Introduction
Pancreatic cancer has one of the highest mortality
rates in cancer, with five-year overall survival (OS) rate <5%
and despite significant advances in medical technologies, this
situation of short survival has not improved for four decades. The
dismal prognosis of pancreatic cancer patients and the lack of
effective drugs to improve survival beyond few months, necessitates
understanding of the pathogenic mechanisms of this cancer and the
factors that drive its rapid growth and to identify better and
efficacious therapeutics. It has been thought that diabetes
mellitus is a primary risk factor for the development of pancreatic
cancer and nearly 45% of the pancreatic cancer cases are likely to
present as new onset diabetes cases, with somewhat elevated
incidence in males (1,2). The strong link between diabetes and
pancreatic cancer can be mostly due to new-onset diabetes. However,
whether diabetes is a risk factor for pancreatic cancer or only the
manifestation of pancreatic cancer has been debated and more
studies suggested that diabetes as well as metabolic syndrome are
potential risk factors for pancreatic cancer (3). Type 2 diabetes mellitus (T2D) is a
metabolic disease with characteristic hyperglycemia that arises
because of defective insulin secretion by pancreatic islets in
response to elevated post-prandial blood glucose levels and insulin
resistance of peripheral tissues as well as dysregulated hepatic
glucose production (4). T2D is often
associated with obesity, which has been on the increase across the
globe. Defective response of body tissues to insulin, i.e., reduced
insulin sensitivity, places an increased demand on pancreatic
islets to secrete higher quantities of insulin, leading to
hyperinsulinemia and these are usually the primary events in the
pathogenesis of T2D, which are precipitated by genetic as well as
environmental factors (5).
Insulin is known to function as a regulator of
glucose and lipid metabolism and to act as a potential growth
factor in the promotion of cell proliferation and angiogenesis.
Although diabetes and obesity are suspected of increasing the risk
of different types of cancers, the risk for pancreatic cancer is
thought to be particularly high (6).
Malignant transformation of pancreatic cells, predominantly the
ductal epithelial cells of the exocrine pancreas, when associated
with locally elevated supply of insulin coming from the endocrine
islets of pancreas, grow rapidly and probably such an association
is the cause for the devastating outcome of pancreatic cancer
(7). The nature of association
between T2D and pancreatic cancer is controversial as some studies
indicated T2D lowering the OS (8,9) while
others did not find such an effect (10,11).
Additionally, epidemiological studies indicated an increased
incidence of diabetes in pancreatic cancer and an elevated number
of cases of pancreatic cancer in diabetic patients, raising the
question whether diabetes is a cause or consequence of pancreatic
cancer (12,13). In several of these studies, a clear
differentiation between type 1 or 2 diabetes was not made and
diabetes incidence was viewed collectively. In the present
meta-analysis, we have tried to address this issue of association
of T2D with pancreatic cancer, taking into consideration recently
published clinical studies with identified T2D patients. Our
results suggest that new onset T2D (observed ≤2 years before
pancreatic cancer diagnosis) is a strong indicator of pancreatic
cancer development and also that the presence of diabetes for >5
years can be a significant risk factor for pancreatic cancer.
Materials and methods
Objectives
In the present meta-analysis, we analyzed the
results from clinical studies that examined the co-incidence of T2D
and pancreatic adenocarcinoma, along with other variables such as
insulin usage as a therapeutic measure. We also analyzed the
relationship between the time of diagnosis and history of diabetes
and the diagnosis of pancreatic cancer.
Methods
Criteria for considering studies for this
review
Clinical studies that examined the relationship
between the incidences of diabetes and pancreatic cancer were
included in this meta-analysis. Studies that did not clearly
document the diagnosis of diabetes (e.g., by HbA1c levels or
hyperinsulinemia) or did not record the patient history of diabetes
were excluded. While few studies only examined diabetic patients
with pancreatic cancer, others included pancreatic cancer patients
without and with a diagnosis of diabetes. In addition, diabetic
patients with a history of cancer diagnosis that was not primarily
related to pancreatic cancer were excluded from the study. Even
though there appears to be a strong male preponderance in the
incidence of diabetes in pancreatic cancer patients, we included
both male and female patients and analyzed the results
collectively, to eliminate any gender-related bias in the study.
Detailed selection and exclusion criteria of identified studies for
the meta-analysis is shown in Fig.
1.
Search methods
Publications describing the relevant information
were searched in PubMed, Google Scholar, Scopus and Web of Science
databases. Search MeSH terms included pancreatic cancer, diabetes
mellitus, T2D, OS, clinical studies, hyperglycemia, insulin,
insulin resistance, pancreatic ductal carcinoma and pancreatic
adenocarcinoma. Publications in the last 10 years were searched, as
many of the earlier publication did not differentiate between type
1 and T2D in their analysis. All the citations, only in the English
language, were initially screened for relevance of the title and
abstract level and full reports and supplemental information files
were retrieved as per the relevance of the selected study.
Data collection and analysis and quality
assessment
All the co-authors of this meta-analysis
independently screened the full texts of all the selected studies
for the details of patient selection and parameters studied. All
the collected information was then pooled and reviewed collectively
and any differences of opinion or discrepancies were resolved by
discussion and consensus. The following data were extracted from
the included studies: Details of the institutions where the studies
were conducted and the authors, publication details, the total
number of patients studied and the number of patients in pancreatic
cancer with T2D group and pancreatic cancer without T2D group, age,
and gender of the studied patients. In addition, where available,
we collected information regarding the history and onset of
diabetes in comparison to the time of diagnosis of pancreatic
cancer. OS data were obtained only from a few studies.
