Introduction
Pancreatic ductal adenocarcinoma (PDAC) is a fatal
cancer with an overall 5-year survival rate of <5%. Surgical
treatment has the most favorable outcome, with a 5-year survival
rate of ~20%; however, only 15–20% of patients are candidates for
surgical resection (1,2). Standard treatment modalities, including
chemotherapy and chemoradiotherapy, have been shown to be
ineffective for improving survival in patients with pancreatic
cancer (1,2). Therefore, novel treatments are urgently
required for this devastating disease.
Lymph node metastasis, a high tumor grade, a large
tumor size, lymphovascular invasion, perineural invasion, a high
level of preoperative cancer antigen (CA) 19–9, persistently
elevated postoperative levels of CA 19–9 and positive margins of
resection are typically considered the main prognostic factors for
PDAC (2–5). In addition to clinicopathological
features, the tumor-specific host immune response has been reported
to have a crucial role in disease-related survival outcomes for
numerous types of cancers (6–15). Among the parameters representing
tumor-specific immune function, tumor infiltrating lymphocytes
(TILs) are often observed in resected cancer tissue and are thought
to participate in the host immune response against cancer (16). Interactions between the tumor
microenvironment and the immune system significantly affect cancer
development and progression (17).
TILs are considered prognostic factors because they represent local
host antitumor immunity (16,17).
TILs consist of functionally distinct subsets,
including the antitumor effectors, CD8+ T lymphocytes
and CD4+ helper T lymphocytes, which are associated with
a favorable prognosis (7).
Conversely, regulatory T lymphocytes (Tregs) suppress the antitumor
immune response and have been shown to adversely affect patient
survival (6,9,13,14,18. The
forkhead/winged helix transcription factor, forkhead box P3
(Foxp3), which is genetically defective in an autoimmune and
inflammatory syndrome in humans and mice, is specifically expressed
in naturally arising CD4+ Tregs (19). Tregs weaken host antitumor immunity by
suppressing T-cell proliferation, antigen presentation and cytokine
production (20).
A subset of TILs has been identified in PDAC
(21); however, the relationship
between the TILs and patient prognosis is largely unexplored. To
evaluate the prognostic value of TILs in PDAC, the present study
constrained the investigation to left-sided PDAC, as some cases of
cancer of the pancreatic head cannot be differentiated from distal
bile duct, ampulla of Vater or duodenal cancers. The present study
aimed to evaluate the association between TILs in surgically
resected left-sided PDAC and patient outcomes.
Materials and methods
Patients
To avoid potential contamination with other
periampullary cancers, such as distal bile duct, ampulla of Vater
and duodenal cancers, only left-sided pancreatic cancers were
considered. A total of 30 patients who underwent a curative distal
pancreatectomy due to left-sided PDAC at Severance Hospital, Yonsei
University College of Medicine (Seoul, Korea) between January 2000
and December 2008 were enrolled in the present study. In addition,
paraffin-embedded tissue blocks from the patients were included in
the TIL analysis. The present study retrospectively analyzed
patient demographics, histopathological findings and survival
outcomes. Follow-up was completed on May 30, 2012. Patients who
received neoadjuvant chemotherapy or chemoradiotherapy, or had
another primary tumor, were excluded from the study. Overall
survival (OS) time was defined as the interval between surgery and
death, or between surgery and the last observation of surviving
patients. The disease-free survival (DFS) time was defined as the
interval between surgery and recurrence. Data were censored at the
last follow-up for living patients. This study was approved by the
Institutional Review Board of Severance Hospital, Yonsei University
college of Medicine.
Immunohistochemical (IHC) staining and
quantification of TIL subsets
IHC staining for TILs was performed as described
previously (11). Briefly,
paraffin-embedded PDAC tissue sections at a thickness of 4-µm were
deparaffinized in xylene and rehydrated in decreasing
concentrations of ethanol. Antigen retrieval was performed in
citrate buffer in a microwave oven. Endogenous peroxidase activity
was blocked by incubating the tissues with 3% hydrogen peroxide in
methanol for 5 min. The sections were then incubated for 60 min at
room temperature with primary monoclonal antibodies against cluster
of differentiation (CD)3 (cat. no. RM-9107-S; 1:100; Lab Vision
Corporation, Fremont, CA, USA), CD4 (cat. no. NCL-L-CD4-1F6; 1:100;
Novocastra™ Primary Antibodies; Leica Microsystems, Ltd., Milton
Keynes, UK), CD8 (cat. no. IS62330; 1:100; Dako, Glostrup,
Denmark), Foxp3 (cat. no. ab20034; 1:100; Abcam, Cambridge, UK),
and granzyme B (cat. no. MS-1157-S;1:100; Lab Vision Corporation),
which were used to identify total numbers of T lymphocytes, helper
T lymphocytes, cytotoxic T lymphocytes (CTLs), Tregs and activated
CTLs, respectively. After washing the sections twice with 0.05
mol/l Tris-buffered saline containing 0.2% Tween-20, the sections
were incubated with horseradish peroxidase-conjugated secondary
antibody (cat. no. K5007; ready to use; Dako EnVision®
Detection system; Dako), followed by development with
diaminobenzidine and counterstaining with hematoxylin. Normal human
tonsil tissue obtained from a healthy volunteer was used as the
positive control. The negative control for immunostaining was
prepared by incubating tissue sections without primary antibody,
according to a previous study (11).
