Introduction
Endometrial cancer is one of the most prevalent
malignant tumors of the female genital tract, accounting for 6% of
all cases of cancer in women (1).
According to the American Cancer Society, the annual incidence of
endometrial cancer is increasing, with ~40,880 new cases diagnosed
in the USA in 2005 (2) and ~49,560
new cases in 2013 (3). The median age
of patients with endometrial cancer is 58 years, and the 5-year
overall survival (OS) rate of those in the early stages of the
disease is 80–85% (4). The high
incidence and mortality rate highlight the necessity for optimized
therapy for patients with endometrial cancer.
The guidelines of the International Federation of
Gynecology and Obstetrics (FIGO), which were updated in 2009 to
include a revised pathology surgical staging system (5), recommend surgical therapy involving
total hysterectomy and bilateral salpingo-oophorectomy, peritoneal
washing and pelvic and/or para-aortic lymphadenectomy. The
guidelines of the National Comprehensive Cancer Network (NCCN) also
recommend that surgical staging include pelvic and para-aortic
lymphadenectomies for women with endometrial cancer (6). According to guidelines (5,6), a
lymphadenectomy should be performed when myometrial invasion is
>50%, or in tumors of grade 3 or a special pathological type.
Despite the FIGO and NCCN recommendations, the survival benefit of
lymphadenectomy in early-stage endometrial cancer has not been
clearly defined, and the extent and performance of lymphadenectomy
varies from surgeon to surgeon. Several retrospective studies have
suggested that a therapeutic benefit is associated with
lymphadenectomy in early-stage endometrial cancer (7,8); however,
two large randomized control studies have failed to demonstrate a
survival advantage (9,10).
Similarly, the guidelines are lacking on how to
treat pelvic and para-aortic lymph node metastases. Pelvic
metastases may occur in up to 10% of patients with early-stage
endometrial cancer, and para-aortic metastases may occur in as many
as 6% (11). Although clinicians
generally agree that surgery is the best curative treatment option,
they may disagree regarding the optimal procedure to use.
Lymphadenectomy is widely used to assess whether
endometrial cancer has metastasized and reduces the risk of
lymphatic metastasis (8).
Non-systematic lymphadenectomy usually involves removing <11
lymph nodes (7). However, to try to
treat and prevent metastases, physicians often perform systematic
lymphadenectomy, which involves removing ≥11 lymph nodes in the
same area covered by non-systematic lymphadenectomy (9,10).
Systematic lymphadenectomy is significantly more invasive than the
non-systematic procedure, and leaves patients with markedly lower
postoperative lymph function, increasing the risk of various
complications (12). Given the
controversy regarding whether systematic lymphadenectomy is
justified for patients with early-stage endometrial cancer, the
present study aimed to examine its safety and efficacy by
systematically reviewing the literature.
Materials and methods
Search strategy
The current systematic review was conducted in
accordance with the recommendations of the PRISMA statement
(13). PubMed (www.ncbi.nlm.nih.gov/pubmed), Embase (www.embase.com), the Cochrane Library (www.cochranelibrary.com), and the China National
Knowledge Infrastructure (www.cnki.net)
databases (accessed April 2014) were searched during April 2014,
without language restrictions and using the following search terms:
‘Lymphadenectomy’, ‘lymph nodes dissection’, ‘endometrial cancer’,
‘endometrial carcinoma’, ‘early stage’ and ‘low risk’.
Study selection and quality
assessment
Randomized control trials (RCTs) and prospective or
retrospective studies (non-RCTs) directly comparing systematic
lymphadenectomy and no systematic lymphadenectomy in patients with
clinically localized endometrial cancer were eligible for
inclusion. Studies were included if they met the following
criteria: i) They involved patients with pathologically proven
early-stage endometrial cancer determined to be preoperative FIGO
stage I or occult stage II disease; and ii) they provided data on
Kaplan-Meier analysis of OS for patients who underwent surgical
resection. Studies involving patients who were diagnosed with other
malignant neoplasms were excluded.
The methodological quality of included RCTs was
assessed according to the guidelines in the 2008 version of the
Cochrane Handbook for Systematic Reviews of Interventions (14). RCTs were considered to be high-quality
if they reported on three or four of the items, which included
random allocation, concealment of random allocation, blinding of
persons who assess treatment effects and intention-to-treat
analysis. The methodological quality of the included non-RCTs was
assessed using the star scoring system based on the
Newcastle-Ottawa Scale (15), which
examines the method used to select patients, the comparability of
the study groups, and the number of outcomes reported. Non-RCTs
were considered high-quality if they received >7 out of 10
possible stars.
Outcomes
The primary outcome of the current systematic review
was OS. Data on recurrence-free survival (RFS), disease-free
survival (DFS) and operative mortality and morbidity were captured
as a secondary outcome where available. In addition, patients were
classified into risk subgroups based on criteria from the
Gynecologic Oncology Group and FIGO (5).
Data extraction
Data were extracted independently by two authors.
Data included author details, publication year, preoperative
staging, the number of patients, patient characteristics,
interventions used and conclusions, using a data extraction form.
Any discrepancies in data extraction were resolved by
consensus.
Data synthesis
Owing to the clinical heterogeneity among studies,
meta-analysis was not performed. Instead findings from each study
were synthesized and evaluated qualitatively.
