Introduction
Acute myeloid leukemia (AML) is a hematological
malignancy with heterogeneous clinical presentations and subtypes.
AML has been further classified by the French-American-British
Cooperative Group (1–4) and the World Health Organization
(5,6)
based on the clinical features, and the biological, morphological,
immunological and cytogenetic characteristics of the disease. The
most common induction therapies for the treatment of adult AML have
not changed significantly over the past four decades, and these are
chemotherapy or stem cell transplantation (7–9).
Although efforts have been made to develop novel
anticancer agents, the overall prognosis for AML has remained poor,
particularly amongst older patients. The biological characteristics
and clinical features of AML in older adults are different from
younger patients, with higher rates of resistance and a poorer
response to chemotherapy (10,11).
Approximately 70–80% of younger adults achieve complete remission
(CR), with a 5-year-survival rate of ~40–45% (12). By contrast, CR is achieved in ~40–65%
elderly patients (12) and
5-year-survival rates are ≤10% (13).
The most common cause of treatment failure for AML in elderly
patients is refractory AML. The underlying mechanism for this
resistance of AML to treatment remains unclear (14). Thus, an in-depth understanding of the
molecular mechanisms associated with refractory AML is
required.
Leukemic stem cells (LSCs), which are also termed
leukemia-initiating cells, have been reported to be the origin of
leukemic cells (15). LSCs serve key
functions in the initiation and progression of leukemia and also in
relapse or refractory AML, leading to resistance to induction
therapies and poor survival outcomes (16). Several LSC biomarkers have been
reported to be correlated with refractory or relapse AML and poor
prognosis, which may provide instructive information for diagnosis,
progression or treatment (17). The
LSC surface marker CD44 and components of LSC-associated pathways,
including phosphatase and tensin homologue (PTEN), phosphoinositide
3-kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) and
nuclear factor-κB (NF-κB), have been demonstrated to have
prognostic value for adult AML patients (18). Previous studies have demonstrated that
increased expression levels of CD44 in hematological malignancies
is correlated with poor clinical outcomes (19,20). It
has also previously been reported that patients in receipt of
autologous hematopoietic stem cell transplantations exhibited lower
expression levels of CD44 and improved survival outcomes (21). However, the reliability of the
correlation between these LSC-associated biomarkers and the
prognosis of patients with refractory AML is currently
insufficient.
In the present study, the expression levels of CD44,
PTEN, mTOR and NF-κB were evaluated in elderly refractory AML
patients to determine whether these molecules have prognostic
implications and may be potential therapeutic targets for
treatment.
Materials and methods
Patients and tissue samples
Bone marrow (BM) samples were obtained from 20
elderly patients with diagnosed refractory AML (2,22), who
were treated at Dongzhimen Hospital (Beijing, China) between
December 2011 and April 2013, and possessed complete clinical
pathological diagnosis information and the associated follow-up
data. The induction chemotherapy drugs that were administered to
the patients were Acla, Ara-C, cytoxan, vindesine, epirubicin and
VP-16. The bone marrow samples were divided into two groups: CR
(n=9) and NR (n=11), following induction chemotherapy treatment. CR
was defined as patients with ≤5% leukemic blasts in the BM with
signs of normal hematopoiesis and regeneration of normal
peripheral-blood cell production (platelets >1×1011/l
without transfusions, neutrophils >1.5×109/l) and an
absence of leukemic cells in the peripheral blood or other
locations (22). The refractory AML
diagnosis for all patients in the study was confirmed
histologically and cytologically. The mean age at diagnosis was
62.05±8.24 years and the range was 51–77 years, 11 patients were
male and 8 patients were female. All the patients were followed up
until June 2014 or death. The study was approved by the ethics
committee of Dongzhimen Hospital and all samples were acquired
following informed consent and ethical approval.
Immunohistochemistry
Immunohistochemical (IHC) analysis was performed as
previously described (23), with
minor modifications. Briefly, sections (4-µm thick) from the
paraffin-embedded bone marrow biopsy specimens were collected,
deparaffinized, hydrated, heated for antigen retrieval and treated
with 1% bovine albumin serum (Sigma-Aldrich) to prevent
non-specific binding. Rabbit anti-human PTEN (1:125; Cell Signaling
Technology, Inc., Danvers, MA, USA), rabbit anti-human NF-κB
(1:300; Cell Signaling Technology, Inc.), rabbit anti-human mTOR
(1:200; Abcam, Cambridge, MA, USA) and rabbit anti-human CD44
(1:100; Abcam) were used as the primary antibodies. Non-specific
rabbit anti-human immunoglobulin G (1:200; Abcam) was used as a
negative control. Following washing with phosphate-buffered saline
(PBS), the sections were incubated with the primary antibodies
overnight at 4°C. Next, the sections were washed three times with
PBS and incubated with goat anti-rabbit IgG secondary antibody
(1:2,000; Abcam) for 30 min at 37°C. The sections were
counterstained with 5 g/l hematoxylin (Dako North America, Inc.,
Carpinteria, CA, USA) and 20 µl/ml diaminobenzidine (Dako North
America, Inc.) using the Cytomation Envision Plus peroxidase system
(Dako North America, Inc.).
