Introduction
Patients with esophageal cancer (EC), regardless of
histology (squamous or adenocarcinoma), have a poor prognosis, with
a reported 3-year overall survival rate of between 40 and 50%
(1). Despite recent advances in
radiation treatments and the field of medical oncology during
recent decades, the treatment of EC has not changed significantly,
and the results remain disappointing. The RTOG 85-01 trial
demonstrated that patients treated with chemoradiation have a
significantly better outcome compared with patients treated with
radiotherapy alone (2). At the same
time, the Intergroup 0123 (RTOG 9405) trial provided evidence that
dose escalation (increasing the dose from 50.4 to 64.8 Gy) has no
benefit in EC patients (3). The
reasons for these negative findings remain unclear, however, the
treatment-related toxicity (specifically lung toxicity) of the
higher dose may be the cause of the inferior prognosis of patients
randomized in the arm with a higher radiation dose. Moreover, the
CROSS trial showed the benefit of even lower doses of radiation
using 41.4 Gy in 23 fractions, administered with weekly carboplatin
and paclitaxel chemotherapy (4). As a
complete response is obtained in only ~30% of patients treated with
concomitant chemoradiation, subsequent esophagectomy appears to be
necessary (5). However, surgery alone
has conferred a worse outcome compared with tri-modality treatment
(6). Patient selection for this
treatment should be carefully performed, particularly with regard
to patient nutrition and performance status. Tri-modality
treatment, i.e., neoadjuvant chemoradiation followed by surgery,
represents the current standard of care for patients with localized
EC. However, this treatment is associated with significant
morbidity (7).
There are no clear recommendations regarding the
frequency and imaging techniques to be used during the follow-up of
EC patients following radical therapy. The monitoring strategies
range from tri-monthly upper gastrointestinal endoscopy together
with computed tomography (CT), to total omission of the follow-up,
referring the patients to a general practitioner and waiting for
clinically manifested disease relapse. There is no evidence of any
benefit of using imaging modalities, endoscopy or circulating tumor
markers for the follow-up of patients and a number of medical or
radiation oncologists have argued against the use of any follow-up
due to the extra cost, without any advantage of an early diagnosis
of EC recurrence. In fact, there is only limited evidence that
salvage treatments prolong patient survival (8).
The majority of EC patients following radical
therapy will eventually experience disease relapse. Several
treatment options are available for these patients. In the case of
local relapse in the esophagus, surgery represents a potentially
curative approach. Intraluminal brachytherapy and chemotherapy are
only palliative treatments (9).
Stenting is another effective method of palliation (10). If the tumor relapse occurs outside the
esophagus in the form of only limited oligometastatic disease, such
as occurs in the lymph nodes, then surgery or palliative
chemotherapy could again be considered. Radiotherapy using
conventional fractionation is frequently not feasible due to the
dose constraints after the primary neoadjuvant chemoradiation
(11). Subsequent to further
progression or in the case of metastatic disease when local therapy
is not possible, palliative chemotherapy based on cisplatin,
carboplatin, 5-fluorouracil or paclitaxel is another option
(12).
The use of stereotactic body radiotherapy (SBRT) is
rapidly expanding in the treatment of almost all tumor types and
anatomical regions. However, data for the use of SBRT in local EC
recurrence is currently missing (13,14). SBRT
utilizes a high-dose gradient drop off, a limited number of
fractions and a high dose per fraction, with a biological
equivalent dose usually exceeding 100 Gy. SBRT has the advantage of
a high probability of local tumor control and, at the same time, a
short treatment duration and limited toxicity, leaving the
palliative chemotherapy as an option for a subsequent line of
treatment following disease progression. Quality of life in EC
patients is extremely important and platinum-based chemotherapy
(cisplatin or carboplatin) poses a significant risk of toxicity.
The present study concerns the usage of SBRT in patients with the
recurrence of esophageal cancer and aims to demonstrate the
favorable safety and efficacy of the technique.
