Introduction
The occurrence of cancer is increasing in
association with the prevalence of established risk factors such as
smoking, obesity and life style (1).
In 2012, ~14.1 million incident cancer cases and 8.2 million
mortalities occurred worldwide (1).
Lung cancer is the leading cause of cancer mortality in developed
countries. In 2015, 221,200 incident cases of lung and bronchial
cancer were estimated to be diagnosed and 158,040 mortalities were
estimated to occur in the United States (2). Non-small cell lung cancer (NSCLC) is
currently defined by pathological characteristics (3,4). NSCLC
represents >85% incidences of lung cancer, for which the
predicted 5-year survival rate is 15.9% and recurrence rates remain
high at 30–50% (5). NSCLC is
classified into two major histological phenotypes: Adenocarcinoma
(ADC; ~50%) and squamous cell carcinoma (SCC; ~40%). ADCs generally
arise in the distal airways, whereas SCCs arise in the proximal
airways. Conversely, SCCs are more closely associated with
cigarette smoking and chronic inflammation compared with ADCs
(3,4).
A number of complex somatic alterations that extend beyond protein
kinase activity to include transcription factors, epigenetic
modifiers, and splicing variants were recently reported in NSCLCs
(5–8).
When somatic point mutations were analyzed using whole-exome
sequence across 21 different tumor types, the mutation frequency in
lung SCC and ADC ranked second and third highest, respectively
(9). Additionally, heterogeneity of
tumor microenvironments, such as tumor-associated macrophages and
neutrophils, are associated with poor prognosis in NSCLC (10–12).
Therefore, tumor heterogeneity provides explanation for poor
responses to treatment of NSCLC.
The CD117 gene, termed c-Kit, encodes a tyrosine
kinase growth factor receptor for stem cell factor (SCF), and has
been extensively examined in hematopoietic stem cells (13). CD117 reportedly serves an important
oncogenic role in solid tumors including gastrointestinal stromal
tumors (GISTs) (14). Notably, it has
been reported that CD117 expression was observed in small cell lung
cancer (SCLC), and this molecule is associated with therapeutic and
prognostic consequences in patients with SCLC (15,16). Based
on these findings, STI-571 (imatinib), which blocks the
phosphorylation of the CD117 tyrosine kinase, has been developed
and used for patients with GISTs. Additionally, it has been
demonstrated that STI-571 demonstrates inhibitory effects on SCLC
cell lines (17,18). The overexpression of CD117 has been
observed in NSCLC tumors (19,20),
suggesting that CD117 may be a therapeutic target in a subset of
NSCLCs. In addition, CD117-positive NSCLC cells reportedly exhibit
cancer stem cell (CSC) characteristics including self-renewal and
chemoresistance (19). Previous
experimental evidence suggests that the presence of CSCs may be
associated with the prognosis of the patient in various types of
tumor (21,22). In the present study, it was
hypothesized that if CD117 possesses prognostic significance in the
patients with NSCLC, it may be used as a therapeutic target and
prognostic marker for patients with NSCLC. To confirm this
hypothesis, the association of CD117 expression with the
clinicopathological characteristics of NSCLC was examined.
Materials and methods
Patients and clinical specimens
Formalin-fixed paraffin embedded tissue samples of
NSCLC were obtained from 99 patients who were admitted to Tottori
University Hospital (Yonago, Japan) between January 2005 and
December 2007 and underwent curative surgical resection subsequent
to informed consent. Detailed clinicopathological characteristics
for these patients are summarized in Table I. The present study followed the
principles of the Declaration of Helsinki and was approved by the
ethics committees of Tottori University Faculty of Medicine
(Yonago, Japan; approval no. 1830).
 | Table I.Clinicopathological factors of
patients with lung cancer. |
Table I.
Clinicopathological factors of
patients with lung cancer.