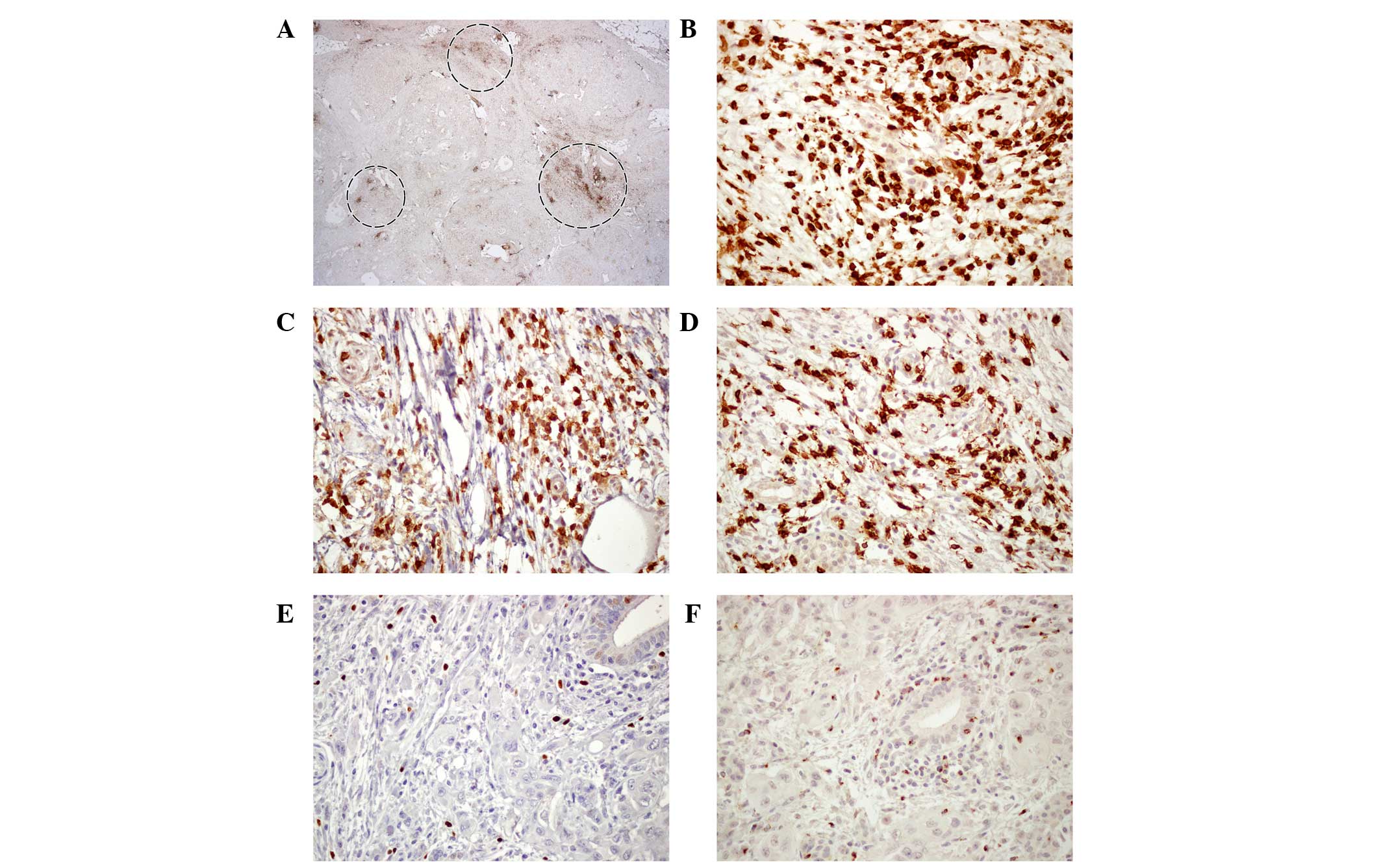
IHC staining was quantified by two experienced
pathologists who were blinded to the patient data. Three intense
foci of staining in the tumor sections were selected and four
high-power fields (magnification, ×400) from each slide were
selected for calculation of the IHC staining results. Fields with
necrosis or hemorrhage in the tumor portion were avoided. The
median value of positively stained cells in each part was recorded.
Using the absolute counts and relative ratios of lymphocytes
stained by each antibody (CD3, CD4, CD8, Foxp3 and granzyme B;
Fig. 1), the patients were divided
into low and high groups.
Statistical analysis
All statistical analyses were performed with SPSS
20.0 software (IBM SPSS, Armonk, NY, USA). Categorical data were
compared using χ2 or Fisher's exact tests. Absolute
counts of TIL subsets and the relative ratios between two different
TIL subsets were dichotomized in the survival analysis using
cut-off values derived by the median, as described previously
(6,10,11,22). OS
and DFS times were calculated using the Kaplan-Meier method and
significance was evaluated using the log-rank test. Cox
proportional hazard models were used for univariate and
multivariate survival analysis. P<0.05 was considered to
indicate a statistical significance.