Patients and methods
Tumor volumes
For the purposes of conturing and treatment
planning, CTs with a 3-mm slide thickness were obtained for the two
patients. Involved lymph nodes were contoured as the gross tumor
volume (GTV). The clinical target volume (CTV) was identical to the
GTV, assuming no extranodal extension of the disease. The planning
target volume (PTV) was created by adding a 3-mm margin to the CTV
for possible intrafractional movements. The PTV margin was based on
institutional SBRT standards. A 3-point thermoplastic mask was
utilized for patient immobilization. Organs at risk (OAR; trachea,
major vessels and spinal cord) in the vicinity of the PTV were
contoured at least 1 cm above and below the PTV. The treatment plan
was prepared utilizing the Monaco® planning system
(Elekta Instrument AB, Stockholm, Sweden) using the Monte Carlo
calculation algorithm.
Plan evaluation
In the 2 patients, the local recurrence was outside
the high-dose region of previous radiotherapy (refining the high
dose as a region with a dose >30 Gy). For the treatment, Elekta
Synergy linear accelerators (Elekta Instrument AB) were employed
(6-MV photon beam, volumetric arc therapy technique). Doses of 30
Gy in the first case and 40 Gy in the second case were prescribed
in 5 daily fractions. Since no recommendations or any publications
exist regarding the dose for use in the lymph node recurrence of
EC, a dose was selected with respect to the dose constraints of
surrounding OARs. The dose gradient as a ratio of the volume of a
100 and 50% isodose was assessed (Paddick) (15), as well as the conformity index (ICRU
83) (16), defined as a ratio of the
volume of the 100% isodose and the volume of the PTV that received
the prescribed dose as recommended in ICRU 83. To confirm
appropriate patient immobilization and setup, three cone beam CTs
were utilized, two prior to and one subsequent to dose
delivery.
Results
A total of 2 patients with esophageal adenocarcinoma
and squamous cell carcinoma, respectively, who were initially
treated with concurrent chemoradiation (50 Gy in 25 fractions,
along with 3 cycles of cisplatin and 5-fluorouracil chemotherapy),
followed by esophagectomy in the first case and observation in the
second case, were enrolled in the present study. Surgery was not
completed for the second patient due to co-morbidities and a
complete response after the neoadjuvant treatment, as confirmed by
positron emission tomography combined with CT (PET/CT). Nodal
recurrences occurred in the neck region in each case. Disease
recurrence in the form of isolated nodal disease with no evidence
of other metastases was diagnosed in the 2 patients using PET/CT.
As PET/CT is not able to distinguish between the tumor and
inflammation, particularly in the case of lymph nodes in the head
and neck region where inflammatory lymph nodes are frequent
findings, and as the lymph nodes in the patients could not be
biopsied by fine-needle aspiration biopsy, a decision was made to
perform 3-deoxy-3-[18F]-fluorothymidine PET (FLT-PET). This
technique was used to aid the differential diagnosis, as it
exhibits a significantly higher positive predictive value for the
diagnosis of neoplasia compared with PET/CT. FLT-PET showed uptake
in the same lymph nodes, confirming the high suspicion for the
presence of metastatic disease. Each patient was discussed during
the multidisciplinary team meetings. Due to the significant risk of
surgery in each case, it was decided to proceed with SBRT. These
conclusions were discussed with the patients and the rationale,
practical aspects and potential side effects of radiotherapy were
explained to them. Written informed consent for SBRT and
publication of the present study was obtained from the two
patients. In total, 2 patients, 1 man and 1 woman aged 62 and 57
years, respectively, were treated at the University Hospital
Olomouc. Each patient completed the treatment with SBRT at the
beginning of 2016. For disease staging purposes, the TNM 7th
classification was utilized (17).
