Introduction
Bladder cancer is the fifth most common type of
malignant tumor. Among bladder malignancies, urothelial carcinomas
are the most frequent histological type, of which adenocarcinoma,
squamous cell cancer and small-cell cancer account for small
percentages (1,2). Primary adenocarcinomas were reported to
account for 0.5–2% of primary bladder epithelial malignancies;
these malignancies most commonly arise in the urachus (3). In addition, secondary adenocarcinomas
may also occur as a result of direct invasion from the surrounding
organs, including prostate, colorectal and cervical sites (3). Furthermore, metastatic spread may occur
via lymphogenous or hematogenous routes (4). However, the bladder is not a favored
site for tumor metastases; in particular, adenocarcinoma from the
lung is exceptionally rare (5). The
present study describes a case of metastatic adenocarcinoma from
the lung to the bladder and reports the histopathological
characteristics and immunohistochemical features of the patient.
The aim of the present study was to emphasize the importance of
considering of metastatic adenocarcinoma from the lung as a
possible diagnosis, in addition to primary adenocarcinoma and
direct invasion of adenocarcinoma from the immediate surrounding
organs.
Case report
A 71-year-old Chinese male with known lung cancer
for >2 years was referred to the People's Liberation Army 205
Hospital (Jinzhou, China) due to a gross hematuria, which had
persisted for 5 days. This initial diagnosis of lung adenocarcinoma
occurred >2 years previously, when the patient was admitted to a
local hospital due to a cough and expectoration. Following the
initial admission to hospital, a thoracic computed tomography (CT)
revealed a 3×2×2 cm mass in the lower lobe of the patient's left
lung; consequently, a needle biopsy was performed and the patient
was diagnosed with adenocarcinoma of the lung (histological
sections were not available for review). The patient elected not to
undergo any therapy, including surgical resection, chemical therapy
or radiotherapy. On admission to the People's Liberation Army 205
Hospital due to gross hematuria, ultrasonography of the pelvic
cavity was performed, which revealed a solid occupying lesion,
0.6×0.4×0.4 cm in size, within the right lateral wall of the
bladder. Consequently, a transurethral resection of a bladder tumor
was performed. During this procedure, the tumor was identified to
be pedunculated and conch-shaped with a smooth surface.
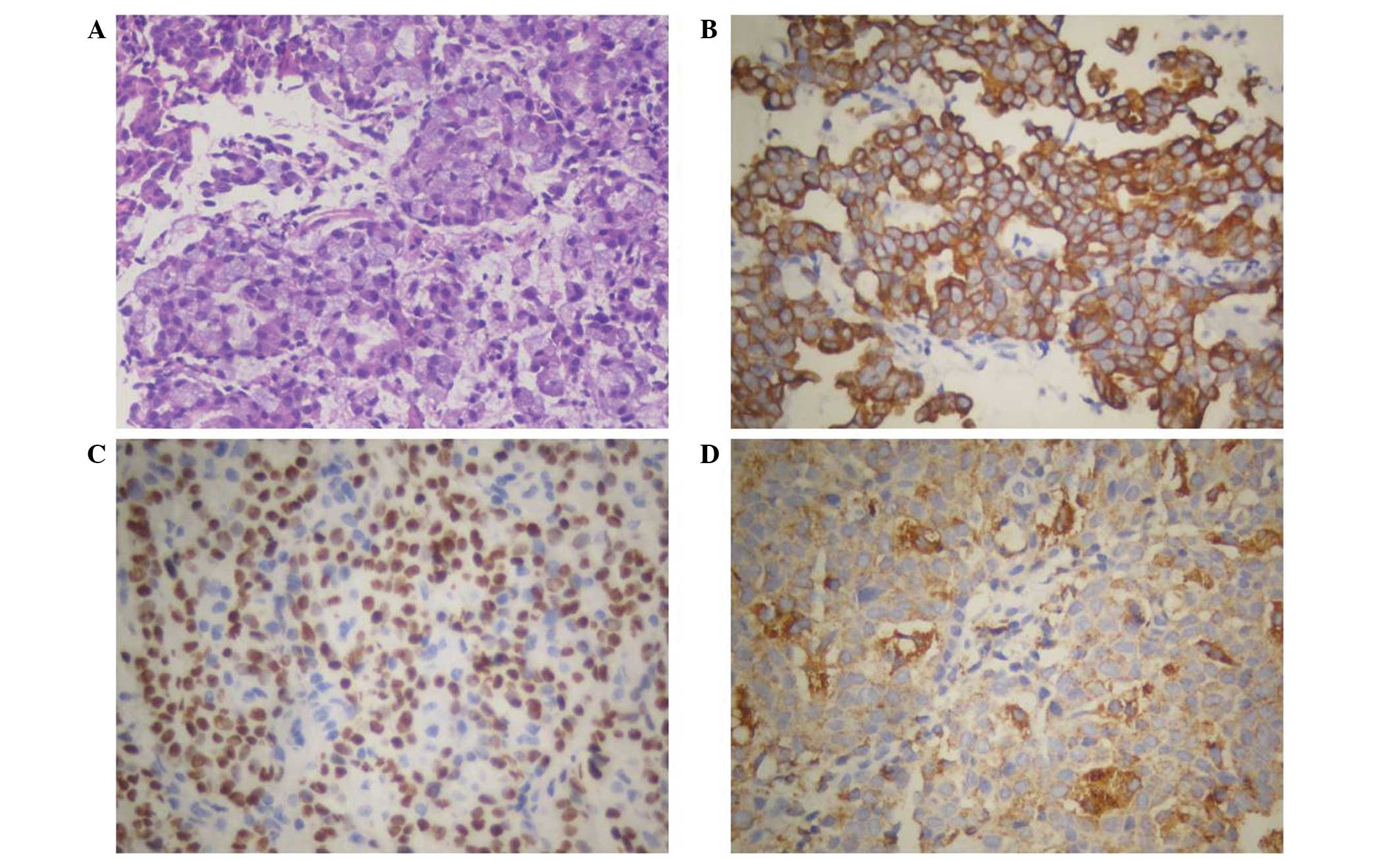
