Introduction
Breast cancer (BC) is the most common cancer in
women, and is a heterogeneous disease, which has complicated its
treatment and study (1). Based on the
expression of specific receptors, BC is clinically divided into
estrogen receptor (ER)-positive BC (the most common and diverse
group), progesterone receptor (PR)-positive BC and human epidermal
growth factor receptor 2 (HER2; also known as ERBB2)-positive BC,
or in the absence of the three receptors, triple-negative BC (TNBC)
(2).
Breast-conserving therapy (BCT) includes a wide
local excision followed by adjuvant radiotherapy to the whole
breast, and frequently, an additional boost to the tumor bed,
including intraoperative radiotherapy (IORT) as one of the more
novel strategies (3–6). The rationale for local dose escalation
originates in the fact that after BCT, up to 90% of (at least
first) local recurrences in the breast occur in the same quadrant
as the primary cancer (7,8). The largest evidence for boost IORT
preceding whole breast irradiation exists for intraoperative
electron radiotherapy (IOERT) with single doses of ~10 Gy. In any
risk constellation, local recurrence rates are among the lowest
reported thus far, as well as those of long-term follow-up analyses
(9). Apart from the mere dose
augmentation effect and the high topographical precision in
delivery, immediate irradiation during surgery has been
hypothesized to exhibit an effect on the tumor microenvironment,
abrogating the proliferative cascade induced by surgical wound
healing (10–13). Published data have suggested that the
wound healing process subsequent to surgery alters the area
surrounding the original tumor and around the scar, and that the
modified microenvironment is more favorable for the tumor to recur.
Local recurrence after surgery is particularly common in tumors
characterized by HER2 overexpression (14). It has been shown that wound fluids
contain growth factors inducing the proliferation of HER2-positive
BCs (15). Radiotherapy is not the
only treatment that affects cell survival, surgery also has an
impact on the tumor microenvironment. Belletti et al
demonstrated the stimulatory effect of post-surgical drainage
fluids on BC cells in fluids harvested from a group of patients
after IORT treatment and from patients after breast-conserving
surgery. It was shown that wound fluids from conservative surgery
(without IORT) could stimulate the proliferation, migration and
invasion of the BC cell lines, while fluids collected after IORT
demonstrated different properties (16).
It has been proposed that cancer cells displaying
the stem-like phenotype play a critical role in local recurrence,
invasion and metastasis, as well as in radio- and chemoresistance
(17–21). Al-Hajj et al identified a
population of cluster of differentiation
(CD)44+/CD24−/low cells from human breast
tumors, which are more tumorigenic than other cell populations
(22). In vivo experiments
have shown that CD44+/CD24−/low cells were
able to generate tumors in NOD/SCID mice. Although a statistically
significant association between the clinical behavior and the
frequency of these cell populations was not observed, tumors with
distant metastases exhibited a higher fraction of the
CD44+/CD24−/low phenotype (23).
The presence of high aldehyde dehydrogenase 1
(ALDH1) activity is also associated with stem cell properties, with
resistance to chemotherapy and a worse prognosis (24–26).
Previous studies found that ALDH is involved in intracellular
retinoic acid production correlated with metastasis, tumor grade,
and HER2 and Ki-67 status (26–28).
Dysregulation of signal transducer and activator of transcription 3
(STAT3) is sufficient for neoplastic transformation, and a previous
study showed that constitutively active forms are able to promote
malignant transformation in fibroblasts and tumor formation in mice
(29). It has also been demonstrated
that ALDH+ and
ALDH+/CD44+/CD24− subpopulations
of BC cells express higher levels of phosphorylated STAT3 (30). The pharmacological targeting on STAT3
can suppress ALDH+ and
ALDH+/CD44+/CD24− cells in
vitro and in vivo.
The aim of the present study was to determine the
effect of surgical wound fluids from IOERT treatment (RT-WF)
compared with wound fluids from conservative-breast surgery only
(WF) on the CD44+/CD24−/low phenotype and
ALDH1 activity in a range of different BC cell lines. The results
obtained will enable a better understanding of the mechanism of
recurrence and metastasis following BC surgery.
Materials and methods
Surgical wound fluids
Post-operative wound fluids were collected from 44
female patients, who underwent surgery for BC in Greater Poland
Cancer Centre in Poznań, Poland. The mean age of the patients was
58 years and the age range was 38–76 years. Two groups were
analyzed. In the first group, following resection of the tumor
(quadrantectomy), the patients underwent IOERT with up to a dose of
10 Gy per tumor bed and surrounding tissues. In the second group,
the patients did not receive IOERT. In the two groups, the patients
left the ward on the second day after the surgery. The follow-up
examination was scheduled for 7 days post-surgery in the Hospital
Outpatient Clinic. The patients underwent ultrasonography and were
assessed for the presence of fluid in the tumor bed. If fluid was
found, it was collected for tests by means of percutaneous
aspiration. Fluids collected from the intraoperative group were
marked as RT-WF (22 samples), and fluids from the surgery alone
group were marked as WF (22 samples). Fluids were centrifuged for
25 min at 1,100 × g in 40°C, sterile filtered and stored at −80°C.