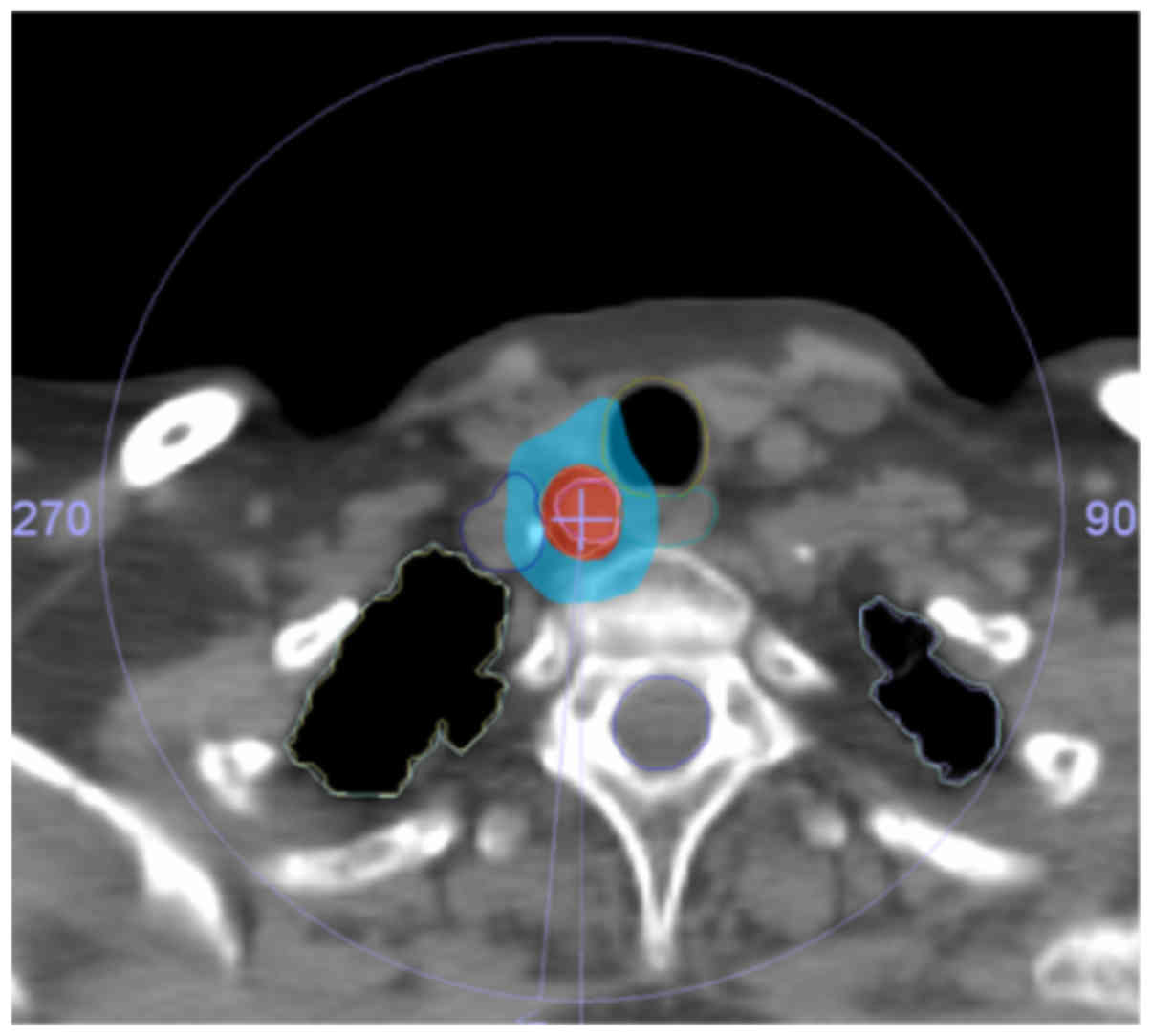
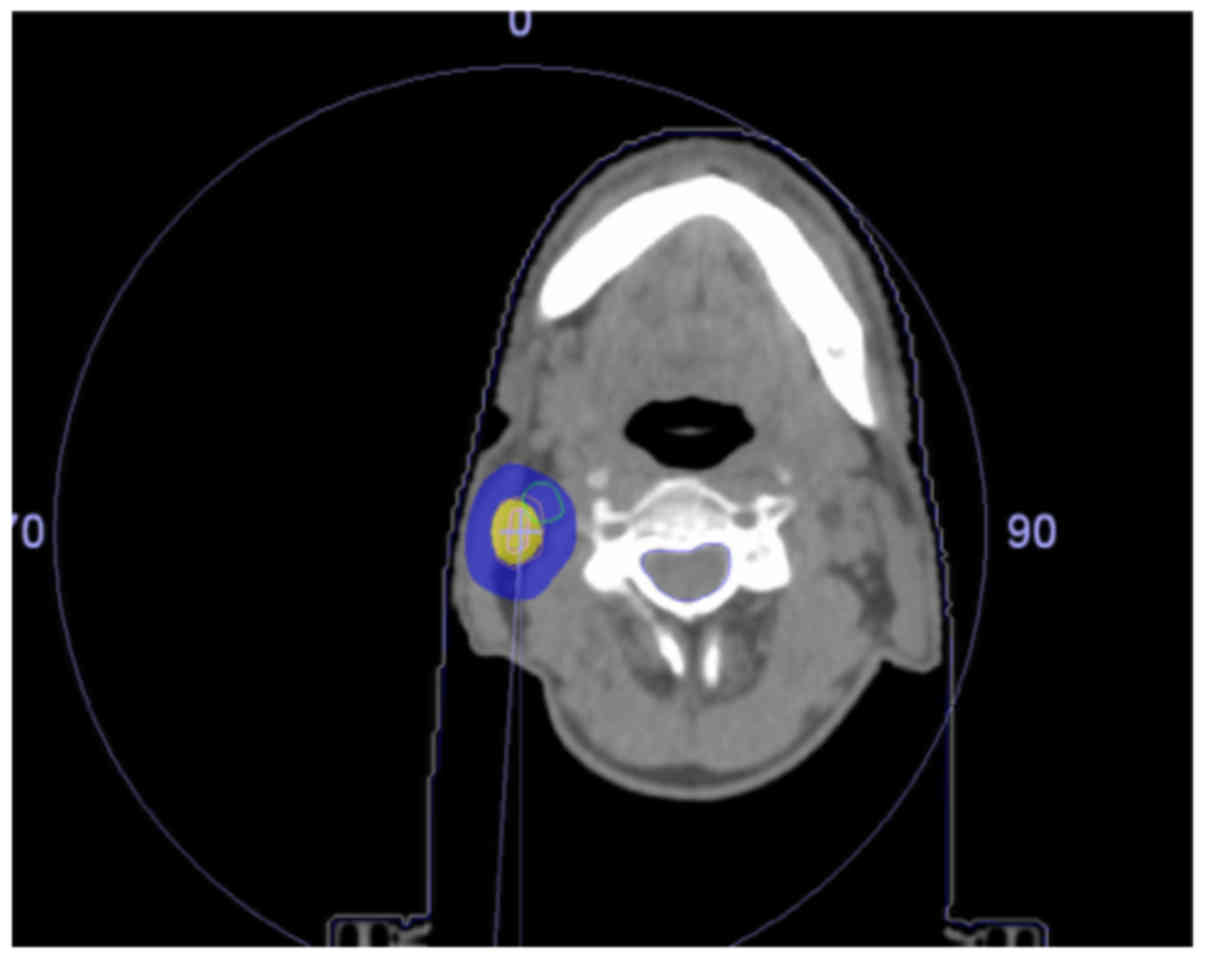
The patient characteristics are summarized in
Table I. The isodose distribution for
the treatment plans are presented in Figs.1 and 2,
and show 100 and 50% isodoses together with contours for the OAR.
