Introduction
Systemic immunosuppression in cancer patients is
considered to affect the progression of cancer, and therefore the
treatment outcome (1,2). Renal cell carcinoma (RCC) is known to be
resistant to conventional chemotherapeutic agents and is known to
induce an immunosuppressive environment. Although tyrosine kinase
inhibitors (TKIs), including sorafenib and sunitinib, are widely
utilized for the treatment of patients with metastatic RCC and TKIs
are expected to act as adjuvants for immunotherapeutic effects
(3,4),
the anticancer effects of TKIs may be unable to overcome the
immunosuppressive microenvironment of RCC hosts (5).
Previous studies have indicated that myeloid lineage
cells, including tumor-associated macrophages, inflammatory
monocytes and myeloid-derived suppressor cells (MDSCs), have a
significant role in cancer-induced immunosuppression (6,7). MDSCs
were initially described in murine cancer models. However, it
remains to be elucidated which cell populations in humans are
comparable to murine MDSCs (6).
Several studies have revealed that cancer patients exhibit an
increase in the number of cluster of differentiation
(CD)14+ human leukocyte antigen
(HLA)-DRlow/− cells, those with a lower
HLA-DR expression or are negative for HLA-DR, circulating in the
blood (8–10).
CD14+HLA-DRlow/− cells that were
isolated from cancer patients were identified to suppress T-cell
activation in culture, and thus these
CD14+HLA-DRlow/− monocyte
populations were considered to act as MDSCs (6,8–10).
In the present study, in order to investigate the
immunological characteristics of human monocyte populations, HLA-DR
and the gene expression of immune-associated molecules in
circulating CD14+ myeloid cells from RCC patients were
evaluated.
Materials and methods
Blood samples
The protocol of the present study was approved by
the Kumamoto University Review Board (ethical permit no. 509;
Kumamoto University Hospital, Kumamoto, Japan). All healthy donors
and patients reviewed the study objectives and agreed to provide a
blood sample based on consent in accordance with the Declaration of
Helsinki. The clinical data of all patients and healthy donors is
summarized in Table I. Additional
blood samples were collected from 4 of the patients 2–3 months
after surgery. All patients had not received treatment with TKIs or
immunotherapy prior to sample collection. Patients with chronic
renal failure and diabetes mellitus were excluded from the present
study.
 | Table I.Data from healthy donors and renal
cell carcinoma patients. |
Table I.
Data from healthy donors and renal
cell carcinoma patients.
| Patient | Age, years | Gender | Tumor
classification | Surgery | Histology | Size, cm | White blood cells,
cells/µl | Lymphocytes, % | Monocytes, % |
CD14+HLADRlow/−, % |
|---|
| HD1 | 37 | M | – | – | – | – | – | – | – | 14 |
| HD2 | 58 | F | – | – | – | – | – | – | – | 16 |
| HD3 | 49 | F | – | – | – | – | – | – | – | 13 |
| HD4 | 58 | M | – | – | – | – | – | – | – | 10 |
| HD5 | 57 | M | – | – | – | – | – | – | – | 10 |
| P1 | 64 | M | T3a(rt),cT1a(lt) | Yes | Clear cell | 6.5 (rt), 2.5
(lt) | 3700 | 34 | 5.9 | 38 |
| P2 | 62 | F | T1a | Yes | Clear cell |
3.1 | 3200 | 45 |
6.0 | 29 |
| P3 | 61 | M | T2a | Yes | Clear cell |
7.1 | 4600 | 54 |
4.5 | 24 |
| P4 | 64 | F | T1a | Yes | Papillary |
2.5 | 6100 | 53 |
6.3 | 24 |
| P5 | 51 | M | T1a | Yes | Clear cell |
3.0 | 4100 | 70 |
5.4 | 18 |
| P6 | 75 | F | T1b | Yes | Clear cell |
6.5 | 6300 | 68 |
8.6 | 35 |
| P7 | 65 | M | – | Yes | – | – | 7000 | 65 |
5.1 | 31 |
| P8 | 71 | M |