The present study was approved by the Bioethics Committee of Poznań
University of Medical Sciences (Poznań, Poland).
Cell culture
A total of 8 human BC cell lines were used:
MDA-MB-231 (ER/PR−; HER2/Neu−), MDA-MB-468
(ER/PR−; HER2/Neu−), BT-20
(ER/PR−; HER2/Neu−), BT-549
(ER/PR−; HER2/Neu−), defined as TNBC, SK-BR-3
(ER/PR−; HER2/Neu+), BT-474
(ER/PR+; HER2/Neu+), MCF7 (ER/PR+;
HER2/Neu−) and T47D (ER/PR+;
HER2/Neu−). All cell lines were obtained from the
American Type Culture Collection (ATCC; Manassas, VA, USA) and
cultured according to the ATCC instructions in a humidified
atmosphere with 5% carbon dioxide at 37°C. The BC cell lines were
chosen due to their distinct molecular profiles (31,32). At 24
h prior to the experiments, the cells were seeded in 6-cm Petri
dishes and cultured in standard medium overnight. Next, culture
medium was changed to fresh medium containing 10% RT-WF or 10% WF.
The cells were incubated for 4 days. A total of 22 samples of RT-WF
and WF, respectively, were analyzed. Control cells were cultured in
standard medium under the same conditions.
Flow cytometry
After 4 days of incubation, the cells were washed
twice with phosphate-buffered saline (PBS; Sigma-Aldrich, St.
Louis, MO, USA), detached using Accutase (Thermo Fisher Scientific
Inc., Waltham, MA, USA) and re-suspended in PBS supplemented with
1% bovine serum albumin (Thermo Fisher Scientific Inc.). Cell
density was calculated using a Moxi Z automated cell counter (Orflo
Technologies, Ketchum, ID, USA). In total, 1×106 cells
were used for the analysis. Combinations of fluorochrome-conjugated
mouse anti-human monoclonal antibodies CD44 (APC; dilution, 1:20;
catalog no. 559942), CD24 (PE; dilution, 1:20; catalog no. 555428)
and appropriate isotype controls were obtained from BD Biosciences
(Franklin Lakes, NJ, USA). The cells were incubated with the
antibodies at 4°C in the dark for 1 h. The labeled cells were
analyzed using FACS Aria (BD Biosciences).
Aldefluor assay
The ALDEFLUOR kit (Stemcell Technologies, Grenoble,
France) was used according to the manufacturer's protocol. Briefly,
the cells were washed twice with PBS (Sigma-Aldrich) and detached
using Accutase (Thermo Fisher Scientific, Inc.). Detached cells
were re-suspended in fresh medium and cell density was calculated
using a Moxi Z automated cell counter (Orflo Technologies). In
total, 2×105 cells were used for the analysis and
incubated in ALDEFLUOR assay buffer containing ALDH substrate for
45 min at 37°C. For each sample, negative controls were incubated
under the same conditions with diethylaminobenzaldehyde. The