| Characteristics | n |
|---|
| No. of patients | 99 |
| Age (year) | 69 (26–81) |
| Gender |
|
|
Male/female | 59/40 |
| Maximum tumor size
(mm) | 26 (11–82) |
| Lymph node
metastasis |
|
|
Negative/positive | 77/22 |
| Pleural invasion |
|
|
Negative/positive | 73/26 |
| Lymphatic
invasion |
|
|
Negative/positive | 26/73 |
| Venous invasion |
|
|
Negative/positive | 51/48 |
| Pathological
stage |
|
| Stage
I/Stage II/Stage III | 73/14/12 |
| Differentiation |
|
|
Well/moderate/poor | 21/69/9 |
| Histological
type |
|
|
Ad/Sq | 73/26 |
| Recurrence |
|
|
Negative/positive | 85/14 |
| Overall survival
(month) | 72 (2–104) |
| Relapse-free survival
(month) | 66 (2–104) |
Immunohistochemical analysis
All specimens from 99 patients with NSCLC were fixed
in 10% neutrally buffered formalin and embedded in paraffin. The
fixed tissue sections of 3-µm thickness were deparaffinized and
treated with 3% hydrogen peroxide solution to block endogenous
peroxidase activity. Subsequently, the sections were treated in
sodium citrate buffer (pH 6.0) using a 500-watt microwave oven for
12 min to improve the antigen retrieval. Subsequent to cooling to
room temperature, the specimens were incubated for 1 h at 37°C with
anti-CD117 monoclonal antibody (cat. no. ab32363; clone YR145;
dilution, 1:250; Abcam, Cambridge, MA, USA). The sections were
treated for 30 min at room temperature with biotinylated
anti-rabbit immunoglobulin G (IgG) antibody (cat. no. BA-1000;
dilution, 1:200; Vector Laboratories, Inc., Burlingame, CA, USA)
and then incubated for 30 min at 37°C with
streptavidin-biotinylated horseradish peroxidase complex (cat. no.
SA-5004; dilution, 1:500; Vector Laboratories, Inc.). Color
development was achieved by the treatment with ImmPACT DAB
Substrate (Vector Laboratories, Inc.) and counterstained with
hematoxylin. Images were acquired using a Nikon Eclipse E800
upright microscope (Nikon Corporation, Tokyo, Japan). The results
were evaluated by a pathologist who was blinded with respect to the
clinicopathological characteristics. The stained samples were
