surveillance and asbestos exposure tracking
in Italy. Ann Ist Super Sanita. 48:300–310. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Loreto C, Carnazza ML, Cardile V, et al:
Mineral fiber-mediated activation of phosphoinositide-specific
phospholipase c in human bronchoalveolar carcinoma-derived alveolar
epithelial A549 cells. Int J Oncol. 34:371–376. 2009.PubMed/NCBI
|
|
13
|
Musumeci G, Loreto C, Cardile V, et al:
Immunohistochemical expression of retinoblastoma and
phospho-retinoblastoma protein in sheep lung exposed to
fluoro-edenite fibers. Anat Sci Int. 85:74–78. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Biggeri A, Pasetto R, Belli S, et al:
Mortality from chronic obstructive pulmonary disease and pleural
mesothelioma in an area contaminated by natural fiber
(fluoro-edenite). Scand J Work Environ Health. 30:249–252. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Standards for the diagnosis and care of
patients with chronic obstructive pulmonary disease. American
Thoracic Society. Am J Respir Crit Care Med. 152:S77–S121.
1995.PubMed/NCBI
|
|
16
|
Putzu MG, Bruno C, Zona A, et al:
Fluoro-edenitic fibres in the sputum of subjects from Biancavilla
(Sicily): a pilot study. Environ Health. 5:202006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gangemi S, Rapisarda V, Minciullo PL, et
al: Circulating levels of interleukin-18 in asbestos-exposed
workers. Toxicol Ind Health. 21:125–129. 2005. View Article : Google Scholar
|
|
18
|
Miller MR, Hankinson J, Brusasco V, et al:
Standardisation of spirometry. Eur Respir J. 26:319–338. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hansell DM, Bankier AA, MacMahon H, et al:
Fleischner Society: glossary of terms for thoracic imaging.
Radiology. 246:697–722. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
International Labour Organization, . ILO
standards-related activities in the area of occupational safety and
health: An in-depth study for discussion with a view to the
elaboration of a plan of action for such activities. Report VI.
Geneva, International Labour Office. 2003.
|
|
21
|
Bariş B, Demir AU, Shehu V, et al:
Environmental fibrous zeolite (erionite) exposure and malignant
tumors other than mesothelioma. J Environ Pathol Toxicol Oncol.
15:183–189. 1996.PubMed/NCBI
|
|
22
|
Temel A and Gündoǧdu MN: Zeolite
occurrences and the erionite-mesothelioma relationship in
Cappadocia, central Anatolia, Turkey. Miner Deposita. 31:539–547.
1996. View Article : Google Scholar
|
|
23
|
Dogan AU: Mesothelioma in Cappadocian
villages. Indoor Built Env. 12:367–375. 2003. View Article : Google Scholar
|
|
24
|
Metintas M, Hillerdal G and Metintas S:
Malignant mesothelioma due to environmental exposure to erionite:
follow-up of a Turkish emigrant cohort. Eur Respir J. 13:523–526.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Roushdy-Hammady I, Siegel J, Emri S, et
al: Genetic-susceptibility factor and malignant mesothelioma in the
Cappadocian region of Turkey. Lancet. 357:444–445. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Boschmann KF, Burns PC, Hawthorne FC, et
al: A-site disorder in synthetic fluor-edenite, a crystal-structure
study. Can Mineral. 32:21–30. 1994.
|
|
27
|
Eugene CJ and Arnold KJ: Study on
synthetic fluor-tremolite, part 1 of synthetic asbestos
investigations. Am Mineral. 39:537–548. 1954.
|
|
28
|
Robert JL, Della Ventura G and Thauvin JL:
The infrared OH-stretching region of synthetic richterites in the
system
Na2O-K2O-CaO-MgO-SiO2-H2O-HF.
Eur J Mineral. 1:203–212. 1989. View Article : Google Scholar
|
|
29
|
Laitakari A: Uber die Petrographie der
kalksteingerstatten von Parainen (Pargas). Bulletin de la
Commission Geologique de Finlande. 54:101921.
|
|
30
|
Moore JN and Kerrick DM: Equilibria in
siliceous dolomites of the Alta aureole. Utah. Am J Sci.
276:502–524. 1976. View Article : Google Scholar
|
|
31
|
Kearns LE, Kite LE, Leavens PB and Nelen
JA: Fluorine distribution in the hydrous silicate minerals of the
Franklin Marble, Orange County, New York. Am Mineral. 65:557–562.