labeled cells were analyzed using FACS Aria (BD Biosciences).
Statistical analysis
Data are expressed as the mean ± standard deviation.
Differences between two sample means were assessed using the
Student's t-test. P≤0.05 was considered to indicate a
statistically significant difference. Statistical tests were
performed using QuickCalcs, GraphPad online statistical calculator
(GraphPad, La Jolla, CA, USA
Results
Cell selection
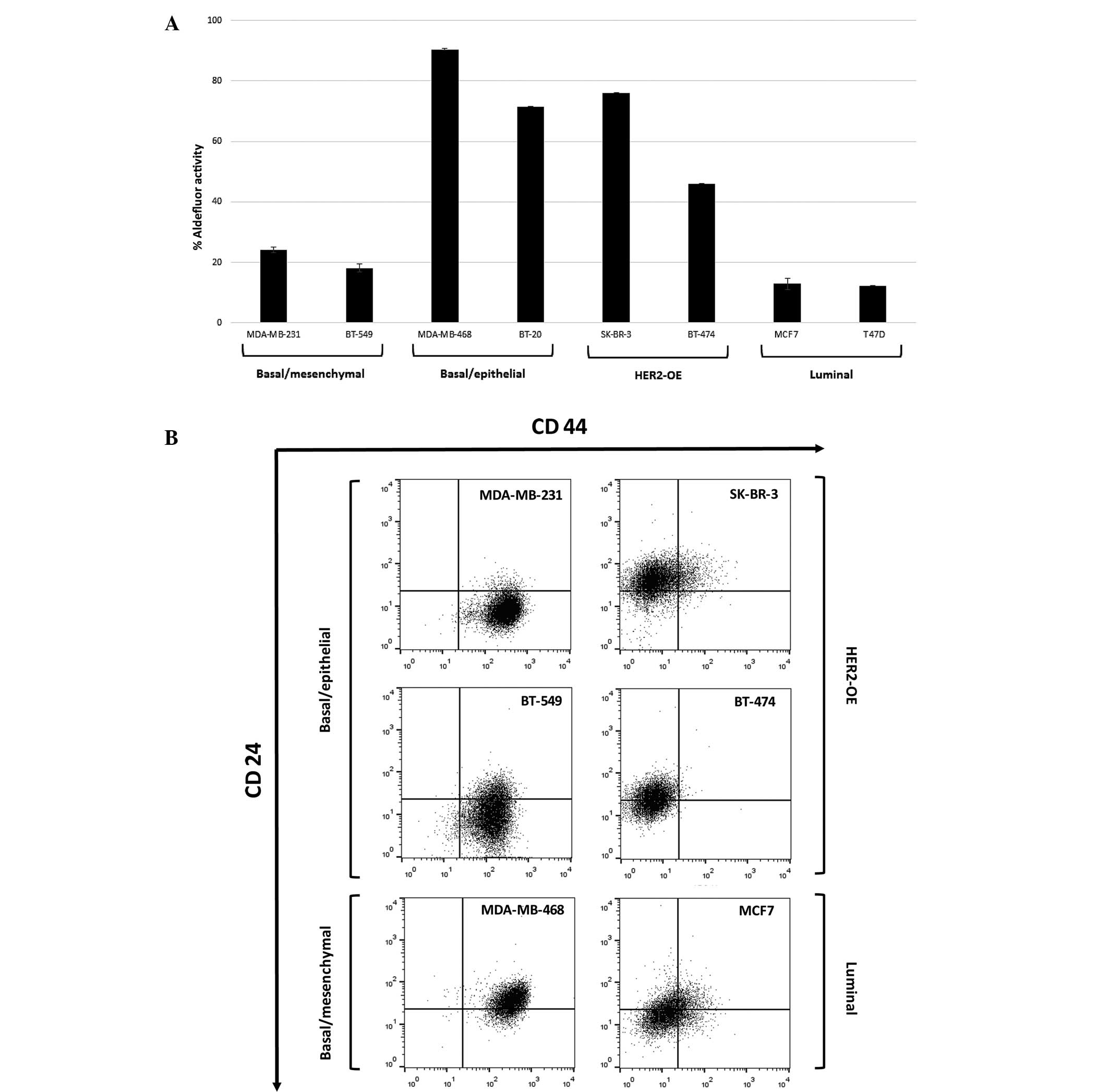
In total, 8 human BC cell lines were selected to be
examined due to their histopathological and molecular profiles.
Each cell line was characterized by different aldehyde
dehydrogenase 1 (ALDH1) activity and the expression of a
CD44+/CD24−/low subpopulation, even in cells
of the same cancer subtypes (Fig. 1).
The basal/epithelial (MDA-MB-468 and BT-20) and HER2-overexpressing
(HER2-OE; SK-BR-3 and BT-474) BC cell lines showed strong ALDH1
activity compared with the luminal (MCF7 and T47D) cell lines. Only
the basal type (MDA-MB-231 and BT-549) expressed a high percentage
of CD44-positive cells. All TNBC cell lines were characterized by a
high proportion of CD44+/CD24−/low
subpopulation cells compared with other cell lines.
Surgical wound fluids affect ALDH1
activity
ALDH1 activity was evaluated in the human BC cell
lines using the ALDEFLUOR assay. Fig.
2 shows the percentage of the cell population with ALDH1
activity in cells incubated with 10% conditioned medium that were
harvested after 4 days in standard conditions. In all cell lines,
with the exception of the BT-549 cell line (WF vs. RT-WF, P=0.029),
surgical wound fluids from both the conservative surgery and IORT
procedure groups induced ALDH1 activity compared with the control
group supplemented with 10% FBS. The MDA-MB-468 and MDA-MB-231 cell
lines demonstrated virtually no difference in ALDH1 activity
between the control group and the treated cells (MDA-MB-468: CTR
vs. WF, P=0.207; CTR vs. RT-WF, P=0.671; and WF vs. RT-WF, P=0.418;
MDA-MB231: CTR vs. WF, P=0.055; CTR vs. RT-WF, P=0.141; and WF vs.
RT-WF, P=0.651). Notably, WF demonstrated a stronger stimulating
effect compared with RT-WF in the luminal subtypes of cell lines
that were characterized by low ALDH1 activity in the control group
(MCF-7: CTR vs. WF, P=0.006; CTR vs. RT-WF, P=0.142; and WF vs.
RT-WF, P=0.045).
Surgical wound fluids affect the
CD44/CD24 phenotype
The surface expression of CD44 and CD24 was analyzed
in the human BC cell lines using flow cytometry. Regarding specific
molecular subtypes, the markers were differentially expressed.