classified into the following two groups: The positive group, which
was defined as the samples with the cell membrane expression of
CD117; and the negative group, which was defined as the samples
with no expression or cytoplasmic expression of CD117.
Statistical analysis
Microsoft Excel 2013 (Microsoft Corporation,
Redmond, WA) and SPSS statics (version 22.0; SPSS, Inc., Chicago,
IL, USA) were used for the statistical calculations. A
χ2 test was performed to calculate the association
between CD117 expression and the clinicopathological factors in
patients with lung cancer. A univariable analysis using the
log-rank test was performed to compare the overall survival ratio
and disease free survival ratio in patients with lung cancer. A Cox
regression model was used for the multivariable analysis. P<0.05
were considered to indicate a statistically significant
difference.
Results
Clinicopathological features
The clinicopathological features of 99 patients
enrolled in the present study are summarized in Table I. All patients were classified into
two groups based on histology: ADC, 73 patients, and SCC, 26
patients. Of those patients, 14 patients relapsed. The median
overall survival and relapse-free survival were 72 (range 2–104)
months and 66 (range 2–104) months in patients with ADC and SCC,
respectively.
Expression of CD117 in NSCLC
patients
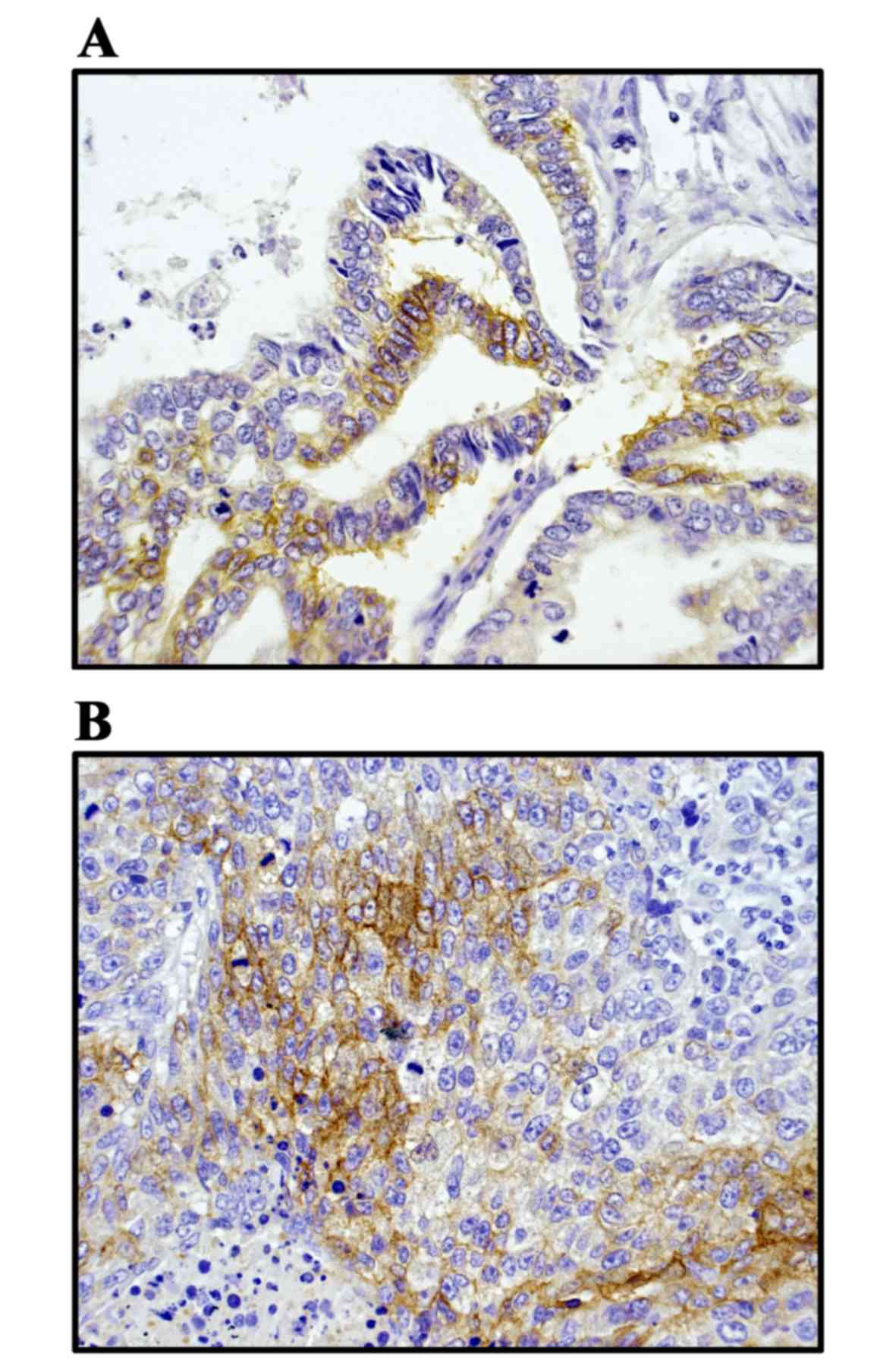
Immunohistochemical staining of CD117 expressions in
99 patients with NSCLC was performed. The representative images of
CD117 expression in formalin-fixed paraffin-embedded sections are
demonstrated in Fig. 1. Positive
expression of CD117 in lung ADC and SCC tissues are illustrated in
Fig. 1A and B, respectively. CD117
was expressed mainly on the cell membrane and occasionally in the
cytoplasm of cancer cells.
Association of CD117 expression with
clinicopathological features
The CD117 protein expression was positive in 17
cases, whereas it was negative in 82 cases, as summarized in
Table II. The result from
clinicopathological analysis revealed that CD117 positivity is
