Introduction
Lung cancer is a common and very serious type of
cancer, is one of the major causes of cancer related mortality
worldwide (1), and >80% of lung
cancer cases are non-small cell lung cancer (NSCLC) (2). Although there have been improvements in
diagnostic approaches and the introduction of novel therapeutic
agents during the last decades, the 5-year survival rate of lung
cancers remains low due to high recurrence rates and early
metastasis (3). Thus, it is important
and urgent to identify novel markers to predict NSCLC recurrence
and metastasis.
5-methylcytosine (5-mC) is a usual epigenetic
modification in mammalian DNA, and the process of cytosine
converting to 5-mC is catalyzed by DNA methyltransferases (DNMTs)
(4). In mammals, the ten-eleven
translocation (TET) family proteins can hydroxylate 5-mC to
5-hydroxymethylcytosine (5-hmC) (5),
which can be further oxidized to produce 5-formylcytosine (5-fC)
and 5-carboxylcytosine (5-caC), which is finally be corrected by
thymine DNA glycosylase (TDG) (6).
Generally, this circulation of cytosine methylation and
demethylation exists in all kinds of elementary processes in
mammalian cells, such as genome stability and imprinting (7). As an intermediate in DNA demethylation
processes, 5-hmC is considered to serve an important role in the
diagnosis and prognosis prediction of several malignant tumors; for
example, the loss of 5-hmC has been reported to be involved in
intrahepatic cholangiocarcinoma (ICC) and gastric cancer
progression, and high levels of 5-hmC are associated with favorable
prognosis in hepatocellular carcinoma (HCC) (8). Notably, a previous study has indicated
that the loss of 5-hmC was implicated in the onset of malignant
cellular transformation, and may serve as an epigenetic hallmark of
a number of types of cancer (9).
Although the importance of 5-hmC in cancer has been established,
its role and clinical significance in NSCLC remain to be
determined.
The present study aimed to determine the level of
5-hmC in NSCLC and their adjacent normal tissues, and then detected
the 5-hmC level by immunohistochemistry in NSCLC tissue
microarrays. In addition, the relationship between the 5-hmC level
and the NSCLC clinical and pathological characteristics were
analyzed. Finally, the clinical value of 5-hmC in NSCLC was also
determined.
Patients and methods
Patients and specimens
All specimens were obtained from 208 NSCLC patients
who received curative resection at Zhongshan Hospital of Fudan
University (Shanghai, China) in 2005. The collection and
conservation of samples and details of the cohort are in agreement
with the description of our previous study (10). Briefly, tumor stage was adjudged on
the basis of the tumor node metastasis (TNM) 7th edition of
International Union Against Cancer Staging Manual (11). Pathological classification was ruled
according to the World Health Organization criteria (12). The follow-up was terminated in July
2010. The median follow-up period was 43 months (range, 1–66
months). The overall survival (OS) was defined as the interval
between surgery and death or between surgery and the last
observation for surviving patients. Ethical approval was obtained
from the Zhongshan Hospital Research Ethics Committee, and written
consent was obtained from all patients.
Dot-blot analysis
Dot-blot protocol was described elsewhere (8). In brief, total DNA was denatured with
0.4 M NaOH, 10 mM EDTA at 99°C for 5 min and then neutralized by
adding an equal volume of cold 2 M ammonium acetate (pH 7.0). An
equal value of genomic DNA was then spotted on nitrocellulose
membranes (2 µl per spot; 150 ng/µl). After ultraviolet
cross-linking, membranes were blocked 1 h with 5% BSA in TBST and
then incubated with mouse monoclonal anti-5-hmC antibody (1:10,000;
catalog no., 39999; Active Motif, La Hulpe, Belgium) overnight at
4°C and followed subjecting to western blotting detection. The
protocol of western blotting was described elsewhere (13).
Tissue microarrays and
immunohistochemistry
Tissue microarrays (TMAs) were established by
Shanghai Biochip Co. Ltd (Shanghai, China) and are described in our
previous study (10).
Immunohistochemistry was performed according to our previous study
(14). In brief, the slides were
dewaxed at 65°C for 2 h, followed by washing with xylene,
rehydrating in ethanol, and then endogenous peroxidase activity was
blocked in 3% H2O2 for 15 min. Antigen
retrieval was performed by heating the samples at 100°C for 20 min
in 10 mmol/l sodium citrate (pH 6.0). Then, after cooling to room
temperature, the TMA slides were placed in 2 M HCl for 30 min,
rinsed in PBS buffer, and further placed in 100 mM Tris-HCl (pH
8.0) for 10 min. They were then incubated in 5% BSA at room
temperature for 60 min to reduce nonspecific reactions.