1980.
|
|
32
|
Makino K, Yamaguchi Y and Tomita K: Fluor
edenite from the Ishigamiyama lava dome of the Kimpo volcano,
Kumamoto, southwest Japan. GANKO. 91:419–423. 1996.[(In
Japanese)].
|
|
33
|
DeNardo P, Bruni B, Paoletti L, et al:
Pulmonary fibre burden in sheep living in the Biancavilla area
(Sicily): preliminary results. Sci Total Environ. 325:51–58. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Rapisarda V, Rapisarda G, Vico GD, et al:
Monitoring of fluoro-edenite fibre pollution through the study of
sheep lymph nodes as a model of a biological indicator. Occup
Environ Med. 62:6562005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kilburn KH, Powers D and Warshaw RH:
Pulmonary effects of exposure to fine fibreglass: irregular
opacities and small airways obstruction. Br J Ind Med. 49:714–720.
1992.PubMed/NCBI
|
|
36
|
Albin M, Engholm G, Hallin N and Hagmar L:
Impact of exposure to insulation wool on lung function and cough in
Swedish construction workers. Occup Environ Med. 55:661–667. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sripaiboonkij P, Sripaiboonkij N,
Phanprasit W and Jaakkola MS: Respiratory and skin health among
glass microfiber production workers: a cross-sectional study.
Environ Health. 8:362009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Pairon J, Laurent F, Rinaldo M, et al:
Pleural plaques and the risk of pleural mesothelioma. J Natl Cancer
Inst. 105:293–301. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Elshazley M, Shibata E, Hisanaga N, et al:
Pleural plaque profiles on the chest radiographs and CT scans of
asbestos-exposed Japanese construction workers. Ind Health.
49:626–633. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Metintas M, Metintas S, Hillerdal G, et
al: Nonmalignant pleural lesions due to environmental exposure to
asbestos: A field-based, cross-sectional study. Eur Respir J.
26:875–880. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Hillerdal G and Henderson DW: Asbestos,
asbestosis, pleural plaques and lung cancer. Scand J Work Environ
Health. 23:93–103. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Hillerdal G: Pleural plaques and risk for
bronchial carcinoma and mesothelioma. A prospective study. Chest.
105:144–150. 1994.
|
|
43
|
Perticaroli P, Mengucci R, Carletti M, et
al: Asbestos-related diseases in former asbestos-cement workers in
Senigallia. Med Lav. 104:277–288. 2013.[(In Italian)]. PubMed/NCBI
|
|
44
|
American Thoracic Society, . Diagnosis and
initial management of nonmalignant diseases related to asbestos. Am
J Respir Crit Care Med. 170:691–715. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kamp DW and Weitzman SA: The molecular
basis of asbestos induced lung injury. Thorax. 54:638–652. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kamp DW: Asbestos-induced lung diseases:
an update. Transl Res. 153:143–152. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Soffritti M, Minardi F, Bua L, et al:
First experimental evidence of peritoneal and pleural mesotheliomas
induced by fluoro-edenite fibres present in Etnean volcanic
material from Biancavilla (Sicily, Italy). Eur J Oncol. 9:169–175.
2004.
|
|
48
|
Loreto C, Rapisarda V, Carnazza ML, et al:
Fluoro-edenite fibres induce lung cell apoptosis: an in vivo study.
Histol Histopathol. 23:319–326. 2008.PubMed/NCBI
|
|
49
|
Martinez G, Musumeci G, Loreto C and
Carnazza ML: Immunohistochemical changes in vulnerable rat brain
regions after reversible global brain ischaemia. J Mol Histol.
38:295–302. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Travaglione S, Bruni B, Falzano L, et al:
Effects of the new-identified amphibole fluoro-edenite in lung
epithelial cells. Toxicol In Vitro. 17:547–552. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Cardile V, Renis M, Scifo C, et al:
Behaviour of the new asbestos amphibole fluor-edenite in different
lung cell systems. Int J Biochem Cell Biol. 36:849–860. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Ledda C, Rapisarda V, Bracci M, et al:
Professional exposure to basaltic rock dust: assessment by the
Vibrio fischeri ecotoxicological test. J Occup Med Toxicol.
8:232013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Chiappino G, Sebastien P and Todaro A:
Atmospheric asbestos pollution in the urban environment: Milan,
Casale Monferrato, Brescia, Ancona, Bologna and Florence. Med Lav.
82:424–438. 1991.[(In Italian)]. PubMed/NCBI
|