Evaluation of immunohistochemical
staining
The intensity of the IHC staining was
semi-quantitatively scored using a previously described method
(24,25). Briefly, according to the positive area
that was occupied, expression levels were scored as: - (0,
negative), + (1–20%, weak), ++ (20–50%, moderate) and +++ (>50%,
strong) (26,27). Images of the sections were captured
using a microscope (BX51; Olympus Corp., Tokyo, Japan) and a SPOT
Imaging Solutions system (Diagnostic Instruments, Inc., Sterling
Heights, MI, USA), and analyzed with Image-Pro Plus software,
version 6.0 (Media Cybernetics, Inc., Rockville, MD, USA). All the
areas were selected from five random visual fields. The mean
densitometry of the digital images (magnification, ×400) were
designated as representative staining intensities of PTEN, CD44,
mTOR, PI3K and NF-κB, in order to determine the relative expression
levels. All the slides were independently evaluated by two
specialized pathologists in a blinded manner, and subjected to
statistical analysis.
Statistical analysis
Values are expressed as the mean ± standard
deviation. The statistical evaluations were performed with SPSS
software, version 17.0 (SPSS, Inc., Chicago, IL, USA). P<0.05
was considered to indicate a statistically significant difference.
Semi-quantitative results were evaluated using the χ2
test. The mean density of protein expressions were measured by
Image-Pro Plus and two sample t-tests were used when data were
normally distributed, otherwise, non-parametric and Wilcoxon rank
sum tests were used for analysis. The correlation was studied using
Pearson's coefficient. The cumulative OS analysis was plotted using
Kaplan-Meier curves with log rank analysis. The variables were then
analyzed by multivariate Cox regression analysis, which was
performed to identify independent prognostic survival factors.
Results
Patient characteristics
A total of 20 bone marrow samples from AML patients
were divided into two groups: The CR and NR groups. The median age
of the patients was 59 years (range, 51–77 years). The demographics
and baseline characteristics of the elderly refractory AML patients
are presented in Table I. When
comparing the CR and NR groups, the percentage of bone marrow
blasts, peripheral blood blasts and the total bilirubin levels were
significantly higher in the NR group when compared with the CR
group (P<0.05; Table I). These
results indicated that patients in the CR and NR groups exhibited
different responses to therapy. The percentage of bone marrow
blasts was also significantly associated with PTEN expression
(P=0.016; Table II); the percentage
of bone marrow blasts was significantly higher in PTEN-negative
cases when compared with PTEN-positive cases (P=0.016). It has
previously been demonstrated that AML patients with lower bone
marrow blast percentages following therapy may exhibit a better
prognosis (28,29). Thus, the results of the present study
indicate that PTEN expression may also affect the prognosis of AML
patients.
 | Table I.Demographics and baseline
characteristics of elderly refractory acute myeloid leukemia
patients. |
Table I.
Demographics and baseline
characteristics of elderly refractory acute myeloid leukemia
patients.
| A,
Demographics |
|---|
|
|---|
| Characteristic | CR, n (%) | NR, n (%) | P-value |
|---|
| Number |
9 |
11 |
|
| Gender |
|
|
|
|
Female |
4 (44.4) |
3 (27.3) | 0.42 |
|
Male |
5 (55.6) |
8 (72.7) |
|
| Age, years |
|
|
|
|
Median | 58 | 60 | 0.94 |
|
Range | 55–77 | 51–73 |
|
|
| B, Baseline
laboratory values |
|
| Laboratory
values | Median (range) | Median (range) | P-value |
| White blood cell,
×109/l |
3.6 (1.7–8.8) |
4.5
(1.8–26.1) | 0.57 |
| Platelet count,
×109/l |
109 (43–226) |
80 (7–354) | 0.31 |
| Hemoglobin,
g/l |
109 (81–130) |
82 (53–142) | 0.13 |
| Bone marrow blasts,
% | 0.62 (0–3) |
30 (18–94.5) | 0.00 |
| Peripheral blood
blasts, % | 0.00
(0.00–2.59) |
33 (1–80) | 0.00 |
| Total bilirubin,
µmol/l | 10.5 (5.5–22) | 21.8 (8–96) | 0.02 |
| Creatinine,
µmol/l | 55.7 (49.3–76) | 64.1
(38.1–90.4) | 0.96 |
| Table II.Correlation between PTEN and CD44
expression and baseline characteristics. |
Table II.