Results
Patient demographics
A total of 54 patients underwent curative distal
pancreatectomy with or without splenectomy for left-sided PDAC.
Among them, 7 patients who underwent neoadjuvant chemoradiotherapy
were excluded. Paraffin-embedded tissue blocks were not available
for 9 patients and the qualities of the paraffin-embedded tissue
blocks were not good for 8 patients. Therefore, 30 patients were
enrolled in this study. The mean age of the enrolled patients was
62.4±8.9 years and 21 patients (70%) were male. The mean operation
time was 327±190 min. Combined organ resection was performed in 8
patients (26.7%), and an intraoperative transfusion was required in
9 patients (30%). The mean tumor size was 3.9±1.5 cm. The
pathological T stage was T2 in 3 patients (10%), T3 in 25 patients
(83.3%) and T4 in 2 patients (6.7%); the pathological N1 stage was
observed in 13 patients (43.3%). Lymphovascular invasion and
perineural invasion were observed in 8 patients (26.7%) and 11
patients (36.7%), respectively. In terms of tumor differentiation,
there were 7 well-differentiated, 20 moderately-differentiated and
2 poorly-differentiated tumors, as well as 1 case of an
undifferentiated tumor. Resection margin status was R0 in 27
patients, R1 in 1 patient and R2 in 2 patients. The median duration
of follow-up was 23 months (range, 5–94 months).
Survival outcomes
Table I shows survival
outcomes based on a univariate analysis according to the
clinicopathological parameters and operative findings. No factors
were significantly predictive of DFS or OS. However, low levels of
preoperative CA 19–9 were associated with a longer OS, with a
marginal statistical significance (37 vs. 18 months; P=0.061).
 | Table I.Univariate survival analysis
according to clinicopathological and operative findings. |
Table I.
Univariate survival analysis
according to clinicopathological and operative findings.
|
| Disease-free
survival | Overall
survival |
|---|
|
|
|
|
|---|
| Characteristic | Months
(median) | P-value | Months
(median) | P-value |
|---|
| Age, years |
| 0.273 |
| 0.261 |
| <59
(n=13) | 11 |
| 18 |
|
| ≥59
(n=17) | 12 |
| 29 |
|
| Gender |
| 0.483 |
| 0.419 |
| Male
(n=21) | 12 |
| 22 |
|
| Female
(n=9) | 10 |
| 23 |
|
| CA 19-9,
U/mla |
| 0.152 |
| 0.061 |
| ≤109
(n=15) | 13 |
| 37 |
|
| >109
(n=14) | 7 |
| 18 |
|
| Tumor size, cm |
| 0.404 |
| 0.467 |
| <3.5
(n=15) | 12 |
| 35 |
|
| ≥3.5
(n=15) | 8 |
| 18 |
|
| N stage |
| 0.219 |
| 0.137 |
| N0
(n=17) | 12 |
| 35 |
|
| N1
(n-13) | 8 |
| 18 |
|
| Combined organ
resection |
| 0.100 |
| 0.480 |
| No
(n=22) | 12 |
| 25 |
|
| Yes
(n=8) | 7 |
| 20 |
|
|
Differentiation |
| 0.178 |
| 0.219 |
| Well
(n=7) | 25 |
| 37 |
|
|
Moderate (n=20) | 10 |
| 20 |
|
| Poor
(n=2) | 3 |
| 9 |
|
|
Undifferentiated (n=1) | 7 |
| 21 |
|
| Lymphovascular
invasionb |
| 0.799 |
| 0.685 |
| No
(n=20) | 11 |
| 22 |
|
| Yes
(n=8) | 7 |
| 25 |
|
| Perineural
invasionb |
| 0.682 |
| 0.438 |
| No
(n=17) | 12 |
| 20 |
|
| Yes
(n=11) | 10 |
| 25 |
|
| Transfusion |
| 0.084 |
| 0.091 |
| No
(n=21) | 12 |
| 35 |
|
| Yes
(n=9) | 7 |
| 18 |
|
Table II shows
survival outcomes based on the univariate analysis according to the
TIL subsets. High levels of granzyme B+ TILs were
significantly related to a longer DFS time (25 vs. 10 months;
P=0.023), and a low Foxp3+/granzyme B+ ratio
was significantly associated with a favorable DFS time (25 vs. 8
months; P=0.008) and OS (47 vs. 17 months; P=0.003). High levels of
CD4+ were marginally related to good DFS (25 vs. 8
months; P=0.063). In the multivariate survival analysis, the ratio
of Foxp3+/granzyme B+ was an independent
prognostic factor for determining DFS [Exp(B), 3.060; 95%
confidence interval (CI), 1.259–7.436; P=0.014) and OS [Exp(B),
3.580; 95% CI, 1.460–8.780; P=0.005) (Table III and Fig. 2).
| Table II.Univariate survival analysis
according to TIL subset counts. |
Table II.
