Introduction
The majority of patients (75–80%) exhibiting bladder
cancer (BC) typically present with papillary non-invasive (stage
pTa) or early invasive (stage pT1) urothelial tumours. The
remaining 20–25% of patients demonstrate more advanced,
muscle-invasive tumours (≥pT2) (1). A
total of 70% of patients exhibiting stage pTa or pT1 BC will
undergo recurrence, and up to 25% will develop muscle-invasive
tumours (2). Therefore, patients with
BC must be carefully monitored for signs of disease recurrence or
progression. However, to date, there are no established biomarkers
in clinical practice that are able to predict the risk of tumour
progression.
Based on genetic data, the 2004 World Health
Organization (WHO) classification indicates that urinary bladder
neoplasia may be subdivided into low- and high-grade lesions
(3). There are two genetic subtypes
of BC tumour, which possess marked differences in their levels of
genetic instability, and correspond to morphologically distinct
entities (4). The first of these
subtypes, the genetically stable category, includes low-grade
non-invasive papillary tumours. The second genetic subtype, the
genetically unstable category, encompasses high-grade and invasive
carcinomas, including pTaG3 and pTis, as well as ≥pT1, respectively
(3). Burger et al (5) compared the WHO 1973 and 2004 tumour
classification systems, and each system contributed significant
information regarding the progression of BC. The inter-observer
variability of the WHO 2004 grading system, however, remains an
unsolved problem for surgical pathology.
Fibroblast growth factor receptors (FGFRs) control
crucial signalling pathways, which are responsible for numerous
cellular functions, including proliferation and migration (6). FGFRs have been revealed to possess an
oncogenic role in numerous types of cancer (7). By contrast, FGFR signalling may also
have a suppressive effect on tumours (6). It has been established that BC possesses
a link with FGFR mutations, and ~50% of BCs possess somatic
mutations within the FGFR3 coding sequence (8). Mutation of FGFR3 is a common
feature of low-grade, non-invasive papillary urothelial BC,
occurring in ~75% of cases (9–12); while
occurring at a markedly lower frequency in high-grade invasive BC
(13,14), and rarely with adjacent carcinoma
in situ (9,14). Patients exhibiting primary BCs
accompanied by an activating FGFR3 mutation had
significantly improved disease-specific survival (DSS) when
compared with patients without FGFR3 mutations (11,15).
FGFR3 and TP53 mutations were revealed to be mutually
exclusive and may represent two distinct pathways for the
development of BC (11,16,17). In
these pathways, bladder cancer lesions with activating FGFR3
mutations represent a type of genetically stable, low-grade,
papillary tumour. In addition, amalgamation of the analysis of
FGFR3 mutations and Ki-67 immunohistochemistry, defined as
molecular grading, was revealed to be superior to other parameters
for predicting the progression and survival of patients exhibiting
BC (11).
FGFR3 mutation status in BC, and the
association of BC with the expression of FGFR3 protein, has
previously been examined (18,19). The
combination of WHO 2004 grading with FGFR3 mutation status
facilitated improved risk stratification for patients exhibiting
high-grade, non-muscle-invasive urothelial BC (5). However, studies of FGFR3
immunoreactivity and its clinical significance are uncommon
(20,21). Immunohistochemical detection of the
FGFR3 receptor may provide a simpler, cheaper and faster approach
for histopathological practice, compared with the current method of
determination of FGFR3 mutation status. Overall, FGFR3
protein has significant potential for use as a diagnostic and
prognostic marker, as well as a potential therapeutic target or
screening tool (22).
In order to study the prognostic and diagnostic
value of FGFR3 protein expression in urothelial BC, a large series
of unselected primary urothelial BC tumours were analysed for FGFR3
immunoreactivity and FGFR3 mutations in association with
tumour stage, WHO 2004 grade, multifocality, presence of adjacent
carcinoma in situ and patient outcome.
Patients and methods
Bladder cancer tissue microarray
(TMA)
As previously described (10), a TMA was generated using 255
consecutive, formalin-fixed, paraffin-embedded, primary urothelial
BC tissue samples obtained from the Institute of Pathology,
University of Regensburg (Regensburg, Germany). Clinical data were
obtained from the Central Tumour Registry, Regensburg (Germany),
and by telephone interviews when data could not be located. The
Institutional Review Board of the University of Regensburg
(Regensburg, Germany) approved the analysis of tissues from human
subjects. Haematoxylin and eosin-stained slides of all tumour
samples were evaluated by a single surgical pathologist (Dr Arndt
Hartman). Tumour stages and grades were assigned according to Union
for International Cancer Control and WHO 2004 criteria (www.uicc.org/). The growth pattern was determined for
all tumours classified as invasive (≥pT1). Papillary growth was
defined by the presence of a papillary tumour component (≥20%),
possessing a histological grade identical to that of the invasive
tumour. All other tumours were considered to possess a pattern of
solid growth. Clinicopathological data are summarised in Table I. Retrospective clinical follow-up
data were available regarding the end-points, defined as
recurrence-free survival (RFS) and disease-specific survival (DSS),
for all patients, and the median follow-up period was 75 months
(range, 0–147 months). The median follow-up period for censored
patients was 81 months. Recurrence was defined as the presence of
cystoscopically visible tumours, and was further confirmed by
histological verification. Data regarding progression-free survival
(PFS) were not available.
 | Table I.Patient and tumour characteristics
and results of molecular and immunohistochemical analyses. |
Table I.