T1a(rt),T1b(lt) | Yes | Papillary | 2.0 (rt), 4.8
(lt) | 6500 | 51 |
4.8 | 12 |
| P9 | 73 | F | T1a | Yes | Clear cell |
4.0 | 6800 | 47 |
3.9 | 34 |
| P10 | 81 | F | T1a | Yes | Clear cell |
3.3 | 2900 | 44 |
5.5 | 10 |
| P11 | 66 | M | T1a | Yes | Papillary |
3.0 | 6600 | 63 |
4.1 | 17 |
| P12 | 47 | M | multiple(NA) | No | Papillary | – | 2500 | 66 |
5.7 | 12 |
| P13 | 42 | M | T1a | Yes | Clear cell |
1.8 | 4000 | 49 |
4.5 | 14 |
| P14 | 82 | F | T1b | Yes | Clear cell |
4.7 | 7400 | 56 |
4.3 | 20 |
| P15 | 77 | F |
T1b(rt),T1a(lt) | Yes | Clear cell | 4.7 (rt), 1.8
(lt) | 3700 | 44 |
7.5 | 28 |
| P16 | 57 | F | T1b | Yes | Clear cell |
5.0 | 4200 | 44 |
5.5 | 31 |
| P17 | 79 | M | T3a | Yes | Clear cell |
7.0 | 5600 | 67 |
6.4 | 8 |
| P18 | 69 | M | T3a | Yes | Clear cell | – | 5900 | 65 |
6.8 | 23 |
| P19 | 51 | M | T1b | Yes | Clear cell |
5.0 | 7100 | 66 |
3.7 | 10 |
| P20 | 66 | F | T3a | Yes | Clear cell |
7.0 | 7200 | 81 |
5.2 | 45 |
| P21 | 75 | M | T4 | No | Clear cell | – | 5100 | 66 |
8.9 | 40 |
| P22 | 37 | M | T4 | Yes | Clear cell | 10.0 | 3900 | 61 | 10.6 | 23 |
Isolation of peripheral blood
mononuclear cells and CD14+ monocytes
Peripheral blood mononuclear cells (PBMCs) were
obtained from 30-ml blood samples using Lymphoprep™ (Axis-Shield
Density Gradient Media; Alere Technologies GmbH, Jena, Germany)
according to the manufacturer's protocols. Half of the PBMCs were
suspended in CELLBANKER® medium (Nippon Zenyaku Kogyo Co., Ltd.,
Fukushima, Japan) and were stored in liquid nitrogen. The remaining
half of the PBMCs were used for isolation of CD14+ monocytes using
CD14 MicroBeads (Miltenyi Biotec, Inc., Auburn, CA, USA) according
to the manufacturer's protocols.
Flow cytometry
PBMCs (5×105/tube) were treated with Fc Receptor
Blocking Solution and subsequently stained with mouse monoclonal
fluorescein isothiocyanate-labeled anti-human CD14 (catalog no.,
325604; clone, HCD14; 1:20) and phycoerythrin-labeled anti-human
HLA-DR (catalog no., 307606; clone, L243; 1:20) antibodies. Fc
receptor Blocking Solution and all antibodies, including mouse
monoclonal isotype-matched control antibodies (clones, MOPC-173 and
MOPC-21; catalog no's., 400212 and 400110, respectively; 1:20),
were obtained from BioLegend, Inc. (San Diego, CA, USA). The
stained cell samples were analyzed using a FACSverse™ and FACSuite
software (BD Biosciences, San Jose, CA, USA).
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA was extracted with RNAiso Plus (catalog
no., 6110A; Takara Bio Inc., Otsu, Japan). RNA was
reverse-transcribed using the PrimeScript RT Reagent kit and DNase
(catalog no., 2270A) from Takara Bio, Inc. The complementary DNA
product (25 µl) was amplified using qPCR at 94°C for 5 min, then 40
cycles of 94°C for 30 sec and 60°C for 30 sec. qPCR was performed
using TaqMan polymerase with SYBR Green fluorescence (Takara
Bio, Inc.) with an ABI PRISM® 7300 Sequence Detection System
(Applied Biosystems; Thermo Fisher Scientific, Waltham, MA, USA).
The relative expression level was determined using the
2−∆∆Cq normalization method (11). The sequences of the primers were
designed using the Primer3 website (version 0.4.0; avaliable from
http://bioinfo.ut.ee/primer3–0.4.0/) and were
synthesised by Hokkaido System Science Co., Ltd. (Tokyo, Japan).
The primer seqeunces are shown in Table
II. The internal control gene used was β-actin, and 3 parallel
wells were set up for each DNA sample (25 µl/well). The data was
representative of ≥2 independent experiments.
| Table II.List of primers used for reverse
transcription-quantitative polymerase chain reaction. |
Table II.