Univariate survival analysis
according to TIL subset counts.
|
| Disease-free
survival | Overall
survival |
|---|
|
|
|
|
|---|
| TIL subset | Months
(median) | P-value | Months
(median) | P-value |
|---|
| Absolute count |
|
|
|
|
|
CD3+ |
| 0.290 |
| 0.643 |
|
Low (<256,
n=15) | 11 |
| 21 |
|
|
High (≥256,
n=15) | 13 |
| 25 |
|
|
CD4+ |
| 0.063 |
| 0.164 |
|
Low (<160,
n=15) | 8 |
| 18 |
|
|
High (≥160,
n=15) | 25 |
| 37 |
|
|
CD8+ |
| 0.116 |
| 0.208 |
|
Low (<115,
n=15) | 8 |
| 18 |
|
|
High (≥115,
n=15) | 13 |
| 35 |
|
|
Granzyme B+ |
| 0.023a |
| 0.084 |
|
Low (<24,
n=15) | 10 |
| 18 |
|
|
High (≥24,
n=15) | 25 |
| 37 |
|
|
Foxp3+ |
| 0.538 |
| 0.603 |
|
Low (<28,
n=15) | 12 |
| 22 |
|
|
High (≥28,
n=15) | 10 |
| 23 |
|
| Relative ratio |
|
|
|
|
|
Foxp3+/CD3+ |
| 0.408 |
| 0.421 |
|
Low (<0.111,
n=15) | 13 |
| 29 |
|
|
High (≥0.111,
n=15) | 10 |
| 20 |
|
|
Foxp3+/CD4+ |
| 0.104 |
| 0.094 |
|
Low (<0.169,
n=15) | 14 |
| 37 |
|
|
High (≥0.169,
n=15) | 10 |
| 18 |
|
|
Foxp3+/CD8+ |
| 0.173 |
| 0.124 |
|
Low (<0.026,
n=15) | 13 |
| 37 |
|
|
High (≥0.026,
n=15) | 10 |
| 18 |
|
|
Foxp3+/granzyme
B+ |
| 0.008a |
| 0.003a |
|
Low (<0.110,
n=15) | 25 |
| 47 |
|
|
High (≥0.110,
n=15) | 8 |
| 17 |
|
| Table III.Multivariate survival analysis
according to TIL subset counts. |
Table III.
Multivariate survival analysis
according to TIL subset counts.
|
| Disease-free
survival | Overall
survival |
|---|
|
|
|
|
|---|
| TIL | Exp(B) | 95% CI | P-value | Exp(B) | 95% CI | P-value |
|---|
| CD4+
(low vs. high) | 1.738 | 0.725–4.167 | 0.215 | 1.617 | 0.684–3.825 | 0.273 |
| Granzyme
B+ (low vs. high) | 1.405 | 0.485–4.068 | 0.531 | 0.979 | 0.331–2.895 | 0.970 |
|
Foxp3+/granzyme B+
(high vs. low) | 3.060 | 1.259–7.436 | 0.014a | 3.580 | 1.460–8.780 | 0.005a |
Association between TIL subsets and
clinicopathological factors
Among the clinicopathological factors, age, gender,
tumor size, pathological nodal stage, combined organ resection,
lymphovascular invasion, perineural invasion and transfusion were
not associated with TIL subsets (CD4+, granzyme
B+ and Foxp3+/granzyme B+).
However, low levels of CA 19–9 were significantly associated with a
low Foxp3+/granzyme B+ ratio (P=0.016;
Table IV).
| Table IV.Association between
tumor-infiltrating lymphocyte subsets and clinicopathological
factors. |
Table IV.
Association between
tumor-infiltrating lymphocyte subsets and clinicopathological
factors.