Histopathological analysis of the resected tumor revealed that the
tumor cells grew diffusely and were located beneath the intact
urothelial epithelium, without bladder muscle invasion; in
addition, mucus was identified in certain tumor cells, as
determined following hematoxylin and eosin staining (Fig. 1A). Immunohistochemically, the tumor
cells stained positively for cytokeratin (CK)7, thyroid
transcription factor-1 (TTF-1) and Napsin A (Fig. 1B–D, respectively); however, the tumor
cells were negative for CK20, prostate-specific antigen (PSA),
P504S, prostatic acid phosphatase (PAP) and caudel-type homeobox
(CDX)2. Combining the histopathological and immunohistochemical
features with the patient's clinical history, it was considered
that the tumor was a metastatic adenocarcinoma from the lung;
however, the primary tumor slides were not available for review.
This conclusion was reached as adenocarcinoma from the prostate
would usually express PSA, PAP and P504S, while adenocarcinoma from
the gastrointestinal tract are often positive for CK20 and CDX2.
Written informed consent was obtained from the patient prior to
publication of the present study.
Discussion
Cancer metastases to the bladder from adjacent
sites, including prostate, colorectal and cervical sites, are
common; whereas metastases from stomach, skin, breast and lung
primary tumors are less common (4).
Metastatic adenocarcinoma from the lung to the bladder is rare and
only six cases have been reported in the literature since 1997
(4–9).
Furthermore, in a retrospective study from 282 cases of secondary
bladder neoplasms, only one case (0.4%) originating from lung
adenocarcinoma was identified (5).
Among the six cases reported in the literature, four
cases presented clinical data, including age, gender and clinical
symptoms (4,7–9). The age
range of the subjects was 40–81 years, with a mean age of 66 years.
Three of the patients were male and one was female. Clinically,
hematuria and pelvic pain are often the presenting symptoms in
patients with secondary bladder cancer (10). Out of these previous studies, two
patients presented with gross hematuria, one presented with pain
and bilateral hydronephrosis, and one was initially referred to the
neurosurgical clinic for left carpal tunnel syndrome. However, both
patients were confirmed to have a history of primary lung cancer
following careful physical examination (8,9). In the
current case, the patient presented with a gross hematuria >2
years following diagnosis of the primary lung adenocarcinoma.