List of primers used for reverse
transcription-quantitative polymerase chain reaction.
| Gene | Primer sequence
(5′-3′) |
|---|
| TGF-β | F:
TTGCTTCAGCTCCACGGAGAA |
|
| R:
ACGTAGTACACGATGGGCAGC |
| CXCL10 | F:
CGCTGTACCTGCATCAGCATTAG |
|
| R:
CTGGATTCAGACATCTCTTCTCACC |
| PTGS2 (COX2) | F:
ACTATGGCTACAAAAGCTGGGAAG |
|
| R:
ATCATCAGGCACAGGAGGAAG |
| VEGFA | F:
CAGGAGTACCCTGATGAGATCG |
|
| R:
TCTGCATGGTGATGTTGGAC |
| IL-6R | F:
CACGACTCTGGAAACTATTCATGC |
|
| R:
AGGACCCCACTCACAAACAAC |
| CCL2 | F:
GTGTCCCAAAGAAGCTGTGATCT |
|
| R:
TGTCCAGGTGGTCCATGGA |
| OSM | F:
GCCCAGGATTTGGAGAGGTCTGG |
|
| R:
GCGATGGTAGCCATGCAGGAACCT |
| β-actin | F:
ATTCCTATGTGGGCGACGAG |
|
| R:
AAGGTGTGGTGCCAGATTTTC |
Statistical analysis
The Mann-Whitney U and Spearman's rank correlation
tests were performed for statistical analysis using StatMate
(GraphPad Software, Inc., La Jolla, CA, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
CD14+HLA-DRlow/− monocyte
percentage is increased in patients with RCC
In total, 22 patients with RCC and 5 age-matched
healthy donors were enrolled in the present study (Table I). The mean percentage of
CD14+HLA-DRlow/- cells in CD14+ monocytes isolated from PBMCs was
23.9% in the RCC patients and 12.6% in the healthy donors. This
difference was statistically significant (P=0.035; Fig. 1A and B). For 4 patients, the
percentage of CD14+HLA-DRlow/- cells was compared pre- and
post-surgery (2–3 months later). A significant reduction in the
percentage of CD14+HLA-DRlow/- cells was observed following
surgical resection in 3 of the 4 patients (Fig. 1C). By contrast, the percentage of
CD14+HLA-DRlow/- monocytes demonstrated no correlation with age,
gender, tumor classification or other laboratory data (Table I).
 | Figure 1.Percentage of
CD14+HLA-DRlow/− monocytes in circulating
blood is increased in patients with RCC. (A) Representative FACS
analysis of CD14+HLA-DRlow/− monocytes in the
peripheral blood mononuclear cells of a healthy control donor and a
patient with RCC. (B) The percentage of
CD14+HLA-DRlow/− monocytes in circulating
CD14+ monocytes of healthy donors and patients was
analyzed. The difference between the groups was statistically
analyzed using the Mann-Whitney U test. (C) The percentage of
CD14+HLA-DRlow/− monocytes in blood samples
of 4 RCC patients pre-surgery and post-surgery. Left panel:
Representative FACS analysis of pt.4. Right panel: Quantification
of all patients. CD, cluster of differentiation; HLA, human
leukocyte antigen; RCC, renal cell carcinoma;
HLA-DRlow/−, cells with a lower HLA-DR expression or are
negative for HLA-DR; FSC, forward scatter; SSC, side scatter; PE,
phycoerythrin; FITC, fluorescein isothiocyanate; Pt, patient; FACS,
fluorescence-activated cell sorting. |
mRNA expression of chemokine (C-C
motif) ligand 2 (CCL2) and chemokine (C-X-C motif) ligand 10
(CXCL10) is negatively associated with the percentage of
CD14+HLA-DRlow/− monocytes
The present study analyzed the mRNA expression of
immune-associated molecules in CD14+ monocytes, and subsequently
evaluated the association between mRNA expression levels and
frequency of CD14+HLA-DRlow/- monocytes. This method of analysis
was used due to the fact that the mRNA expression of
CD14+HLA-DRlow/- monocytes could not be directly measured, as the
total number of CD14+HLA-DRlow/- monocytes was too low to undergo
mRNA extraction. mRNA was extracted from 16 patient and 4 healthy
donor samples. A total of 6 patient samples and 1 healthy donor
sample were excluded due to the low quality of the mRNA. Extremely
low levels of gene expression of interleukin (IL)-6, IL-10,
programmed death-1 (PD-1), PD-1 ligand (PD-L1), PD-L2, nitric oxide
synthase 2, indoleamine 2,3-dioxygenase 1 and arginase 1 were
observed in the preliminary analysis of microarray data (data not
shown). The gene expression levels of cyclooxygenase 2 (COX2),
transforming growth factor β (TGF-β), IL-6R, CCL2, CXCL10,
oncostatin M (OSM) and vascular endothelial growth factor A
(VEGF-A) were quantified using RT-qPCR (Fig. 2). Increased expression levels of CCL2
and CXCL10 were significantly correlated with a reduced percentage
of CD14+HLA-DRlow/- monocytes (P<0.010; R=−0.58; and P=0.013;
R=−0.55; respectively).