Subsequently, the slides were incubated overnight at 4°C with
rabbit monoclonal anti-5-hmC antibody (1:10,000). Then the slides
were incubated with goat polyclonal anti-mouse IgG2a-hydrogen
peroxidase conjugated secondary antibody (1:2000; catalog no.,
ab97245; Abcam, Cambridge, UK) for 60 min at 37°C and stained with
diaminobenzidine-H2O2 (Beyotime Institute of
Biotechnology, Haimen, China). Finally, the TMA slides were
counterstained with hematoxylin (Sigma-Aldrich, St. Louis, MO,
USA), dehydrated, and mounted with a cover slip using a neutral
resin.
Evaluation of immunostaining
intensity
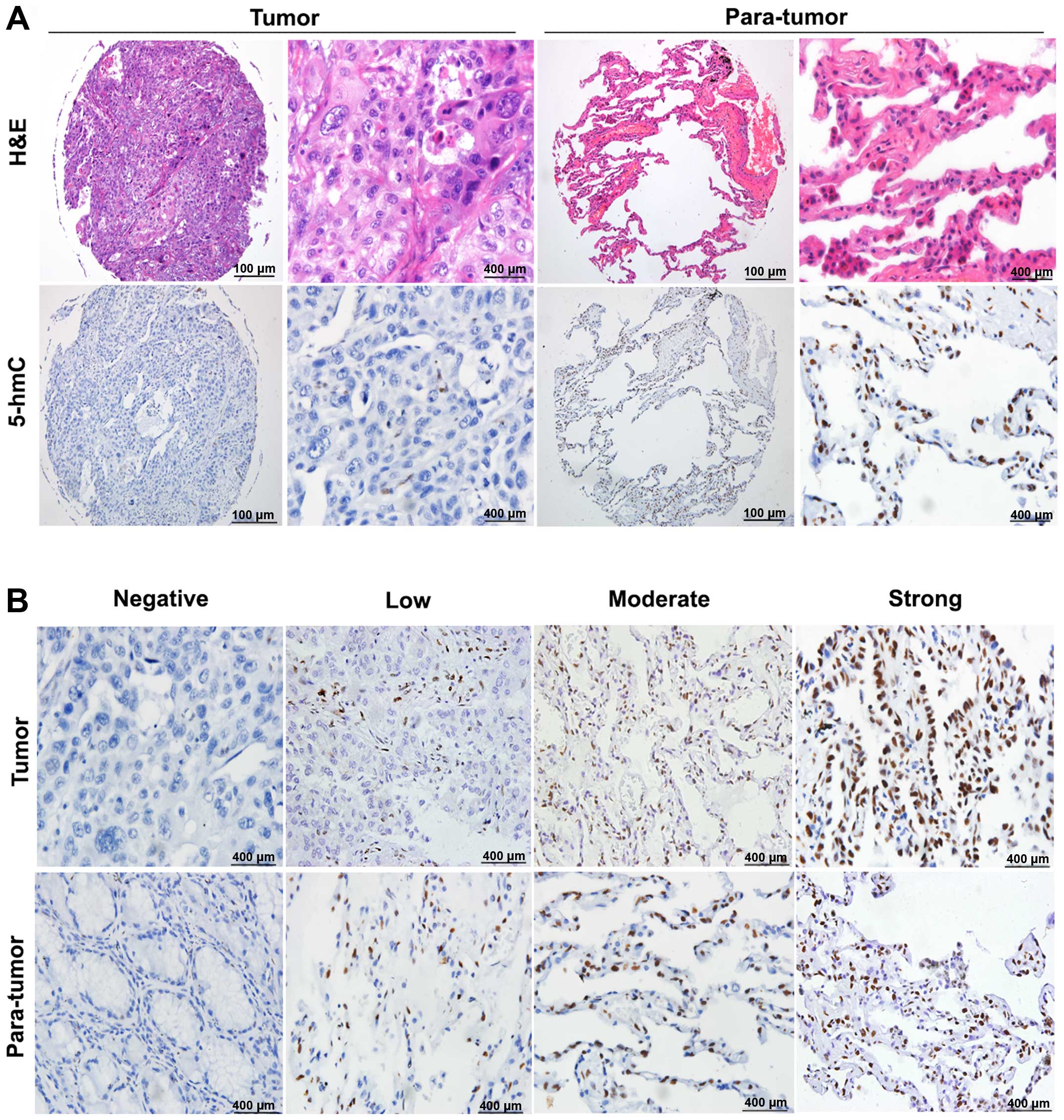
The 5-hmC was immunohistochemically stained yellow
or brown located in the cell nucleus. The method for judging
immunohistochemical staining was described elsewhere (8). Briefly, the samples were scored
independently according to the intensity of cellular staining and
the proportion of stained cells. The proportion of stained cells in
total cell number of every point about ≤25%, 25 to 50%, 50 to 75%,
>75% were scored as 0, 1, 2, 3, 4 points, respectively. The
intensity of cellular staining was determined by the degree of
color, namely none, weak (yellow), medium (brown), and strong (dark
brown) were scored as 0, 1, 2, 3 points, respectively. The final
additive score of 0–1, 2–3, 4–5 and 6–7 points were divided into
negative (−), weak positive (+), moderate positive (++) and strong
positive (+ + +), respectively. The negative and weak positive
staining were defined as the low level group, and the moderate
positive and strong positive staining were defined as the high
level group of 5-hmC level, respectively.