Due to the location of the recurrences, the doses to the trachea,
major vessels and esophagus had to be assessed in the first
patient, while only the dose to the major blood vessels had to be
evaluated in the second patient. The maximum doses to the trachea,
the esophagus and the major vessels in the first patient were 32.6,
27.0 and 35.4 Gy, respectively, and the maximal dose to the major
blood vessels was 45.7 Gy in the second patient. The doses to the
spinal cord, brachial plexus and lungs were not significant for
either patient. The dose to the thyroid gland was not specifically
evaluated. The maximum dose was 45.9 Gy in patient 1 and 49.2 Gy in
patient 2. The treatment dose was delivered without any
unintentional treatment interruptions and the intrafractional
movements during all fractions of radiotherapy were under 3 mm,
indicating that a 3-point thermoplastic mask is appropriate for
patient immobilization during SBRT in the neck region. The patients
tolerated the treatment well and did not experience any significant
treatment-related toxicity during the follow-up.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristic | Patient 1 | Patient 2 |
|---|
| Age at diagnosis,
years | 57 | 62 |
| Primary tumor
staging | cT3cN0M0 | cTxcN1M0 |
| Histology | Squamous cell
carcinoma | Adenocarcinoma |
| Primary
treatment | Chemoradiotherapy
followed by surgery | Chemoradiotherapy
(surgery not indicated due to comorbidities) |
| Disease-free
interval, months | 18 | 21 |
| Site of
recurrence | Lower neck lymph
nodes | Neck lymph nodes |
| Number of fractions
of SBRT | 5 | 5 |
| Dose prescribed,
Gy | 30 | 40 |
| Prescription isodose,
% | 65 | 81 |
| Maximum dose, Gy | 45.9 | 49.2 |
| Dose gradient
(Paddick) | 0.17 | 0.12 |
| Conformity index
(ICRU 83) | 0.91 | 0.88 |
| Maximum dose to
trachea, Gy | 32.6 | Not applicable |
| Maximum dose to major
blood vessels, Gy | 35.4 | 45.7 |
| Maximum dose to
esophagus, Gy | 27 | Not applicable |
Discussion
The treatment options for patients with recurrent EC
are limited and the prognosis is poor, with expected survival
restricted to months rather than years. Evidence of any convincing
activity for a given therapeutic approach to support the selection
of an optimal treatment modality is mostly missing. Patient
performance status, co-morbidities and the patient's own preference
should be considered. In general, there are two treatment options
in a case of localized relapse, consisting of either surgical
removal of the tumor recurrence, which is often not feasible due to
previous radiotherapy and surgery, or systemic palliative
chemotherapy. Surgeons are frequently reluctant to attempt a
surgical resection in patients with recurrent EC due to the poor
prognosis. Chemotherapy based on the combination of cisplatin and
5-fluorouracil has a limited effect on the survival of patients
with EC, and the addition of taxanes, such as paclitaxel, has been
shown to not significantly affect the outcome (18). The targeted agents ramucirumab and
trastuzumab have been introduced into the therapy of patients with
metastatic adenocarcinoma of the gastroesophageal junction, but the
activity of these drugs is limited (19,20). The
data to support the use of immunotherapy in patients with
primary/recurrent EC is currently limited, although numerous trials
are ongoing. In the case of asymptomatic recurrence, there is also
an option to observe the patient and intervene at the time of the
manifestation of symptoms, taking into account the marginal
survival benefit of palliative treatment for recurrent disease.
However, this option may not be acceptable for a number of the
patients and their attending oncologists. The quality of life of
affected patients must always be one of the principal
considerations during the decision on the selection of an
appropriate treatment strategy.
SBRT utilizing conventional linear accelerators is a
rapidly evolving technique that, due to low toxicity and a short
overall treatment time, may be considered an ideal therapeutic
option for patients with a poor prognosis, such as those with
recurrent EC in whom the balance between quality of life and
treatment toxicity should be carefully weighed. The utilization of
SBRT has been widely reported in patients with primary lung cancer,
primary liver cancer and metastatic disease, and in individuals
with recurrences of gynecological tumors and brain metastases, with
SBRT quickly becoming a standard institutional treatment worldwide
(21–23). However, there are few studies
describing the use of SBRT in locally recurrent EC patients without
distant metastases, and further studies are required to clarify the
optimal treatment approach in this group of patients (24,25).