|
|
CD4+ | Granzyme
B+ |
Foxp3+/granzyme
B+ |
|---|
|
|
|
|
|
|---|
| Characteristic | Low | High | P-value | Low | High | P-value | Low | High | P-value |
|---|
| Age, years |
|
| 0.713 |
|
| 0.269 |
|
| 0.713 |
| <59
(n=13) | 6 (40.0) | 7 (46.7) |
| 8 (53.3) | 5 (33.3) |
| 7 (46.7) | 6 (40.0) |
|
| ≥59
(n=17) | 9 (60.0) | 8 (53.3) |
| 7 (46.7) | 10 (66.7) |
| 8 (53.3) | 9 (60.0) |
|
| Gender |
|
| 0.427 |
|
| 0.427 |
|
| 1.000 |
| Male
(n=21) | 9 (60.0) | 12 (80.0) |
| 9 (60.0) | 12 (80) |
| 10 (66.7) | 11 (73.3) |
|
| Female
(n=9) | 6 (40.0) | 3 (20.0) |
| 6 (40.0) | 3 (20) |
| 5 (33.3%) | 4 (26.7) |
|
| Tumor size, cm |
|
| 0.715 |
|
| 0.715 |
|
| 0.715 |
| <3.5
(n=15) | 8 (53.3) | 7 (46.7) |
| 7 (46.7) | 8 (53.3) |
| 8 (53.3) | 7 (46.7) |
|
| ≥3.5
(n=15) | 7 (46.7) | 8 (53.3) |
| 8 (53.3) | 7 (46.7) |
| 7 (46.7) | 8 (53.3) |
|
| Nodal stage |
|
| 0.713 |
|
| 0.713 |
|
| 0.269 |
| N0
(n=17) | 8 (53.3) | 9 (60.0) |
| 8 (53.3) | 9 (60.0) |
| 10 (66.7) | 7 (46.7) |
|
| N1
(n=13) | 7 (46.7) | 6 (40.0) |
| 7 (46.7) | 6 (40.0) |
| 5 (33.3) | 8 (53.3) |
|
| Combined
resection |
|
| 1.000 |
|
| 1.000 |
|
| 0.682 |
| No
(n=22) | 11 (73.3) | 11 (73.3) |
| 11 (73.3) | 11 (73.3) |
| 12 (80.0) | 10 (66.7) |
|
| Yes
(n=8) | 4 (26.7) | 4 (26.7) |
| 4 (26.7) | 4 (26.7) |
| 3 (20.0) | 5 (33.3) |
|
| Lymphovascular
invasionb |
|
| 0.678 |
|
| 1.000 |
|
| 1.000 |
| No
(n=20) | 11 (78.6) | 9 (64.3) |
| 11 (73.3) | 9 (69.2) |
| 9 (69.2) | 11 (73.3) |
|
| Yes
(n=8) | 3 (21.4) | 5 (35.7) |
| 4 (26.7) | 4 (46.2) |
| 4 (30.8) | 4 (26.7) |
|
| Perineural
invasionb |
|
| 0.699 |
|
| 0.488 |
|
| 0.934 |
| No
(n=17) | 8 (57.1) | 9 (64.3) |
| 10 (66.7) | 7 (53.3) |
| 8 (61.5) | 9 (60.0) |
|
| Yes
(n=11) | 6 (42.9) | 5 (35.7) |
| 5 (33.3) | 6 (46.2) |
| 5 (38.5) | 6 (40.0) |
|
| Transfusion |
|
| 1.000 |
|
| 1.000 |
|
| 1.000 |
| No
(n=21) | 11 (73.3) | 10 (66.7) |
| 11 (73.3) | 10 (66.7) |
| 11 (73.3) | 10 (66.7) |
|
| Yes
(n=9) | 4 (26.7) | 5 (33.3) |
| 4 (26.7) | 5 (33.3) |
| 4 (26.7) | 5 (33.3) |
|
| CA 19-9,
U/mlc |
|
| 0.573 |
|
| 0.356 |
|
| 0.016a |
| ≤109
(n=15) | 8 (57.1) | 7 (46.7) |
| 6 (42.9) | 9 (60.0) |
| 11 (73.3) | 4 (28.6) |
|
| >109
(n=14) | 6 (42.9) | 8 (53.3) |
| 8 (57.1) | 6 (40.0) |
| 4 (26.7) | 10 (71.4) |
|
Discussion
The present study demonstrated the clinical impact
of TILs in left-sided PDAC. Although lymph node metastasis, a high
tumor grade, a large tumor size, lymphovascular invasion,
perineural invasion, high levels of preoperative CA19-9,
persistently elevated postoperative CA19-9 levels and positive
margins of resection are typically considered prognostic factors
for pancreatic cancer (2–5), none were significantly correlated with
DFS and OS in the present study. Instead, the ratio of
Foxp3+/granzyme B+ was an independent
prognostic factor in a multivariate analysis and low levels of
CA19-9 were associated with a low Foxp3+/granzyme
B+ ratio, despite the small sample size.
Previous studies have reported that the host immune
response to tumors has a critical role in disease-associated
survival outcomes (6–15), suggesting that host immune factors may
offer a useful tool for predicting prognosis (23). Although the status of peripheral blood
lymphocytes has been reported as a prognostic factor (24), TILs in resected cancer specimens are
thought to be a more reliable measure of the host immune response
to cancer (16,23,25). TILs
consist of functionally distinct subsets. Tumor-infiltrating
CD8+ CTLs and CD4+ helper T lymphocytes
operate as antitumor effectors and are associated with a favorable
prognosis (7). Activated
CD8+ T-cells attack tumor cells presenting
tumor-associated antigens via the peptide/major histocompatibility
complex class I on the tumor cell surface (26,27).
Activated CD8+ CTLs express granzyme B on their surface
(22,28). CD4+ T-cells have a central
role in initiating and maintaining the host immune response against
cancer through numerous mechanisms. CD4+ T-cells provide
crucial help to the priming of CD8+ T-cells via
activation of antigen-presenting cells. Furthermore,
CD4+ T-cells secrete cytokines required for maintaining
CD8+ T-cell function and proliferation, and can also
inhibit tumor growth directly or indirectly. In addition,
CD4+ T-cells promote B-cell activation (29,30).
Tregs, which make up a small fraction (5–6%) of the overall
CD4+ T-cell population, reduce the antitumor immune
response by suppressing effector T-cells and the production of
several immunosuppressive cytokines, including interleukin-10 and
transforming growth factor-β (31,32). Tregs
have been shown to adversely affect patient survival (6,9,13,14,18. The
role of Tregs in PDAC is well-understood, and circulating Tregs and
PDAC tissue-specific Treg cells are significantly higher in
patients with pancreatic cancer compared with healthy controls
(24,33–37).