Statistical analysis
Statistical analyses were handled using the SPSS
17.0 software package (SPSS Inc., Chicago, IL, USA). OS was
calculated using the Kaplan-Meier method and was analyzed using the
log-rank test. A Cox proportional hazards regression model was used
to analyze independent prognostic factors. For comparisons of
individual variables, t-tests, chi-square tests, Fisher exact
tests, and Spearman coefficient tests were used when necessary.
Statistical significance was determined for 2-tailed tests at
P<0.05.
Results
The 5-hmC level was significantly
down-regulated in NSCLC tissues
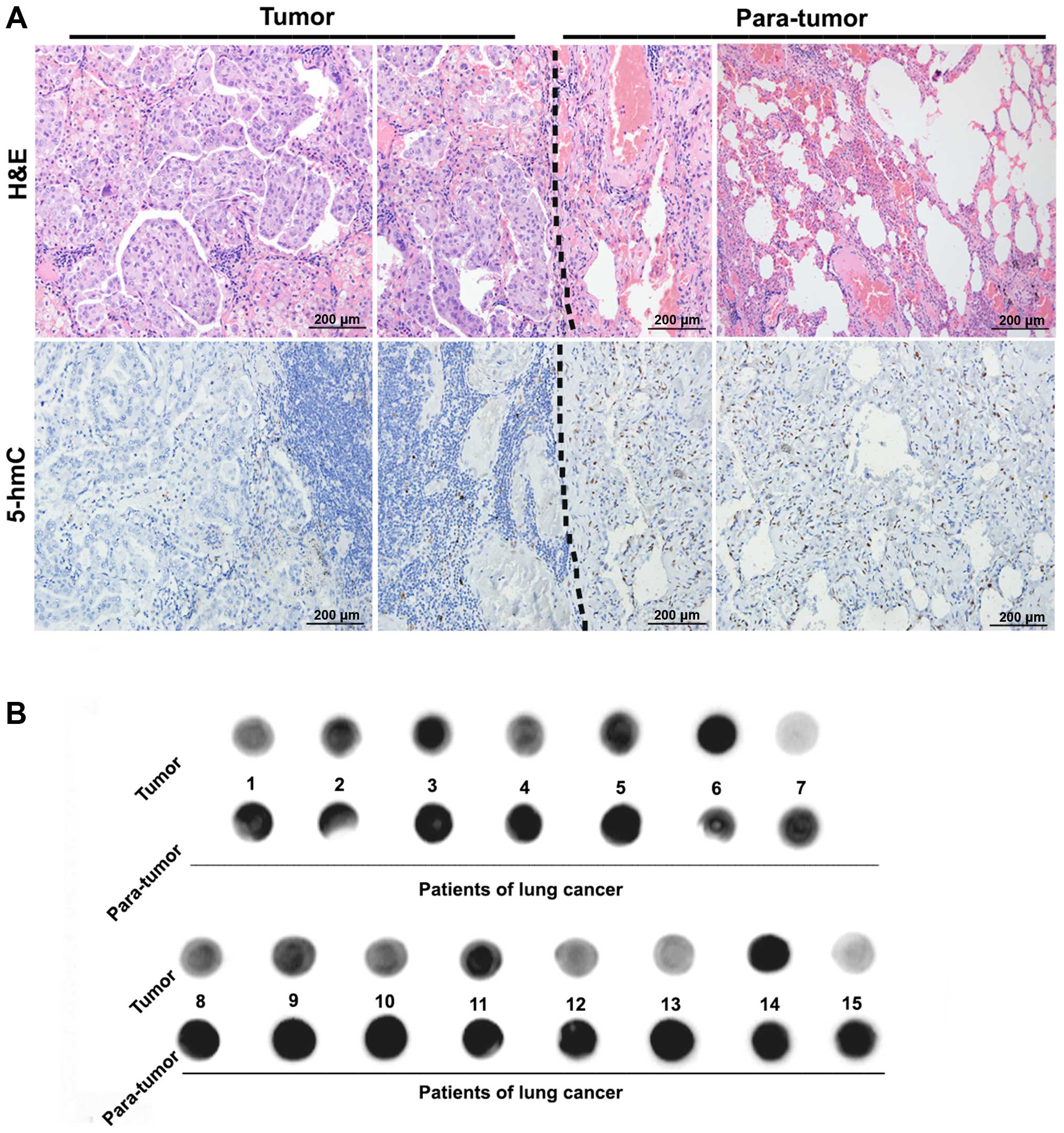
The level of 5-hmC in NSCLC and their adjacent lung
tissues in the same slides were detected by immunohistochemical
staining. As presented in (Fig. 1A),
after identification of NSCLC and normal lung tissues by
hematoxylin and eosin (H&E) staining, it was observed that the
staining of 5-hmC was located in the nucleus, and the level of
5-hmC in NSCLC tissues was lower than that in the adjacent normal
lung tissues, the difference was significant (P<0.05) as was
observed in a previous report in HCC (8). Furthermore, the dot-blot analysis also
supported the results from the immunochemical analysis (Fig. 1B). The above results indicate that the
loss of 5-hmC may be involved in the onset and progression of
NSCLC.