Results
Description of studies
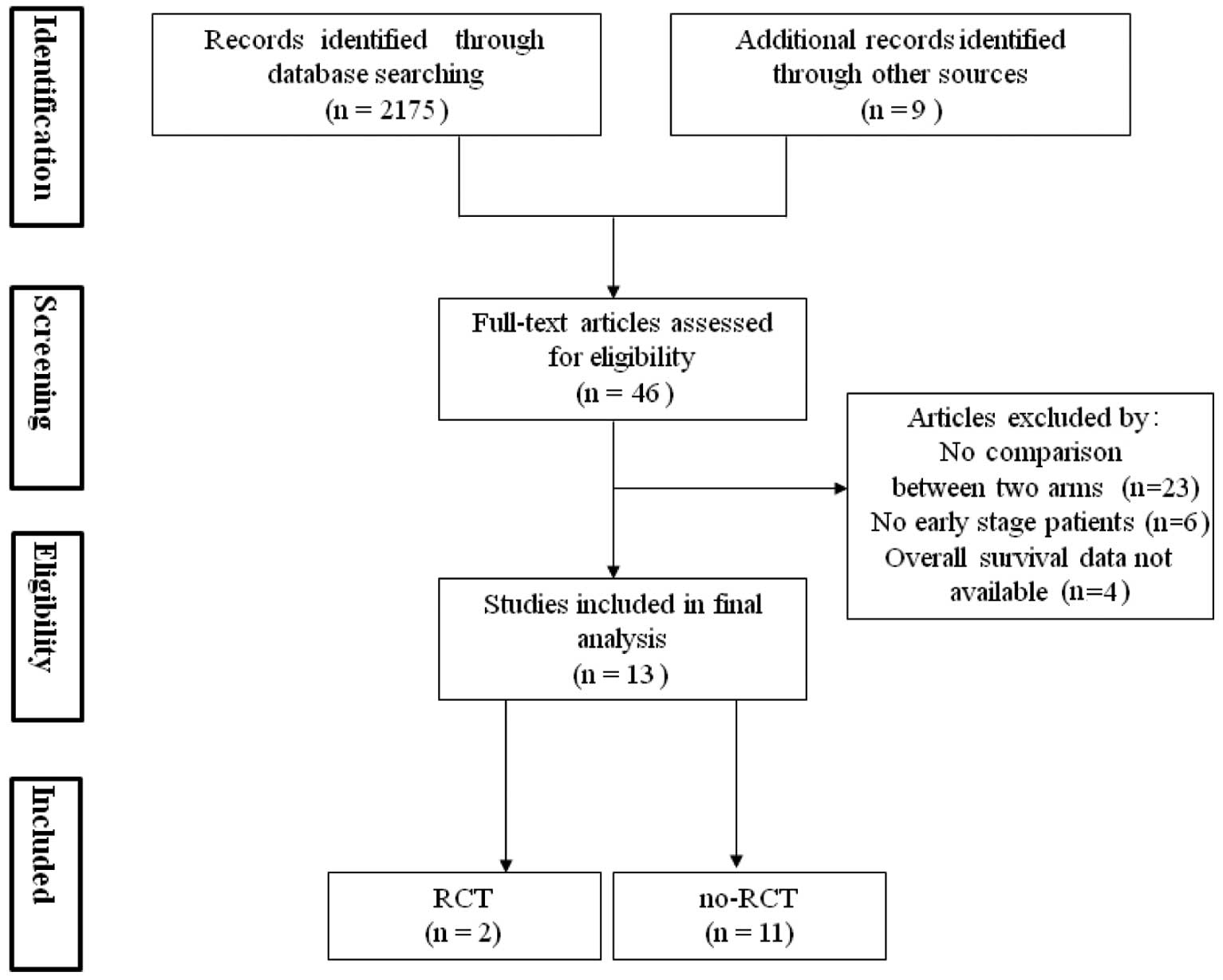
A total of 2,184 potentially eligible studies were
identified and, ultimately, 13 studies involving 51,155 patients
were included in the review (Fig. 1).
The total population included 20,676 patients in the systematic
lymphadenectomy group and 30,479 patients in the no systematic
lymphadenectomy group. Two of the 13 studies were RCTs (9,10) while
the remaining 11 were retrospective non-RCTs (7,8,16–24). Study
recruitment periods extended from 1969 to 2008, and the studies
involved centers from Italy, the USA, Germany, South Korea, Canada
and China. Two studies (20,24), involving a total of 253 patients, did
not report the numbers of lymph nodes dissected in the systematic
lymphadenectomy and no systematic lymphadenectomy groups. All
studies were in English, except for two that were in Chinese
(20,24). Two studies involved only the
adenocarcinoma type of endometrial cancer (22,23),
whereas the other studies involved endometrial cancer of various
pathological types.
A total of 1,487 patients from four studies
(10,17,22,24)
underwent only pelvic lymph node dissection. As expected, the
recurrence rate was higher in patients exhibiting greater numbers
of cancer-positive lymph nodes or a greater extent of lymph node
metastasis (7–10,17,19,22,23).
The median number of lymph nodes removed during systematic
lymphadenectomy ranged from 11 to 30. The key characteristics of
the studies are presented in Table
I.
 | Table I.Characteristics of included studies
comparing systematic and no systematic lymphadenectomy in patients
with early-stage endometrial cancer. |
Table I.
Characteristics of included studies
comparing systematic and no systematic lymphadenectomy in patients
with early-stage endometrial cancer.
| Study | Year | Follow-up,
months | Preoperative
stagea | Number of cases,
SLA / no SLA |
Interventionsb | Refs. |
|---|
|
|
| Kilgore et
al | 1995 | 36 (mean) | Stage I or occult
Stage II | 204 / 192 | 1. Based on pelvic
or minus pelvic and para-aortic lymphadenectomy | (23) |
|
|
|
| Low risk | 137 / 135 | with
peritoneal washing |
|
|
|
|
| High risk | 67 / 57 | 2. Standard surgery
group |
|
| Gao et
al | 2000 | 60 | Stage I–II | 67 / 70 | 1. Based on
lymphadenectomy | (20) |
|
|
|
| Low risk | 17 / 28 | 2. Standard surgery
group |
|
|
|
|
| High risk | 23 / 31 |
|
|
| Ceccaroni et
al | 2004 | 60 | Stage I and grades
1–3 | 55 / 75 | 1. Based on pelvic
lymphadenectomy | (17) |
|
|
|
|
|
| 2. Standard surgery
group Peritoneal cytology (washing) in all series |
|
| Cragun et
al | 2005 | 60 | Stage I or occult
Stage II | 246 / 263 | 1. Based on pelvic
or pelvic and aortic lymphadenectomy | (7) |
|
|
|
| Low risk | 123 / 152 | 2.