Statistical analysis
We prepared a Preferred Reporting Items for
Systematic Reviews and Meta-Analyses (PRISMA) checklist (Table I). Methods suggested by the Cochrane
Collaboration guidelines for meta-analysis have been used.
Statistical analyses were performed by Review Manager (RevMan)
version 5.3 (The Cochrane Collaboration). The association of T2D
duration before and along with pancreatic cancer was analyzed
independent of each other. Mantel-Haenszel statistics were applied
in the random-effect model, for the analyses of body mass index
(BMI), carbohydrate antigen 19-9 (CA19-9), HbA1c and OS and odds
ratios (OR) were derived at 95% confidence intervals (CI).
Mantel-Haenszel statistics were applied in the fixed-effect model
for the analyses of association between pancreatic cancer and
duration and history of diabetes, and OR were derived at 95% CI.
Publication bias was analyzed by Funnel plot of sample size of each
study. Sensitivity analysis was performed for T2D and pancreatic
cancer association by excluding one study at a time in analyzing
the results.
 | Table I.PRISMA check list. |
Table I.
PRISMA check list.
| Section/topic | No. | Checklist item | Reported on page
no. |
|---|
| Title |
|
|
|
|
|
Title | 1 | Identify the report
as a systematic review, meta-analysis, or both. | 1 |
| Abstract |
|
|
|
|
Structured summary | 2 | Provide a structured
summary including, as applicable: Background; objectives; data
sources; study eligibility criteria, participants, and
interventions; study appraisal and synthesis methods; results;
limitations; conclusions and implications of key findings;
systematic review registration number. | 2 |
| Introduction |
|
|
|
|
Rationale | 3 | Describe the
rationale for the review in the context of what is already
known. | 2,3 |
|
Objectives | 4 | Provide an explicit
statement of questions being addressed with reference to
participants, interventions, comparisons, outcomes, and study
design (PICOS). | 4 |
| Methods |
|
|
|
| Protocol
and registration | 5 | Indicate if a review
protocol exists, if and where it can be accessed (e.g., web
address), and, if available, provide registration information
including registration number. | N/A |
|
Eligibility criteria | 6 | Specify study
characteristics (e.g., PICOS, length of follow-up) and report
characteristics (e.g., years considered, language, publication
status) used as criteria for eligibility, giving rationale. | 5 |
|
Information sources | 7 | Describe all
information sources (e.g., databases with dates of coverage,
contact with study authors to identify additional studies) in the
search and date last searched. | 5 |
|
Search | 8 | Present full
electronic search strategy for at least one database, including any
limits used, such that it could be repeated. | 5 |
| Study
selection | 9 | State the process for
selecting studies (i.e., screening, eligibility, included in
systematic review, and, if applicable, included in the
meta-analysis). | 6 |
| Data
collection process | 10 | Describe method of
data extraction from reports (e.g., piloted forms, independently,
in duplicate) and any processes for obtaining and confirming data
from investigators. | 5 |
| Data
items | 11 | List and define all
variables for which data were sought (e.g., PICOS, funding sources)
and any assumptions and simplifications made. | 5 |
| Risk of
bias in individual studies | 12 | Describe methods
used for assessing risk of bias of individual studies (including
specification of whether this was done at the study or outcome
level), and how this information is to be used in any data
synthesis. | 6 |
| Summary
measures | 13 | State the principal
summary measures (e.g., risk ratio, difference in means). | 5,6 |
|
Synthesis of results | 14 | Describe the
methods of handling data and combining results of studies, if done,
including measures of consistency (e.g., I2) for each
meta-analysis. | 5,6 |
| Risk of
bias across studies | 15 | Specify any
assessment of risk of bias that may affect the cumulative evidence
(e.g., publication bias, selective reporting within studies). | 6 |
|
Additional analyses | 16 | Describe methods of
additional analyses (e.g., sensitivity or subgroup analyses,
meta-regression), if done, indicating which were
pre-specified. | 6 |
| Results |
|
|
|
| Study
selection | 17 | Give numbers of
studies screened, assessed for eligibility, and included in the
review, with reasons for exclusions at each stage, ideally with a
flow diagram. | 6,7 |
| Study
characteristics | 18 | For each study,
present characteristics for which data were extracted (e.g., study
size, PICOS, follow-up period) and provide the citations. | 7,8 |
| Risk of
bias within studies | 19 | Present data on
risk of bias of each study and, if available, any outcome level
assessment (see item 12). | 9 |
| Results
of individual studies | 20 | For all outcomes
considered (benefits or harms), present, for each study: a) Simple
summary data for each intervention group; b) effect estimates and
confidence intervals, ideally with a forest plot. | 7,9 |
|
Synthesis of results | 21 | Present results of
each meta-analysis done, including confidence intervals and
measures of consistency. | 8,9 |
| Risk of
bias across studies | 22 | Present results of
any assessment of risk of bias across studies (see item 15). | 9 |
|
Additional analysis | 23 | Give results of
additional analyses, if done [e.g., sensitivity or subgroup
analyses, meta-regression (see item 16)]. | 9 |
| Discussion |
|
|
|
| Summary
of evidence | 24 | Summarize the main
findings including the strength of evidence for each main outcome;
consider their relevance to key groups (e.g., healthcare providers,
users, and policy makers). | 8,9 |
|
Limitations | 25 | Discuss limitations
at study and outcome level (e.g., risk of bias), and at review
level (e.g., incomplete retrieval of identified research, reporting
bias). | 9 |
|
Conclusions | 26 | Provide a general
interpretation of the results in the context of other evidence, and
implications for future research. | 9 |
| Funding |
|
|
|
|
Funding | 27 | Describe sources of
funding for the systematic review and other support (e.g., supply
of data); role of funders for the systematic review. | N/A |
Results
Database searches using the MeSH terms yielded a
total of 4,243 studies, which also included some non-clinical and
experimental studies. First round of screening to eliminate
experimental and non-patient studies (a total of 2,656) yielded
1,587 studies. Further screening to eliminate studies that are not
clinically oriented (a total of 1,012), resulted in identification
of 575 studies. After applying the criteria of T2D inclusion, 465
studies were removed from the analysis. Subsequent screening to
remove review type articles and studies older than 10 years, led to
exclusion of 87 studies and 23 studies remained in the analysis.