TMAs analysis and clinicopathological
features
The difference in 5-hmC levels were determined
between NSCLC tissues and the corresponding para-tumor tissues
using a tissue microarray technique. The results demonstrated that
the overall level of 5-hmC in NSCLC tissues was markedly lower than
that in matched adjacent normal tissues. Fig. 2A presents representative photos
including H&E and immunohistochemical staining to highlight the
difference. Notably, we also observed a phenomenon that several
levels of 5-hmC simultaneously came in the results of NSCLC tissues
and paired adjacent normal tissues (Fig.
2B).
Subsequently, the clinicopathological features of
NSCLC in this cohort were analyzed. A total of 208 cases of primary
NSCLC were involved in this analysis, the cohort contained 148
males and 60 females, and 85 squamous cell carcinoma, 110
adenocarcinomas and 13 other pathologic subtypes of NSCLC
(including adenosquamous carcinoma, large-cell carcinoma,
mucoepidermoid carcinoma and carcinosarcoma). A total of 144 tumors
were in TNM stages I–II and 64 tumors were in stages III–IV. In
addition, 93 tumors were low differentiation, and 115 tumors were
highly differentiated. The statistical details about patients and
the association between 5-hmC level and the clinicopathological
features are displayed in Table
I.
 | Table I.Correlation between 5-hmC and
clinicopathological characteristics in 208 NSCLCs. |
Table I.
Correlation between 5-hmC and
clinicopathological characteristics in 208 NSCLCs.
|
|
| 5-hmC level |
|
|---|
|
|
|
|
|
|---|
| Variables | No. of patients | Low | High | P |
|---|
| Age |
|
|
| 0.468 |
|
<60 | 102 | 64 | 38 |
|
| ≥60 | 106 | 72 | 34 |
|
| Gender |
|
|
| 0.004 |
| Male | 148 | 106 | 42 |
|
|
Female | 60 | 30 | 30 |
|
| Smoking status |
|
|
| 0.140 |
|
Smoker | 84 | 60 | 24 |
|
|
Non-smoker | 124 | 76 | 48 |
|
| Histological
type |
|
|
|
<0.001b |
| Squamous
