Introduction
Hepatocellular carcinoma (HCC) is one of the most
common malignancies in the world, with high incidence and mortality
rates (1). Statistically among
patients with HCC, males account for a higher proportion than
females, and HCC is now the second leading cause of
cancer-associated mortality worldwide in men (1). Globally, ~50% of patients with HCC are
from China (1), where HCC occupies
the third reason for cancer-associated mortality (2). In China, the leading cause of HCC
(>80%) is infection with hepatitis B virus (HBV) (3). As the patients with HCC are often
diagnosed at an advanced stage, the majority of them are not able
to receive curative therapies, including ablation, transplant and
surgery. Although novel antitumor agents and clinical trials
frequently emerge, the overall survival of the patients with HCC at
advanced stage remains poor, and the life expectancy is too short
to assess the effectiveness of novel anticancer agents (4–7). Life
expectancy >3 months is an inclusion criterion for the majority
of systemic drug trials in advanced HCC (4,5).
Eligibility for clinical trials is usually determined by Child-Pugh
score and performance status (4,5).
Alternative staging systems may be better at predicting survival
and selecting patients for clinical trials in advanced HCC
(7,8).
Clinical staging aims to predict survival outcomes
and assist in deciding the optimal therapeutic options for patients
with cancer. However, HCC differs from other types of cancer in
that its prognosis and treatment depend on two aspects: The tumor
burden and liver function (6–9). Previous studies have developed staging
systems that include these two features (6–11). Over
previous decades, a number of staging systems have been developed
based on specific populations of local regions (10–14).
Numerous studies have attempted to identify a universally accepted
staging system and prognosis assessment of HCC remains
controversial (6–11,15). It
appears that different staging systems possess particular
applicability among different groups of patients with HCC (10–14).
Existing data provide a small amount of information (15) regarding which staging system is the
most suitable candidate to accurately predict the prognosis of the
patients with advanced HCC, which would assist clinicians in
recruiting the appropriate candidates for clinical trials. In a
previous study, Xing et al (12) revealed that the Advanced Liver Cancer
Prognostic System (ALCPS) was the optimal staging system for
predicting 3-month and overall survival rates among 12 systems
analyzed. However, ALCPS is too complicated for clinical use. The
ALCPS was based on 11 prognostic factors with different weights:
Ascites; abdominal pain; weight loss; Child-Pugh class; alkaline
phosphatase; total bilirubin; α-fetoprotein (AFP); urea; portal
vein thrombosis; tumor size; and presence of lung metastases
(16). HCC patients were scored and
classified into 3 groups: Good risk (0–8); intermediate risk
(9–15); and poor risk (>15). It is difficult
to keep in mind all the factors and the scores. Zhang et al
(13) suggested that CUPI was the
optimal staging system in predicting survival in patients with
unresectable HCC. In the study by Zhang et al, 89% of
subjects were infected with HBV, 3% of subjects were infected with
HCV and 2% of subjects developed HCC due to alcohol (13). As no consensus currently exists, the
present study aimed to identify the best staging system for use in
clinical trials in China, by restricting the subjects to only
patients with HBV-associated advanced HCC without any antitumor
therapy. The results of the present study will assist patients and
their doctors to gain insight into the natural history of untreated
HCC, which will aid clinicians in making decisions of whether to
accept other palliative treatments.
In the present study, the ability of seven different
staging systems to predict 3- and 6-month and cumulative survival
rates of patients with advanced HBV-associated HCC was evaluated.
This large cohort of patients from The Third Affiliated Hospital of
Sun Yat-sen University (SYSU) in Guangzhou, China, will assist in
establishing the inclusion criteria for clinical trials in
China.
Patients and methods
Ethical approval
The present study was reviewed and approved by The
Third Affiliated Hospital of SYSU Institutional Review Board. All
study participants, or their legal guardian, provided written
informed consent prior to study enrollment. The technical appendix,
statistical code and full datasets are available from the
corresponding author. Participants provided informed consent for
data sharing. No additional data are available.
Patients
A total of 220 consecutive patients diagnosed with
advanced HBV-associated HCC between September 2008 and June 2010 at
The Third Affiliated Hospital of SYSU were retrospectively
collected and analyzed. Patients were included if they were
diagnosed with HCC and were hepatitis B surface antigen-positive.
According to American Association for the study of Liver diseases
guidelines (17), the diagnosis of
HCC was confirmed by biopsy, or based on the non-invasive criteria
which is only applicable to cirrhotic patients: In nodules >2
cm, one imaging technique demonstrating arterial hypervascularity
and venous/late phase washout. In nodules of between 1 and 2 cm,
two techniques with a high coincidence [computed tomography (CT),
contrast-enhanced ultrasound and magnetic resonance imaging (MRI)]
are required (17). Patients
diagnosed with advanced HBV-associated HCC belong to a
heterogeneous group with marked differences in median survival
ranges, from 1 month to >1.5 years. Patients included in the
present study belonged to Barcelona Clinic Liver Cancer (BCLC)
staging for hepatocellular carcinoma stages C and D (17). Specific patients with BCLC C and D
stage HCC in The Third Affiliated Hospital of SYSU also received
standard antitumor therapy and were excluded from the present
study, in order to study the natural history of advanced HCC.