significantly associated with gender and recurrence rate. The
positivity of CD117 expression was higher in males compared with
females (P<0.05) and was also higher in recurrent patients
compared with non-recurrent patients (P<0.001). Notably, 50% of
recurrent patients exhibited CD117 positivity. Meanwhile, CD117
positivity was not associated with age, tumor size, pleural
effusion, venous invasion, pathological stage, histological type or
differentiation.
| Table II.χ2 test of
clinicopathological factors and CD117 expression. |
Table II.
χ2 test of
clinicopathological factors and CD117 expression.
|
| Sample size (%) |
|
|---|
|
|
|
|
|---|
| Characteristics | CD117- | CD117+ | P-value |
|---|
| Age (years) |
|
| 0.957 |
| ≤69 | 44 (44.4) | 9 (9.1) |
|
>69 | 38 (38.4) | 8 (8.1) |
| Gender |
|
| 0.036 |
| Male | 45 (45.5) | 14 (14.1) |
|
Female | 37 (37.4) | 3 (3.0) |
| Maximum tumor
size |
|
| 0.897 |
|
≤26 | 42 (42.4) | 9 (9.1) |
|
>26 | 40 (40.4) | 8 (8.1) |
| Lymph node
metastasis |
|
| 0.254 |
|
Negative | 62 (62.6) | 15 (15.2) |
|
Positive | 20 (20.2) | 2 (2.0) |
| Pleural
invasion |
|
| 0.746 |
|
Negative | 61 (61.6) | 12 (12.1) |
|
Positive | 21 (21.2) | 5 (5.1) |
| Lymphatic
invasion |
|
| 0.778 |
|
Negative | 22 (22.2) | 4 (4.0) |
|
Positive | 60 (60.6) | 13 (13.1) |
| Venous
invasion |
|
| 0.349 |
|
Negative | 44 (44.4) | 7 (7.1) |
|
Positive | 38 (38.4) | 10 (10.1) |
| Pathological
stage |
|
| 0.375 |
| Stage
I | 59 (59.6) | 14 (14.1) |
| Stage
II/III | 23 (23.2) | 3 (3.0) |
| Histological
type |
|
| 0.352 |
| Ad | 62 (62.6) | 11 (11.1) |
| Sq | 20 (20.2) | 6 (6.1) |
|
Differentiation |
|
| 0.693 |
|
Well | 18 (18.2) | 3 (3.0) |
|
Moderately/poorly | 64 (64.6) | 14 (14.1) |
| Recurrence |
|
| <0.001 |
|
Absence | 75 (75.8) | 10 (10.1) |
|
Presence | 7 (7.1) | 7 (7.1) |
Prognostic significance of CD117
expression in NSCLC patients
To investigate the association between
clinicopathological variables, including CD117 expression, and
prognosis of patients with NSCLC, a Kaplan-Meier analysis was
performed. As demonstrated in Table
III, the univariate analysis identified that overall survival