Correlation between PTEN and CD44
expression and baseline characteristics.
|
| CD44 | PTEN |
|---|
|
|
|
|
|---|
| Characteristic | Positive | Negative | P-value | Positive | Negative | P-value |
|---|
| Number, n | 9 | 11 |
| 10 | 10 |
|
| Gender, n (%) |
|
|
|
|
|
|
|
Female | 4 (44.4) | 4 (33.3) | 0.604 | 4 (40.0) | 7 (70.0) | 0.64 |
|
Male | 5 (55.6) | 8 (66.7) |
| 6 (60.0) | 3 (30.0) |
|
| Age, years |
|
|
|
|
|
|
|
Median | 58 | 60 | 0.400 | 65 | 60 | 0.19 |
|
Range | 51–72 | 55–77 |
| 55–77 | 51–73 |
|
| Laboratory values,
median (range) |
|
|
|
|
|
|
| WBC,
×109/l | 4.4 (1.8–21.0) | 3.6 (1.7–26.1) | 0.856 | 4 (1.7–18.7) | 3.9 (1.8–26.1) | 0.76 |
|
Platelet count,
×109/l | 74 (7–147) | 106 (43–354) | 0.341 | 106 (43–226) | 95 (7–354) | 0.93 |
|
Hemoglobin, g/l | 82 (61–130) | 109 (53–142) | 0.341 | 111.5 (71–130) | 83 (53–142) | 0.12 |
| Bone
marrow blasts, % | 22 (0–44) | 2 (0–94.5) | 0.526 | 0.81 (0–60.5) | 26.5 (2–94.5) | 0.02 |
|
Peripheral blood blasts,
% | 4 (0–80) | 0.15 (0–52) | 0.312 | 0 (0–52) | 4 (0–80) | 0.06 |
| Total
bilirubin, µmol/l | 18.4 (8–96) | 16.7
(5.5–34.5) | 0.704 | 10.5
(5.5–34.5) | 20.3 (18–96) | 0.14 |
|
Creatinine, µmol/l | 48.8
(38.1–74.5) | 63.2 (52–90.4) | 0.056 | 60.5 (49.3–76) | 52 (38–90) | 0.35 |
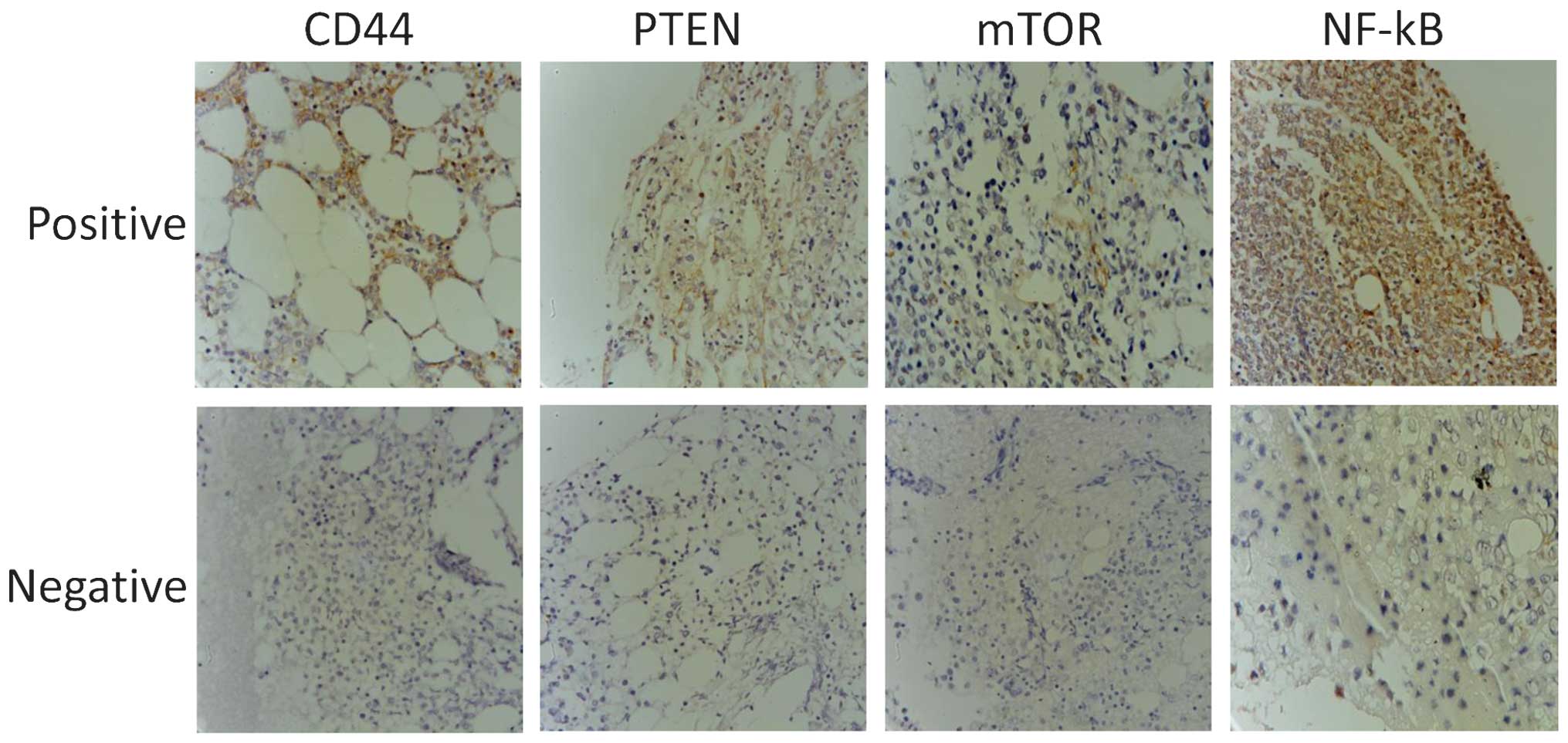
PTEN and CD44 are differentially
expressed between the two groups
IHC was used to determine the expression levels of
PTEN, CD44, mTOR and NF-κB in the patient samples. Representative
immunohistochemical stains are presented in Fig. 1. In the CR group the mean densities
were as follows: PTEN, 277.32±283.25; CD44, 408.45±303.47; mTOR,
205.72±242.53; and NF-κB, 642.66±312.21. In the NR group the mean
densities were: PTEN, 109.59±60.85; CD44, 840.06±335.95; mTOR,
285.79±242.53; and NF-κB, 776.26±380.63, as presented in Fig. 2. The results demonstrated that the
PTEN expression levels in the CR group were significantly
increased, compared with those of the NR group (P=0.025), whereas
CD44 was expressed at significantly reduced levels in the CR group
compared with that of the NR group (P=0.020, Fig. 2). By contrast, slightly increased