Finally, a few more studies were removed due to incomplete
information, lack of proper controls and foreign language (other
than English) studies, with 11 studies remaining in the final
analysis. Inclusion criteria were: Pancreatic cancer diagnosis,
history or occurrence of T2D, clear diagnosis of T2D (HbA1c
>6.5%). Patients with metastatic disease were not excluded from
the analysis. Control patients had pancreatic cancer but were not
diagnosed with T2D and did not have a history of T2D. The total
number of patients in the included studies were 14,399, of which
T2D diagnosis was positive in 4,080 patients and the non-diabetics
were 9,721. The included studies were (Table II): Nakai et al (2013)
(10); Li et al (2015)
(14); Bosetti et al (2014)
(15); Mizuno et al (2013)
(16); Li et al (2011)
(17); Oberaigner et al (2014)
(18); Lu et al (2015)
(19); Wang et al (2006)
(20); Choi et al (2016)
(21); Wolpin et al (2013)
(22); and Sadr-Azodi et al
(2015) (23).
| Table II.Patient characteristics. |
Table II.
Patient characteristics.
|
|
|
|
| Pancreatic cancer
patients with T2D | Pancreatic cancer
patients without T2D |
|---|
|
|
|
|
|
|
|
|---|
| Study Author, year
(Ref.) | Total no. of
cases | Males | Age (years) | T2D patients | No. of patients
with BMI >25 | No. of patients
without T2D | No. of patients
with BMI >25 |
|---|
| Nakai et al,
2013 (10) | 250 | 147 | 66 | 124 | – | 126 | – |
| Li et al,
2015 (14) | 1,328 | 787 | 67 | 590 | 472 | 738 | 498 |
| Bosetti et
al, 2014 (15) | 8,305 | 4,589 | 72 | 1,767 | 1,205 | 6,404 | 3,410 |
| Mizuno et
al, 2013 (16) | 40 | 31 | 70 | 40 | – | – | – |
| Li et al,
2011 (17) | 2,192 | 977 | 63 | 448 | 218 | 1,744 | 647 |
| Oberaigner et
al, 2014 (18) | 34 | 18 | 66 | 34 | – | – | – |
| Lu et al,
2015 (19) | 529 | 307 | 66 | 175 | 286 | 354 | – |
| Wang et al,
2006 (20) | 532 | 314 | 60 | 68 | 51 | – | – |
| Choi et al,
2016 (21) | 349 | 224 | 60 | 183 | 27 | 166 | 15 |
| Wolpin et
al, 2013 (22) | 449 | 128 | 63.1 | 260 | 243 | 189 | – |
| Sadr-Azodi et
al, 2015 (23) | 391 | 220 | 67 | 391 | 270 | – | – |
Patient characteristics
The included patients had an average age of 66.5
years, with 6,657 female and 7,742 male patients. A total of 4,080
pancreatic cancer patients with T2D and 9,721 patients without T2D
were further analyzed (Table II).
Among the T2D pancreatic cancer patients, nearly 68% were with BMI
above 25 kg/m2 and 47% of the pancreatic cancer patients
without T2D had a BMI above 25 kg/m2. The average HbA1c
for the diabetic patients is 7.41%, which is above the normal
values (6.5%) and for non-diabetic patients it is 5.4%. As there is
considerable variation in sample size among the included studies,
this has introduced significant heterogeneity (see below). The
values for CA19-9, a cancer biomarker, are particularly high in T2D
pancreatic cancer patients as compared to patients without T2D
(Table III). The OS was reported in
only three studies and this ranged from 8.4 to 13.3 months in T2D
patients with pancreatic cancer and from 7.5 to 14.2 months in
pancreatic cancer patients without T2D (Table III).
| Table III.Differences in CA19-9, HbA1c and OS
in pancreatic cancer patients with and without T2D. |
Table III.
Differences in CA19-9, HbA1c and OS
in pancreatic cancer patients with and without T2D.