Patients included in the present study did not receive any standard
antitumor therapy. The majority of patients with Cancer of the
Liver Italian Program (CLIP) 0, Okuda 0, Japan Integrated Staging
(JIS) 0 or 1 HCC exhibited treatable disease, but did not receive
antitumor treatment, partially due to lack of insurance coverage.
Certain patients rejected antitumor therapy, but received the best
supportive care and traditional Chinese herbal medicine. In the
present study, 82 patients were classified with BCLC D HCC. A total
of 24 patients survived >3 months, and these patients exhibited
improved prognosis compared with the other 58 patients, who
survived <3 months. Certain patients were classified with BCLC D
HCC due to a diagnosis of performance status (PS) 3–4 (18) at first diagnosis and following the
best supportive care, PS may improve. Patients with BCLC D were a
mixed group with different prognoses.
In the baseline evaluation, laboratory studies,
imaging studies (CT or MRI) and clinical examination were required.
Data were collected once the patients were diagnosed with advanced
HBV-associated HCC. The survival time was defined as the time from
diagnosed date to the date of mortality or last contact with
surviving patients.
Standard antitumor therapy refers to therapies
recommended by National Comprehensive Cancer Network guidelines,
including transplantation, surgery, transarterial chemoembolization
or percutaneous ethanol injection, chemotherapy or targeted therapy
(19). The patients in the present
study did not receive standard antitumor therapy as they were not
suitable for treatment, or they declined all therapeutic
options.
Patients lacking data required for any of the
studied staging systems or with prior malignancies or secondary
cancers were excluded. If they were lost to follow-up within 3
months of diagnosis, they were also excluded.
Data collection
Data acquisition from the electronic charts was
approved by the institutional ethics committee. Baseline data were
collected to classify patients according to the CLIP, CUPI,
tumor-node-metastasis (TNM), JIS, Okuda, China Integrated Score
(CIS) and BCLC systems.
JIS scores may be original or modified (11). In modified JIS scores, the ICGR15
value is used instead of hepatic encephalopathy, and the threshold
levels for prothrombin time is different from the Child-Pugh score.
As the indocyanine green retention test value is not routinely
examined in The Third Affiliated Hospital of SYSU, original JIS
scores were used in the present study. Original JIS scores used the
Child-Pugh score.
A range of demographic data was collected, including
risk factors, clinical data including performance status, imaging
data and liver cirrhosis manifestations.
In particular, the following variables were
retrieved for the analysis of the present study: Gender, age, date
of diagnoses and date of mortality or last follow-up, the general
condition of the patients (abdominal pain, weight loss).
Performance status (PS) was retrospectively assessed from the
clinical records (18). Tumor
characteristics were assessed via CT or MRI, including the diameter
of the largest lesion, the number of lesions, organ invasion, lymph
node status and portal vein thrombosis. Laboratory data were also
collected, including routine blood tests, liver function tests
[total bilirubin, albumin and γ-glutamyltranspeptidase (GGT)],
alkaline phosphatase (ALP), aspartate aminotransferase (AST), AFP
levels, blood urea nitrogen (BUN) and coagulation function
(prothrombin time/international normalized ratio values). A chest
X-ray was routinely performed for distant metastases. A brain CT
was performed if they had paralysis or terrible headache. Bone
Emission Computed Tomography was performed if they had bone pain or
bone mass.
Statistical analysis
The main endpoints of the present study were 3-month
survival and overall survival. The secondary endpoint was 6-month
survival. Kaplan-Meier estimator survival curves and log-rank tests
were used to compare overall survival rate predicted using
different staging systems.
Different staging systems consist of a different
number of stages. For example, CLIP includes 7 stages, JIS and CIS
include 6 stages, and Okuda and CUPI include only 3 stages.
Likelihood ratio tests (LRTs) were used to compare different
staging systems. The degree of freedom was set at 1, such that
different prognostic systems with different stages were able to be
compared. Akaike information criterion (AIC) values were also used
to avoid statistical bias. If the likelihood ratio value of a
staging system is higher and AIC value is lower compared with other
systems, it was considered to have an improved prognostic
ability.
Cox's proportional hazard model was used to identify
independent predictive variables of survival. Statistically
significant prognostic variables were identified in univariate
analyses. Subsequently, these variables were included in
multivariate analyses.
The sensitivity and specificity of the predictive
value each staging system for 3- and 6-month mortality were
analyzed by relative operating characteristic (ROC) curve analysis,
and the DeLong et al (12)
test was used to compare the area under curve (AUC) of the ROC
curves. A larger area indicated an improved discriminatory ability
in stratifying patients with different outcomes.