Hysterectomy |
|
|
|
|
| High risk | 123 / 111 |
|
|
| Benedetti et
al | 2008 | 60 | Stage I | 264 / 250 | 1. Based on pelvic
or pelvic and aortic lymphadenectomy | (9) |
|
|
|
|
|
| 2. Standard surgery
group other than bulky lymph node |
|
| Kang et
al | 2009 | 60 | Stage I and grade 1
or 2 | 64 / 58 | 1. Based on pelvic
lymphadenectomy | (22) |
|
|
|
|
|
| 2. Hysterectomy
and/or bilateral salpingo-oophorectomy |
| Kitchener et
al | 2009 | 37 (median) | Stage I | 546 / 573 | 1. Based on pelvic
lymphadenectomy and sampling of para-aortic LNs | (10) |
|
|
|
| Low risk | 282 / 330 | 2. Standard surgery
group other than suspicious LNs |
|
|
|
|
| High risk | 264 / 243 |
|
|
| Ji et
al | 2009 | 60 | Stage I | 40 / 76 | 1. Based on pelvic
lymphadenectomy | (24) |
|
|
|
|
|
| 2. Standard surgery
group |
|
| Bassarak et
al | 2010 | 86 (median) | Stage I | 120 / 51 | 1. Based on pelvic
and/or para-aortic LNs | (16) |
|
|
|
| Low risk | 121 (total) | 2. The standard
surgery group |
|
| Jeong et
al | 2010 | 35 (median) | Stage I | 547 / 211 | 1. Based on pelvic
and/or para-aortic lymphadenectomy | (21) |
|
|
|
| Low risk | 566 (total) | 2. Standard surgery
group other than suspicious LNs |
|
|
|
|
| High risk | 162 / 30 |
|
|
|
| Chino et
al | 2011 | 60 (median) | Stage I | 18197 / 28252 | 1. Based on
lymphadenectomy | (18) |
|
|
|
| Low risk | 12637 / 23364 |
|
|
|
|
|
| Intermediate
risk | 5097 / 4628 | 2. Standard surgery
group |
|
|
|
|
| High risk | 463 / 260 |
|
|
| Zhang et
al | 2012 | 42.5 (median) | Stage I | 246 / 103 | 1. Based on
optional systematic pelvic and/or para-aortic lymphadenectomy | (8) |
|
|
|
| Low risk | 212 (total) | 2. Standard surgery
group and peritoneal washing cytology |
|
|
|
|
| Intermediate
risk | 137 (total) |
|
|
| Dowdy et
al | 2012 | 64 (median) | Stage I | 80 / 305 | 1. Based on
optional systematic pelvic and/or para-aortic lymphadenectomy | (19) |
|
|
|
| Low risk | 80 / 305 | 2. Standard surgery
group and peritoneal washing cytology |
|
Methodological quality
Quality assessment scores of the included studies
are summarized in Tables II and
III. The RCTs were considered to be
high quality as they reported at least three items. Similarly, the
non-RCTs were judged to be of moderate to high quality, scoring 7–9
stars.
| Table II.Assessment of methodological quality
of randomized controlled trials included in the current review. |
Table II.
Assessment of methodological quality
of randomized controlled trials included in the current review.
| Study | Random allocation
(description of procedure) | Concealment of
random allocation | Blinding of persons
who assess treatment effects | Intention-to-treat
analysis |
|---|
| Benedetti et
al (9) | + | + | + | + |
| Kitchener et
al (10) | + | + | + | − |
| Table III.Assessment of methodological quality
of non-randomized trials included in the current
review.a |
Table III.
Assessment of methodological quality
of non-randomized trials included in the current
review.a
|
| Patient
selectiona | Group
comparabilityb | Outcome
reportingc |
|
|---|
|
|
|
|
|
|
|---|
| Study | S1 | S2 | S3 | C1 | C2 | O1 | O2 | Starsd |
|---|
| Kilgore et
al (23) | * | * | * | * | * | * | * | 7 |
| Gao et al
(20) | * | * | * | * | * | * | * | 7 |
| Ceccaroni et
al (17) | * | * | * | * | ** | * | ** | 9 |
| Cragun et al
(7) | * | * | * | ** | * | * | ** | 9 |
| Kang et al
(22) | * | * | * | * | ** | * | * | 8 |
| Ji et al
(24) | * | * | * | * | * | * | * | 7 |
| Bassarak et
al (16) | * | * | * | * | * | * | * | 7 |
| Jeong et al
(21) | * | * | * | * | ** | * | ** | 9 |
| Chino et al
(18) | * | * | * | * | ** | * | * | 8 |
| Zhang et al
(8) | * | * | * | * | ** | * | * | 7 |
| Dowdy et al
(19) | * | * | * | * | ** | * | ** | 9 |
Clinical characteristics
The clinical characteristics of the 13 studies
comprising 51,155 patients are listed in Tables I and IV. In the absence of international
standards regarding the difference between the two types of
lymphadenectomy, systematic dissection was considered to involve
the removal of ≥11 lymph nodes (7–10,16–19,21–23),
including the dissection of iliac, obturator (17,18,20,22,24)
and selective para-aortic lymph nodes (7–10,16,19,21,23).
The cases that were classed as not systematic lymphadenectomy
consisted of 9 cases that did not undergo lymphadenectomy (8,16–20,22–24), 3
cases that involved the removal of suspicious lymph nodes (9,10,21) and 1 case that involved the removal of
<11 nodes (7). As the definitions
of systematic and no systematic lymphadenectomy were different
among all 13 studies, systematic vs. no systematic lymphadenectomy
were defined using two criteria: Systematic dissection of lymphatic
tissues vs. no lymphadenectomy other than suspicious lymph nodes or
not performed; and removal of <11 vs. ≥11 lymph nodes.
| Table IV.Summary of results comparing survival
outcomes for systematic lymphadenectomy vs. no systematic
lymphadenectomy. |
Table IV.