Patient and tumour characteristics
and results of molecular and immunohistochemical analyses.
| Clinicopathological
variable | Cases,
na (%) |
|---|
| Age at diagnosis,
yearsb |
|
|
<70 | 141 (55.3) |
|
≥70 | 114 (44.7) |
| Gender |
|
|
Female | 64
(25.1) |
|
Male | 191 (74.9) |
| Tumour
stageb |
|
|
PUNLMP | 22
(8.6) |
|
pTa | 124 (48.6) |
|
pT1 | 48
(18.8) |
|
pT2 | 56 (22.0) |
|
pT3 | 2
(0.8) |
|
pT4 | 3
(1.2) |
| Histological
gradec |
|
| 1 | 81
(31.8) |
| 2 | 69
(27.1) |
| 3 | 105 (41.2) |
| Histological
graded |
|
|
Low | 150 (58.8) |
|
High | 105 (41.2) |
| Adjacent carcinoma
in situ |
|
| No | 222 (87.1) |
|
Yes | 33
(12.9) |
| Multiplicity |
|
|
Solitary | 53
(20.8) |
|
Multifocal | 202 (79.2) |
| Growth pattern |
|
|
Papillary | 207 (81.5) |
|
Solid | 47
(18.5) |
| FGFR3 gene |
|
|
Wild-type | 110 (52.9) |
|
Mutation | 98
(47.9) |
| FGFR3
immunohistochemistry |
|
|
Negative | 94
(45.4) |
|
Positive | 113 (54.6) |
Immunohistochemistry
Immunohistochemical analysis used an avidin-biotin
peroxidase method with a diaminobenzidine chromatogen. Following
antigen retrieval (using a microwave oven at 250 W for 30 min),
immunohistochemistry was performed using an automated NEXES
immunostainer (Ventana Medical Systems, Inc., Tucson, AZ, USA)
according to the manufacturer's instructions. The following primary
antibody was used: anti-FGFR3 [rabbit monoclonal Immunoglobulin G,
clone aa 359–372 (E10234); Spring Bioscience, Fremont, CA, USA;
dilution 1:50]. FGFR3 immunoreactivity was scored as either
negative or positive, irrespective of the staining intensity. Focal
(partly positive stained urothelial tissue on the TMA section) or
weak FGFR3 (positive but with reduced intensity) immunoreactivity
was also considered to be positive.
FGFR3 mutation analysis
FGFR3 mutation analysis was performed using
the SNaPshot method as described previously (12,22), using
the ABI PRISM SNaPshot Multiplex Kit (Applied Biosystems, Foster
City, CA, USA). Three regions of the FGFR3 gene, comprising
all FGFR3 mutations identified in BC (23), were simultaneously amplified in a
multiplex polymerase chain reaction (PCR). Briefly, the multiplex
PCR was performed in a volume of 15 µl, containing 1X PCR buffer,
1.5 mmol/l MgCl2, 0.5 U Taq polymerase (Promega
Corporation, Madison, WI, USA), 0.17 mmol/l deoxynucleotide
triphosphates (Roche Diagnostics, Basel, Switzerland), 10 pmol of
exon 7 and exon 15 primers, 7.5 pmol of exon 10 primers
(Invitrogen, Carlsbad, CA, USA), 5% glycerol (Fluka, Buchs SG,
Switzerland), and 1–250 ng of genomic DNA. Cycling conditions were
as follows: 5 min at 95°C, 35 cycles at 95°C for 45 sec, 60°C for
45 sec, and 72°C for 45 sec, followed by 10 min at 72°C. Following
removal of excess primers and dNTPs, 8 SNaPshot primers for
detection of 9 FGFR3 mutations were annealed to the PCR
products and extended using a labelled dideoxynucleotide. These
extended primers were analysed using an ABI PRISM 3100 Genetic
Analyzer automatic sequencer (Applied Biosystems, Foster City, CA,
USA); the label attached to the incorporated nucleotide indicated
the presence or absence of mutations. All mutations were verified
using a second independent SNaPshot analysis.
Statistical analysis
Statistical analyses were performed using the
survival package in R version 3.0.3 (http://www.r-project.org) and SPSS version 22.0 (IBM
SPSS, Armonk, NY, USA). P<0.05 was considered to indicate a
statistically significant difference. Associations between the
measured parameters were obtained by applying two-sided
χ2 and Fisher's exact tests. Non-parametric Kaplan-Meier
estimators were used to analyse DSS. Point-wise bands at a
confidence level of 0.95 were computed. Differences between
survival estimates were evaluated using the Log-Rank test. Cox
regression analysis was performed for the variables with regard to
DSS. For the analysis of RFS, patients were censored when
cystectomy was performed or at the time of their last tumour-free
clinical follow-up appointment. For DSS analysis, patients were
censored at their final tumour-free clinical follow-up appointment
or at their date of mortality unrelated to the tumour.