cell carcinoma | 85 | 71 | 14 |
|
|
Adenocarcinoma | 110 | 55 | 55 |
|
|
Othera | 13 | 10 | 3 |
|
| Tumor stage |
|
|
| 0.059 |
| I–II | 144 | 88 | 56 |
|
|
III–IV | 64 | 48 | 16 |
|
| Lymph node
metastasis |
|
|
| <0.001 |
| Yes | 90 | 71 | 19 |
|
| No | 118 | 65 | 53 |
|
| Tumor size |
|
|
| 0.031 |
| <3
cm | 69 | 38 | 31 |
|
| ≥3
cm | 139 | 98 | 41 |
|
|
Differentiation |
|
|
| 0.381 |
|
Well/moderate | 115 | 72 | 43 |
|
|
Poor | 93 | 64 | 29 |
|
Association between 5-hmC level and
the clinicopathological parameters of NSCLC
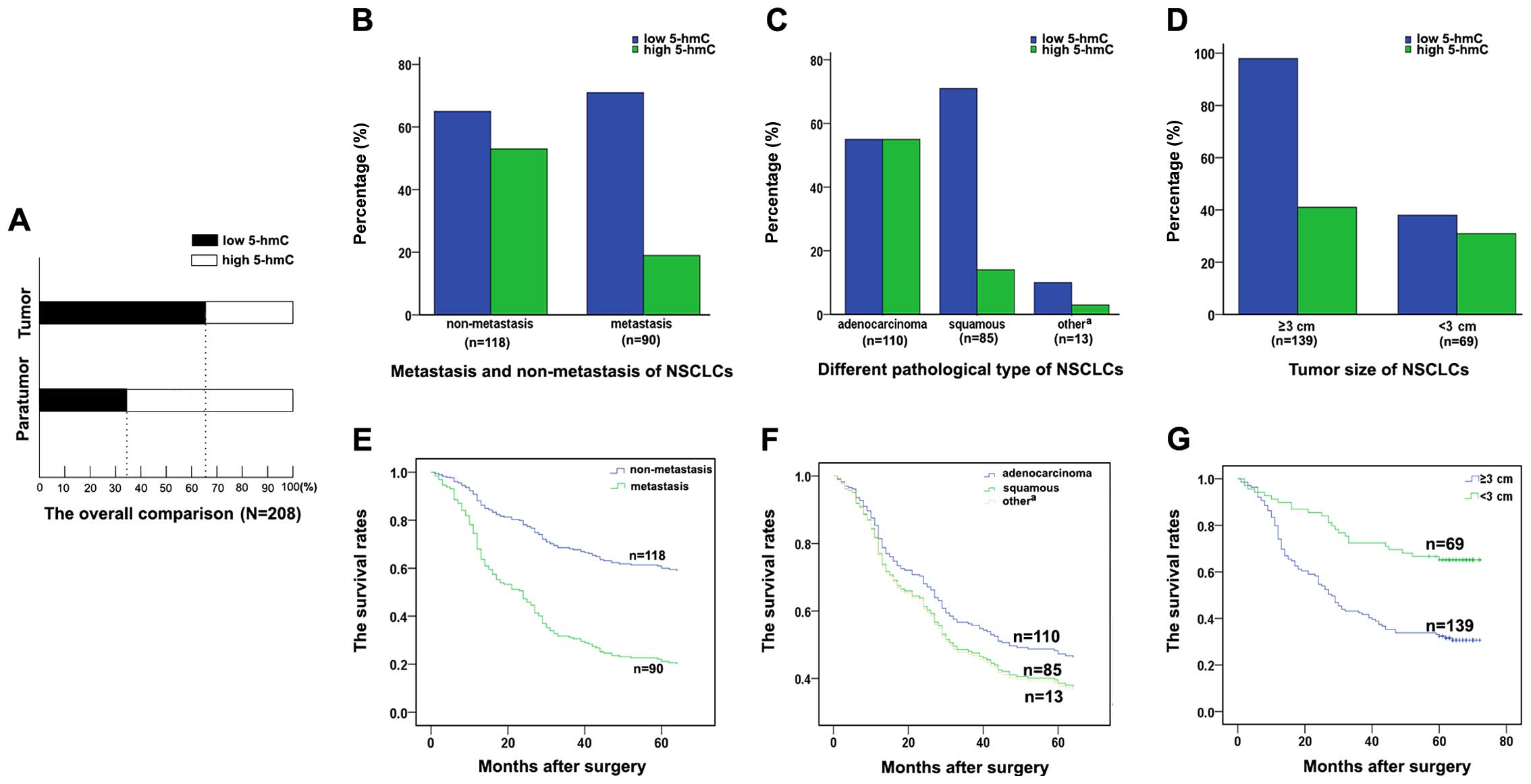
The relationship between the clinicopathological
parameters of NSCLC and 5-hmC levels were analyzed, and it
demonstrated that a low level of 5-hmC accounted for 65.38%
(136/208) specimens from NSCLC patients (P<0.001, Fig. 3A). Furthermore, the 5-hmC level was
significantly associated with lymph node metastasis (P<0.001),
histological type (P<0.001) and tumor size (P=0.031). NSCLC
patients with lymph node metastases had significantly higher
proportion of low 5-hmC level than those without lymph node
metastases (Fig. 3B). Particularly,
this high proportion of low 5-hmC level was more strongly
associated with squamous cell carcinomas than with adenocarcinomas
(Fig. 3C). Notably, a high proportion
of low 5-hmC level was also present in tissues with large tumor
size (Fig. 3D). The patients with a
high proportion of low 5-hmC level possessed a more unfavorable
prognosis compared with the patients with a low proportion of low
5-hmC level (Fig. 3E–G). However,
other clinicopathological features, including age, smoking status,
were not directly associated with the level of 5-hmC.
Low level of 5-hmC was correlated with
poor prognosis of NSCLC
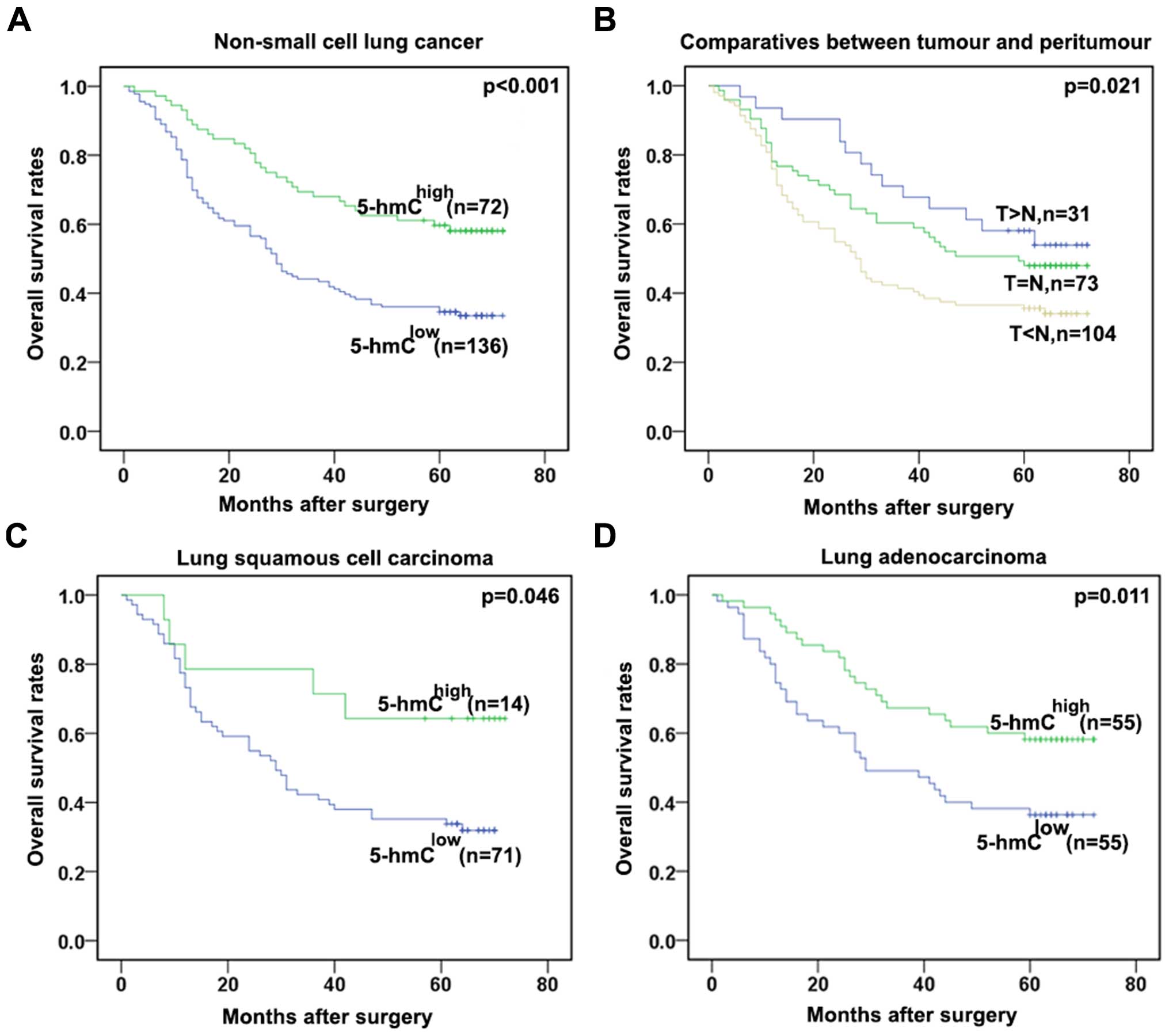
During the following-up, 120 patients succumbed to
recurrence or metastasis of disease. The 5-year OS rate after
surgery for all patients was 47.6%. The 5-year OS rate for patients