Summary of results comparing survival
outcomes for systematic lymphadenectomy vs. no systematic
lymphadenectomy.
| Study | Survival no.
(%) | No. of lymph nodes
removed | Outcomes of
systematic lymphadenectomy relative to no systematic
lymphadenectomy | Refs. |
|---|
| Kilgore et
al | >11 LNs, 204
(52%); 0 LNs, 192 (48%) | 11 (mean) | Significantly
improved OS | (23) |
| Gao et
al | NR | NR | Did not
significantly improve OS | (20) |
| Ceccaroni et
al | >11 LNs, 55
(42%); 0 LNs, 75 (58%) | 29 (median) | Did not
significantly improve OS | (17) |
| Cragun et
al | >11 LNs, 246
(48%); <11 LNs, 263 (52%) | 15 (median) | Significantly
improved OS (but not in low risk group) and PFS | (7) |
| Benedetti et
al | >11 LNs, 264
(51%); 0 LNs, 250 (49%) | 30 (median) | Did not
significantly improve OS and DFS | (9) |
| Kitchener et
al | >12 LNs, 546
(49%); <2 LNs, 573 (51%) | 12 (median) | Did not
significantly improve OS and RFS | (10) |
| Kang et
al | >17.5 LNs, 64
(52%); 0 LNs, 58 (48%) | 18 (mean) | Did not
significantly improve OS and PFS | (22) |
| Ji et
al | NR | NR | Did not
significantly improve OS | (24) |
| Bassarak et
al | >11 LNs, 120
(71%); 0 LNs, 51 (29%) | NR | Significantly
improved OS and CSS, but not PFS | (16) |
| Jeong et
al | >11 LNs, 547
(72.1%); 0 LNs, 211 (27.9%) | 25 (median) | Significantly
improved OS only in high risk group | (21) |
| Chino et
al | >11 LNs, 18,197
(32%); 0 LNs, 28,252 (68%) | 11 (median) | Significantly
improved OS for intermediate and high risk groups | (18) |
| Zhang et
al | >18 LNs, 246
(70%); 0 LNs, 103 (30%) | 22 (mean) | Significantly
improved OS and DFS | (8) |
| Dowdy et
al | >11 LNs, 80
(21%); 0 LNs, 305 (79%) | 30 (mean) | Did not
significantly improve OS, RFS or CSS | (19) |
Association of disease-related
survival associated with lymphadenectomy
Three studies (7,16,22) reported data on progression-free
survival (PFS), which was significantly higher for patients who
underwent systematic lymphadenectomy of ≥11 lymph nodes (86%)
compared with those who underwent no systematic lymphadenectomy
(75%; P<0.001) (7). This
difference in PFS was particularly notable among patients with
intermediate- and high-risk disease. The other two retrospective
studies reported similar PFS for the systematic lymphadenectomy and
no systematic lymphadenectomy groups (16,22).
One study reported that DFS was significantly higher
for the group who underwent the systematic procedure involving ≥11
lymph nodes (88.1%) than for the no systematic procedure (76.3%;
P<0.05) patients with intermediate- and high-risk disease
(8). The same study also found DFS to
be similar for the systematic and no systematic procedures among
patients with low-risk disease (91.2% vs. 83.7%; P>0.05).
Another study identified DFS to be marginally higher following the
systematic procedure for patients of mixed risk types, but this
difference did not achieve statistical significance (9).
Two studies examined RFS
One study reported that systematic lymphadenectomy
involving removal of ≥11 lymph nodes was associated with lower RFS
compared with no systematic lymphadenectomy, regardless of patient
endometrial cancer risk classification (10). Another study (19) reported similar RFS for systematic
lymphadenectomy and no systematic lymphadenectomy.
Taken together, these data suggest that systematic
lymphadenectomy is associated with a higher combined rate of DFS
and PFS and a lower recurrence rate when compared with no
systematic lymphadenectomy (Tables
IV and V).
| Table V.Summary of results comparing
disease-related survival for SLA vs. no SLA. |
Table V.
Summary of results comparing
disease-related survival for SLA vs. no SLA.
| Study | Survival no.
(%) | Summary survival
dataa | P-value | Refs. |
|---|
| Progression-free
survival |
|
| Cragun
et al | >11 LNs, 246
(48%); <11 LNs, 263 (52%) | 5-year rate: 86.0%
vs. 75.0% | <0.001 | (7) |
|
|
| Low risk: 92.0% vs.
86.0% | >0.05 |
|
|
|
| High risk: 80.0%
vs. 60.0% | 0.001 |
|
| Kang
et al | >17.5 LNs, 64
(52%); 0 LNs, 58 (48%) | 5-year rate: 96.6%
vs. 98.3% | 0.61 | (22) |
|
Bassarak et al | >11 LNs, 120
(71%); 0 LNs, 51 (29%) | 5-year rate: 89.0%
vs. 87.0% | 0.69 | (16) |
| Disease-free
survival |
|
|
Benedetti et al | >11 LNs, 264
(51%); 0 LNs, 250 (49%) | 5-year rate: 81.7%
vs. 81.0% | 0.68 | (9) |
| Zhang
et al | >18 LNs, 246
(70%); 0 LNs, 103 (30%) | 5-year rate: 89.0%
vs. 80.7% | 0.02 | (8) |
|
|
| Low risk: 91.2% vs.