Human BC cell lines after 4 days of incubation in 10% wound fluid
conditioned medium demonstrated an altered proportion of
CD44+/CD24−/low cell populations (described
as a BC stem cell marker). The results varied markedly between each
cell line, even between the same histological subtypes (Fig. 3). The TNBC MDA-MB-231 cell line did
not exhibit changes in the expression profile (CTR vs. WF, P=0.465;
CTR vs. RT-WF, P=0.262; and WF vs. RT-WF, P=0.092). Notably, other
TNBC cell lines, such as BT-549 and MDA-MB-468, demonstrated the
stimulatory effect of WF and the inhibitory effect of RT-WF
compared with the control group (BT-549: CTR vs. WF, P=0.017; CTR
vs. RT-WF, P=0.021; and WF vs. RT-WF, P=0.007; MDA-MB-468: CTR vs.
WF, P=0.001; CTR vs. RT-WF, P=0.159; and WF vs. RT-WF, P=0.017).
These three cell lines were defined as exhibiting a basal-like
phenotype and harbored more CD44+/CD24−/low
than non-TNBC cells. The SK-BR-3 cell line was constituted of low
levels of the CD44-positive cell population, however, unexpectedly,
the two types of post-operative fluids each had a significant
stimulating effect on the CD44+/CD24−/low
phenotype (CTR vs. WF, P=0.005; CTR vs. RT-WF, P=0.001; and WF vs.
RT-WF, P=0.074). The luminal MCF7 cell line was mainly constituted
by CD24-positive cells, nevertheless, the small population of
CD44+/CD24−/low cells decreased significantly
due to incubation with WF and RT-WF (CTR vs. WF, P=0.018; CTR vs.
RT-WF, P=0.006; and WF vs. RT-WF, P=0.680). BT-474 did not contain
a detectable CSC population in any variant.
The BT-20 cell line is mainly constituted by cells
with the CD44+/CD24+ non-invasive phenotype
and is not altered by incubation with surgical wound fluid (data
not shown). By contrast, the T47D cell line is shown to be enriched
with a CD44−/CD24+ cell population, which is
considered to be unable to give rise to the invasive phenotype. The
experiments were unable to identify how incubation with surgical
wound fluid affected the CD44/CD24 phenotype in T47D, which had a
high standard deviation and strong statistical insignificance (data
not shown). Since these data are derived from different patients
from the limited group, it was not possible to increase the
research panel and try to redefine the associations between the
cell line CD44/CD24 phenotype and the surgical wound fluids. For
this reason, the BT549, BT-20 and T47D cell lines are not
represented in certain cases, as the results were unreliable due to
extreme results. These data indicate that each surgical wound fluid
can affect the cell line biology individual.
Changes in all CD44 and CD24
expression variants
The impact of RT-WF and WF fluids on CD44 and CD24
(all expression variants) is presented in Fig. 4. In the basal-like cell lines, with
the exception of the MDA-MB-231 cell line, RT-WF decreased the
CD44+/CD24−/low population while stimulating
the CD44+/CD24+ population, representing a
non-invasive epithelial-like phenotype
(CD44+/CD24−/low BT-549: CTR vs. WF, P=
0.017; CTR vs. RT-WF, P=0.021; and WF vs RT-WF, P=0.007;
MDA-MB-468: CTR vs. WF, P=0.008; CTR vs. RT-WF, P=0.159; and WF vs.
RT-WF, P=0.017; CD44+/CD24+ BT-549: CTR vs.
WF, P=0.175; CTR vs. RT-WF, P=0.004; and WF vs. RT-WF, P=0.003;
MDA-MB-468: CTR vs. WF, P=0.009; CTR vs. RT-WF, P=0.085; and WF vs.
RT-WF, P=0.001). HER2-OE-positive cell lines and luminal lines
consist of the highest percentage of the
CD44−/CD24+ population, which is decreased by
WF. In the BT-474 cell lines, all surgical fluids stimulated a
CD44-positive and CD24-postive population, whereas in the SK-BR-3
and MCF7 cell lines they stimulated a negative phenotype in these
populations (BT-474 CD44+/CD24+: CTR vs. WF,
P=0.003; CTR vs. RT-WF, P=0.007; and WF vs. RT-WF, P=0.707; SK-BR-3
CD44−/CD24−: CTR vs. WF, P=0.042; CTR vs.
RT-WF, P=0.001; and WF vs. RT-WF, P=0.008; MCF-7
CD44−/CD24−: CTR vs. WF, P=0.005; CTR vs.
RT-WF, P=0.001, and WF vs. RT-WF, P=0.042). Luminal and HER2-OE BC
cell lines were constituted of cells with low levels of the
CD44-positive population.
Discussion
The present study demonstrated that post-operative
fluids harvested from patients who underwent breast-conserving
surgery alone and from patients who received IOERT affect the stem
cell phenotype in human BC cell lines. It is well established that
surgery modifies the microenvironment, and that primary tumor
removal may stimulate or accelerate metastatic spread. This
phenomenon is known as tumor cell dormancy (33) and is likely to be important in
treatment failure. Metastatic disease usually develops within 5
years of primary tumor treatment and more than half of patients
succumb due to it (34). The wound
healing process is a typical consequence of surgery, and it is
currently believed that accompanying inflammation may contribute to
aggressiveness and treatment resistance (35). The dormancy theory explains that
molecular events associated with healing play a pivotal role as a
‘start signal’ to proliferation and the stimulation of angiogenesis
(34). It has been shown that
post-surgery wound fluids taken from BC patients can stimulate
proliferation, metastasis and invasion (15,16). The
aforementioned results support the clinical observations and proves
that surgery is a perturbing factor and a cause of treatment
failure. Notably, the complete inhibition of proliferation and the
delayed occurrence of metastases has been achieved in murine
mammary studies using systemic treatment prior to or following
surgery (36).