|
|
| Pancreatic cancer
patients with T2D | Pancreatic cancer
patients without T2D |
|---|
|
|
|
|
|
|---|
| Study Author, year
(Ref.) | Total no. of
cases | No. of patients
with CA19.9 (>500) | HbA1c, % | OS (months) | No. of patients
with CA19-9 (>100) | HbA1c, % | OS (months) |
|---|
| Nakai et al,
2013 (10) | 250 | 100 | 8.45+/−0.88 | 13.3+/−1.1 | 89 | 5.1+/−0.3 | 10+/−0.5 |
| Li et al,
2015 (14) | 1,328 | 335 | – | 11.7+/−1.1 | 378 |
| 14.2+/−1.5 |
| Bosetti et
al, 2014 (15) | 8,305 | – | – | – |
|
|
|
| Mizuno et
al, 2013 (16) | 40 | – | – | – |
|
|
|
| Li et al,
2011 (17) | 2,192 | – | – | – |
|
|
|
| Oberaigner et
al, 2014 (18) | 34 | – | 7.7+/−0.5 | – |
|
|
|
| Lu et al,
2015 (19) | 529 | – | 7.9+/−1 | – |
| 6+/−0.2 |
|
| Wang et al,
2006 (20) | 532 | – | – | – |
|
|
|
| Choi et al,
2016 (21) | 349 | 149 | – | 8.4+/−0.8 | 133 |
| 7.5+/−0.6 |
| Wolpin et
al, 2013 (22) | 449 | – | 5.11+/−0.24 | – |
| 5.09+/−0.2 |
|
| Sadr-Azodi et
al, 2015 (23) | 391 | – | 7.9+/−1.1 | – |
|
|
|
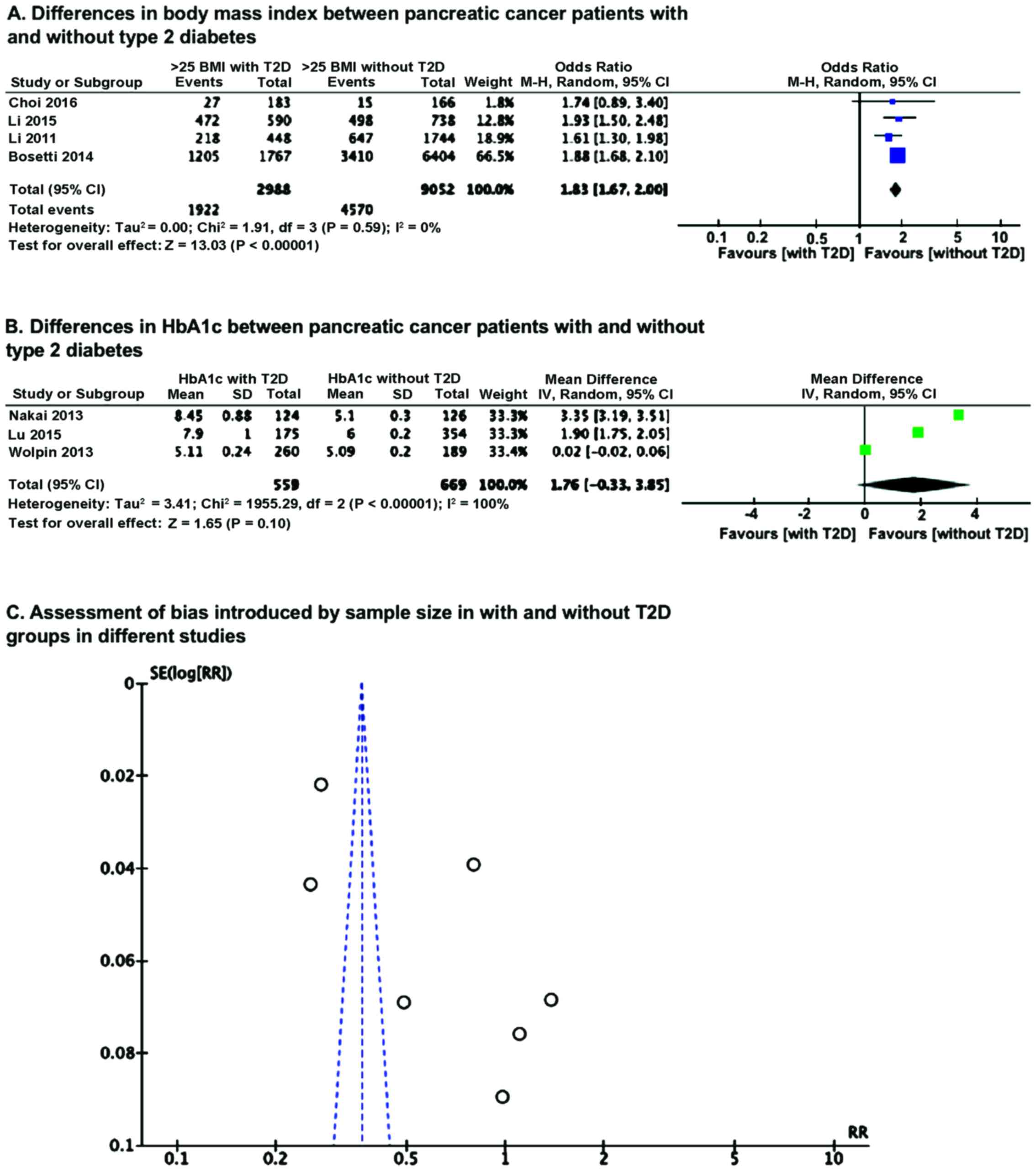
OR analysis of BMI using Mantel-Haenszel statistics
in the random-effect model, revealed that the number of patients
having BMI of <25 kg/m2 in without T2D group is
significantly higher (P<0.00001) than in group with T2D
pancreatic cancer patients (Fig. 2A).
However, a mean difference analysis of HbA1c level between the with
and without T2D groups revealed no significant difference (Fig. 2B), which could be because of smaller
number of studies and also wide variation, as reflected in
significant heterogeneity. Because of this heterogeneity, we
examined whether there was any sample size effect bias in the
results due to variation in sample size among the included studies,
by Funnel plot and found this had introduced significant
heterogeneity (Fig. 2C).