83.7% | 0.09 |
|
|
|
| Intermediate risk:
88.1% vs. 76.3% | 0.03 |
|
| Recurrence-free
survival |
|
|
Kitchener et al | >12 LNs, 546
(49%); <2 LNs, 573 (51%) | NR | 0.35 | (10) |
|
|
| Low risk: HR, 0.63
(CI, −6.28–7.53) | 0.86 |
|
|
|
| Intermediate and
high risk: |
|
|
|
|
| HR, 0.13 (CI,
−9.69–9.95) | 0.98 |
|
| Dowdy
et al | >11 LNs, 80
(21%); 0 LNs, 305 (79 %) | 5-year rate: 96.0%
vs. 97.6% | 0.64 | (19) |
| Cause-specific
survival |
|
|
Bassarak et al | >11 LNs, 120
(71%); 0 LNs, 51 (29%) | NR | 0.04 | (16) |
| Dowdy
et al | >11 LNs, 80
(21%); 0 LNs, 305 (79%) | 5-year rate: 97.3%
vs. 99.0% | 0.32 | (19) |
Association of OS with
lymphadenectomy
The 5-year OS rate, determined from 11 studies
(7–9,15,16,18–23),
ranged from 73.1 to 98.3% (median, 90%) in the systematic
lymphadenectomy group; this was higher than the rate in the no
systematic lymphadenectomy group, which ranged from 68 to 98.4%
(median, 88.2%). In the majority of studies, however, the OS
difference did not achieve statistical significance. Among
non-RCTs, only six trials (7,8,16,17,21,23) found
the difference to be significant (P<0.05), and neither of the
RCTs in the current review found the difference to be significant
after analyzing subgroups with different risk classifications
(9,10). The number of mortalities ranged from 1
to 53 patients across all studies, while recurrence ranged from 2.4
to 13.0%.
Subsequently, OS was investigated in subgroups of
patients with different risk classifications. Seven studies
reported subgroup data for a total of 38,489 patients with low-risk
disease and 11,696 with intermediate- to high-risk disease
(7,8,10,18,20,21,23).
The non-RCTs reported significantly higher OS rates for the
systematic lymphadenectomy than for the no systematic
lymphadenectomy procedure in patients with intermediate- and
high-risk disease (P<0.05) (7,8,18,21,23), while
OS rates were similar for the two procedures among patients with
low-risk disease. Data from these trials indicated a trend that
removal of ≥11 lymph nodes was associated with more favorable OS
compared with removal of <11 lymph nodes (7,8,18,21,23). The
results for OS are summarized in Tables
IV and VI.
| Table VI.Overall survival comparison of
systematic lymphadenectomy and no systematic lymphadenectomy, with
and without stratification by risk subgroup. |
Table VI.
Overall survival comparison of
systematic lymphadenectomy and no systematic lymphadenectomy, with
and without stratification by risk subgroup.
|
| Number of
patients | Overall
survivala |
|
|
|---|
|
|
|
|
|
|
|---|
| Study | Total | Mortalities | Recurrences | All risk
groups | Stratified by risk
group | P-value | Refs. |
|---|
| Kilgore et
al | 625 | NR | NR | 5-year rate: 87.0%
vs. 71.0% |
| <0.001 | (23) |
|
|
|
|
|
| Low risk: 95% vs.
83% | 0.53 |
|
|
|
|
|
|
| High risk: 63% vs.
36% | <0.001 |
|
| Gao et
al | 137 | NR | NR | 5-year rate: 73.1%
vs. 82.9% |
| >0.05 | (20) |
|
|
|
|
|
| Low risk: 82.4% vs.
96.4% | >0.05 |
|
|
|
|
|
|
| High risk: 73.9%
vs. 74.2% | >0.05 |
|
| Ceccaroni et
al | 130 | 1 | NR | 5-year rate: 92.7%
vs. 88.2% |
| 0.38 | (17) |
| Cragun et
al | 509 | 4 | 48 | 5-year rate: 88.0%
vs. 79.0% |
| <0.001 | (7) |
|
|
|
|
|
| Low risk: 94% vs.
89% | 0.45 |
|
|
|
|
|
|
| High risk: 82% vs.
64% | 0.001 |
|
| Benedetti et
al | 514 | 53 | 67 | 5-year rate: 85.9%
vs. 90.0% |
| 0.50 | (9) |
| Kang et
al | 122 | 2 | 3 | 5-year rate: 98.3%
vs. 98.4% |
| 0.95 | (22) |
| Kitchener et
al | 1119 | NR | NR | NR |
| 0.55 | (10) |
|
|
|
|
|
| Low risk: HR, 0.38
(CI, −4.89–5.64) | 0.88 |
|
|
|
|
|
|
| High risk: HR, 0.06
(CI, −8.65–8.77) | 0.99 |
|
| Ji et
al | 116 | NR | 12 | 5-year rate: 90.0%
vs. 89.5% |
| >0.05 | (24) |
| Bassrak et
al | 171 | NR | NR | 5-year rate: 89.0%
vs. 68.0% |
| <0.001 | (16) |
| Jeong et
al | 758 | NR | NR | 5-year rate: 95.0%
vs. 93.1% |
| 0.45 | (21) |
|
|
|
|
|
| High risk: 91.6%
vs. 70.6% | 0.009 |
|
| Chino et
al | 46449 | NR | NR | NR |
|
| (18) |
|
|
|
|
|
| Low risk: 93.8% vs.
92.9% | NR |
|
|
|
|
|
|
| Intermediate risk:
81.2% vs. 74.9% | <0.001 |
|
|
|
|
|
|
| High risk: 63.5%
vs. 48.2% | <0.001 |
|
| Zhang et
al | 349 | 32 | 40 | 5-year rate: 92.8%
vs. 81.5% |
| 0.001 | (8) |
|
|
|
|
|
| Low risk: 93.1% vs.