Results
Positive FGFR3 immunoreactivity and
FGFR3 mutations are associated with positive histopathological
characteristics
FGFR3 staining of any intensity was classified as
positive, and was observed in 113/207 patients. Positive staining
was mainly present in pTa/pT1 tumours (64%; 89/140). In addition,
activating mutations in the FGFR3 gene were detected in
98/208 (47%) analysable BC tumours, of which 59% (83/140) were pTa
and pT1 tumours.
Table II exhibits the
associations between FGFR3 immunohistochemistry and various
clinicopathological parameters. A positive FGFR3 staining pattern
was largely observed in tumours classified as low-grade and stage
pTa. In the low-grade tumour group, 69% of tumours were FGFR3
positive (Table II) and 74% carried
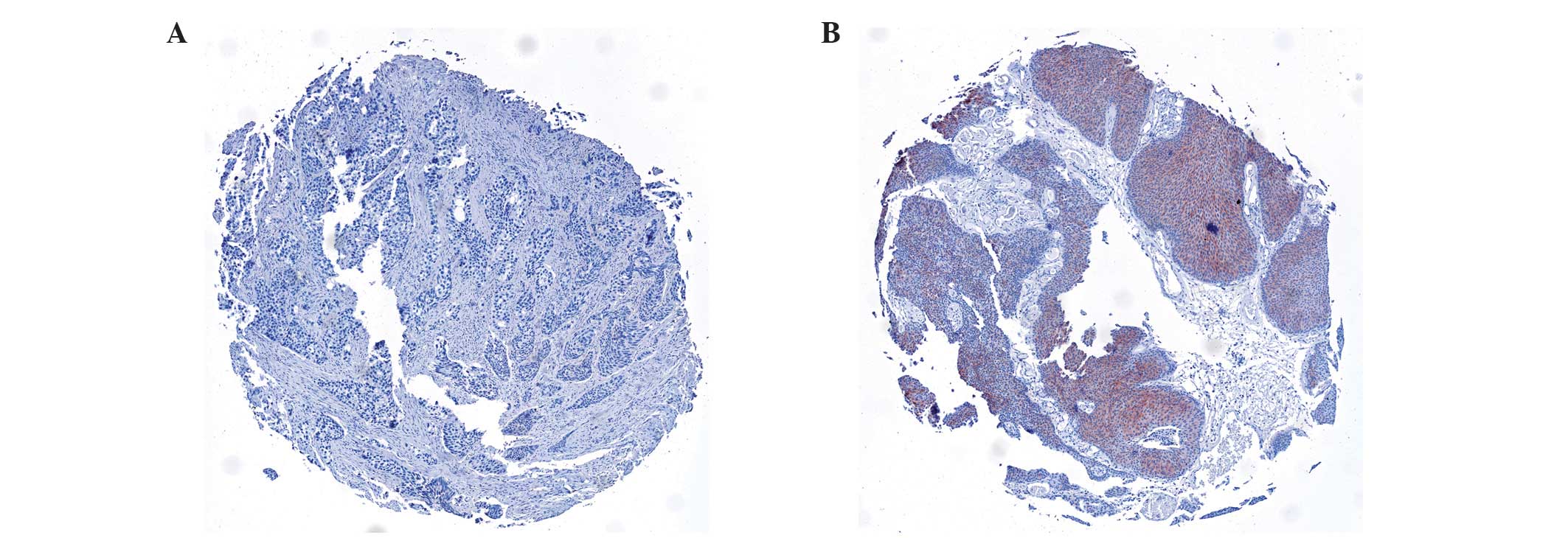
FGFR3 mutations (data not shown). Fig. 1A demonstrates a typical example of an
FGFR3-negative invasive high-grade tumour, while Fig. 1B illustrates an example of an FGFR3
positive non-invasive low-grade tumour. In total, 69% of pTa
lesions were positive for FGFR3, as demonstrated by immunostaining.