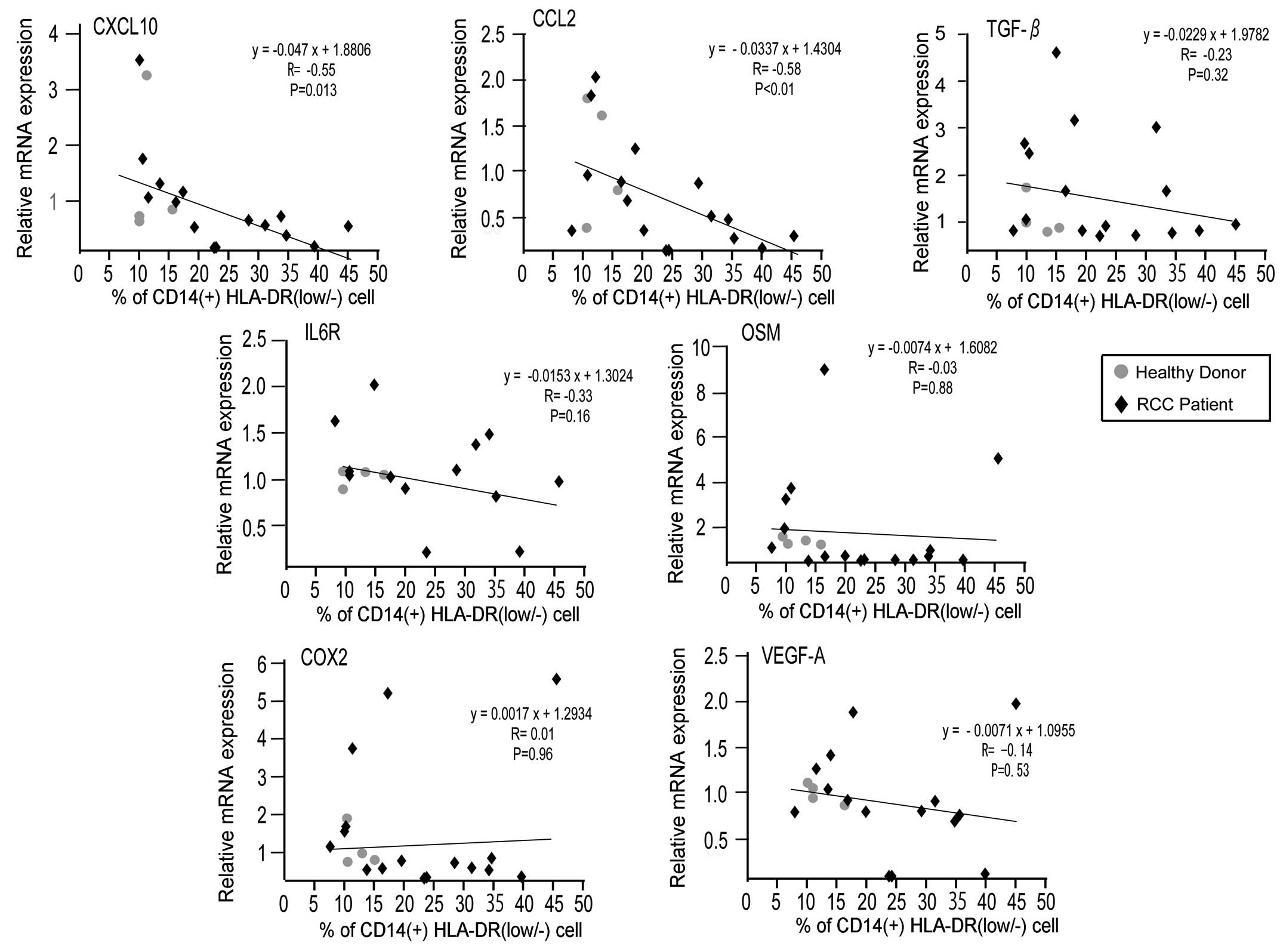 | Figure 2.mRNA expression of immune-associated
genes is negatively associated with a low percentage of
CD14+HLA-DRlow/− monocytes. The mRNA
expression of COX2, TGF-β, IL-6R, CCL2, CXCL10, OSM and VEGF-A in
CD14+ monocytes of healthy donors and RCC patients was
examined by reverse transcription-quantitative polymerase chain
reaction. The correlation between indicated gene expression and the
percentage of CD14+HLA-DRlow/− monocytes in
CD14+ monocytes was evaluated using Spearman's rank
correlation test. CD, cluster of differentiation; HLA, human
leukocyte antigen; HLA-DRlow/−, cells with a lower
HLA-DR expression or are negative for HLA-DR; COX2, cyclooxygenase
2; TGF-β, transforming growth factor β; IL, interleukin; CCL2,
chemokine (C-C motif) ligand 2; CXCL10, chemokine (C-X-C motif)
ligand 10; OSM, oncostatin M; VEGF, vascular endothelial growth
factor; RCC, renal cell carcinoma. |
Discussion
The present study evaluated the mRNA expression of
immune-associated molecules in circulating CD14+
monocytes. The number of
CD14+HLA-DRlow/− monocytes is
considered to be a prognostic factor; however, an evaluation of the
association with the clinical prognosis of patients was not
performed by the present study. A high number (>40%) of
CD14+HLA-DRlow/− monocytes was
significantly associated with a poorer clinical prognosis in
patients with chronic lymphocytic leukemia (12). In addition, an increased number of
CD14+HLA-DRlow/− monocytes was
demonstrated to be an independent prognostic factor in patients
with non-small lung cancer (13). The
present study revealed that the number of
CD14+HLA-DRlow/− monocytes was
associated with CXCL10 and CCL2 expression, and in a previous study
a high CXCL10 expression in cancer tissues was demonstrated to be
associated with a favorable survival rate in patients with
esophageal cancer (14). Therefore,
it may be of interest to investigate whether the serum
concentration of CXCL10 or CCL2 is a useful prognostic marker for
patients with cancer. A higher frequency of
CD14+HLA-DRlow/− monocytes in RCC
patients was observed compared with healthy donors, confirming
observations made in previous studies (8–10).
Notably, he present study showed that the frequency of
CD14+HLA-DRlow/− monocytes