84.6% | 0.17 |
|
|
|
|
|
|
| Intermediate risk:
86.2% vs. 73.3% | 0.21 |
|
| Dowdy et
al | 385 | 31 | 11 | 5-year rate: 94.2%
vs. 92.1% |
| 0.72 | (19) |
Complications
The complications of lymphadenectomy were most often
reported to be lymphocysts and lymphedema, both of which were
reported in three studies (8,9,22). In one
of these studies, the two complications occurred in 35 of the 264
patients (13.2%) in the systematic lymphadenectomy group, but in
only 4 of the 250 patients (1.6%) in the no systematic
lymphadenectomy group (8). In the
other two studies, however, the rates of these complications were
similar between the two groups. Infrequent complications were
directly related to surgery (e.g., wound infection and nerve or
bladder injury)or the patient's medical condition (e.g., bowel
obstruction, deep venous thrombus and pneumonia). No
surgery-related mortalities were reported in any of the included
studies. Furthermore, no long-term complications and none of the
reported complications appeared to significantly affect long-term
survival.
Discussion
Whether systematic or no systematic lymphadenectomy
is more appropriate for patients in the early stages of endometrial
cancer is controversial. Although the systematic procedure should,
in principle, offer better protection against metastasis and
recurrence, the current systematic review of studies involving a
total of >50,000 patients from 6 countries suggests that
systematic lymphadenectomy does not reliably improve survival time
over no systematic lymphadenectomy when patients of all endometrial
cancer risk classes are combined. In addition, the systematic
procedure may be associated with higher rates of complications,
including lymphedema and lymphocysts, which reduce postoperative
quality of life and increase risk of mortality (12,25).
In the enrolled studies, the results were not
consistent. Certain studies reported no difference in OS rates
between systematic and no systematic lymphadenectomy (9,10), while
other studies indicated that systematic lymphadenectomy improved OS
(7,8,16,17,21,23). These
results must be interpreted carefully for a number of reasons.
Firstly, it is possible that only a small proportion of patients in
the systematic lymphadenectomy group underwent para-aortic
lymphadenectomy; in one study, for example, the proportion was only
26% (9). Secondly, it is possible
that a high proportion of patients in the systematic
lymphadenectomy group did not, in fact, undergo such extensive
dissection; in one study, for example, 60% of the systematic
lymphadenectomy group underwent dissection of <14 lymph nodes,
including the pelvic lymph nodes but not the para-aortic ones
(10). Furthermore, systematic and no
systematic lymphadenectomy were defined differently among the
included studies; six studies presented a vague definition of
systematic and no systematic lymphadenectomy (9,10,16,18,20,24),
while seven studies showed definite cut-off values of numbers of
removed lymph nodes for defining the two types of lymphadenectomy
(7,8,17,19,21–23). As
previous studies have emphasized that the number of removed lymph
nodes affects survival in patients with endometrial cancer
(26,27), the diverse definitions of systematic
lymphadenectomy may be the cause of the different efficacies of
systematic lymphadenectomy for OS in patients with endometrial
cancer.
The role of adjuvant radiation in early-stage
endometrial cancer is also controversial. Eight of the enrolled
studies, involving a total of 50,046 patients, reported the use of
postoperative adjuvant radiotherapy (7,9,10,16–18,21,23).
Four studies (7,16,18,23)
observed that systematic lymphadenectomy in patients with grade III
lesions and deep myometrial invasion and who were receiving
postoperative adjuvant radiotherapy resulted in better survival
than no systematic lymphadenectomy. However, four studies (9,10,17,21)
reported similar survival rates when comparing patients receiving
adjuvant radiotherapy. There may be potential for bias due to
adjuvant radiation blunting the effect of systematic
lymphadenectomy. Therefore, future investigation is required to
define the role of adjuvant radiation in early-stage endometrial
cancer.
Nevertheless, the current analysis does provide
evidence that systematic lymphadenectomy leads to higher OS rates
than the no systematic procedure specifically in patients with
intermediate- or high-risk early-stage endometrial cancer. Removing
≥11 lymph nodes from these patients led to more favorable OS
compared with the removal of a smaller number, regardless of the
cancer status of the lymph nodes. However, no definitive guidelines
are available regarding the number of lymph nodes that should be
dissected. Although nodal count is indicative of the extent of
lymphadenectomy, the number of nodes reported by the pathologist
depends not only on anatomical variations in patients, but also on
surgical expertise and the comprehensiveness of pathological
analysis. Chan and Kapp (28)
reported that systematic removal of all lymphatic tissue in the
retroperitoneal region may be the most accurate definition of a
complete lymphadenectomy. These findings suggest that systematic
lymphadenectomy to remove ≥11 lymph nodes, or even a complete
systematic removal of all lymphatic tissue, may be appropriate
therapy for patients with intermediate- or high-risk early-stage
endometrial cancer.
Metastasis of endometrial cancer to the lymph nodes
worsens prognosis and increases the risk of lymphatic recurrence
(29); 90% of patients who suffer
such recurrence succumb to the disease (30). One study reported 5-year survival rate
of 90% for patients with stage I endometrial cancer, compared to
only 54% for patients with metastatic stage III disease (31).
Several studies suggest that lymph node resection is
more reliable than surgery alone to determine whether endometrial
cancer has metastasized and to reduce the risk of metastasis
(10,11,32).
Although one study reported that only 4.6% of patients with
low-risk disease (stage I, grade 1) have lymph node metastases
(32), other studies have reported
that 98% of patients with para-aortic involvement have grossly
positive pelvic nodes (11), and that
9% of stage I patients have positive pelvic lymph nodes while 6%
have positive para-aortic nodes (33). Although several histopathological risk
factors have been demonstrated to correlate closely with lymph node
metastasis, including tumor grade, depth of myometrial invasion and
the presence of 30–50% serous or clear cell histology (34), lymphadenectomy remains the most direct
way to assess and reduce risk of metastasis. Previous studies
reported that high-risk patients who undergo para-aortic
lymphadenectomy as part of their surgical staging procedure exhibit
higher survival rates than those who undergo simple surgical
staging (35,36).