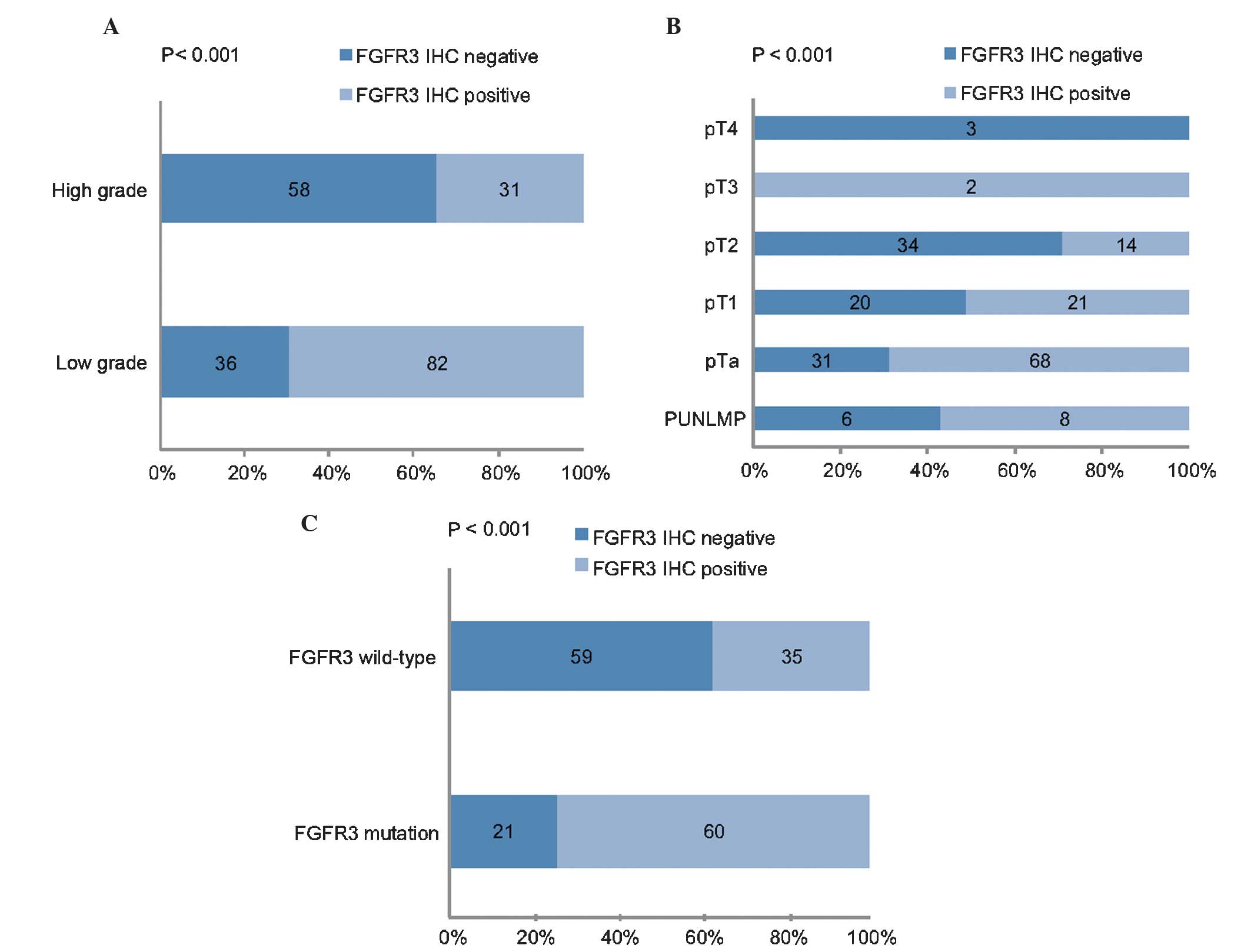
Fig. 2A and B depict the significant
association between tumour stage and grade, and FGFR3
immunoreactivity (both P<0.001). Papillary non-invasive (pTa)
and low-grade tumours were predominantly positive for FGFR3, as
demonstrated by immunohistochemical analysis. There was a
significant association between positive FGFR3 immunoreactivity and
activating FGFR3 mutations (P<0.001; Fig. 2C).
| Table II.Comparison of FGFR3 immunoreactivity
with clinicopathological and IHC parameters (n=207). |
Table II.
Comparison of FGFR3 immunoreactivity
with clinicopathological and IHC parameters (n=207).
|
| FGFR3 IHC staining
pattern |
|
|---|
|
|
|
|
|---|
| Clinicopathological
variable | Negative, n | Positive, n | P-value |
|---|
| Tumour
stagea |
|
|
<0.001c |
|
PUNLMP | 6 | 8 |
|
|
pTa | 31 | 68 |
|
|
pT1 | 20 | 21 |
|
|
pT2 | 34 | 14 |
|
|
pT3 | 0 | 2 |
|
|
pT4 | 3 | 0 |
|
| Histological
gradea |
|
|
<0.001c |
| 1 | 23 | 35 |
|
| 2 | 13 | 47 |
|
| 3 | 58 | 31 |
|
| Histological
gradeb |
|
|
<0.001c |
|
Low | 36 | 82 |
|
|
High | 58 | 31 |
|
| Adjacent carcinoma
in situb |
|
| 0.062 |
| No | 77 | 103 |
|
|
Yes | 17 | 10 |
|
|
Multiplicityb |
|
| 1.000 |
|
Solitary | 20 | 25 |
|
|
Multifocal | 74 | 88 |
|
| Growth
patternb,d |
|
|
<0.001c |
|
Papillary | 63 | 103 |
|
|
Solid | 30 | 10 |
|
Positive FGFR3 immunoreactivity was more frequent in
tumours that did not posses adjacent carcinoma in situ
(P=0.062). Considering only those tumours with solid growth
patterns, which are known to be associated with a worse prognosis
(24), positive FGFR3
immunoreactivity was present in a minority of cases (25%;
P<0.001).
It was concluded that positive FGFR3 staining was
associated with low tumour stage and grade, and with a papillary
pattern of tumour growth (all P<0.001). In a previous study
(12), FGFR3 mutation status was
observed to be associated with identical clinicopathological
parameters such as positive FGFR3 staining in the present
study.