with low 5-hmC level was significantly lower than patients with
high 5-hmC level (P<0.001, Fig.
4A). In order to determine the effect exerted on the tumors of
corresponding patients of different 5-hmC levels, the 208 patients
were divided into 3 groups according to the difference in the
intensity of immunostaining between tumors and their matched
adjacent tissues in TMAs. The T<N group, whose immumostaining
intensity was significantly lower in tumor tissues compared with
the paired peritumors, had the worst OS rate. By contrast, the
T>N group with a higher immunostaining intensity in the tumor
tissues compared with the matched para-tumor possessed a better
prognosis than the other groups (T>N vs. T=N; P=0.021; Fig. 4B). As the 5-hmC levels were different
between the squamous cell carcinoma and adenocarcinomas, a subgroup
analysis by pathological subtype was performed. In squamous cell
carcinoma and adenocarcinomas, the association remained significant
(P=0.046 and P=0.011, respectively) (Fig.
4C and D). These data further revealed that low 5-hmC levels
may predict a poor prognosis of NSCLC patients.
Univariate and multivariate analyses
of predictive factors of OS for patients
Univariate analysis revealed that tumor size (≥3
cm), lymph node metastasis, high TNM stage, poor differentiation
and low 5-hmC level were associated with a shorter OS. Univariate
analysis revealed that tumor size (≥3 cm; P<0.001), lymph node
metastasis (P<0.001), high TNM stage (P<0.001), poor
differentiation (P<0.001) and low 5-hmC level (P<0.001) were
associated with a shorter OS rate. In multivariate analysis, tumor
size (P=0.003), lymph node metastasis (P=0.050), tumor stage
(P=0.034) and 5-hmC level (P=0.014) were identified as independent
prognostic factors in patients' OS rate (Table II).
| Table II.Univariate and multivariate analysis
of factors associated with OS. |
Table II.