Ultrasonography of the pelvic cavity revealed a solid occupying
lesion, 0.6×0.4×0.4 cm in size, within the right lateral wall of
the bladder. Histopathological analysis identified the lesion as an
adenocarcinoma. Primary adenocarcinoma of the bladder and secondary
adenocarcinoma from its adjacent organs should be ruled out based
on immunohistochemical studies, which may be used to determine the
origin of the primary tumor from uncommon sites, such as
colorectal, breast or lung. Positive staining for TTF-1, CK7 and
Napsin A have been demonstrated to be reliable markers for the
identification of lung adenocarcinoma (2,11). In the
present case report, the tumor cells stained positive for TTF-1,
CK7 and Napsin A. In addition, the tumor cells were negative for
CK20, PSA, P504S, PAP and CDX2; thus, adenocarcinomas from the
prostate, rectum and stomach may be excluded.
In conclusion, it is proposed that in cases
comparable to the current study, pathologists should consider the
possibility of metastatic adenocarcinoma from the lung, rather than
primary adenocarcinoma of the bladder or direct invasion of
adenocarcinoma from the surrounding organs. Furthermore, it is
essential to determine the medical history of each patient and
observe the immunohistochemical features of all tumors prior to
diagnosis.
References
|
1
|
Howlader N, Noone AM, Krapcho M, et al:
SEER Cancer Statistics Review, 1975–2009 (Vintage 2009
Populations)National Cancer Institute; Bethesda, MD: 2012
|
|
2
|
Wasco MJ, Daignault S, Zhang Y, et al:
Urothelial carcinoma with divergent histologic differentiation
(Mixed Histologic Features) predicts the presence of locally
advanced bladder cancer when detected at transurethral resection.
Urology. 70:69–74. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thomas DG, Ward AM and Williams JL: A
study of 52 cases of adenocarcinoma of the bladder. Br J Urol.
43:4–15. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Modh RA, Corbyons KA and Yeung LL: A rare
metastasis to the bladder. Case Rep Urol.
2013:7890392013.PubMed/NCBI
|
|
5
|
Bates AW and Baithun SI: Secondary
neoplasms of the bladder are histological mimics of nontransitional
cell primary tumours: Clinicopathological and histological features
of 282 cases. Histopathology. 36:32–40. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Martín-Marquina Aspiunza A, Díez-Caballero
Alonso F, Rodríguez-Rubio Cortadellas FI, Díez Fernández L, Abad
Vivas-Pérez JI, et al: Bladder metastasis of lung adenocarcinoma.
Actas Urol Esp. 21:406–408. 1997.(In Spanish). PubMed/NCBI
|
|
7
|
Sakhri L, Mennecier B, Jacqmin D, Di Marco
A, Schumacher C, Chenard MP, Bergmann E and Quoix E: Atypical
metastatic site of lung adenocarcinoma. Rev Pneumol Clin.
67:375–379. 2011.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Karle W, Barazani Y and Tareen B: A rare
case of metastatic lung cancer to the bladder. Can Urol Assoc J.
6:E147–E149. 2012.PubMed/NCBI
|
|
9
|
Shirakawa H, Kozakai N, Sawafuji M,
Sugiura H and Hara S: Urinary bladder metastasis originating from
lung adenocarcinoma: A case definitively diagnosed by
immunohistochemistry. Urol J. 9:530–532. 2012.PubMed/NCBI
|
|
10
|
Acino SM and Hampel N: Renal cell
carcinoma presenting with gross haematuria from a solitary bladder
metastasis. Eur Urol. 15:294–296. 1988.PubMed/NCBI
|
|
11
|
Turner BM, Cagle PT, Sainz IM, et al:
Napsin A, a new marker for lung adenocarcinoma, is complementary
and more sensitive and specific than thyroid transcription factor 1
in the differential diagnosis of primary pulmonary carcinoma:
evaluation of 1674 cases by tissue microarray. Arch Pathol Lab Med.
136:163–171. 2012. View Article : Google Scholar : PubMed/NCBI
|