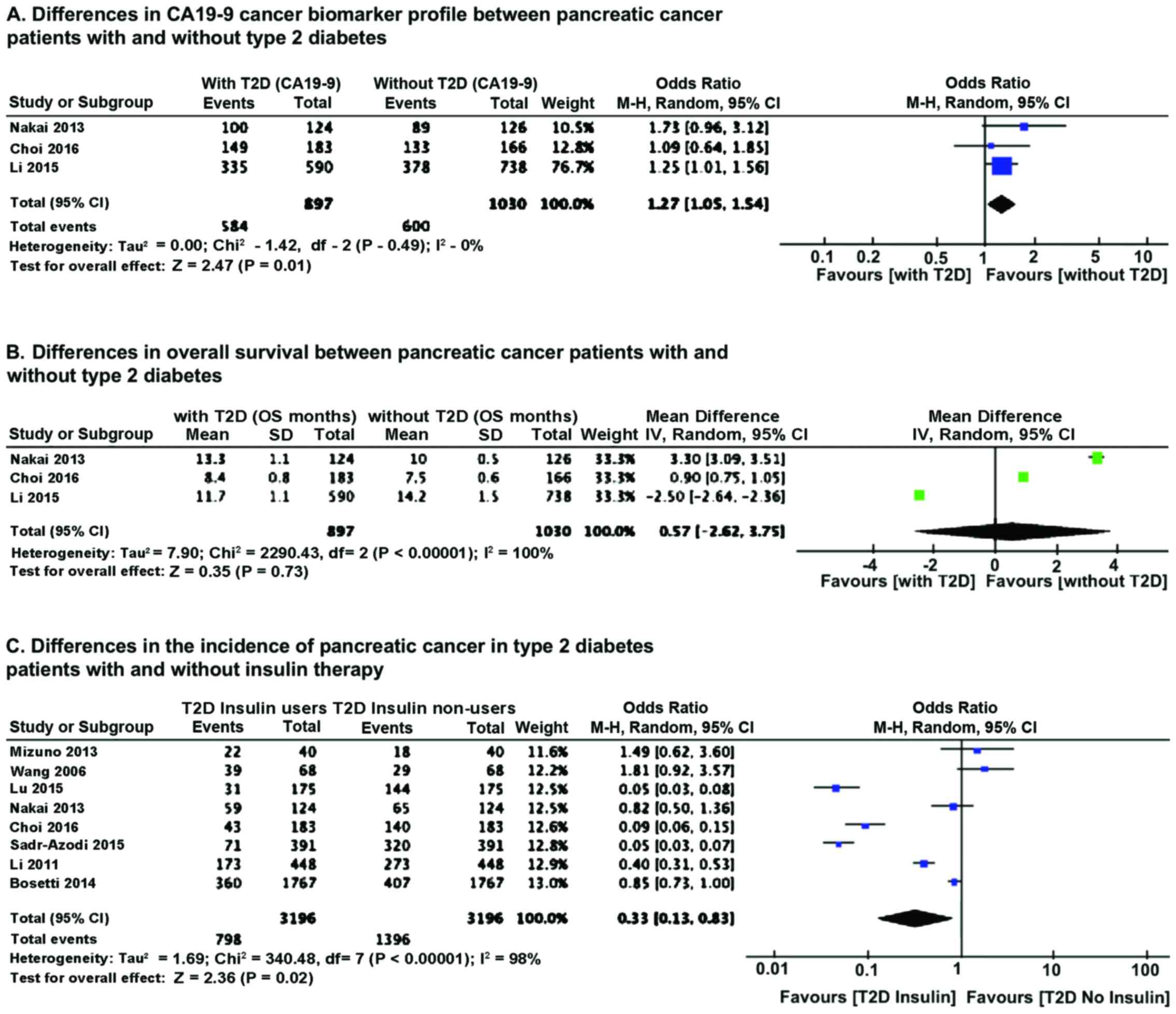
OR analysis of CA19-9 cancer biomarker showed that
T2D pancreatic cancer patients had a much higher level of CA19-9
(P=0.01) compared to pancreatic cancer patients without T2D
(Fig. 3A). Heterogeneity did not
influence the results. No major differences were noted in OS
between patients without and with T2D. However, there was
significant heterogeneity in the samples (Fig. 3B). We further analyzed the effect of
insulin therapy of diabetic patients on the incidence of pancreatic
cancer. Results of OR analysis using Mantel-Haenszel statistics in
the random-effect model indicated that the incidence of pancreatic
cancer is lower (P=0.02) in T2D patients on insulin therapy
(Fig. 3C).