was associated with maximum tumor size (P=0.003), lymph node
metastasis (P<0.001), pleural effusion (P=0.015), venous
invasion (P=0.001), pathological stage (P<0.001),
differentiation (P=0.005) and recurrence (P<0.001). However,
overall survival was not associated with age, gender or CD117
expression. Additionally, the multivariate analysis showed that
only lymph node metastasis and recurrence were significantly
associated with overall survival (P<0.001, each), as illustrated
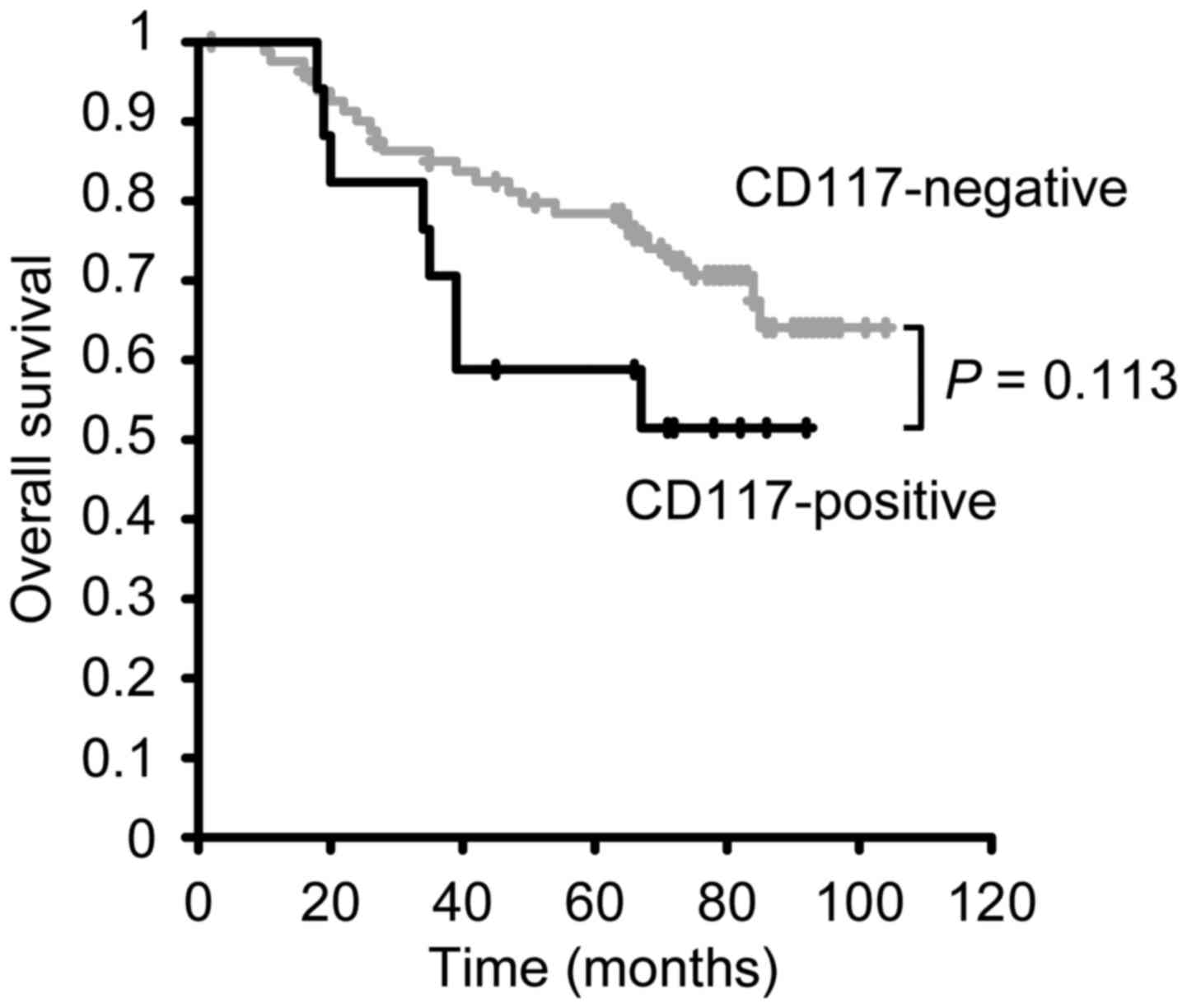
in Table III. When patients were
classified into CD117-negative and CD117-positive groups, the
Kaplan-Meier analysis for overall survival demonstrated that
patients with CD117-positive cell populations tended to exhibit
shorter overall survival rates compared with patients with
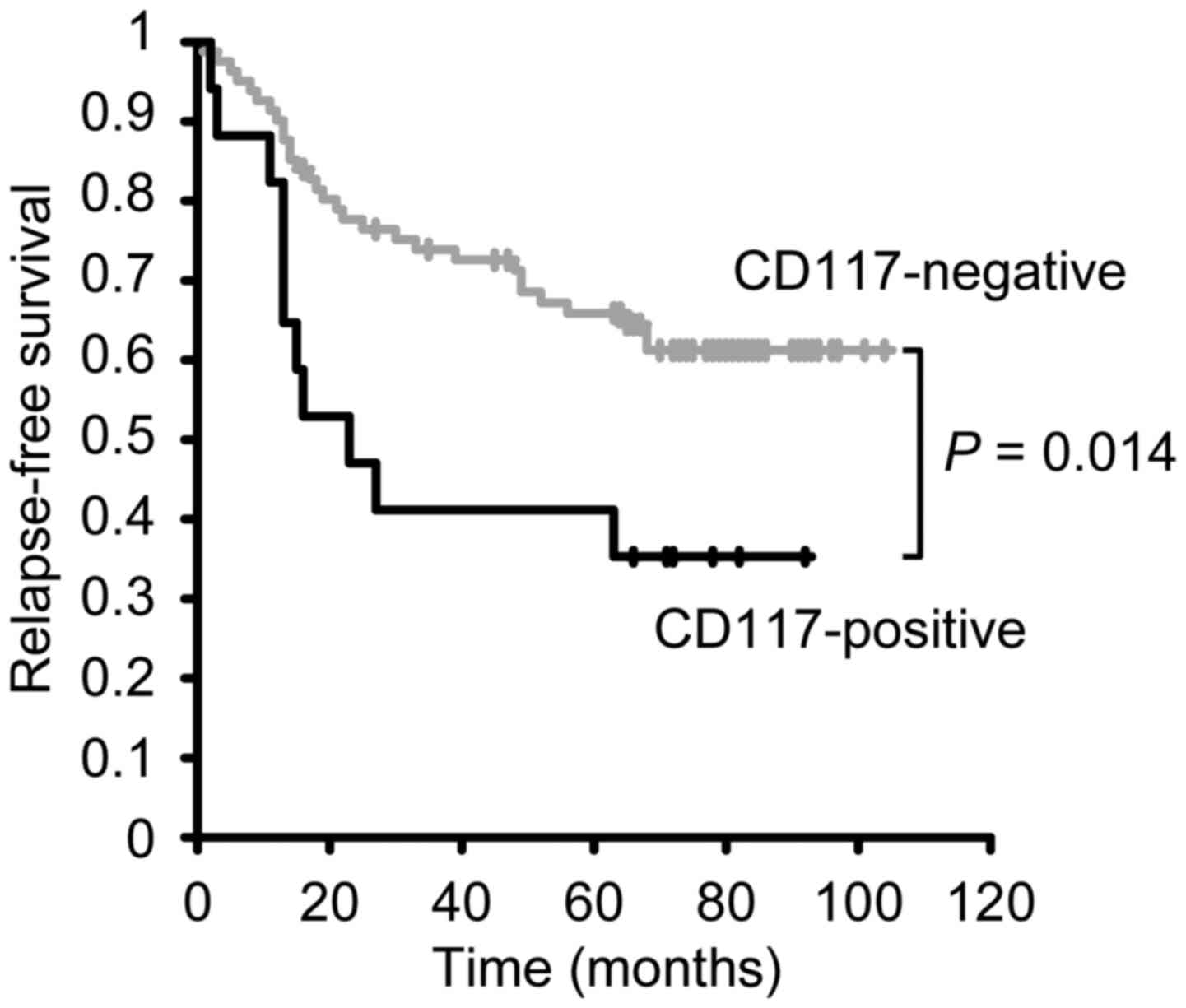
CD117-negative cell populations (P=0.113; Fig. 2). Additionally, the Kaplan-Meier
analysis for relapse-free survival was performed according to the
expression of CD117 and revealed that patients with CD117-positive
cell populations exhibited significantly shorter survival rates
compared with patients with CD117-negative cell populations
(P=0.014; Fig. 3). In addition to
CD117 expression, the following clinicopathological variables were
associated with relapse-free survival: Maximum tumor size
(P<0.001), lymph node metastasis (P<0.001), pleural effusion
(P=0.002), venous invasion (P<0.001), pathological stage
(P<0.001) and differentiation (P<0.001), as summarized in
Table IV. The multivariable analysis
revealed that relapse-free survival was significantly associated
with venous invasion (P<0.001), pathological stage (P=0.001) and
CD117 expression (P=0.002). These findings suggest that CD117
expression is an independent factor for predicting relapse-free
survival and may serve as a prognostic marker for tumor recurrence
and survival in patients with NSCLC.
| Table III.Univariate and multivariate analysis
of clinical variables associated with overall survival in patients
with lung cancer. |
Table III.