FGFR3 is a prognostic biomarker for
patients with BC
The end-points for the present study were RFS and
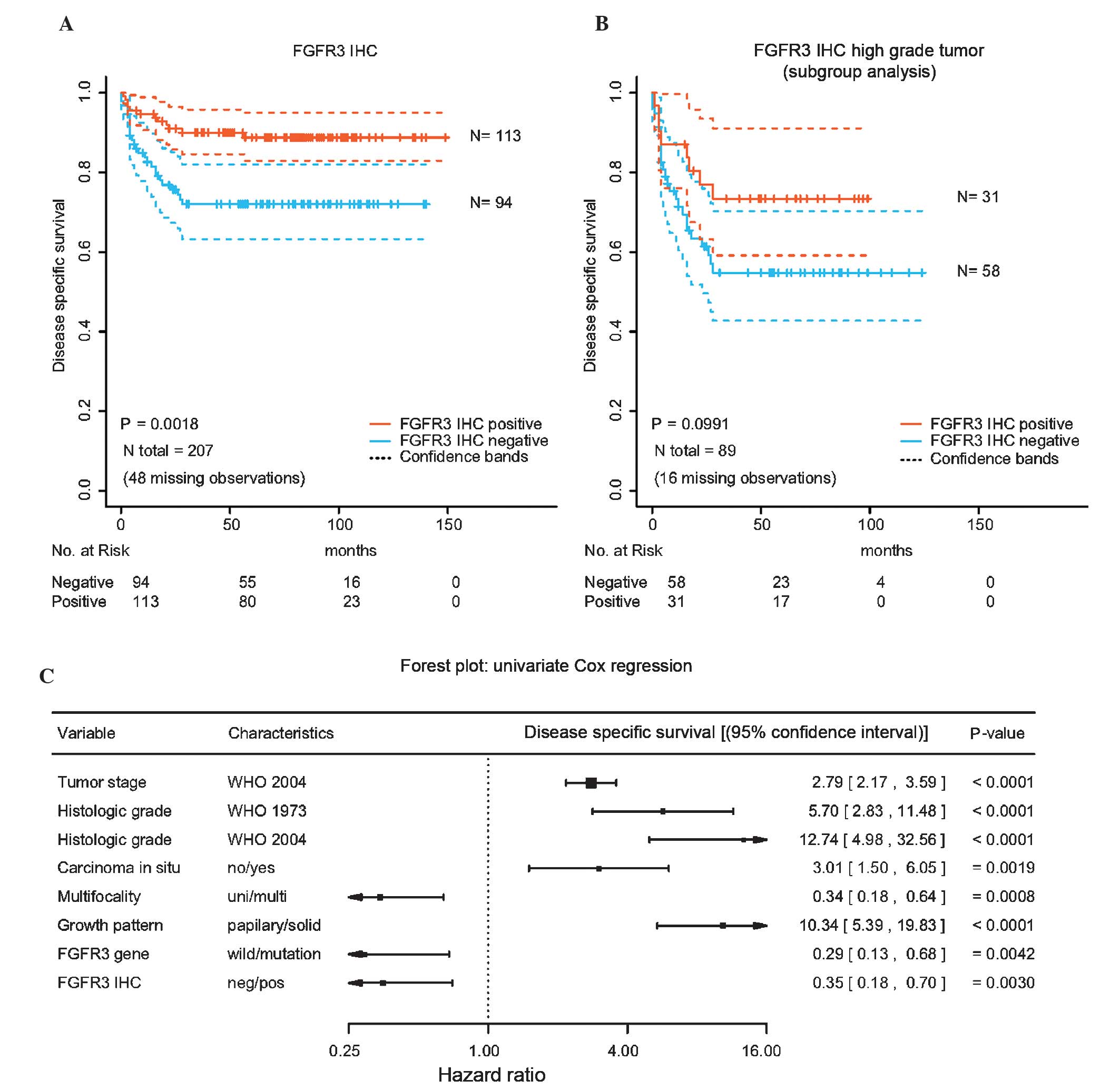
DSS. Kaplan-Meier analyses for DSS are exhibited in Fig. 3A and B, and reveal that BC patients
with positive FGFR3 staining had a significantly increased DSS
compared with that of patients with negative FGFR3 staining
(P=0.0018). In a subgroup analysis for high-grade tumours, positive
FGFR3 staining demonstrated a trend for improved prognosis
(Fig. 3B), however this trend was not
statistically significant (P=0.0991).
Fig. 3C summarises the
results of the univariate survival analysis for DSS and indicates
that positive FGFR3 staining is associated with longer DSS (hazard
ratio, 0.35; 95% confidence interval, 0.18–0.70; P=0.0030).
Multivariate Cox regression analysis revealed that FGFR3
immunoreactivity was not observed to be a significant parameter
associated with DSS (data not shown). None of the investigated
parameters demonstrated a correlation with RFS (data not
shown).
Discussion
The present study aimed to investigate FGFR3
immunoreactivity as a potential prognostic biomarker and diagnostic
tool in surgical pathology, for patients with BC. The results of
the present study revealed that FGFR3 immunoreactivity of any
intensity was markedly associated with a low tumour grade and
stage, and longer DSS.
In the present study, increased protein expression
was identified in 69% of pTa and 51% of pT1 tumours. This finding
corresponds with the results of previous studies, which have
previously investigated FGFR3 protein expression using
immunohistochemistry, which have reported similar percentages of
increased FGFR3 protein expression to those observed in the present
study (18,19,23).