reverted to normal following surgical resection of the primary
tumor. This observation indicated that unknown molecules derived
from RCC tissues may affect the frequency of
CD14+HLA-DRlow/− monocytes. The
combined observations of the present study suggested that
modification of circulating monocytes by cancer-derived factors may
be involved in immunosuppression in patients with RCC. However, to
the best of our knowledge, there has been no evidence (such as mRNA
expression levels of immune-associated molecules) that has been
able to directly support the possibility that immunosuppressive
molecules are expressed by
CD14+HLA-DRlow/− monocytes. The
present study speculated that increased expression levels of
immunosuppressive molecules would be observed in circulating
monocytes along with the high percentage of
CD14+HLA-DRlow/− monocytes.
However, the results of the present study revealed that the
expression of major immunosuppressive molecules, including COX2,
OSM, TGF-β and VEGF-A, was not correlated with the frequency of
CD14+HLA-DRlow/− monocytes. By
contrast, increased expression levels of CXCL10, which is
associated with immune activation, and CCL2, which is known to be
secreted from activated monocytes and macrophages, were
significantly associated with a reduced percentage of
CD14+HLA-DRlow/− monocytes
(15). The results of the present
study suggested that the expression of inflammatory cytokines is
typically decreased in
CD14+HLA-DRlow/− monocytes.
In conclusion, the present study did not observe an
increase in the expression of any immune-associated molecules
investigated in CD14+ monocytes isolated from patients
with RCC. However, increased mRNA expression of CCL2 and CXCL10 was
inversely correlated with the frequency of
CD14+HLA-DRlow/− monocytes,
suggesting that cytokine expression may be suppressed in these
cells. As the dysfunction of monocytes appears to be attributable
to immunosuppression in RCC patients, we are currently in the
process of identifying the molecules that are derived from cancer
tissue and are able to suppress monocytes. Additional investigation
regarding the strategy required to overcome the dysfunction of
CD14+HLA-DRlow/− monocytes and to
generate immune stimulatory myeloid lineages is required in order
to achieve an improved outcome for cancer patients.