Inflammatory factors and changes in the
microenvironment have been identified as modifying agents to tumor
stem cells (37). CSCs exhibit the
ability to self-renew, migrate and invade into surrounding tissues
or distant organs, and are associated with radio- and
chemoresistance. Due to these properties, CSCs have been proposed
as attractive targets and a number of studies have been conducted
to identify subpopulations of the cells responsible for treatment
failure and tumor progression. Breast CSCs were first described by
Al-Hajj et al (22) and
identified as a CD44+/CD24−/low high
tumorigenic population. In vivo experiments showed that
CD44+/CD24−/low cells were able to generate
tumors in NOD/SCID mice. Numerous other studies confirmed these
results in BC (23,38,39) and
various other human tumor types (40). Generally, tumorigenicity and the
stemness phenotype of these putative cells have been demonstrated
by in vitro clonogenicity and in vivo tumorigenicity.
A paradoxical phenomenon of tumor stem cells in BC exists, as there
is no statistically significant association in the clinical
behavior and the frequency of these cell populations (23,36),
however, tumors that develop distant metastases indeed exhibit a
higher fraction of CD44+/CD24−/low phenotype
cells (23,41).
In order to better understand the effect of surgical
wound fluids on the putative stem cell population in BC, 8
different cell lines were examined in the present study. All models
used in the study differed not only by the histological subtype,
but also by the expression of the CD44 and CD24 subpopulation
(Fig. 2). Basal-like cell lines
expressed more CD44+/CD24−/low population
cells as opposed to the luminal type, and according to literature
data and clinical observations, these cells are associated with a
worse prognosis (42). Belletti et
al (16) observed changes in the
proteomic profile between cells incubated in surgical fluids
harvested from patients who underwent surgery alone and from those
patients who received intraoperative radiotherapy. The fluids taken
from the patients that received intraoperative radiotherapy showed
reduced expression in several molecules linked to tumor growth and
motility, including HGF and leptin, which can explain the different
biological activities between the two groups of surgical fluids
(16). It was therefore reasonable to
hypothesize that surgical fluids can induce a putative stem cell
population. Indeed, post-operative fluids affect the population,
but those taken from patients treated using IORT (RT-WF) in the
present study decreased the population of
CD44+/CD24−/low cells in the basal and
luminal groups. The strongest effect was observed in the BT-549 and
MDA-MB-468 cell lines, whereas in HER-OE cell lines, identified as
poorly equipped with CD44+/CD24−/low, the
result was the opposite. In the SK-BR-3 and BT-474 cell lines, the
two surgical fluids were each able to stimulate the putative stem
population. No effect was observed in the MDA-MB-231 cell line. A
decrease in the CD44+/CD24−/low population
was compensated for by an increase in the
CD44+/CD24+ population, which is considered
to be not as tumorigenic (Fig.
4).
A study by Segatto et al largely explains how
the surgery-wound response can promote a stem-like phenotype in BC
cells via the STAT3 signaling pathway (37). A strong stimulation of the ability of
mammosphere formation by wound fluid sera was observed in all
examined cell lines. The presented results differed slightly. A
dependence in the surgical fluid response according to the receptor
expression in the cell line and the surgical fluid type used in the
examination was observed (WF or RT-WF). Most likely, this effect is
caused by the different times of fluid collection. In the present
study, WF and RT-WF were collected at 7 days post-surgery by
percutaneous aspiration, while in the aforementioned study
(37), fluids were collected from
drains at 24 h post-surgery. The difference in the time of
collection is crucial in fluids, particularly in the panel of
IORT-treated cell lines. Based on Belletti's results of the
molecular analysis and the knowledge of surgery-induced
inflammation (16), we believe that
during the 1 week of the healing process, a pool of various
molecules was accumulated that was responsible for the stronger
effect on the putative stem phenotype.
While the subpopulation of cells with
CD44+/CD24−/low expression has the highest
invasiveness and metastatic potential in BC, more and more studies
indicate that the CD44−/CD24+ population is a
better prognostic marker in BC (43).
The tissue microarray and histopathological analysis of patients'
tumor samples indicates that CD44−/CD24+
tumors have the worst prognosis in early invasive BC (43), and the tumor group exhibiting the
CD44+/CD24−/low phenotype is considered a
favorable prognostic subgroup in BC. Notably, in the present study,
in the HER-OE cell lines and the luminal MCF7 cell line, this
population was decreased by surgical fluids (Fig. 4). Meyer et al demonstrated that
CD24 expression is under dynamic regulation in vitro and
in vivo, and that the population of
CD44−/CD24+ cells can interconvert into
CD44+/CD24−/low cells and vice versa
(44). This phenomenon can be
explained as a consequence of loss of CD24 activity during tumor
development or treatment.