Univariate and multivariate analysis
of clinical variables associated with overall survival in patients
with lung cancer.
|
|
| Univariate | Multivariate
univariate |
|---|
|
|
|
|
|
|---|
|
Characteristics | Category | P-value | HR (95% CI) | P-value |
|---|
| Age | ≤69 vs. >69 |
0.172 |
|
|
| Gender | Male vs.
Female |
0.596 |
|
|
| Maximum tumor
size | ≤26 vs. >26 |
0.003 |
|
|
| Lymph node
metastasis | Negative vs.
Positive | <0.001 | 4.055
(2.004–8.004) | <0.001 |
| Pleural
invasion | Negative vs.
Positive |
0.015 |
|
|
| Venous
invasion | Negative vs.
Positive |
0.001 |
|
|
| Pathological
stage | Stage I vs. Stage
II/III | <0.001 |
|
|
|
Differentiation | Well vs.
Moderate/Poor |
0.005 |
|
|
| Recurrence | Negative vs.
Positive | <0.001 | 4.672
(2.264–9.264) | <0.001 |
| CD117
expression | Negative vs.
Positive |
0.113 |
|
|
| Table IV.Univariate and multivariate analysis
of clinical variables associated with relapse-free survival in
patients with lung cancer. |
Table IV.
Univariate and multivariate analysis
of clinical variables associated with relapse-free survival in
patients with lung cancer.
|
|
| Univariate | Multivariate
univariate |
|---|
|
|
|
|
|
|---|
|
Characteristics | Category | P-value | HR (95% CI) | P-value |
|---|
| Age | ≤69 vs. >69 |
0.213 |
|
|
| Gender | Male vs.
Female |
0.458 |
|
|
| Maximum tumor
size | ≤26 vs. >26 | <0.001 |
|
|
| Lymph node
metastasis | Negative vs.
Positive | <0.001 |
|
|
| Pleural
invasion | Negative vs.
Positive |
0.002 |
|
|
| Venous
invasion | Negative vs.
Positive | <0.001 | 4.596
(2.053–10.053) | <0.001 |
| Pathological
stage | Stage I vs. Stage
II/III | <0.001 | 3.347
(1.685–6.685) |
0.001 |
|
Differentiation | Well vs.
Moderate/Poor | <0.001 |
|
|
| CD117
expression | Negative vs.
Positive |
0.014 | 3.352
(1.583–7.583) |
0.002 |
Discussion
In the present study, the patients with
CD117-positive expression in NSCLC tissues exhibited significantly
shorter relapse-free survival compared with patients with
CD117-negative expression. This is the first report that CD117
expression may be a predictive marker for poor prognosis in the
patients with NSCLC. CD117 expression in a subset of patients with
NSCLC was not predictive of overall survival (20), which is in agreement with the present
study due to the small number of patients enrolled. However, the
present study demonstrates that CD117 expression is associated with
the relapse-free survival. Additionally, the combined treatment of
cisplatin with imatinib or anti-SCF antibody reportedly inhibits
the growth of NSCLC cells (19).
These findings are similar to the reports that CD117 expression is
associated with poor prognosis in SCLC (15,16). Taken
together, these data suggest that the SCF/CD117 axis is a
therapeutic target of a subset of lung cancer cells, and the
inhibition of this signaling pathway may improve the efficacy of
chemotherapy in lung cancer.