expression levels of NF-κB and mTOR were observed in the NR group
compared with those of the CR group, although these differences
were not statistically significant (P>0.05, Fig. 2). Furthermore, statistical correlation
analysis demonstrated that there was a negative correlation between
the expression levels of PTEN and CD44 (R=-0.415, P=0.069; Fig. 3).
CD44 and PTEN expression levels are
associated with patient outcomes
The present study then analyzed whether CD44 and
PTEN expression levels were associated with patient outcomes.
Kaplan-Meier analysis demonstrated that the mean OS for the CR
group was 10.0 months, which was significantly increased compared
with that of the NR group (4.27 months; P=0.009). CD44 expression
levels were significantly associated with the OS in all patients:
Patients that were CD44 positive had a mean OS of ~4.0 months,
whereas CD44-negative patients had a mean OS of 9.27 months. The
hazard ratio was 6.281 (95%CI, 1.78–22.12; P=0.0042; Fig. 4C). Multivariate Cox regression
analysis also demonstrated that CD44 was an independent prognostic
survival factor for patients with refractory AML (P=0.019; Table III). There was also a trend towards
reduced OS in patients who were PTEN negative when compared with
patients who were PTEN positive (mean OS, 4.81 months vs. 8.8
months; hazard ratio, 2.689; 95% CI, 0.89–8.08; P=0.078; Fig. 4B). The correlation between PTEN
positive and CD44 negative or PTEN negative and CD44 positive
patients with OS, was assessed using Kaplan-Meier analysis.
Patients that were PTEN positive and CD44 negative had
significantly increased OS compared with those that were PTEN
negative and CD44 positive. The mean OS for patients that were PTEN
negative and CD44 positive was 9.86 months, whereas the mean OS for
patients that were PTEN negative and CD44 positive was 2.67 months.
The hazard ratio was 0.037 (95% CI, 0.006–0.222; P=0.0006; Fig. 4D).
| Table III.Univariate and multivariate analysis
of overall survival in elderly patients with refractory acute
myeloid leukemia. |
Table III.