Univariate and multivariate analysis
of factors associated with OS.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | HR | 95% CI | P | HR | 95% CI | P |
|---|
| Gender (male vs.
female) | 0.789 | 0.526–1.183 | 0.251 |
|
|
|
| Smoking status
(non-smokers vs. smokers) | 1.284 | 0.895–1.843 | 0.175 |
|
|
|
| Tumor size (≥3 cm
vs. <3 cm) | 2.755 | 1.758–4.318 | <0.001 | 2.019 | 1.269–3.211 | 0.003 |
| Lymph node
metastasis (yes vs. no) | 3.042 | 2.103–4.399 | <0.001 | 1.902 | 1.210–2.989 | 0.005 |
| Tumor stage (III–IV
vs. I–II) | 2.771 | 1.922–3.993 | <0.001 | 1.611 | 1.036–2.506 | 0.034 |
| Differentiation
(well/moderate vs. poor) | 1.431 | 1.000–2.049 | 0.050 | 1.202 | 0.833–1.735 | 0.325 |
| 5-hmC level (low
vs. high) | 0.476 | 0.315–0.720 | <0.001 | 0.589 | 0.386–0.897 | 0.014 |
Discussion
5-hmC, as the hydroxylated form of 5-mC, was first
discovered in T-even phage DNA in 1952 (15). A previous study indicated that 5-hmC
was associated with diseases such as nerve disorders, leukemia and
tumors (16). In recent years, 5-hmC
has become more extensively studied. Previous studies have reported
its position and prognostic value in a variety of tumors (17). However, the relationship between 5-hmC
level and the progression of lung cancer and prognosis of patients
with lung cancer remains unknown. In the present study, a
significant decrease in 5-hmC levels were obserevd in lung cancer
tissues compared with the adjacent tissues and the OS of patients
with low 5-hmC levels were distinctly lower than patients with high
5-hmC level, which were both in line with the previous reports in
HCC, ICC and gastric cancer (8).
Clinically, 5-hmC level was significantly related to lymph node
metastasis, histological type and tumor size. Furthermore, the
5-hmC level was identified as an independent prognostic factor for
NSCLC patients' OS in this cohort. Thus, it can be concluded that
low levels of 5-hmC promote the NSCLC progression.
In 2009, two reports (18,19)
published in Science, indicated that 5-hmC exists as
prevalently as 5-mC in mammalian genomic DNA, and 5-hmC is now
generally accepted as ‘the sixth base’ of genomes of higher
organisms (20). Similar to 5-mC,
5-hmC not only exhibits its universal and dynamic characteristics,
but also participates in a number of important regulations of
cellular functions including tumorigenesis and tumor progression
(21). In the present study, the
level of 5-hmC in NSCLC and their corresponding paired normal lung
tissues was detected by immunohistochemistry and dot-blot
semi-quantitative analysis. Furthermore, it was demonstrated that
the proportion of low 5-hmC level was less frequent in
adenocarinoma compared with the other types of NSCLC, and there
were varying expression levels of 5-hmC in lung cancer and normal
tissues. Generally, the 5-hmC levels were lower in NSCLC
samples.
The relationship between the 5-hmC level and
pathological characteristics of NSCLC were further analyzed.
Consitent with other reports (22),
in the present study, low levels of 5-hmC were more common in
patients with lymph node metastases, high histological types and
large tumor sizes, which are recognized prognostic factors for lung
cancer (23). The proportion of low
5-hmC level in NSCLC patients with lymph node metastases was
markedly higher than those patients without lymph node metastases,
as well as the histological types and tumor sizes. Moreover, for
the association between the 5-hmC levels and prognostic factors of
lung cancer the analytic results demonstrated that low levels of
5-hmC was associated with the poor prognosis of NSCLC. The
multivariate analyses demonstrated that low levels of 5-hmC may be
an independent prognostic factor in NSCLC.
In summary, the present study demonstrated that the
5-hmC levels were significantly lower in NSCLC tissues compared
with the corresponding adjacent cancer tissues, and revealed that
low levels of 5-hmC may be an important and potential prognostic
biomarker to screen patients with an unfavorable prognosis.
Acknowledgements
The present work was supported by the National
Natural Science Foundation of China (grant nos. 81201834, 81372313
and 81401876), the Fund of Shanghai Municipal Health Bureau (grant
nos. 20124324 and 20134322), and the project for the development of
young teachers (grant no. JJF152065).
Glossary
Abbreviations
Abbreviations:
|
NSCLC
|
non-small cell lung cancer
|
|
5-mC
|
5-methylcytosine
|
|
5-hmC
|
5-hydroxymethylcytosine
|
|
DNMTs
|
DNA methyltransferases
|
|
TET
|
ten-eleven translocation
|
|
TNM
|
tumor-lymph-node metastasis
|
|
OS
|
overall survival
|
|
TMAs
|
tissue microarrays
|
References
|
1
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Qiu X, Liang Y, Sellers RS, Perez-Soler R
and Zou Y: Aerosol azacytidine inhibits orthotopic lung cancers in
mice through Its DNA demethylation and gene reactivation effects.
PLoS One. 9:e1098742014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goldstraw P, Crowley J, Chansky K, Giroux
DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V and Sobin L:
International Association for the Study of Lung Cancer
International Staging Committee; Participating Institutions: The
IASLC lung cancer staging project: Proposals for the revision of
the TNM stage groupings in the forthcoming (seventh) edition of the
TNM Classification of malignant tumours. J Thorac Oncol. 2:706–714.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liutkevičiūtė Z, Kriukienė E, Ličytė J,
Rudytė M, Urbanavičiūtė G and Klimašauskas S: Direct
decarboxylation of 5-carboxylcytosine by DNA C5-methyltransferases.