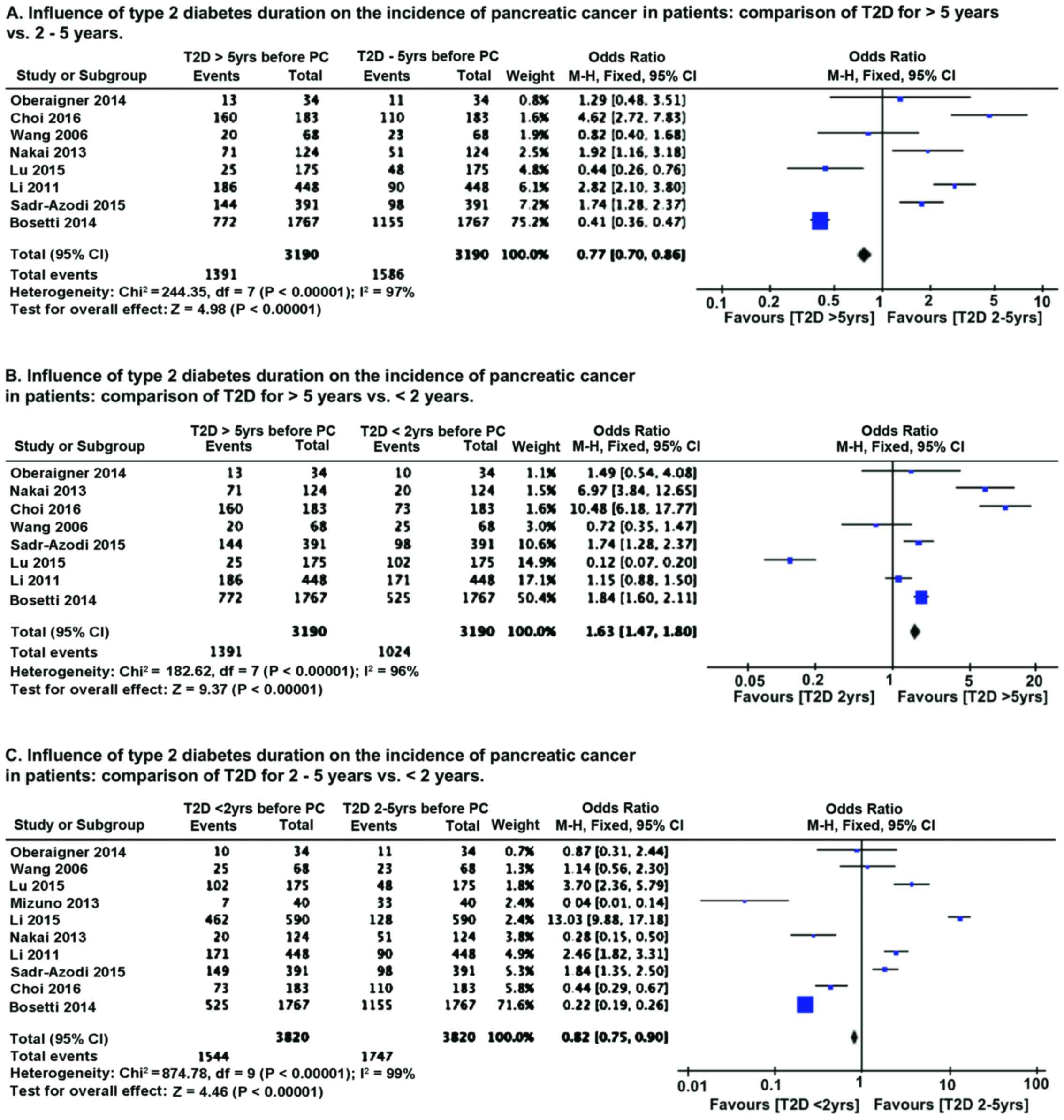
We compared the influence of diabetes history and
duration on the incidence of pancreatic cancer. Because of the
relatively smaller number of studies with varying sample size, we
performed OR analysis using Mantel-Haenszel statistics in the
fixed-effect model. As compared to patients with long history of
T2D (>5 years), patients with T2D diagnosed between 2–5 years
prior to pancreatic cancer diagnosis had lower (P<0.00001)
incidence of pancreatic cancer (Fig.
4A). However, patients with recent onset of T2D (diagnosed
<2 years before cancer detection) had higher (P<0.00001)
incidence of pancreatic cancer (Fig.
4B). Comparison of T2D patients with diagnosis 2–5 years before
cancer detection with recent onset T2D patients (<2 years)
revealed that pancreatic cancer incidence is higher (P<0.00001)
in recent onset T2D patients (Fig.
4C). Sensitivity analysis by removing one study at a time, for
all the parameters analyzed, revealed no change in the pattern of
association of T2D with pancreatic cancer incidence.
Discussion
Diabetes and pancreatic cancer are associated with
each other; however, depending on how the sampling is carried out
and the focus of the study, it was not clear whether diabetes
promotes pancreatic cancer incidence or diabetes is one of the
primary symptoms of developing pancreatic cancer (12,13).
Similarly, it has been observed in some studies that diabetes has
no significant effect on the duration of OS (10,24), but
other studies indicated that diabetes significantly reduced the OS
(25,26). A recent meta-analysis indicated an
association of diabetes with increased overall mortality in
pancreatic cancer patients and that the survival of the patient is
also dependent on the stage of tumor and the duration of diabetes
(27). Also, there is some
discrepancy regarding the risk of pancreatic cancer - whether it is
insulin resistance or hyperglycemia, both of which are
characteristics of T2D. A recent study indicated that peripheral
insulin resistance, rather than hyperglycemia or pancreatic β-cell
dysfunction, is associated with risk of pancreatic adenocarcinoma
(22).
In the present meta-analysis, we find that the
levels of CA19-9 cancer biomarker are much higher in T2D pancreatic
cancer patients. Inasmuch as CA19-9 is likely an indicator of the
aggressiveness of cancer growth (28,29), the
present analysis provides direct evidence showing diabetes promotes
rapid growth and aggressiveness of pancreatic cancer and thus
likely contributes to increased mortality in these patients.
However, because of high level of sample heterogeneity, and smaller
number of studies which reported OS, we could not get an accurate
estimate of the effect of diabetes on OS.