The current systematic review suggests that
systematic lymphadenectomy should be applied carefully to patients
with early-stage endometrial cancer, as it is unlikely to produce
clinical benefits in a high proportion of patients. A similar story
emerges from systematic reviews of lymphadenectomy to treat for
other malignancies, including prostatic cancer (37) and gastric cancer (38,39). These
reviews come to divergent conclusions, and the overall evidence of
clinical benefit is weak. This highlights the need for more
prospective, high-quality, controlled studies of the safety and
efficacy of systematic lymphadenectomy, in the context not only of
endometrial cancer but of other cancers as well.
While this systematic review contributes
significantly to the literature by examining a large number of
patients in several countries and ethnic groups, its findings are
nevertheless subject to several limitations. Firstly, only two of
the included trials are RCTs, while the remaining 11 are
retrospective non-RCTs. Secondly, patient selection, techniques
used to dissect lymph nodes and perform surgery, and postoperative
care and follow-up varied substantially across the included
studies, which weakens the strength of the conclusions. Thirdly, a
previous meta-analysis (40) has
shown that, in one of the included trials (26), which accounts for 12,333 of the
patients in the population included the present study, body mass
index varies significantly between the systematic and no systematic
lymphadenectomy groups and that controlling for this leads to a
significantly higher OS rate for the systematic lymphadenectomy
group than for the no systematic lymphadenectomy group. This
highlights the requirement for future studies to control for all
possible confounders when examining the clinical effects of
systematic lymphadenectomy.
In conclusion, the available evidence suggests that
systematic lymphadenectomy may improve OS in patients with
intermediate- or high-risk early-stage endometrial cancer,
particularly when ≥11 lymph nodes are removed; however, this may
not be the case in patients with low-risk disease. In addition,
systematic lymphadenectomy may be associated with higher rates of
lymphocysts and lymphedema. These findings argue that the use of
systematic lymphadenectomy in carefully selected patients may
improve endometrial cancer staging, choice of adjuvant therapy and
prognosis prediction.
Acknowledgements
This work was supported by the National Natural
Science Foundation of China (project no. 81060219).
References
|
1
|
Bray F, Loos AH, Oostindier M and
Weiderpass E: Geographic and temporal variations in cancer of the
corpus uteri: Incidence and mortality in pre- and postmenopausal
women in Europe. Int J Cancer. 117:123–131. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Murray T, Ward E, Samuels A,
Tiwari RC, Ghafoor A, Feuer EJ and Thun MJ: Cancer statistics,
2005. CA Cancer J Clin. 55:10–30. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sant M, Aareleid T, Berrino F, Bielska
Lasota M, Carli PM, Faivre J, Grosclaude P, Hédelin G, Matsuda T,
Møller H, et al: EUROCARE-3: Survival of cancer patients diagnosed
1990–94-results and commentary. Ann Oncol. 14(Suppl 5): S61–S118.
2003. View Article : Google Scholar
|
|
5
|
Creasman W: Revised FIGO staging for
carcinoma of the endometrium. Int J Gynaecol Obstet. 105:1092009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Greer BE, Koh WJ, Abu-Rustum N, Bookman
MA, Bristow RE, Campos S, Cho KR, Copeland L, Eifel P, Jaggernauth
W, et al: Uterine cancers. J Natl Compr Canc Netw. 4:438–462.
2006.PubMed/NCBI
|
|
7
|
Cragun JM, Havrilesky LJ, Calingaert B,
Synan I, Secord AA, Soper JT, Clarke-Pearson DL and Berchuck A:
Retrospective analysis of selective lymphadenectomy in apparent
early-stage endometrial cancer. J Clin Oncol. 23:3668–3675. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang H, Jia L, Zhang Q, Zhang Y, Yang X
and Kong B: Therapeutic role of systematic retroperitoneal
lymphadenectomy in endometrial cancer. Bull Cancer. 99:E10–E17.
2012.PubMed/NCBI
|
|
9
|
Benedetti Panici P, Basile S, Maneschi F,
Alberto Lissoni A, Signorelli M, Scambia G, Angioli R, Tateo S,
Mangili G, Katsaros D, et al: Systematic pelvic lymphadenectomy vs.
no lymphadenectomy in early-stage endometrial carcinoma: Randomized
clinical trial. J Natl Cancer Inst. 100:1707–1716. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
ASTEC study group. Kitchener H, Swart AM,
Qian Q, Amos C and Parmar MK: Efficacy of systematic pelvic
lymphadenectomy in endometrial cancer (MRC ASTEC trial): A
randomised study. Lancet. 373:125–136. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Morrow CP, Bundy BN, Kurman RJ, Creasman
WT, Heller P, Homesley HD and Graham JE: Relationship between
surgical-pathological risk factors and outcome in clinical stage I
and II carcinoma of the endometrium: A Gynecologic Oncology Group
study. Gynecol Oncol. 40:55–65. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Achouri A, Huchon C, Bats AS, Bensaid C,
Nos C and Lécuru F: Complications of lymphadenectomy for
gynecologic cancer. Eur J Surg Oncol. 39:81–86. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group: Preferred reporting items for systematic reviews
and meta-analyses: The PRISMA statement. Ann Intern Med.
151:264–269. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Green S, Higgins JPT, Alderson P, Clarke
M, Mulrow CD and Oxman AD: Cochrane Handbook for Systematic Reviews
of Interventions. Version 5.0.2.The Cochrane Book Series. John
Wiley & Sons, Ltd. (Hoboken, NJ). 2008.
|
|
15
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bassarak N, Blankenstein T, Brüning A,
Dian D, Bergauer F, Friese K and Mylonas I: Is lymphadenectomy a
prognostic marker in endometrioid adenocarcinoma of the human
endometrium? BMC Cancer. 10:2242010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ceccaroni M, Savelli L, Bovicelli A, Dian
D, Bergauer F, Friese K and Mylonas I: Prognostic value of pelvic
lymphadenectomy in surgical treatment of apparent stage I
endometrial cancer. Anticancer Res. 24:2073–2078. 2004.PubMed/NCBI
|
|
18
|
Chino JP, Jones E, Berchuck A, Secord AA
and Havrilesky LJ: The influence of radiation modality and lymph
node dissection on survival in early-stage endometrial cancer. Int
J Radiat Oncol Biol Phys. 82:1872–1879. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dowdy SC, Borah BJ, Bakkum-Gamez JN,
Weaver AL, McGree ME, Haas LR, Keeney GL, Mariani A and Podratz KC:
Prospective assessment of survival, morbidity and cost associated
with lymphadenectomy in low-risk endometrial cancer. Gynecol Oncol.