In conclusion, SBRT is a technically feasible and
safe option for patients with locally recurrent EC that provides
the possibility of local control and a good quality of life during
and after the treatment.
Acknowledgements
The study was supported by grant IGA_LF_2016_014,
provided by Palacky University (Olomouc, Czech Republic).
References
|
1
|
Koshy M, Greenwald BD, Hausner P, Krasna
MJ, Horiba N, Battafarano RJ, Burrows W and Suntharalingam M:
Outcomes after trimodality therapy for esophageal cancer: The
impact of histology on failure patterns. Am J Clin Oncol.
34:259–264. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cooper JS, Guo MD, Herskovic A, Macdonald
JS, Martenson JA Jr, Al-Sarraf M, Byhardt R, Russell AH, Beitler
JJ, Spencer S, et al: Chemoradiotherapy of locally advanced
esophageal cancer: Long-term follow-up of a prospective randomized
trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA.
281:1623–1627. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Minsky BD, Pajak TF, Ginsberg RJ, Pisansky
TM, Martenson J, Komaki R, Okawara G, Rosenthal SA and Kelsen DP:
INT 0123 (Radiation Therapy Oncology Group 94–05) phase III trial
of combined-modality therapy for esophageal cancer: High-dose
versus standard-dose radiation therapy. J Clin Oncol. 20:1167–1174.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shapiro J, van Lanschot JJ, Hulshof MC,
van Hagen P, van Berge Henegouwen MI, Wijnhoven BP, van Laarhoven
HW, Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, et al: Neoadjuvant
chemoradiotherapy plus surgery versus surgery alone for oesophageal
or junctional cancer (CROSS): Long-term results of a randomised
controlled trial. Lancet Oncol. 16:1090–1098. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Van Hagen P, Hulshof MC, van Lanschot JJ,
Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ,
Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, et al: Preoperative
chemoradiotherapy for esophageal or junctional cancer. N Engl J
Med. 366:2074–2084. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tepper J, Krasna MJ, Niedzwiecki D, Hollis
D, Reed CE, Goldberg R, Kiel K, Willett C, Sugarbaker D and Mayer
R: Phase III trial of trimodality therapy with cisplatin,
fluorouracil, radiotherapy, and surgery compared with surgery alone
for esophageal cancer: CALGB 9781. J Clin Oncol. 26:1086–1092.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hoeppner J, Zirlik K, Brunner T, Bronsert
P, Kulemann B, Sick O, Marjanovic G, Hopt UT and Makowiec F:
Multimodal treatment of locally advanced esophageal adenocarcinoma:
Which regimen should we choose? Outcome analysis of perioperative
chemotherapy versus neoadjuvant chemoradiation in 105 patients. J
Surg Oncol. 109:287–293. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ford HE, Marshall A, Bridgewater JA,
Janowitz T, Coxon FY, Wadsley J, Mansoor W, Fyfe D, Madhusudan S,
Middleton GW, et al: Docetaxel versus active symptom control for
refractory oesophagogastric adenocarcinoma (COUGAR-02): An
open-label, phase 3 randomised controlled trial. Lancet Oncol.
15:78–86. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Laskar SG, Lewis S, Agarwal JP, Mishra S,
Mehta S and Patil P: Combined brachytherapy and external beam
radiation: An effective approach for palliation in esophageal
cancer. J Contemp Brachytherapy. 7:453–461. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rabenstein T: Palliative endoscopic
therapy of esophageal cancer. Viszeralmedizin. 31:354–359. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim YS, Lee CG, Kim KH, Kim T, Lee J, Cho
Y and Koom WS: Re-irradiation of recurrent esophageal cancer after
primary definitive radiotherapy. Radiat Oncol J. 30:182–188. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ilson DH: Esophageal cancer chemotherapy:
Recent advances. Gastrointest Cancer Res. 2:85–92. 2008.PubMed/NCBI
|
|
13
|
Crane CH: Hypofractionated ablative
radiotherapy for locally advanced pancreatic cancer. J Radiat Res.