Univariate and multivariate analysis
of overall survival in elderly patients with refractory acute
myeloid leukemia.
|
| Univariate survival
analysis | Multivariate
survival analysis |
|---|
|
|
|
|
|---|
| Variable | Risk ratio (95%
CI) | P-value | Risk ratio (95%
CI) | P-value |
|---|
| Gender | 1.069
(0.391–2.923) | 0.896 | 0.502
(0.014–17.64) | 0.704 |
| Age | 0.999
(0.938–1.064) | 0.975 | 1.245
(0.978–1.584) | 0.075 |
| White blood
cell | 1.117
(1.033–1.208) | 0.006 | 1.266
(1.017–1.576) | 0.035 |
| Platelet count | 0.995
(0.987–1.004) | 0.303 | 0.945
(0.893–0.995) | 0.033 |
| Hemoglobin | 0.983
(0.961–1.005) | 0.136 | 1.036
(0.926–1.160) | 0.534 |
| Bone marrow
blasts | 1.017
(0.999–1.036) | 0.058 | 1.161
(1.003–1.343) | 0.046 |
| Peripheral blood
blasts | 1.021
(1.001–1.041) | 0.039 | 0.881
(0.783–0.991) | 0.035 |
| Total
bilirubin | 1.025
(0.999–1.052) | 0.059 | 0.943
(0.875–1.02) | 0.126 |
| Creatinine | 0.982
(0.942–1.023) | 0.392 | 1.112
(1.005–1.223) | 0.039 |
| PTEN positive | 0.372
(0.123–1.117) | 0.078 | 0.000
(0.913–31.81) | 0.056 |
| CD44 positive | 6.281
(1.784–22.12) | 0.004 | 30.69
(0.000–0.208) | 0.019 |
Discussion
In the present study, IHC staining was used to
detect the expression of CD44, PTEN, mTOR and NF-κB in elderly
patients with refractory AML, who were divided into CR and NR
groups. It has previously been reported that an increase in CD44
expression contributes to poorer AML prognosis, and CD44 may
therefore serve as an adverse prognostic marker (25). The present study indicated that CD44
expression was significantly increased in the NR group compared
with that of the CR group. Increased CD44 expression was associated
with significantly reduced OS compared with that of CD44 negative
patients, which was consistent with the results of a previous
report (30). CD44 is a cell surface
glycoprotein involved in diverse cellular processes in malignancy,
including cell transformation (31),
proliferation (31), migration
(32) and anti-apoptosis (33). CD44 is also considered to be one of
the particular markers that mediate efficient homing and
engraftment of LSC in AML (34–36). In
addition, CD44 expression is specific to LSC as it is rarely
expressed on normal hematopoietic stem cells (37,38).
Previous studies have demonstrated that CD44 knockout
(CD44−/−) mice survived significantly longer and that
tumors developed more slowly compared with those of wild-type mice,
when injected with murine breast carcinoma cells (30). The expression of CD44 may be
associated with adverse prognosis of AML (39), which is consistent with the results
obtained in the present study.
In contrast to the expression of CD44, PTEN
expression was significantly increased in the CR group compared
with that of the NR group. Patients that were PTEN positive tended
to have an improved prognosis compared with those that were PTEN
negative, although the difference was not statistically
significant, possibly due to the relatively small sample size used
in the present study. PTEN is a tumor suppressor gene, which is
critical for cell proliferation, apoptosis and survival (40–42), and
is commonly inactivated in hematological malignancies, resulting in
loss of function (42,43). Loss of PTEN function has been
demonstrated to be associated with tumor progression (44) and poor prognosis (45), by disturbing the balance of
microenvironments, transforming normal stem cells into cancer stem
cells (46–48) or promoting the generation of LSCs into
unlimited self-renewal (49). The
absence of PTEN expression is considered to promote leukemia
development and be associated with poor patient outcomes. The
results of the present study indicate that further studies with
more homogeneous patient samples are required in order to draw
conclusions regarding the association between expression of PTEN
with the outcome of refractory AML.
It has previously been reported that knockdown of
PTEN may upregulate CD44 expression in hepatoma cells and human
Huh-7 cells (50). In the present
study, when PTEN expression was reduced, OS was significantly
improved in the CR group compared with that of the NR group.
Furthermore, a significant association between CD44 and PTEN
expression was identified. PTEN positive and CD44 negative cases
demonstrated a strong correlation with enhanced OS. Analysis of
CD44 and PTEN expression was combined and the results demonstrated
that there was negative correlation between them. The results of
the present study indicate that CD44 may be an adverse prognostic
marker, whereas PTEN presents as a favorable biomarker in
refractory AML.
PTEN has been shown to negatively regulate the
PI3K/Akt/mTOR and NF-κB signaling pathways (51), and NF-κB and PI3K/Akt/mTOR signaling
is known to be involved in multiple types of cancer (52), promoting carcinogenesis, cancer cell
proliferation and apoptosis (27,53). It
has previously been reported that the PI3K/Akt/mTOR signaling
pathway may be a prognostic marker in gastric cancer. NF-κB is
activated in hematological and solid tumors (54), and has also been demonstrated to be an
adverse prognostic factor (55). In
children with acute lymphoblastic leukemia, increased expression of
NF-κB is associated with treatment failure (56). PI3K/Akt/mTOR also activates downstream
signaling of Bcr-Abl, which leads to treatment failure and poor
clinical outcomes in patients with imatinib (Bcr-Abl
inhibitor)-resistant chronic myeloid leukemia (57). The results of the present study
demonstrated that there was increased expression of NF-κB and mTOR
in the NR group compared with that of the CR group. However, this
increase was not statistically significant, potentially due to the
small sample sizes.