127:5–10. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gao Y, Yu A and Chen L: Place of value of
pelvic lymphadenectomy for treatment of endometrial neoplasms.
Zhonghua Fu Chan Ke Za Zhi. 35:264–266. 2000.(In Chinese).
PubMed/NCBI
|
|
21
|
Jeong NH, Lee JM, Lee JK, Kim MK, Kim YJ,
Cho CH, Kim SM, Park SY, Park CY and Kim KT: Role of systematic
lymphadenectomy and adjuvant radiation in early-stage endometrioid
uterine cancer. Ann Surg Oncol. 17:2951–2957. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kang WD, Kim CH, Cho MK, Kim JW, Kim YH,
Choi HS and Kim SM: Lymphadenectomy for low-risk endometrial cancer
based on preoperative and intraoperative assessments. Int J Gynecol
Cancer. 19:657–661. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kilgore LC, Partridge EE, Alvarez RD,
Austin JM, Shingleton HM, Noojin F III and Conner W: Adenocarcinoma
of the endometrium: Survival comparisons of patients with and
without pelvic node sampling. Gynecol Oncol. 56:29–33. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ji RY, Gao N, Li Y, Yang Y, Liu S and Yao
X: Clinical analysis of 116 cases of early stage endometrial
cancer. Chinese Journal of Clinical Oncology. 36:917–919. 2009.
|
|
25
|
Angioli R, Plotti F, Cafà EV, Dugo N,
Capriglione S, Terranova C, Montera R, Guzzo F and Panici PB:
Quality of life in patients with endometrial cancer treated with or
without systematic lymphadenectomy. Eur J Obstet Gynecol Reprod
Biol. 170:539–543. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chan JK, Cheung MK, Huh WK, Osann K,
Husain A, Teng NN and Kapp DS: Therapeutic role of lymph node
resection in endometrioid corpus cancer: A study of 12,333
patients. Cancer. 107:1823–1830. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lutman CV, Havrilesky LJ, Cragun JM,
Secord AA, Calingaert B, Berchuck A, Clarke-Pearson DL and Soper
JT: Pelvic lymph node count is an important prognostic variable for
FIGO stage I and II endometrial carcinoma with high-risk histology.
Gynecol Oncol. 102:92–97. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chan JK and Kapp DS: Role of complete
lymphadenectomy in endometrioid uterine cancer. Lancet Oncol.
8:831–841. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mariani A, Webb MJ, Keeney GL, Aletti G
and Podratz KC: Predictors of lymphatic failure in endometrial
cancer. Gynecol Oncol. 84:437–442. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Mariani A, Webb MJ, Keeney GL and Podratz
KC: Routes of lymphatic spread: A study of 112 consecutive patients
with endometrial cancer. Gynecol Oncol. 81:100–104. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lurain JR, Rice BL, Rademaker AW,
Poggensee LE, Schink JC and Miller DS: Prognostic factors
associated with recurrence in clinical stage I adenocarcinoma of
the endometrium. Obstet Gynecol. 78:63–69. 1991.PubMed/NCBI
|
|
32
|
Abu-Rustum NR, Iasonos A, Zhou Q, Oke E,
Soslow RA, Alektiar KM, Chi DS and Barakat RR: Is there a
therapeutic impact to regional lymphadenectomy in the surgical
treatment of endometrial carcinoma? Am J Obstet Gynecol. 198(457):
e451–455. 2008.(Discussion 457, e455–456).
|
|
33
|
Creasman WT, Morrow CP, Bundy BN, Homesley
HD, Graham JE and Heller PB: Surgical pathologic spread patterns of
endometrial cancer. A Gynecologic Oncology Group Study. Cancer.
60(8 Suppl): S2035–S2041. 1987. View Article : Google Scholar
|
|
34
|
Creasman WT, Mutch DE and Herzog TJ: ASTEC
lymphadenectomy and radiation therapy studies: Are conclusions
valid? Gynecol Oncol. 116:293–294. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mariani A, Webb MJ, Galli L and Podratz
KC: Potential therapeutic role of para-aortic lymphadenectomy in
node-positive endometrial cancer. Gynecol Oncol. 76:348–356. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Todo Y, Kato H, Kaneuchi M, Watari H,
Takeda M and Sakuragi N: Survival effect of para-aortic
lymphadenectomy in endometrial cancer (SEPAL study): A
retrospective cohort analysis. Lancet. 375:1165–1172. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Gao L, Yang L, Lv X, Bu S, Wan F, Qian S,
Wei Q, Han P and Fan T: A systematic review and meta-analysis of
comparative studies on the efficacy of extended pelvic lymph node
dissection in patients with clinically localized prostatic
carcinoma. J Cancer Res Clin Oncol. 140:243–256. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wang Z, Chen JQ and Cao YF: Systematic
review of D2 lymphadenectomy versus D2 with para-aortic nodal
dissection for advanced gastric cancer. World J Gastroenterol.
16:1138–1149. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Brar SS, Seevaratnam R, Cardoso R, Law C,
Helyer L and Coburn N: A systematic review of spleen and pancreas
preservation in extended lymphadenectomy for gastric cancer.
Gastric Cancer. 15(Suppl 1): S89–S99. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kim HS, Suh DH, Kim MK, Chung HH, Park NH
and Song YS: Systematic lymphadenectomy for survival in patients
with endometrial cancer: A meta-analysis. Jpn J Clin Oncol.
42:405–412. 2012. View Article : Google Scholar : PubMed/NCBI
|