Accordingly, the aforementioned studies identified a significant
association between FGFR3 expression and tumour stage and grade. By
contrast, Matsumoto et al (25) identified no association between FGFR3
expression levels and pathological parameters, including grade and
stage, potentially due to the low number of cases evaluated leading
to a low statistical power (n=126).
Furthermore, the present study demonstrated a
correlation between FGFR3 expression and FGFR3 mutation. In
the present study, 74% of tumours with positive FGFR3 expression
demonstrated an FGFR3 mutation. This association has additionally
been verified using semi-quantitative reverse transcription-PCR,
where FGFR3 messenger RNA expression was clearly associated with
FGFR3 mutation status (26).
Similarly to the results of the present study, Tomlinson et
al (18) demonstrated a
significant association between FGFR3 expression levels and
FGFR3 mutation, as well as tumour grade and stage,
respectively.
Previously, FGFR3 mutation status has been
demonstrated to be a marker for the prognosis of patients with BC
(11,27,28). In
the present study, the correlation between FGFR3 mutations
and tumours of low stage and grade was confirmed (9,11).
Previous studies have investigated the use of FGFR3 expression as a
predictor of prognosis in BC. While a number of authors were able
to demonstrate a shorter RFS associated with FGFR3 expression
(20,29), Gudjonsson et al (21) did not identify any difference in time
to recurrence. In general, the role of molecular markers for
predicting BC recurrence appears to be limited, as reviewed by van
Rhijn (30). Even the FGFR3
mutation, which facilitates selective identification of
non-muscle-invasive BC with good prognosis, did not predict
recurrence in two studies investigating >200 patients, alone or
in combination with other molecular markers (5,11).
Therefore, it was not noteworthy that the present study was unable
to predict recurrence using FGFR3 mutation or
expression.
To best of our knowledge, the present study is the
first report of an association between FGFR3 protein expression and
DSS. The present study demonstrated that in addition to
FGFR3 mutation, FGFR3 protein expression was able to predict
longer DSS in patients with BC. However, FGFR3 protein expression
did not remain an independent predictor of worse DSS following
multivariate analysis.
FGFR3 mutation has been proven to be capable
of predicting prognosis in several previous studies. Tomlinson
et al (18), described the
association between FGFR3 mutation and protein expression
levels, and identified a marked association between FGFR3 protein
expression and tumour grade and stage. However, data on progression
and DSS were not presented. Bodoor et al (31) studied FGFR3 protein expression and
disease course and identified no association between FGFR3
expression and overall survival, although data on DSS was not
available. However, two recent studies reported no association
between FGFR3 protein expression and prognosis. Guancial et
al (32) and Turo et al
(33) investigated FGFR3 protein
expression in muscle-invasive BC and identified no association with
overall survival. Guancial et al (32) investigated FGFR3 protein expression in
231 primary invasive BCs, while Turo et al (33) studied FGFR3 protein expression in 150
invasive BCs. Guancial et al (32) found FGFR3 mutations in just 2%
of all tumours, whereas Turo et al (33) did not investigate FGFR3
mutation status.
In the present study it was revealed that FGFR3
protein expression was increased in tumours of lower stage and
grade. Consequently, FGFR3 protein expression was associated with
improved outcomes, as grading and staging are significant,
well-known pathological predictors for disease progression in
BC.
A significant limitation of the present study was
that a major end-point for BC, PFS, was not able to be assessed in
this cohort. FGFR3 protein expression was not an independent
marker, but was markedly influenced by the pathological parameters,
stage and grade for the prediction of disease course. However,
FGFR3 protein expression has the potential to serve as an
additional molecular marker, alongside tumour grading and staging,
in the prediction of prognosis.
FGFR3 mutation analysis using the SNaPshot
method has not been implemented in routine practice, due to the
high associated costs and complexity. By contrast, FGFR3
immunohistochemistry appears to be more convenient and feasible for
use on a routine basis. Analysis of FGFR3 protein expression may
provide a tool for use in the assessment of the prognosis of
patients exhibiting BC. The present study proposes to use FGFR3
immunoreactivity as an additional diagnostic measure for grading in
difficult cases, to better differentiate between low- and
high-grade urothelial lesions.
The prognosis of non-muscle-invasive BC relies on
clinicopathological variables to predict outcomes. The present
study revealed that the FGFR3 receptor is a significant, but not
independent, marker for DSS of BC patients. The present study
concluded that FGFR3 protein expression and mutant FGFR3 may
provide prognostic information for non-invasive BC, and may aid
pathologists with appropriate grading in difficult cases. In
addition, loss of FGFR3 expression may identify a subgroup of
high-grade tumours with worse prognoses. Further prospective
studies evaluating all end-points are required to confirm these
data.
Acknowledgements
The authors would like to thank Rudolf Jung
(Institute of Pathology, University of Erlangen, Erlangen,
Germany), Martina Storz, Silvia Behnke, Susanne Dettwiler, and
Andre Fitsche (All Institute of Surgical Pathology, University
Hospital Zurich, University of Zurich, Zurich, Switzerland) for
excellent technical assistance and Armin Pauer (Central Tumor
Registry, Regensburg, Germany) for help in obtaining the clinical
data.