Acknowledgements
The authors would like to thank Mr. Takenobu
Nakagawa, Mr. Osamu Nakamura, Ms. Emi Kiyota and Ms. Yui Hayashida
(Department of Cell Pathology, Graduate School of Medical Sciences,
Kumamoto University, Kumamoto, Japan) for providing technical
assistance. The present study was supported by a research grant
from Ono Pharmaceutical Corporation (Osaka, Japan; grant no.
#ONO-2013-Kumamoto1).
References
|
1
|
Vieweg J, Su Z, Dahm P and Kusmartsev S:
Reversal of tumor-mediated immunosuppression. Clin Cancer Res.
13(Suppl): S727–S732. 2007. View Article : Google Scholar
|
|
2
|
Dunn GP, Koebel CM and Schreiber RD:
Interferons, immunity and cancer immunoediting. Nat Rev Immunol.
6:836–848. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Motzer RJ and Bukowski RM: Targeted
therapy for metastatic renal cell carcinoma. J Clin Oncol.
24:5601–5608. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tanigawa G, Kawashima A, Yamaguchi S,
Nishimura K, Miyoshi S, Kajikawa J, Meguro N, Yosioka T, Oka T,
Hara T, et al: Clinical outcome and prognostic factors of sorafenib
in Japanese patients with advanced renal cell carcinoma in general
clinical practice. Jap J Clin Oncol. 41:1265–1270. 2011. View Article : Google Scholar
|
|
5
|
Finke JH, Rayman PA, Ko JS, Bradley JM,
Gendler SJ and Cohen PA: Modification of the tumor microenvironment
as a novel target of renal cell carcinoma therapeutics. Cancer J.
19:353–364. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Greten TF, Manns MP and Korangy F: Myeloid
derived suppressor cells in human diseases. Int Immunopharmacol.
11:802–807. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ochoa AC, Zea AH, Hernandez C and
Rodriguez PC: Arginase, prostaglandins, and myeloid-derived
suppressor cells in renal cell carcinoma. Clin Cancer Res.
13(Suppl): S721–S726. 2007. View Article : Google Scholar
|
|
8
|
Lin Y, Gustafson MP, Bulur PA, Gastineau
DA, Witzig TE and Dietz AB: Immunosuppressive CD14+HLA-DR(low)/-
monocytes in B-cell non-Hodgkin lymphoma. Blood. 117:872–881. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chikamatsu K, Sakakura K, Toyoda M,
Takahashi K, Yamamoto T and Masuyama K: Immunosuppressive activity
of CD14+ HLA-DR- cells in squamous cell carcinoma of the head and
neck. Cancer Sci. 103:976–983. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hoechst B, Ormandy LA, Ballmaier M, Lehner
F, Krüger C, Manns MP, Greten TF and Korangy F: A new population of
myeloid-derived suppressor cells in hepatocellular carcinoma
patients induces CD4(+)CD25(+)Foxp3(+) T cells. Gastroenterology.
135:234–243. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu J, Zhou Y, Huang Q and Qiu L:
CD14+HLA-DRlow/− expression: A novel
prognostic factor in chronic lymphocytic leukemia. Oncol Lett.
9:1167–1172. 2015.PubMed/NCBI
|
|
13
|
Vetsika EK, Koinis F, Gioulbasani M,
Aggouraki D, Koutoulaki A, Skalidaki E, Mavroudis D, Georgoulias V
and Kotsakis A: A circulating subpopulation of monocytic
myeloid-derived suppressor cells as an independent
prognostic/predictive factor in untreated non-small lung cancer
patients. J Immunol Res. 2014:6592942014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sato Y, Motoyama S, Nanjo H, Wakita A,
Yoshino K, Sasaki T, Nagaki Y, Liu J, Imai K, Saito H and Minamiya
Y: CXCL10 expression status is prognostic in patients with advanced
thoracic esophageal squamous cell carcinoma. Ann Surg Oncol: Oct.
13:2015.(Epub ahead of print).
|
|
15
|
Fujita M, Kohanbash G, Fellows-Mayle W,
Hamilton RL, Komohara Y, Decker SA, Ohlfest JR and Okada H: COX-2
blockade suppresses gliomagenesis by inhibiting myeloid-derived
suppressor cells. Cancer Res. 71:2664–2674. 2011. View Article : Google Scholar : PubMed/NCBI
|