57:(Suppl 1). i53–i57. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pontoriero A, Iatì G, Aiello D and
Pergolizzi S: Stereotactic radiotherapy in the retreatment of
recurrent cervical cancers, assessment of toxicity, and treatment
response: Initial results and literature review. Technol Cancer Res
Treat. 15:759–765. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Paddick I and Lippitz B: A simple dose
gradient measurement tool to complement the conformity index. J
Neurosurg. 105:(Suppl). S194–S201. 2006.
|
|
16
|
International Commission on Radiation
Units and Measurements, . Prescribing, Recording and Reporting
Intensity-Modulated Photon-Beam Therapy (IMRT) (ICRU Report 83). J
ICRU. 10:1–10618. 2010.
|
|
17
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM Classification Of Malignant Tumours. 7th.
Wiley-Blackwell; pp. 62–66. 2009
|
|
18
|
Mizota A, Shitara K, Kondo C, Nomura M,
Yokota T, Takahari D, Ura T and Muro K: A retrospective comparison
of docetaxel and paclitaxel for patients with advanced or recurrent
esophageal cancer who previously received platinum-based
chemotherapy. Oncology. 81:237–242. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wilke H, Muro K, Van Cutsem E, Oh SC,
Bodoky G, Shimada Y, Hironaka S, Sugimoto N, Lipatov O, Kim TY, et
al: Ramucirumab plus paclitaxel versus placebo plus paclitaxel in
patients with previously treated advanced gastric or
gastro-oesophageal junction adenocarcinoma (RAINBOW): A
double-blind, randomised phase 3 trial. Lancet Oncol. 15:1224–1235.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bang YJ, Van Cutsem E, Feyereislova A,
Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T,
et al: Trastuzumab in combination with chemotherapy versus
chemotherapy alone for treatment of HER2-positive advanced gastric
or gastro-oesophageal junction cancer (ToGA): A phase 3,
open-label, randomised controlled trial. Lancet. 376:687–697. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kirichenko A, Gayou O, Parda D,
Kudithipudi V, Tom K, Khan A, Abrams P, Szramowski M, Oliva J,
Monga D, et al: Stereotactic body radiotherapy (SBRT) with or
without surgery for primary and metastatic liver tumors. HPB
(Oxford). 18:88–97. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Matzenauer M, Vrana D, Vlachova Z,
Cwiertka K, Kalita O and Melichar B: Radiotherapy management of
brain metastases using conventional linear accelerator. Biomed Pap
Med Fac Univ Palacky Olomouc Czech Repub. 160:412–416.
2016.PubMed/NCBI
|
|
23
|
Vrána D, Študentová H, Matzenauer M,
Vlachová Z, Cwierka K, Gremlica D and Kalita O: Treatment of brain
metastases of renal cell cancer with combined hypofractionated
stereotactic radiotherapy and whole brain radiotherapy with
hippocampal sparing. Oncology Lett. 11:3777–3781. 2016.
|
|
24
|
Santeufemia DA, Tumolo S, De Paoli A, Lo
Re G, Boz G, Miolo GM, Baresic T, Basso SM and Innocente R:
Chemo/tomotherapy stereotactic body radiation therapy (chemo/SBRT)
for the salvage treatment of esophageal carcinoma following
trimodality therapy: A case report. Tumori. 98:143e–145e.
2012.PubMed/NCBI
|
|
25
|
Russo JK and Rosen L: TomoTherapy
stereotactic body radiation therapy (SBRT) for the salvage
treatment of locally recurrent esophageal adenocarcinoma following
trimodality therapy: A case report. Tumori. 97:406–410.
2011.PubMed/NCBI
|