The majority of solid tumors are composed of a
heterogeneous population including cells characterized by capacity
for differentiation, self-renewal and resistance to chemotherapy,
and radiotherapy (23,24). Although ~20% of patients with NSCLC
exhibited surgically-correctable tumors at presentation, the
recurrence rates following surgery remain high at 30–50% (25). This indicates that there is minimal
residual disease, which contains a population that possesses a high
proliferative potential and self-renewal capacity. To delay or
prevent tumor recurrence in lung cancer, there should be a focus on
the stem-like cells present. Some CSC markers have been identified
in lung cancer, including a subset of keratin 14-expressing
progenitor epithelial cells, which are involved in airway
epithelial repair subsequent to injury, were reported to be
tumor-initiating cells in the subgroup of smokers with NSCLC
(26). Additionally, CD133-positive
lung cancer cells exhibited CSC-like features, such as increased
tumorigenic potential and higher sphere-forming ability (27,28). CD133
expression in NSCLC represents an anticancer drug resistance
phenotype and evidence of metastatic cells, but does not correlate
with the survival of patients with NSCLC (29). Conversely, another study suggests that
CD133 expression is a temporary marker of CSCs in SCLC but not in
NSCLC (30). CSC populations isolated
from NSCLC cell lines were reported to express SCF and CD117 in an
autocrine fashion (19). Although
cisplatin treatment did not eliminate CSCs from NSCLC cells,
inhibition of the SCF-CD117 axis by imatinib or anti-SCF antibody
suppressed CSC proliferation (19),
which suggests that this signaling pathway serves an important role
in lung CSCs maintenance and survival. In the present study,
CD117-positivity was associated with relapse-free survival, but not
with overall survival, suggesting that CD117-positive cells may
exhibit some CSC characteristics. Additional research is required
to demonstrate that the acquisition of cancer stemness in NSCLC
cells is associated with poor prognosis in patients with NSCLC.
In conclusion, the present study demonstrated that
the positive expression of CD117 is significantly associated with a
shorter relapse-free survival rate in patients with NSCLC. This
observation suggests that CD117 may serve as a prognostic marker
for predicting poor prognoses and a novel therapeutic target for
patients with NSCLC.
Acknowledgements
The present study was supported by Management
Expenses Grants from Ministry of Education, Culture, Sports,
Science and Technology in Japan.
Glossary
Abbreviations
Abbreviations:
|
NSCLC
|
non-small cell lung cancer
|
|
SCLC
|
small cell lung cancer
|
|
CSC
|
cancer stem cell
|
|
ADC
|
adenocarcinoma
|
|
SCC
|
squamous carcinoma
|
|
SCF
|
stem cell factor
|
|
GISTs
|
gastrointestinal stromal tumors
|
|
IgG
|
immunoglobulin G
|
|
K14
|
keratin 14
|
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ettinger DS, Wood DE, Akerley W, Bazhenova
LA, Borghaei H, Camidge DR, Cheney RT, Chirieac LR, D'Amico TA,
Demmy TL, et al: Non-small cell lung cancer, version 6.2015. J Natl
Compr Canc Netw. 13:515–524. 2015.PubMed/NCBI
|
|
3
|
Langer CJ, Besse B, Gualberto A, Brambilla
E and Soria JC: The evolving role of histology in the management of
advanced non-small-cell lung cancer. J Clin Oncol. 28:5311–5320.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Davidson MR, Gazdar AF and Clarke BE: The
pivotal role of pathology in the management of lung cancer. J
Thorac Dis. 5:(Suppl 5). S463–S478. 2013.PubMed/NCBI
|
|
5
|
Chen Z, Fillmore CM, Hammerman PS, Kim CF
and Wong KK: Non-small-cell lung cancers: A heterogeneous set of
diseases. Nat Rev Cancer. 14:535–546. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cancer Genome Atlas Research Network.
Comprehensive genomic characterization of squamous cell lung
cancers. Nature. 489:519–525. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kandoth C, McLellan MD, Vandin F, Ye K,
Niu B, Lu C, Xie M, Zhang Q, McMichael JF, Wyczalkowski MA, et al:
Mutational landscape and significance across 12 major cancer types.
Nature. 502:333–339. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cancer Genome Atlas Research Network.
Comprehensive molecular profiling of lung adenocarcinoma. Nature.
511:543–550. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lawrence MS, Stojanov P, Mermel CH,
Robinson JT, Garraway LA, Golub TR, Meyerson M, Gabriel SB, Lander
ES and Getz G: Discovery and saturation analysis of cancer genes
across 21 tumour types. Nature. 505:495–501. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bellocq A, Antoine M, Flahault A, Philippe
C, Crestani B, Bernaudin JF, Mayaud C, Milleron B, Baud L and
Cadranel J: Neutrophil alveolitis in bronchioloalveolar carcinoma:
Induction by tumor-derived interleukin-8 and relation to clinical
outcome. Am J Pathol. 152:83–92. 1998.PubMed/NCBI
|
|
11
|
Murdoch C, Muthana M, Coffelt SB and Lewis
CE: The role of myeloid cells in the promotion of tumour
angiogenesis. Nat Rev Cancer. 8:618–631. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Houghton AM, Rzymkiewicz DM, Ji H, Gregory
AD, Egea EE, Metz HE, Stolz DB, Land SR, Marconcini LA, Kliment CR,
et al: Neutrophil elastase-mediated degradation of IRS-1
accelerates lung tumor growth. Nat Med. 16:219–223. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yarden Y, Kuang WJ, Yang-Feng T, Coussens
L, Munemitsu S, Dull TJ, Chen E, Schlessinger J, Francke U and
Ullrich A: Human proto-oncogene c-kit: A new cell surface receptor
tyrosine kinase for an unidentified ligand. EMBO J. 6:3341–3351.