The present study supports the notion that recent
onset diabetes (prior to the diagnosis of pancreatic cancer) is
significantly associated with increased incidence of pancreatic
cancer as compared to 2 years or longer duration of diabetes, prior
to pancreatic cancer diagnosis. This is an indication that recent
onset diabetes is more likely a manifestation of subclinical
pancreatic cancer, rather than a causative or risk factor for
cancer. On the other hand, we noted that long-term T2D patients had
increased pancreatic cancer incidence, as compared to short-term
T2D patients (2–5 years), which is suggestive of the idea that
diabetic condition that encompasses insulin resistance and
hyperglycemia are likely risk factors for the development of
pancreatic cancer, as previously indicated (14). Notably, we found that insulin therapy
is associated with reduced pancreatic cancer incidence. As it was
indicated and suspected that elevated levels of insulin in pancreas
may support the growth of pancreatic tumor (30), it appears that reduced incidence of
pancreatic cancer in insulin users is contradictory. However, this
finding suggests that while locally produced elevated levels of
insulin, which has ready access to the tumor cells of pancreatic
cancer and thus promote their aggressive growth, externally
administered insulin may hamper or does not promote the development
of pancreatic cancer, probably by controlling blood glucose levels
and thus reducing the supply of much needed glucose to the
pancreatic cancer cells. It is known that pancreatic cancer cells
are highly glycolytic and glucose-dependent for their growth
(31,32). Therefore, the discrepancy related to
the association of long-term diabetes with pancreatic cancer may
relate to the proportion of patients who use insulin in a given
patient cohort, with higher number of insulin-user patients there
may be reduced risk for pancreatic cancer.
Limitations of this study
One major drawback of this meta-analysis is
incomplete data for OS of the included patients. Also, not all
studies reported HbA1c values for the included T2D patients.
Besides this, the included studies suffered from widely varying
sample size, which led to high degree of heterogeneity, which
probably affected some of the analyses, particularly OS. Another
drawback is inclusion of studies, that enrolled only T2D patients
with pancreatic cancer, which could have introduced certain degree
of bias.
In conclusion, this meta-analysis showed that
recent-onset T2D is probably a manifestation of pancreatic cancer
whereas long-term T2D is likely a risk factor for this cancer. The
increased mortality of pancreatic cancer patients with T2D is
probably related to the aggressive growth of the tumor, as
evidenced by CA19-9 cancer marker. Furthermore, insulin therapy
appears to lower the incidence of pancreatic cancer, probably by
lowering blood glucose and thus curtailing the supply of glucose to
the growing tumor. Further studies are needed to clearly understand
the significance of locally produced elevated levels of insulin as
compared to the protective effects of externally administered
insulin in pancreatic cancer patients with T2D.
References
|
1
|
Ben Q, Cai Q, Li Z, Yuan Y, Ning X, Deng S
and Wang K: The relationship between new-onset diabetes mellitus
and pancreatic cancer risk: a case-control study. Eur J Cancer.
47:248–254. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Siegel R, Ward E, Murray T, Xu J,
Smigal C and Thun MJ: Cancer statistics, 2006. CA Cancer J Clin.
56:106–130. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Esposito K, Chiodini P, Colao A, Lenzi A
and Giugliano D: Metabolic syndrome and risk of cancer: a
systematic review and meta-analysis. Diabetes Care. 35:2402–2411.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Unger RH and Orci L: Paracrinology of
islets and the paracrinopathy of diabetes. Proc Natl Acad Sci USA.
107:16009–16012. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Stumvoll M, Goldstein BJ and van Haeften
TW: Type 2 diabetes: principles of pathogenesis and therapy.
Lancet. 365:1333–1346. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Burney S, Irfan K, Saif MW and Masud F:
Diabetes and pancreatic cancer. JOP. 15:319–321. 2014.PubMed/NCBI
|
|
7
|
Fokas E, O'Neill E, Gordon-Weeks A,
Mukherjee S, McKenna WG and Muschel RJ: Pancreatic ductal
adenocarcinoma: from genetics to biology to radiobiology to
oncoimmunology and all the way back to the clinic. Biochim Biophys
Acta. 1855:61–82. 2015.PubMed/NCBI
|
|
8
|
Walter U, Kohlert T, Rahbari NN, Weitz J
and Welsch T: Impact of preoperative diabetes on long-term survival
after curative resection of pancreatic adenocarcinoma: a systematic
review and meta-analysis. Ann Surg Oncol. 21:1082–1089. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sahin IH, Shama MA, Tanaka M, Abbruzzese
JL, Curley SA, Hassan M and Li D: Association of diabetes and
perineural invasion in pancreatic cancer. Cancer Med. 1:357–362.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nakai Y, Isayama H, Sasaki T, Mizuno S,
Sasahira N, Kogure H, Kawakubo K, Yamamoto N, Hirano K, Ijichi H,
et al: Clinical outcomes of chemotherapy for diabetic and
nondiabetic patients with pancreatic cancer: better prognosis with
statin use in diabetic patients. Pancreas. 42:202–208. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vickers MM, Powell ED, Asmis TR, Jonker
DJ, Hilton JF, O'Callaghan CJ, Tu D, Parulekar W and Moore MJ:
Comorbidity, age and overall survival in patients with advanced
pancreatic cancer - results from NCIC CTG PA.3: a phase III trial
of gemcitabine plus erlotinib or placebo. Eur J Cancer.
48:1434–1442. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chari ST, Leibson CL, Rabe KG, Timmons LJ,
Ransom J, de Andrade M and Petersen GM: Pancreatic
cancer-associated diabetes mellitus: prevalence and temporal
association with diagnosis of cancer. Gastroenterology. 134:95–101.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li J, Cao G, Ma Q, Liu H, Li W and Han L:
The bidirectional interation between pancreatic cancer and
diabetes. World J Surg Oncol. 10:1712012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li D, Mao Y, Chang P, Liu C, Hassan MM,
Yeung SJ and Abbruzzese JL: Impacts of new-onset and long-term
diabetes on clinical outcome of pancreatic cancer. Am J Cancer Res.