Furthermore, the presence of Tregs in tumor tissue correlates with
the stage and progression of pancreatic cancer (24,33–37).
Fukunaga et al (25) reported that the presence of
CD4+ T-cells together with CD8+ T-cells was
negatively correlated with tumor depth and tumor-node-metastasis
stage in pancreatic cancer. Furthermore, in multivariate analyses,
they demonstrated that a CD4+/CD8+ status was
an independent favorable prognostic factor (25). Ino et al (35) reported that higher levels of
tumor-infiltrating CD4+ and CD8+ T-cells were
significantly associated with a longer survival in patients with
PDAC. In the present study, patients with higher CD4+
T-cell counts had longer DFS and OS times, but the results did not
reach statistical significance. High CD8+ T-cell counts
were also associated with longer DFS and OS times, but the trend
also failed to reach statistical significance.
Granzyme B is exclusively expressed on the surface
of activated CD8+ CTLs (38). Activated CTLs (granzyme B+)
have been identified as a favorable prognostic factor in various
cancers (22,28,39–41);
however, their role in PDAC is unknown. In the present study,
patients with high granzyme B+ CTL counts showed
significantly improved DFS (25 vs. 10 months; P=0.023) and longer
OS in the univariate survival analysis (37 vs. 18 months;
P=0.084).
The balance between effector T-cells
(CD4+, CD8+ and granzyme B+
T-cells) and Tregs may more effectively reflect prognosis than
absolute counts alone. A ratio of high effector cell-to-low Treg
density has been reported as a promising independent predictor for
prognosis in various tumors (9,11,14,22,23,42).
Accordingly, the present study analyzed the ratios of
Foxp3+/CD4+,
Foxp3+/CD8+ and Foxp3+/granzyme
B+ as prognostic factors on the basis that they were
more representative of the biological characteristics of TILs. The
univariate survival analysis according to the relative ratios of
TIL subsets indicated that patients with a low ratio of
Foxp3+/granzyme B+ had a significantly
improved DFS (25 vs. 8 months; P=0.008) and OS (47 vs. 17 months;
P=0.003). In the multivariate survival analysis, a low
Foxp3+/granzyme B+ ratio remained a
significant independent prognostic marker with a higher hazard
ratio for DFS [Exp(B), 3.060; 95% CI, 1.259–7.436; P=0.014] and OS
[Exp (B), 3.580; 95% CI, 1.460–8.780; P=0.005).
The present study was limited by the small number of
patients, particularly since we did not observe any statistically
significant differences, even for conventional prognostic factors.
However, despite the small size, the present study demonstrated
that a low Foxp3+/granzyme B+ ratio predicted
a significantly improved prognosis. Further studies with larger
sample sizes are required to clarify the prognostic meaning of TILs
in association with other clinicopathological parameters. This
study also showed that low levels of CA19-9 were significantly
associated with a low Foxp3+/granzyme B+
ratio.
In conclusion, the present study demonstrated that a
low Foxp3+/granzyme B+ ratio was an
independent favorable prognostic marker following surgical
resection of left-sided PDAC. This immunological parameter may be
useful for stratifying patients and planning adjuvant
treatment.
Acknowledgements
This study was supported by a faculty research grant
from Yonsei University College of Medicine for 2010 (grant no.
6-2010-0138).
References
|
1
|
Li D, Xie K, Wolff R and Abbruzzese JL:
Pancreatic cancer. Lancet. 363:1049–1057. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hidalgo M: Pancreatic cancer. N Engl J
Med. 362:1605–1617. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Berger AC, Garcia M Jr, Hoffman JP, Regine
WF, Abrams RA, Safran H, Konski A, Benson AB III, MacDonald J and
Willett CG: Postresection CA 19–9 predicts overall survival in
patients with pancreatic cancer treated with adjuvant
chemoradiation: A prospective validation by RTOG 9704. J Clin
Oncol. 26:5918–5922. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ferrone CR, Finkelstein DM, Thayer SP,
Muzikansky A, Fernandez-delCastillo C and Warshaw AL: Perioperative
CA19-9 levels can predict stage and survival in patients with
resectable pancreatic adenocarcinoma. J Clin Oncol. 24:2897–2902.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Slidell MB, Chang DC, Cameron JL, Wolfgang
C, Herman JM, Schulick RD, Choti MA and Pawlik TM: Impact of total
lymph node count and lymph node ratio on staging and survival after
pancreatectomy for pancreatic adenocarcinoma: A large,
population-based analysis. Ann Surg Oncol. 15:165–174. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bates GJ, Fox SB, Han C, Leek RD, Garcia
JF, Harris AL and Banham AH: Quantification of regulatory T cells
enables the identification of high-risk breast cancer patients and
those at risk of late relapse. J Clin Oncol. 24:5373–5380. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cho Y, Miyamoto M, Kato K, Fukunaga A,
Shichinohe T, Kawarada Y, Hida Y, Oshikiri T, Kurokawa T, Suzuoki
M, et al: CD4+ and CD8+ T cells cooperate to