1987.PubMed/NCBI
|
|
14
|
Hirota S: Gastrointestinal stromal tumors:
Their origin and cause. Int J Clin Oncol. 6:1–5. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Naeem M, Dahiya M, Clark JI, Creech SD and
Alkan S: Analysis of c-kit protein expression in small-cell lung
carcinoma and its implication for prognosis. Hum Pathol.
33:1182–1187. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Micke P, Basrai M, Faldum A, Bittinger F,
Rönnstrand L, Blaukat A, Beeh KM, Oesch F, Fischer B, Buhl R and
Hengstler JG: Characterization of c-kit expression in small cell
lung cancer: Prognostic and therapeutic implications. Clin Cancer
Res. 9:188–194. 2003.PubMed/NCBI
|
|
17
|
Krystal GW, Honsawek S, Litz J and
Buchdunger E: The selective tyrosine kinase inhibitor STI571
inhibits small cell lung cancer growth. Clin Cancer Res.
6:3319–3326. 2000.PubMed/NCBI
|
|
18
|
Wang WL, Healy ME, Sattler M, Verma S, Lin
J, Maulik G, Stiles CD, Griffin JD, Johnson BE and Salgia R: Growth
inhibition and modulation of kinase pathways of small cell lung
cancer cell lines by the novel tyrosine kinase inhibitor STI 571.
Oncogene. 19:3521–3528. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Levina V, Marrangoni A, Wang T, Parikh S,
Su Y, Herberman R, Lokshin A and Gorelik E: Elimination of human
lung cancer stem cells through targeting of the stem cell
factor-c-kit autocrine signaling loop. Cancer Res. 70:338–346.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Donnenberg AD, Zimmerlin L, Landreneau RJ,
Luketich JD and Donnenberg VS: KIT (CD117) expression in a subset
of non-small cell lung carcinoma (NSCLC) patients. PloS One.
7:e528852012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yang F, Cao L, Sun Z, Jin J, Fang H, Zhang
W and Guan X: Evaluation of breast cancer stem cells and intratumor
stemness heterogeneity in triple-negative breast cancer as
prognostic factors. Int J Biol Sci. 12:1568–1577. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Song W, Li H, Tao K, Li R, Song Z, Zhao Q,
Zhang F and Dou K: Expression and clinical significance of the stem
cell marker CD133 in hepatocellular carcinoma. Int J Clin Pract.
62:1212–1218. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hassan HT: c-Kit expression in human
normal and malignant stem cells prognostic and therapeutic
implications. Leuk Res. 33:5–10. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Alamgeer M, Peacock CD, Matsui W, Ganju V
and Watkins DN: Cancer stem cells in lung cancer: Evidence and
controversies. Respirology. 18:757–764. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kelsey CR, Marks LB, Hollis D, Hubbs JL,
Ready NE, D'Amico TA and Boyd JA: Local recurrence after surgery
for early stage lung cancer: An 11-year experience with 975
patients. Cancer. 115:5218–5227. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ooi AT, Mah V, Nickerson DW, Gilbert JL,
Ha VL, Hegab AE, Horvath S, Alavi M, Maresh EL, Chia D, et al:
Presence of a putative tumor-initiating progenitor cell population
predicts poor prognosis in smokers with non-small cell lung cancer.
Cancer Res. 70:6639–6648. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bertolini G, Roz L, Perego P, Tortoreto M,
Fontanella E, Gatti L, Pratesi G, Fabbri A, Andriani F, Tinelli S,
et al: Highly tumorigenic lung cancer CD133+ cells display
stem-like features and are spared by cisplatin treatment. Proc Natl
Acad Sci USA. 106:16281–16286. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Eramo A, Lotti F, Sette G, Pilozzi E,
Biffoni M, Di Virgilio A, Conticello C, Ruco L, Peschle C and De
Maria R: Identification and expansion of the tumorigenic lung
cancer stem cell population. Cell Death Differ. 15:504–514. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Salnikov AV, Gladkich J, Moldenhauer G,
Volm M, Mattern J and Herr I: CD133 is indicative for a resistance
phenotype but does not represent a prognostic marker for survival
of non-small cell lung cancer patients. Int J Cancer. 126:950–958.
2010.PubMed/NCBI
|
|
30
|
Cui F, Wang J, Chen D and Chen YJ: CD133
is a temporary marker of cancer stem cells in small cell lung
cancer, but not in non-small cell lung cancer. Oncol Rep.
25:701–708. 2011.PubMed/NCBI
|