J Am Chem Soc. 136:5884–5887. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Delhommeau F, Dupont S, Della Valle V,
James C, Trannoy S, Massé A, Kosmider O, Le Couedic JP, Robert F,
Alberdi A, et al: Mutation in TET2 in myeloid cancers. N Engl J
Med. 360:2289–2301. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wu H, Wu X, Shen L and Zhang Y:
Single-base resolution analysis of active DNA demethylation using
methylase-assisted bisulfite sequencing. Nat Biotechnol.
32:1231–1240. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li Y, Córdoba-Cañero D, Qian W, Zhu X,
Tang K, Zhang H, Ariza RR, Roldán-Arjona T and Zhu JK: An AP
endonuclease functions in active DNA dimethylation and gene
imprinting in Arabidopsis (corrected). PLoS Genet. 11:e10049052015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dong ZR, Zhang C, Cai JB, Zhang PF, Shi
GM, Gao DM, Sun HC, Qiu SJ, Zhou J, Ke AW and Fan J: Role of
5-hydroxymethylcytosine level in diagnosis and prognosis prediction
of intrahepatic cholangiocarcinoma. Tumour Biol. 36:2763–2771.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kudo Y, Tateishi K, Yamamoto K, Yamamoto
S, Asaoka Y, Ijichi H, Nagae G, Yoshida H, Aburatani H and Koike K:
Loss of 5-hydroxymethylcytosine is accompanied with malignant
cellular transformation. Cancer Sci. 103:670–676. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gu J, Ding JY, Lu CL, Lin ZW, Chu YW, Zhao
GY, Guo J and Ge D: Overexpression of CD88 predicts poor prognosis
in non-small-cell lung cancer. Lung Cancer. 81:259–265. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sica GL and Gal AA: Lung cancer staging:
Pathology issues. Semin Diagn Pathol. 29:116–126. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Travis WD, Brambilla E, Nicholson AG,
Yatabe Y, Austin JH, Beasley MB, Chirieac LR, Dacic S, Duhig E,
Flieder DB, et al: WHO Panel: The 2015 World Health Organization
Classification of Lung Tumors: Impact of Genetic, Clinical and
Radiologic Advances Since the 2004 Classification. J Thorac Oncol.
10:1243–1260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ke AW, Shi GM, Zhou J, Huang XY, Shi YH,
Ding ZB, Wang XY, Devbhandari RP and Fan J: CD151 amplifies
signaling by integrin α6β1 to PI3K and induces the
epithelial-mesenchymal transition in HCC cells. Gastroenterology.
140:1629–1641.e15. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhao GY, Ding JY, Lu CL, Lin ZW and Guo J:
The overexpression of 14-3-3ζ and Hsp27 promotes non-small cell
lung cancer progression. Cancer. 120:652–663. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hattman S: The first recognized epigenetic
signal: DNA glucosylation of T-even bacteriopages. Epigenetics.
4:150–151. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yin R, Mo J, Lu M and Wang H: Detection of
human urinary 5-hydroxymethylcytosine by stable isotope dilution
HPLC-MS/MS analysis. Anal Chem. 87:1846–1852. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang Q, Wu K, Ji M, Jin W, He N, Shi B and
Hou P: Decreased 5-hydroxymethylcytosine (5-hmC) is an independent
poor prognostic factor in gastric cancer patients. J Biomed
Nanotechnol. 9:1607–1616. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kriaucionis S and Heintz N: The nuclear
DNA base 5-hydroxymethylcytosine is present in Purkinje neurons and
the brain. Science. 324:929–930. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tahiliani M, Koh KP, Shen Y, Pastor WA,
Bandukwala H, Brudno Y, Agarwal S, Iyer LM, Liu DR, Aravind L and
Rao A: Conversion of 5-methylcytosine to 5-hydroxymethylcytosine in
mammalian DNA by MLL partner TET1. Science. 324:930–935. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Moen EL, Mariani CJ, Zullow H, Jeff-Eke M,
Litwin E, Nikitas JN and Godley LA: New themes in the biological
functions of 5-methylcytosine and 5-hydroxymethylcytosine. Immunol
Rev. 263:36–49. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ye C and Li L: 5-hydroxymethylcytosine: A
new insight into epigenetics in cancer. Cancer Biol Ther. 15:10–15.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ulas A, Turkoz FP, Silay K, Tokluoglu S,
Avci N, Oksuzoglu B and Alkis N: A laboratory prognostic index
model for patients with advanced non-small cell lung cancer. PLoS
One. 9:e1144712014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Campobasso O, Andrion A, Mancuso M, De
Simone M and Ribotta M: The postoperative survival in pulmonary
carcinomas depending on the histological type and stage. Ann Osp
Maria Vittoria Torino. 31:9–24. 1989.(In Italian). PubMed/NCBI
|