5:3260–3269. 2015.PubMed/NCBI
|
|
15
|
Bosetti C, Rosato V, Li D, Silverman D,
Petersen GM, Bracci PM, Neale RE, Muscat J, Anderson K, Gallinger
S, et al: Diabetes, antidiabetic medications, and pancreatic cancer
risk: an analysis from the International Pancreatic Cancer
Case-Control Consortium. Ann Oncol. 25:2065–2072. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mizuno S, Nakai Y, Isayama H, Yanai A,
Takahara N, Miyabayashi K, Yamamoto K, Kawakubo K, Mohri D, Kogure
H, et al: Risk factors and early signs of pancreatic cancer in
diabetes: screening strategy based on diabetes onset age. J
Gastroenterol. 48:238–246. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li D, Tang H, Hassan MM, Holly EA, Bracci
PM and Silverman DT: Diabetes and risk of pancreatic cancer: a
pooled analysis of three large case-control studies. Cancer Causes
Control. 22:189–197. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oberaigner W, Ebenbichler C, Oberaigner K,
Juchum M, Schönherr HR and Lechleitner M: Increased cancer
incidence risk in type 2 diabetes mellitus: results from a cohort
study in Tyrol/Austria. BMC Public Health. 14:10582014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lu Y, García Rodríguez LA, Malgerud L,
González-Pérez A, Martín-Pérez M, Lagergren J and Bexelius TS:
New-onset type 2 diabetes, elevated HbA1c, anti-diabetic
medications, and risk of pancreatic cancer. Br J Cancer.
113:1607–1614. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang F, Gupta S and Holly EA: Diabetes
mellitus and pancreatic cancer in a population-based case-control
study in the San Francisco Bay Area, California. Cancer Epidemiol
Biomarkers Prev. 15:1458–1463. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Choi Y, Kim TY, Oh DY, Lee KH, Han SW, Im
SA, Kim TY and Bang YJ: The impact of diabetes mellitus and
metformin treatment on survival of patients with advanced
pancreatic cancer undergoing chemotherapy. Cancer Res Treat.
48:171–179. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wolpin BM, Bao Y, Qian ZR, Wu C, Kraft P,
Ogino S, Stampfer MJ, Sato K, Ma J, Buring JE, et al:
Hyperglycemia, insulin resistance, impaired pancreatic β-cell
function, and risk of pancreatic cancer. J Natl Cancer Inst.
105:1027–1035. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sadr-Azodi O, Gudbjörnsdottir S and Ljung
R: Pattern of increasing HbA1c levels in patients with diabetes
mellitus before clinical detection of pancreatic cancer - a
population-based nationwide case-control study. Acta Oncol.
54:986–992. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dandona M, Linehan D, Hawkins W, Strasberg
S, Gao F and Wang-Gillam A: Influence of obesity and other risk
factors on survival outcomes in patients undergoing
pancreaticoduodenectomy for pancreatic cancer. Pancreas.
40:931–937. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cannon RM, LeGrand R, Chagpar RB, Ahmad
SA, McClaine R, Kim HJ, Rupp C, Cho CS, Brinkman A, Weber S, et al:
Multi-institutional analysis of pancreatic adenocarcinoma
demonstrating the effect of diabetes status on survival after
resection. HPB Oxf. 14:228–235. 2012. View Article : Google Scholar
|
|
26
|
van de Poll-Franse LV, Houterman S,
Janssen-Heijnen ML, Dercksen MW, Coebergh JW and Haak HR: Less
aggressive treatment and worse overall survival in cancer patients
with diabetes: a large population based analysis. Int J Cancer.
120:1986–1992. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mao Y, Tao M, Jia X, Xu H, Chen K, Tang H
and Li D: Effect of diabetes mellitus on survival in patients with
pancreatic cancer: a systematic review and meta-analysis. Sci Rep.
5:171022015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Elisei R, Lorusso L, Romei C, Bottici V,
Mazzeo S, Giani C, Fiore E, Torregrossa L, Insilla AC, Basolo F, et
al: Medullary thyroid cancer secreting carbohydrate antigen 19-9
(Ca 19-9): a fatal case report. J Clin Endocrinol Metab.
98:3550–3554. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Pall M, Iqbal J, Singh SK and Rana SV: CA
19-9 as a serum marker in urothelial carcinoma. Urol Ann. 4:98–101.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Biadgo B and Abebe M: Type 2 diabetes
mellitus and its association with the risk of pancreatic
carcinogenesis: a review. Korean J Gastroenterol. 67:168–177. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Guillaumond F, Leca J, Olivares O, Lavaut
MN, Vidal N, Berthezène P, Dusetti NJ, Loncle C, Calvo E, Turrini
O, et al: Strengthened glycolysis under hypoxia supports tumor
symbiosis and hexosamine biosynthesis in pancreatic adenocarcinoma.
Proc Natl Acad Sci USA. 110:3919–3924. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Rajeshkumar NV, Dutta P, Yabuuchi S, de
Wilde RF, Martinez GV, Le A, Kamphorst JJ, Rabinowitz JD, Jain SK,
Hidalgo M, et al: Therapeutic targeting of the Warburg effect in
pancreatic cancer relies on an absence of p53 function. Cancer Res.
75:3355–3364. 2015. View Article : Google Scholar : PubMed/NCBI
|