In conclusion, the present study provides
immunohistochemical evidence that CD44 and PTEN may be used as
biomarkers for AML prognosis and for monitoring the response to
therapy, which may aid the identification of additional potential
strategies to treat refractory disease. The present study used an
elderly patient population (>50 years of age) as AML is
predominantly diagnosed in elderly patients (1). Notably, older AML patients exhibit a
poor prognosis, higher resistance rate and a poorer response to
chemotherapy compared with younger patients (2,3). In
addition, a CR may only be achieved in 40–65% of elderly
patients(4) and in patients >55
years of age, the 5-year-survival rate is <10% (5). Thus, the elderly population (>50
years of age) were selected for this study with the aim of
improving outcomes and the efficacy of treatments for AML. Since
CD44, PTEN, mTOR and NF-κB are involved in AML progression and have
been demonstrated to affect prognosis, the correlation observed
between these biomarkers and prognostic implications in the elderly
population may be observed in younger patients, which presents an
interesting topic for further research. The present study had
certain limitations due to the small sample size, therefore a study
with a larger sample size is required to further validate the
findings.
Acknowledgements
The present study was funded by the Specialized
Research Fund for the Doctoral Program of Higher Education (grant
no. 20100013110008). The authors would like to thank Dr Bingliang
Fang (University of Texas MD Anderson Cancer Center, Houston, TX,
USA) and Dr Bingbing Dai (University of Texas MD Anderson Cancer
Center) for language editing and polishing.
References
|
1
|
Bennett JM, Catovsky D, Daniel MT, et al:
Proposals for the classification of the acute leukaemias
French-American-British (FAB) co-operative group. Br J Haematol.
33:451–458. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bennett JM, Catovsky D, Daniel MT, et al:
Proposed revised criteria for the classification of acute myeloid
leukemia A report of the French-American-British Cooperative Group.
Ann Intern Med. 103:620–625. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bennett JM, Catovsky D, Daniel MT, et al:
Criteria for the diagnosis of acute leukemia of megakaryocyte
lineage (M7). A report of the French-American-British Cooperative
Group. Ann Intern Med. 103:460–462. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bennett JM, Catovsky D, Daniel MT, et al:
Proposal for the recognition of minimally differentiated acute
myeloid leukaemia (AML-MO). Br J Haematol. 78:325–329. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Harris NL, Jaffe ES, Diebold J, et al: The
World Health Organization classification of neoplasms of the
hematopoietic and lymphoid tissues: Report of the Clinical Advisory
Committee meeting - Airlie House, Virginia, November, 1997. Hematol
J. 1:53–66. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vardiman JW, Thiele J, Arber DA, et al:
The 2008 revision of the World Health Organization (WHO)
classification of myeloid neoplasms and acute leukemia: Rationale
and important changes. Blood. 114:937–951. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yates JW, Wallace HJ Jr, Ellison RR and
Holland JF: Cytosine arabinoside (NSC-63878) and daunorubicin
(NSC-83142) therapy in acute nonlymphocytic leukemia. Cancer
Chemother Rep. 57:485–488. 1973.PubMed/NCBI
|
|
8
|
Rai KR, Holland JF, Glidewell OJ, et al:
Treatment of acute myelocytic leukemia: A study by cancer and
leukemia group B. Blood. 58:1203–1212. 1981.PubMed/NCBI
|
|
9
|
O'Donnell MR, Abboud CN, Altman J, et al:
Acute myeloid leukemia. J Natl Compr Canc Netw. 10:984–1021.
2012.PubMed/NCBI
|
|
10
|
Swords R and Santini V: In elderly
patients with AML, which patients should be considered fit or unfit
for standard induction therapy? Hematology Am Soc Hematol Educ
Program. 2012:74–75. 2012.PubMed/NCBI
|
|
11
|
Yanada M and Naoe T: Acute myeloid
leukemia in older adults. Int J Hematol. 96:186–193. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Burnett A, Wetzler M and Löwenberg B:
Therapeutic advances in acute myeloid leukemia. J Clin Oncol.