Abbreviations:
|
BC
|
bladder cancer
|
|
FGFR
|
fibroblast growth factor receptor
|
|
TMA
|
tissue microarray
|
|
RFS
|
recurrence-free survival
|
|
SDS
|
disease-specific survival
|
References
|
1
|
Heney NM: Natural history of superficial
bladder cancer. Prognostic features and long-term disease course.
Urol Clin North Am. 19:429–433. 1992.PubMed/NCBI
|
|
2
|
Hall MC, Chang SS, Dalbagni G, Pruthi RS,
Seigne JD, Skinner EC, Wolf JS Jr and Schellhammer PF: Guideline
for the management of nonmuscle invasive bladder cancer (stages Ta,
T1, and Tis): 2007 update. J Urol. 178:2314–2330. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Eble J, Sauter G, Epstein JI and
Sesterhenn IA: World Health Organization Classification of Tumours.
Pathology and Genetics of Tumours of the Urinary System and Male
Genital Organs. IARC Press. (Lyon). 2004.
|
|
4
|
Wu XR: Urothelial tumorigenesis: A tale of
divergent pathways. Nat Rev Cancer. 5:713–725. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Burger M, van der Aa MN, van Oers JM,
Brinkmann A, van der Kwast TH, Steyerberg EC, Stoehr R, Kirkels WJ,
Denzinger S, Wild PJ, et al: Prediction of progression of
non-muscle-invasive bladder cancer by WHO 1973 and 2004 grading and
by FGFR3 mutation status: A prospective study. Eur Urol.
54:835–843. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Turner N and Grose R: Fibroblast growth
factor signalling: From development to cancer. Nat Rev Cancer.
10:116–129. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dieci MVI, Arnedos M, Andre F and Soria
JC: Fibroblast growth factor receptor inhibitors as a cancer
treatment: From a biologic rationale to medical perspectives.
Cancer Discov. 3:264–279. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cappellen D, De Oliveira C, Ricol D, de
Medina S, Bourdin J, Sastre-Garau X, Chopin D, Thiery JP and
Radvanyi F: Frequent activating mutations of FGFR3 in human bladder
and cervix carcinomas. Nat Genet. 23:18–20. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Billerey C, Chopin D, Aubriot-Lorton MH,
Ricol D, de Medina S Gil Diez, Van Rhijn B, Bralet MP,
Lefrere-Belda MA, Lahaye JB, Abbou CC, et al: Frequent FGFR3
mutations in papillary non-invasive bladder (pTa) tumors. Am J
Pathol. 158:1955–1959. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van Rhijn BW, Montironi R, Zwarthoff EC,
Jöbsis AC and van der Kwast TH: Frequent FGFR3 mutations in
urothelial papilloma. J Pathol. 198:245–251. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
van Rhijn BW, Vis AN, van der Kwast TH,
Kirkels WJ, Radvanyi F, Ooms EC, Chopin DK, Boevé ER, Jöbsis AC and
Zwarthoff EC: Molecular grading of urothelial cell carcinoma with
fibroblast growth factor receptor 3 and MIB-1 is superior to
pathologic grade for the prediction of clinical outcome. J Clin
Oncol. 21:1912–1921. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
van Oers JM, Wild PJ, Burger M, Denzinger
S, Stoehr R, Rosskopf E, Hofstaedter F, Steyerberg EW,
Klinkhammer-Schalke M, Zwarthoff EC, et al: FGFR3 mutations and a
normal CK20 staining pattern define low-grade noninvasive
urothelial bladder tumours. Eur Urol. 52:760–768. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hernández S, López-Knowles E, Lloreta J,
Kogevinas M, Jaramillo R, Amorós A, Tardón A, García-Closas R,
Serra C, Carrato A, et al: FGFR3 and Tp53 mutations in T1G3
transitional bladder carcinomas: Independent distribution and lack
of association with prognosis. Clin Cancer Res. 11:5444–5450. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zieger K, Dyrskjøt L, Wiuf C, Jensen JL,
Anderson CL, Jensen KM and Ørntoft TF: Role of activating
fibroblast growth factor receptor 3 mutations in the development of
bladder tumors. Clin Cancer Res. 11:7709–7719. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
van Rhijn BW, van der Kwast TH, Liu L,
Fleshner NE, Bostrom PJ, Vis AN, Alkhateeb SS, Bangma CH, Jewett
MA, Zwarthoff EC, et al: The FGFR3 mutation is related to favorable
pT1 bladder cancer. J Urol. 187:310–314. 2012.PubMed/NCBI
|
|
16
|
van Rhijn BW, van der Kwast TH, Vis AN,
Kirkels WJ, Boevé ER, Jöbsis AC and Zwarthoff EC: FGFR3 and P53
characterize alternative genetic pathways in the pathogenesis of
urothelial cell carcinoma. Cancer Res. 64:1911–1914. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bakkar AA, Wallerand H, Radvanyi F, Lahaye
JB, Pissard S, Lecerf L, Kouyoumdjian JC, Abbou CC, Pairon JC,
Jaurand MC, et al: FGFR3 and TP53 gene mutations define two
distinct pathways in urothelial cell carcinoma of the bladder.