improve prognosis of patients with esophageal squamous cell
carcinoma. Cancer Res. 63:1555–1559. 2003.PubMed/NCBI
|
|
8
|
Clemente CG, Mihm MC Jr, Bufalino R,
Zurrida S, Collini P and Cascinelli N: Prognostic value of tumor
infiltrating lymphocytes in the vertical growth phase of primary
cutaneous melanoma. Cancer. 77:1303–1310. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fu J, Xu D, Liu Z, Shi M, Zhao P, Fu B,
Zhang Z, Yang H, Zhang H, Zhou C, et al: Increased regulatory T
cells correlate with CD8 T-cell impairment and poor survival in
hepatocellular carcinoma patients. Gastroenterology. 132:2328–2339.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gao Q, Zhou J, Wang XY, Qiu SJ, Song K,
Huang XW, Sun J, Shi YH, Li BZ, Xiao YS and Fan J: Infiltrating
memory/senescent T cell ratio predicts extrahepatic metastasis of
hepatocellular carcinoma. Ann Surg Oncol. 19:455–466. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim HI, Kim H, Cho HW, Kim SY, Song KJ,
Hyung WJ, Park CG and Kim CB: The ratio of intra-tumoral regulatory
T cells (Foxp3+)/helper T cells (CD4+) is a prognostic
factor and associated with recurrence pattern in gastric cardia
cancer. J Surg Oncol. 104:728–733. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pagès F, Berger A, Camus M, Sanchez-Cabo
F, Costes A, Molidor R, Mlecnik B, Kirilovsky A, Nilsson M, Damotte
D, et al: Effector memory T cells, early metastasis and survival in
colorectal cancer. N Engl J Med. 353:2654–2666. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Petersen RP, Campa MJ, Sperlazza J, Conlon
D, Joshi MB, Harpole DH Jr and Patz EF Jr: Tumor infiltrating
Foxp3+ regulatory T-cells are associated with recurrence in
pathologic stage I NSCLC patients. Cancer. 107:2866–2872. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sinicrope FA, Rego RL, Ansell SM, Knutson
KL, Foster NR and Sargent DJ: Intraepithelial effector
(CD3+)/regulatory (FoxP3+) T-cell ratio
predicts a clinical outcome of human colon carcinoma.
Gastroenterology. 137:1270–1279. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang L, Conejo-Garcia JR, Katsaros D,
Gimotty PA, Massobrio M, Regnani G, Makrigiannakis A, Gray H,
Schlienger K, Liebman MN, et al: Intratumoral T cells, recurrence,
and survival in epithelial ovarian cancer. N Engl J Med.
348:203–213. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Balch CM, Riley LB, Bae YJ, Salmeron MA,
Platsoucas CD, von Eschenbach A and Itoh K: Patterns of human
tumor-infiltrating lymphocytes in 120 human cancers. Arch Surg.
125:200–205. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dunn GP, Old LJ and Schreiber RD: The
immunobiology of cancer immunosurveillance and immunoediting.
Immunity. 21:137–148. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Curiel TJ, Coukos G, Zou L, Alvarez X,
Cheng P, Mottram P, Evdemon-Hogan M, Conejo-Garcia JR, Zhang L,
Burow M, et al: Specific recruitment of regulatory T cells in
ovarian carcinoma fosters immune privilege and predicts reduced
survival. Nat Med. 10:942–949. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hori S, Nomura T and Sakaguchi S: Control
of regulatory T cell development by the transcription factor Foxp3.
Science. 299:1057–1061. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sakaguchi S, Sakaguchi N, Shimizu J,
Yamazaki S, Sakihama T, Itoh M, Kuniyasu Y, Nomura T, Toda M and
Takahashi T: Immunologic tolerance maintained by CD25+
CD4+ regulatory T cells: Their common role in
controlling autoimmunity, tumor immunity, and transplantation
tolerance. Immunol Rev. 182:18–32. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ademmer K, Ebert M, Muller-Ostermeyer F,
Friess H, Büchler MW, Schubert W and Malfertheiner P: Effector T
lymphocyte subsets in human pancreatic cancer: Detection of
CD8+CD18+ cells and
CD8+CD103+ cells by multi-epitope imaging.
Clin Exp Immunol. 112:21–26. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gao Q, Qiu SJ, Fan J, Zhou J, Wang XY,
Xiao YS, Xu Y, Li YW and Tang ZY: Intratumoral balance of
regulatory and cytotoxic T cells is associated with prognosis of
hepatocellular carcinoma after resection. J Clin Oncol.
25:2586–2593. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gooden MJ, de Bock GH, Leffers N, Daemen T
and Nijman HW: The prognostic influence of tumour-infiltrating
lymphocytes in cancer: A systematic review with meta-analysis. Br J
Cancer. 105:93–103. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ikemoto T, Yamaguchi T, Morine Y, Imura S,
Soejima Y, Fujii M, Maekawa Y, Yasutomo K and Shimada M: Clinical
roles of increased populations of Foxp3+CD4+
T cells in peripheral blood from advanced pancreatic cancer
patients. Pancreas. 33:386–390. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fukunaga A, Miyamoto M, Cho Y, Murakami S,
Kawarada Y, Oshikiri T, Kato K, Kurokawa T, Suzuoki M, Nakakubo Y,
et al: CD8+ tumor-infiltrating lymphocytes together with
CD4+ tumor-infiltrating lymphocytes and dendritic cells
improve the prognosis of patients with pancreatic adenocarcinoma.