29:487–494. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dombret H, Raffoux E and Gardin C: Acute
myeloid leukemia in the elderly. Semin Oncol. 35:430–438. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Krug U, Büchner T, Berdel WE and
Müller-Tidow C: The treatment of elderly patients with acute
myeloid leukemia. Dtsch Arztebl Int. 108:863–870. 2011.PubMed/NCBI
|
|
15
|
Jordan CT: The leukemic stem cell. Best
Pract Res Clin Haematol. 20:13–18. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
She M, Niu X, Chen X, et al: Resistance of
leukemic stem-like cells in AML cell line KG1a to natural killer
cell-mediated cytotoxicity. Cancer Lett. 318:173–179. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ardekani AM, Akhondi MM and Sadeghi MR:
Application of genomic and proteomic technologies to early
detection of cancer. Arch Iran Med. 11:427–434. 2008.PubMed/NCBI
|
|
18
|
Biomarkers Definitions Working Group, .
Biomarkers and surrogate endpoints: Preferred definitions and
conceptual framework. Clin Pharmacol Ther. 69:89–95. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eisterer W, Bechter O, Hilbe W, et al:
CD44 isoforms are differentially regulated in plasma cell
dyscrasias and CD44v9 represents a new independent prognostic
parameter in multiple myeloma. Leuk Res. 25:1051–1057. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Niitsu N and Iijima K: High serum soluble
CD44 is correlated with a poor outcome of aggressive non-Hodgkin's
lymphoma. Leuk Res. 26:241–248. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Krause DS, Spitzer TR and Stowell CP: The
concentration of CD44 is increased in hematopoietic stem cell
grafts of patients with acute myeloid leukemia, plasma cell
myeloma, and non-Hodgkin's lymphoma. Arch Pathol Lab Med.
134:1033–1038. 2010.PubMed/NCBI
|
|
22
|
Mi Y and Bian S: Acute
leukemiaStandardization of Hematologic Disease Diagnosis and the
Therapeutic Effect. Zhinan Z and Ti S: 1. 3rd. Science Press;
Beijing, China: pp. 131–134. 2007
|
|
23
|
Wang Z, Zheng T, Wu Q and Wang J, Wu C and
Wang J: Immunohistochemical analysis of the mTOR pathway in
intrahepatic cholangiocarcinoma. Neoplasma. 59:137–141. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hu J, Liu YL, Piao SL, et al: Expression
patterns of USP22 and potential targets BMI-1, PTEN, p-AKT in
non-small-cell lung cancer. Lung Cancer. 77:593–599. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cao L, Hu X, Zhang J, Liang P and Zhang Y:
CD44 U(+) CD324(–) expression and prognosis in gastric cancer
patients. J Surg Oncol. 110:727–733. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Opitz I, Soltermann A, Abaecherli M, et
al: PTEN expression is a strong predictor of survival in
mesothelioma patients. Eur J Cardiothorac Surg. 33:502–506. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tapia O, Riquelme I, Leal P, et al: The
PI3K/AKT/mTOR pathway is activated in gastric cancer with potential
prognostic and predictive significance. Virchows Arch. 465:25–33.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sebban C, Browman GP, Lepage E and Fière
D: Prognostic value of early response to chemotherapy assessed by
the day 15 bone marrow aspiration in adult acute lymphoblastic
leukemia: A prospective analysis of 437 cases and its application
for designing induction chemotherapy trials. Leuk Res. 19:861–868.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Cortes J, Fayad L, O'Brien S, Keating M
and Kantarjian H: Persistence of peripheral blood and bone marrow
blasts during remission induction in adult acute lymphoblastic
leukemia confers a poor prognosis depending on treatment intensity.
Clin Cancer Res. 5:2491–2497. 1999.PubMed/NCBI
|
|
30
|
Fitzgerald KA, Bowie AG, Skeffington BS
and O'Neill LA: Ras, protein kinase C zeta, and I kappa B kinases 1
and 2 are downstream effectors of CD44 during the activation of
NF-kappa B by hyaluronic acid fragments in T-24 carcinoma cells. J
Immunol. 164:2053–2063. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bourguignon LY, Zhu H, Shao L, Zhu D and
Chen YW: Rho-kinase (ROK) promotes CD44v(3,8–10)-ankyrin
interaction and tumor cell migration in metastatic breast cancer
cells. Cell Motil Cytoskeleton. 43:269–287. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lin YH and Yang-Yen HF: The
osteopontin-CD44 survival signal involves activation of the
phosphatidylinositol 3-kinase/Akt signaling pathway. J Biol Chem.
276:46024–46030. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Dick JE, Bhatia M, Gan O, Kapp U and Wang
JC: Assay of human stem cells by repopulation of NOD/SCID mice.
Stem Cells. 15:199–207. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Krause DS and Van Etten RA: Right on
target: Eradicating leukemic stem cells. Trends Mol Med.