ALDH activity is also associated with the putative
stem cell phenotype. It was previously demonstrated that the
expression of ALDH1 in breast tumors was a good predictor of a poor
clinical outcome and this high activity was specific to the
stemness phenotype (24). In turn,
Zhong et al found that ALDH1 was not significantly
associated with conventional clinical features such as tumor size
or receptor expression, but was associated with breast tumor
recurrence (45).
The present study assessed the impact of
post-operative fluids on ALDH1 activity. A total of 8 cell lines
were used with varied ALDH1 expression and activity that was
comparable within the histological subtypes (Fig. 1A). to the best of our knowledge, the
study presents the first examination of ALDH1 activity in BC
affected by post-operative surgical fluids. Surgical fluids
stimulated ALDH1 activity in all cell lines. However, RT-WF
demonstrated a less stimulatory effect, which was most noticeable
in the cell lines with a moderate ALDH1 level. Basal-like features
are much more frequently associated with the incidence of
metastasis than other subtypes. The present results showed that, as
in the CD44/CD24 phenotype investigation, in this group of tumors,
RT-WF inhibited the stimulation potential of fluids after surgery.
Therefore, IORT may essentially contribute to treatment
success.
The study did not observe that the examined putative
breast CSC markers of a CD44+/CD24−/low
phenotype and high ALDH1 activity result in the same response under
post-operative surgical fluids, indicating that in vitro
these markers do not correlate with the fluid response, and that
behavior is an independent factor, subsidiary to the
histopathological subtype. These results may be an explanation for
the lower relapse rates in the TARGIT-A trial for patients treated
with immediate IORT using 50-kV orthovoltage (46).
The present study supports the hypothesis that
surgery is a perturbing factor and explains how surgical
intervention can impact the critical CSC behavior. To the best of
our knowledge, this is the first study describing inhibitive
mechanisms for IOERT. With respect to histological phenotype, the
effect of the treatment on tumor progression, either local or
systemic, strongly suggests a requirement for further research and
clinical validation.
In summary, surgical wound fluids from the WF and
RT-WF groups affected the putative stem cell phenotype, as
determined by CD44+/CD24−/low and high ALDH1
activity. Following IOERT, a lower stimulation stem cell phenotype
was observed in the RT-WF compared with the WF.
Acknowledgements
The present study was supported by the National
Science Center, Kraków, Poland (grant no. UMO-2013/09/N/NZ4/02844).
The authors would like to thank Professor Felix Sedlmayer from the
University Clinic for Radiotherapy and Radio-Oncology (Salzburg,
Austria) for providing editorial support and interactive
communication.
Glossary
Abbreviations
Abbreviations:
|
BCT
|
breast-conserving therapy
|
|
IORT
|
intraoperative radiotherapy
|
|
IOERT
|
intraoperative electron
radiotherapy
|
|
WF
|
wound fluids from surgery only
|
|
RT-WF
|
intraoperative radiotherapy wound
fluids
|
References
|
1
|
Campbell LL and Polyak K: Breast tumor
heterogeneity: Cancer stem cells or clonal evolution? Cell Cycle.
6:2332–2338. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cancer Genome Atlas Network, .
Comprehensive molecular portraits of human breast tumours. Nature.
490:61–70. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bitterman A, Kessner R, Goldman I, Shiloni
E and Steiner M: Intraoperative radiotherapy for breast cancer. Isr
Med Assoc J. 14:256–259. 2012.PubMed/NCBI
|
|
4
|
Murawa P, Murawa D, Adamczyk B and Połom
K: Breast cancer: Actual methods of treatment and future trends.
Rep Pract Oncol Radiother. 19:165–172. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Williams NR, Pigott KH and Keshtgar MR:
Intraoperative radiotherapy in the treatment of breast cancer: A
review of the evidence. Int J Breast Cancer. 2011:3751702011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sedlmayer F, Reitsamer R, Fussl C, Ziegler
I, Zehentmayr F, Deutschmann H, Kopp P and Fastner G: Boost IORT in
breast cancer: Body of evidence. Int J Breast Cancer.
2014:4725162014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liberman L, Van Zee KJ, Dershaw DD, Morris
EA, Abramson AF and Samli B: Mammographic features of local
recurrence in women who have undergone breast-conserving therapy
for ductal carcinoma in situ. AJR Am J Roentgenol. 168:489–493.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fisher B, Dignam J, Wolmark N, Mamounas E,
Costantino J, Poller W, Fisher ER, Wickerham DL, Deutsch M,
Margolese R, et al: Lumpectomy and radiation therapy for the
treatment of intraductal breast cancer: Findings from national
surgical adjuvant breast and bowel project B-17. J Clin Oncol.