Cancer Res. 63:8108–8112. 2003.PubMed/NCBI
|
|
18
|
Tomlinson DC, Baldo O, Harnden P and
Knowles MA: FGFR3 protein expression and its relationship to
mutation status and prognostic variables in bladder cancer. J
Pathol. 213:91–98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mhawech-Fauceglia P, Cheney RT, Fischer G,
Beck A and Herrmann FR: FGFR3 and p53 protein expressions in
patients with pTa and pT1 urothelial bladder cancer. Eur J Surg
Oncol. 32:231–237. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Maeng YH, Eun SY and Huh JS: Expression of
fibroblast growth factor receptor 3 in the recurrence of
non-muscle-invasive urothelial carcinoma of the bladder. Korean J
Urol. 51:94–100. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gudjónsson S, Bendahl PO, Chebil G,
Höglund M, Lindgren D, Lundberg LM, Lövgren K, Fernö M, Månsson W
and Liedberg F: Can tissue microarray-based analysis of protein
expression predict recurrence of stage Ta bladder cancer? Scand J
Urol Nephrol. 45:270–277. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
di Martino E, Tomlinson DC and Knowles MA:
A decade of FGF receptor research in bladder cancer: Past, present,
and future challenges. Adv Urol. 2012:4292132012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gómez-Román JJ, Saenz P, Molina M,
González J Cuevas, Escuredo K, Cruz S Santa, Junquera C, Simón L,
Martínez A, Baños JL Gutiérrez, et al: Fibroblast growth factor
receptor 3 is overexpressed in urinary tract carcinomas and
modulates the neoplastic cell growth. Clin Cancer Res. 11(2 Pt 1):
459–465. 2005.PubMed/NCBI
|
|
24
|
Poyet C, Jentsch B, Hermanns T,
Schweckendiek D, Seifert HH, Schmidtpeter≈ M, Sulser T, Moch H,
Wild PJ and Kristiansen G: Expression of histone deacetylases 1, 2
and 3 in urothelial bladder cancer. BMC Clin Pathol. 14:102014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Matsumoto M, Ohtsuki Y, Ochii K, Seike Y,
Iseda N, Sasaki T, Okada Y, Kurabayashi A and Furihata M:
Fibroblast growth factor receptor 3 protein expression in
urothelial carcinoma of the urinary bladder, exhibiting no
association with low-grade and/or non-invasive lesions. Oncol Rep.
12:967–971. 2004.PubMed/NCBI
|
|
26
|
Bernard-Pierrot I, Brams A, Dunois-Lardé
C, Caillault A, de Medina SG Diez, Cappellen D, Graff G, Thiery JP,
Chopin D, Ricol D and Radranyi F: Oncogenic properties of the
mutated forms of fibroblast growth factor receptor 3b.
Carcinogenesis. 27:740–747. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lopez-Beltran A, Luque RJ,
Alvarez-Kindelan J, Quintero A, Merlo F, Requena MJ and Montironi
R: Prognostic factors in survival of patients with stage Ta and T1
bladder urothelial tumors: The role of G1-S modulators (p53,
p21Waf1, p27Kip1, cyclin D1, and cyclin D3), proliferation index,
and clinicopathologic parameters. Am J Clin Pathol. 122:444–452.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hernández S, López-Knowles E, Lloreta J,
Kogevinas M, Amorós A, Tardón A, Carrato A, Serra C, Malats N and
Real FX: Prospective study of FGFR3 mutations as a prognostic
factor in nonmuscle invasive urothelial bladder carcinomas. J Clin
Oncol. 24:3664–3671. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Barbisan F, Santinelli A, Mazzucchelli R,
Lopez-Beltran A, Cheng L, Scarpelli M, van der Kwast T and
Montironi R: Strong immunohistochemical expression of fibroblast
growth factor receptor 3, superficial staining pattern of
cytokeratin 20, and low proliferative activity define those
papillary urothelial neoplasms of low malignant potential that do
not recur. Cancer. 112:636–644. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
van Rhijn BW: Combining molecular and
pathologic data to prognosticate non-muscle-invasive bladder
cancer. Urol Oncol. 30:518–523. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bodoor K, Ghabkari A, Jaradat Z, Alkhateeb
A, Jaradat S, Al-Ghazo MA, Matalka I, Musleh H and Haddad Y: FGFR3
mutational status and protein expression in patients with bladder
cancer in a Jordanian population. Cancer Epidemiol. 34:724–732.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Guancial EA, Werner L, Bellmunt J, Bamias
A, Choueiri TK, Ross R, Schutz FA, Park RS, O'Brien RJ, Hirsch MS,
et al: FGFR3 expression in primary and metastatic urothelial
carcinoma of the bladder. Cancer Med. 3:835–844. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Turo R, Harnden P, Thygesen H, Fleischmann
A, Thalmann GN, Seiler R, Cross WR and Knowles MA: FGFR3 expression
in primary invasive bladder cancers and matched lymph node
metastases. J Urol. 193:325–330. 2015. View Article : Google Scholar : PubMed/NCBI
|