13:470–481. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Oelschlaegel U, Bornhauser M, Boxberger S,
et al: Kinetics of CXCR-4 and adhesion molecule expression during
autologous stem cell mobilisation with G-CSF plus AMD3100 in
patients with multiple myeloma. Ann Hematol. 86:569–573. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
van Rhenen A, Moshaver B, Kelder A, et al:
Aberrant marker expression patterns on the CD34+CD38- stem cell
compartment in acute myeloid leukemia allows to distinguish the
malignant from the normal stem cell compartment both at diagnosis
and in remission. Leukemia. 21:1700–1707. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Buzzai M and Licht JD: New molecular
concepts and targets in acute myeloid leukemia. Curr Opin Hematol.
15:82–87. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Spaeth EL, Labaff AM, Toole BP, et al:
Mesenchymal CD44 expression contributes to the acquisition of an
activated fibroblast phenotype via TWIST activation in the tumor
microenvironment. Cancer Res. 73:5347–5359. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lane SW, Scadden DT and Gilliland DG: The
leukemic stem cell niche: Current concepts and therapeutic
opportunities. Blood. 114:1150–1157. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Maehama T and Dixon JE: The tumor
suppressor, PTEN/MMAC1, dephosphorylates the lipid second
messenger, phosphatidylinositol 3,4,5-trisphosphate. J Biol Chem.
273:13375–13378. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Stiles B, Groszer M, Wang S, Jiao J and Wu
H: PTENless means more. Dev Biol. 273:175–184. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Dahia PL, Aguiar RC, Alberta J, et al:
PTEN is inversely correlated with the cell survival factor Akt/PKB
and is inactivated via multiple mechanisms in haematological
malignancies. Hum Mol Genet. 8:185–193. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cheong JW, Eom JI, Maeng HY, et al:
Phosphatase and tensin homologue phosphorylation in the C-terminal
regulatory domain is frequently observed in acute myeloid leukaemia
and associated with poor clinical outcome. Br J Haematol.
122:454–456. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Squarize CH, Castilho RM, Abrahao AC, et
al: PTEN deficiency contributes to the development and progression
of head and neck cancer. Neoplasia. 15:461–471. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
da Costa AA, D'Almeida Costa F, Ribeiro
AR, et al: Low PTEN expression is associated with worse overall
survival in head and neck squamous cell carcinoma patients treated
with chemotherapy and cetuximab. Int J Clin Oncol. May
27–2014.(Epub ahead of print).
|
|
46
|
Hede K: PTEN takes center stage in cancer
stem cell research, works as tumor suppressor. J Natl Cancer Inst.
98:808–809. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
He XC, Yin T, Grindley JC, et al:
PTEN-deficient intestinal stem cells initiate intestinal polyposis.
Nat Genet. 39:189–198. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
48
|
Yilmaz OH, Valdez R, Theisen BK, et al:
Pten dependence distinguishes haematopoietic stem cells from
leukaemia-initiating cells. Nature. 441:475–482. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Tesio M, Oser GM, Baccelli I, et al: Pten
loss in the bone marrow leads to G-CSF-mediated HSC mobilization. J
Exp Med. 210:2337–2349. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Chu TH, Chan HH, Kuo HM, et al: Celecoxib
suppresses hepatoma stemness and progression by up-regulating PTEN.
Oncotarget. 5:1475–1490. 2014.PubMed/NCBI
|
|
51
|
Salminen A and Kaarniranta K:
Insulin/IGF-1 paradox of aging: Regulation via AKT/IKK/NF-kappaB
signaling. Cell Signal. 22:573–577. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Dubrovska A, Kim S, Salamone RJ, et al:
The role of PTEN/Akt/PI3K signaling in the maintenance and
viability of prostate cancer stem-like cell populations. In: Proc
Natl Acad Sci USA. 106. pp. 268–273. 2009; View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Kim HJ, Hawke N and Baldwin AS: NF-kappaB
and IKK as therapeutic targets in cancer. Cell Death Differ.
13:738–747. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Lee CH, Jeon YT, Kim SH and Song YS:
NF-kappaB as a potential molecular target for cancer therapy.
Biofactors. 29:19–35. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Breccia M and Alimena G: NF-κB as a
potential therapeutic target in myelodysplastic syndromes and acute
myeloid leukemia. Expert Opin Ther Targets. 14:1157–1176. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Kamieńska E, Ociepa T, Wysocki M, et al:
Activation of NF-κB in leukemic cells in response to initial
prednisone therapy in children with acute lymphoblastic leukaemia:
Relation to other prognostic factors. Pol J Pathol. 62:5–11.
2011.PubMed/NCBI
|
|
57
|
Lounnas N, Frelin C, Gonthier N, et al:
NF-kappaB inhibition triggers death of imatinib-sensitive and
imatinib-resistant chronic myeloid leukemia cells including T315I
Bcr-Abl mutants. Int J Cancer. 125:308–317. 2009. View Article : Google Scholar : PubMed/NCBI
|