16:441–452. 1998.PubMed/NCBI
|
|
9
|
Fastner G, Sedlmayer F, Merz F,
Deutschmann H, Reitsamer R, Menzel C, Stierle C, Farmini A, Fischer
T, Ciabattoni A, et al: IORT with electrons as boost strategy
during breast conserving therapy in limited stage breast cancer:
Long term results of an ISIORT pooled analysis. Radiother Oncol.
108:279–286. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Demicheli R, Valagussa P and Bonadonna G:
Does surgery modify growth kinetics of breast cancer
micrometastases? Br J Cancer. 85:490–492. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Baum M, Demicheli R, Hurshesky W and
Retsky M: Does surgery unfavorable perturb the ‘natural history’ of
early breast cancer by accelerating the appearance of distant
metastases? Eur J Cancer. 41:508–515. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fisher B, Gunduz N, Coyle J, Rudock C and
Saffer E: Presence of growth-stimulating factor in serum following
primary tumor removal in mice. Cancer Res. 49:1996–2001.
1989.PubMed/NCBI
|
|
13
|
Tsuchida Y, Sawada S, Yoshioka I, Ohashi
Y, Matsuo M, Harimaya Y, Tsukada K and Saiki I: Increased surgical
stress promotes tumor metastasis. Surgery. 133:547–555. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ménard S, Balsari A, Casalini P, Tagliabue
E, Campiglio M, Bufalino R and Cascinelli N: HER-2 positive breast
carcinomas as a particular subset with peculiar clinical behaviors.
Clin Canc Res. 8:520–525. 2002.
|
|
15
|
Tagliabue E, Agresti R, Carcangiu ML,
Ghirelli C, Morelli D, Campiglio M, Martel M, Giovanazzi R, Greco
M, Balsari A and Ménard S: Role of HER2 in wound-induced breast
carcinoma proliferation. Lancet. 362:527–533. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Belletti B, Vaidya JS, D'Andrea S,
Entschladen F, Roncadin M, Lovat F, Berton S, Perin T, Candiani E,
Reccanello S, et al: Targeted intraoperative radiotherapy impairs
the stimulation of breast cancer cell proliferation and invasion
caused by surgical wounding. Clin Cancer Res. 14:1325–1332. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dalerba P, Cho RW and Clarke MF: Cancer
stem cells: Models and concepts. Annu Rev Med. 58:267–284. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Visvader JE and Lindeman GJ: Cancer stem
cells in solid tumors: Accumulating evidence and unresolved
questions. Nat Rev Cancer. 8:755–768. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dean M, Fojo T and Bates S: Tumor stem
cells and drug resistance. Nat Rev Cancer. 5:275–284. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Brunner TB, Kunz-Schughart LA,
Grosse-Gehling P and Baumann M: Cancer stem cells as a predictive
factor in radiotherapy. Semin Radiat Oncol. 22:151–174. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bapat SA, Mali AM, Koppikar CB and Kurrey
NK: Stem and progenitor-like cells contribute to the aggressive
behavior of human epithelial ovarian cancer. Cancer Res.
65:3025–3029. 2005.PubMed/NCBI
|
|
22
|
Al-Hajj M, Wicha MS, Benito-Hernandez A,
Morrison SJ and Clarke MF: Prospective identification of
tumorigenic breast cancer cells. Proc Natl Acad Sci USA.
100:3983–3988. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Abraham BK, Fritz P, McClellan M,
Hauptvogel P, Athelogou M and Brauch H: Prevalence of
CD44+/CD24−/low cells in breast cancer may
not be associated with clinical outcome but may favor distant
metastasis. Clin Cancer Res. 11:1154–1159. 2005.PubMed/NCBI
|
|
24
|
Ginestier C, Hur MH, Charafe-Jauffret E,
Monville F, Dutcher J, Brown M, Jacquemier J, Viens P, Kleer CG,
Liu S, et al: ALDH is a marker of normal and malignant human
mammary stem cells and a predictor of poor clinical outcome. Cell
Stem Cell. 1:555–567. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tanei T, Morimoto K, Shimazu K, Kim SJ,
Tanji Y, Taguchi T, Tamaki Y and Noguchi S: Association of breast
cancer stem cells identified by aldehyde dehydrogenase 1 expression
with resistance to sequential paclitaxel and epirubicin-based
chemotherapy for breast cancers. Clin Cancer Res. 15:4234–4241.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Croker AK, Goodale D, Chu J, Postenka C,
Hedley BD, Hess DA and Allan AL: High aldehyde dehydrogenase and
expression of cancer stem cell markers selects for breast cancer
cells with enhanced malignant and metastatic ability. J Cell Mol
Med. 13:2236–2252. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Marcato P, Dean CA, Giacomantonio CA and
Lee PW: Aldehyde dehydrogenase: Its role as a cancer stem cell
marker comes down to the specific isoform. Cell Cycle.
10:1378–1384. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Park SY, Lee HE, Li H, Shipitsin M, Gelman
R and Polyak K: Heterogeneity of stem-cell related markers
according to tumor subtype and histologic stage in breast cancer.