Pancreas. 28:e26–e31. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nukaya I, Yasumoto M, Iwasaki T, Ideno M,
Sette A, Celis E, Takesako K and Kato I: Identification of HLA-A24
epitope peptides of carcinoembryonic antigen which induce
tumor-reactive cytotoxic T lymphocyte. Int J Cancer. 80:92–97.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Duffour MT, Chaux P, Lurquin C, Cornelis
G, Boon T and van der Bruggen P: A MAGE-A4 peptide presented by
HLA-A2 is recognized by cytolytic T lymphocytes. Eur J Immunol.
29:3329–3337. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bleackley RC: A molecular view of
cytotoxic T lymphocyte induced killing. Biochem Cell Biol.
83:747–751. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang RF: The role of MHC class
II-restricted tumor antigens and CD4+ T cells in antitumor
immunity. Trends Immunol. 22:269–276. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Marzo AL, Kinnear BF, Lake RA, Frelinger
JJ, Collins EJ, Robinson BW and Scott B: Tumor-specific
CD4+ T cells have a major ‘post-licensing’ role in CTL
mediated anti-tumor immunity. J Immunol. 165:6047–6055. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Thornton AM and Shevach EM:
CD4+CD25+ immunoregulatory T cells suppress
polyclonal T cell activation in vitro by inhibiting
interleukin 2 production. J Exp Med. 188:287–296. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sakaguchi S: Naturally arising
CD4+ regulatory t cells for immunologic self-tolerance
and negative control of immune responses. Annu Rev Immunol.
22:531–562. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hiraoka N, Onozato K, Kosuge T and
Hirohashi S: Prevalence of FOXP3+ regulatory T cells increases
during the progression of pancreatic ductal adenocarcinoma and its
premalignant lesions. Clin Cancer Res. 12:5423–5434. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wachsmann MB, Pop LM and Vitetta ES:
Pancreatic ductal adenocarcinoma: A review of immunologic aspects.
J Investig Med. 60:643–663. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ino Y, Yamazaki-Itoh R, Shimada K, Iwasaki
M, Kosuge T, Kanai Y and Hiraoka N: Immune cell infiltration as an
indicator of the immune microenvironment of pancreatic cancer. Br J
Cancer. 108:914–923. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kobayashi N, Kubota K, Kato S, Watanabe S,
Shimamura T, Kirikoshi H, Saito S, Ueda M, Endo I, Inayama Y, et
al: FOXP3+ regulatory T cells and tumoral indoleamine
2,3-dioxygenase expression predicts the carcinogenesis of
intraductal papillary mucinous neoplasms of the pancreas.
Pancreatology. 10:631–640. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Liyanage UK, Moore TT, Joo HG, Tanaka Y,
Herrmann V, Doherty G, Drebin JA, Strasberg SM, Eberlein TJ,
Goedegebuure PS and Linehan DC: Prevalence of regulatory T cells is
increased in peripheral blood and tumor microenvironment of
patients with pancreas or breast adenocarcinoma. J Immunol.
169:2756–2761. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Oshikiri T, Miyamoto M, Shichinohe T,
Suzuoki M, Hiraoka K, Nakakubo Y, Shinohara T, Itoh T, Kondo S and
Katoh H: Prognostic value of intratumoral CD8+ T
lymphocyte in extrahepatic bile duct carcinoma as essential immune
response. J Surg Oncol. 84:224–228. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Schumacher K, Haensch W, Röefzaad C and
Schlag PM: Prognostic significance of activated CD8(+) T cell
infiltrations within esophageal carcinomas. Cancer Res.
61:3932–3936. 2001.PubMed/NCBI
|
|
40
|
van Beek J, zur Hausen A, Snel SN, Berkhof
J, Kranenbarg EK, van de Velde CJ, van den Brule AJ, Middeldorp JM,
Meijer CJ and Bloemena E: Morphological evidence of an activated
cytotoxic T-cell infiltrate in EBV-positive gastric carcinoma
preventing lymph node metastases. Am J Surg Pathol. 30:59–65. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Grabenbauer GG, Lahmer G, Distel L and
Niedobitek G: Tumor-infiltrating cytotoxic T cells but not
regulatory T cells predict outcome in anal squamous cell carcinoma.
Clin Cancer Res. 12:3355–3360. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Abe M, Kondo S, Hirano S, Ambo Y, Tanaka
E, Morikawa T, Okushiba S and Katoh H: Long-term survival after
radical resection of advanced pancreatic cancer: A case report with
special reference to CD8+ T-cell infiltration. Int J
Gastrointest Cancer. 33:107–110. 2003. View Article : Google Scholar : PubMed/NCBI
|