Clin Cancer Res. 16:876–887. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bromberg JF, Wrzeszczynska MH, Devgan G,
Zhao Y, Pestell RG, Albanese C and Darnell JE Jr: STAT3 as an
oncogene. Cell. 98:295–303. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lin L, Hutzen B, Lee HF, Peng Z, Wang W,
Zhao C, Lin HJ, Sun D, Li PK, Li C, et al: Evaluation of STAT3
signaling in ALDH+ and
ALDH+/CD44+/CD24− subpopulations
of breast cancer cells. PLoS One. 8:e828212013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Holliday DL and Speirs V: Choosing the
right cell line for breast cancer research. Breast Cancer Res.
13:2152011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Neve RM, Chin K, Fridlyand J, Yeh J,
Baehner FL, Fevr T, Clark L, Bayani N, Coppe JP, Tong F, et al: A
collection of breast cancer cell lines for the study of
functionally distinct cancer subtypes. Cancer Cell. 10:515–527.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Demicheli R, Retsky MW, Hrushesky WJ and
Baum M: Tumor dormancy and surgery-driven interruption of dormancy
in breast cancer: Learning from failures. Nat Clin Pract Oncol.
4:699–710. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Marches R, Scheuermann R and Uhr J: Cancer
dormancy: From mice to man. Cell Cycle. 5:1772–1778. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Arnold KM, Opdenaker LM, Flynn D and
Sims-Mourtada J: Wound healing and cancer stem cells: Inflammation
as a driver of treatment resistance in breast cancer. Cancer Growth
Metastasis. 8:1–13. 2015.PubMed/NCBI
|
|
36
|
Fisher B, Gunduz N and Saffer EA:
Influence of the interval between primary tumor removal and
chemotherapy on kinetics and growth of metastases. Cancer Res.
43:1488–1492. 1983.PubMed/NCBI
|
|
37
|
Segatto I, Berton S, Sonego M, Massarut S,
Perin T, Piccoli E, Colombatti A, Vecchione A, Baldassarre G and
Belletti B: Surgery-induced wound response promotes stem-like and
tumor-initiating features of breast cancer cells, via STAT3
signaling. Oncotarget. 5:6267–6279. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ma F, Li H, Wang H, Shi X, Fan Y, Ding X,
Lin C, Zhan Q, Qian H and Xu B: Enriched CD44(+)/CD24(−) population
drives the aggressive phenotypes presented in triple-negative
breast cancer (TNBC). Cancer Lett. 353:153–159. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Camerlingo R, Ferraro GA, De Francesco F,
Romano M, Nicoletti G, Di Bonito M, Rinaldo M, D'Andrea F and
Pirozzi G: The role of CD44+/CD24−/low
biomarker for screening, diagnosis and monitoring of breast cancer.
Oncol Rep. 31:1127–1132. 2014.PubMed/NCBI
|
|
40
|
Shipitsin M, Campbell LL, Argani P,
Weremowicz S, Bloushtain-Qimron N, Yao J, Nikolskaya T,
Serebryiskaya T, Beroukhim R, Hu M, et al: Molecular definition of
breast tumor heterogeneity. Cancer Cell. 11:259–273. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sheridan C, Kishimoto H, Fuchs RK,
Mehrotra S, Bhat-Nakshatri P, Turner CH, Goulet R Jr, Badve S and
Nakshatri H: CD44+/CD24− breast cancer cells
exhibit enhanced invasive properties: An early step necessary for
metastasis. Breast Cancer Res. 8:R592006. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Idowu MO, Kmieciak M, Dumur C, Burton RS,
Grimes MM, Powers CN and Manjili MH: CD44(+)/CD24(−/low) cancer
stem/progenitor cells are more abundant in triple-negative invasive
breast carcinoma phenotype and are associated with poor outcome.
Hum Pathol. 43:364–373. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ahmed MA, Aleskandarany MA, Rakha EA,
Moustafa RZ, Benhasouna A, Nolan C, Green AR, Ilyas M and Ellis IO:
A CD44−/CD24+ phenotype is a poor prognostic
marker in early invasive breast cancer. Breast Cancer Res Treat.
133:979–995. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Meyer MJ, Fleming JM, Ali MA, Pesesky MW,
Ginsburg E and Vonderhaar BK: Dynamic regulation of CD24 and the
invasive, CD44posCD24neg phenotype in breast cancer cell lines.
Breast Cancer Res. 11:R822009. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhong Y, Lin Y, Shen S, Zhou Y, Mao F,
Guan J and Sun Q: Expression of ALDH1 in breast invasive ductal
carcinoma: An independent predictor of early tumor relapse. Cancer
Cell Int. 13:602013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Vaidya JS, Wenz F, Max Bulsara M, Tobias
JS, Joseph DJ, Keshtgar M, Flyger HL, Massarut S, Alvarado M,
Saunders C, et al: Risk-adapted targeted intraoperative
radiotherapy versus whole-breast radiotherapy for breast cancer:
5-year results for local control and overall survival from the
TARGIT-A randomised trial. Lancet. 383:603–613. 2014. View Article : Google Scholar : PubMed/NCBI
|