All the important prognostic factors for advanced
HCC were included in the univariate and multivariate analyses by
Cox's proportional hazard model. These factors included sex, age,
HBV status, PS, AFP, albumin, bilirubin, ALP, hemoglobin, hepatic
encephalopathy, fibrinogen, prothrombin time, ascites, weight loss,
abdominal pain, vascular involvement, tumor size, lymph node
status, metastases and Child-Pugh score.
All the analyses of the data were performed using
SPSS (version 20.0; IBM SPSS, Armonk, NY, USA), STATA (version
12.0; StataCorp LLC, College Station, TX, USA) and SAS (version
9.1.3; SAS Institute, Inc., Cary, NC, USA).
Results
Patient characteristics
All 220 patients included in the present study did
not receive antitumor treatment and were of Chinese ethnicity.
Patients were staged using CLIP, CUPI, TNM, JIS, Okuda, CIS and
BCLC systems. All authors were familiar with the seven staging
systems. Table I summarizes the
baseline characteristics of all patients. The patients included 198
(90%) males and 22 (10%) females. The median age of the patients
was 55.7 (range, 19–85 years). The 90-day survival rate was 45.5%
and the 6-month survival rate was 30.5%. All patients included were
HBV carriers. Of note, 57.7% of the patients were stage III and
20.9% of the patients were stage IV, based on TNM seventh edition
staging (19). A total of 28.6% of
the patients were Child-Pugh class C.
 | Table I.Baseline demographic characteristics
of study participants. |
Table I.
Baseline demographic characteristics
of study participants.
| Characteristic | Patients
(n=220) |
|---|
| Sex, % |
|
|
Male | 90 (198/220) |
|
Female | 10 (22/220) |
| Median age, years
(range) | 55.7 (19–85) |
| Etiology, % |
|
Hepatitis B surface antigen
(+) | 100 (220/220) |
| Tumor size, % |
|
| <2
cm | 8.2 (18/220) |
| 2–5
cm | 14.1 (31/220) |
| >5
cm | 77.7 (171/220) |
| Abdominal pain,
% | 43.6 (96/220) |
| Weight loss, % | 39.1 (86/220) |
| Ascites, % | 58.6 (129/220) |
| Encephalopathy,
% | 2.3 (5/220) |
| Karnofsky
performance status | 70 (20–90) |
| Portal vein
thrombosis, % | 68.2 (150/220) |
| Lung metastases,
% | 14.1 (31/220) |
| White blood cell
count (×109 cells/l) | 6.2
(1.84–25.09) |
| α-fetoprotein
(ng/ml) | 668.8
(1.0–21620.0) |
| Albumin (g/l) | 34.45
(13.6–51.8) |
| Creatinine
(µmol/l) | 68.77
(29.0–277.0) |
| Alkaline
phosphatase (U/l) | 145.5
(33.0–767.0) |
| Platelets
(×109 cells/l) | 137.0 (4–503) |
| Hemoglobin
(g/l) | 119.5
(56.0–177.0) |
| Fibrinogen
(g/l) | 2.91 (0.9–9.4) |
| Total bilirubin
(µmol/l) | 35.88
(4.69–864.86) |
| α-L-fucosidase
(U/l) | 27.0
(4.0–124.0) |
| AST (IU/l) | 141.0
(17.0–2218.0) |
|
γ-glutamyltranspeptidase (U/l) | 177.0
(17.0–1128.0) |
| Blood urea nitrogen
(mmol/l) | 5.27
(1.63–25.42) |
| PT, % | 76 (31–100%) |
| INR | 1.19
(0.85–2.53) |
| 90-day survival
rate, % | 45.5 (100/220) |
| 6-month survival
rate, % | 30.5 (67/220) |
| TNM 7th edition,
% |
|
| I | 11.8 (26/220) |
| II | 9.5 (21/220) |
|
III | 57.7 (127/220) |
| IV | 20.9 (46/220) |
| Child-Pugh class,
% |
|
| A | 25.5 (56/220) |
| B | 45.9 (101/220) |
| C | 28.6 (63/220) |
| CUPI, % |
|
| 0 | 19.5 (43/220) |
| 1 | 48.2 (106/220) |
| 2 | 32.3 (71/220) |
| Okuda, % |
|
| I | 15.5 (34/220) |
| II | 54.1 (119/220) |
|
III | 30.5 (67/220) |
| CLIP, % |
|
| 0 | 2.3 (5/220) |
| 1 | 9.5 (21/220) |
| 2 | 14.1 (31/220) |
| 3 | 16.4 (36/220) |
| 4 | 22.7 (50/220) |
| 5 | 25.9 (57/220) |
| 6 | 9.1 (20/220) |
| BCLC, % |
|
| A | 0 |
| B | 0 |
| C | 62.7 (138/220) |
| D | 37.3 (82/220) |
| JIS, % |
|
| 0 | 0.5 (1/220) |
| 1 | 5.9 (13/220) |
| 2 | 13.6 (30/220) |
| 3 | 25.5 (56/220) |
| 4 | 37.7 (83/220) |
| 5 | 16.8 (37/220) |
| CIS, % |
|
| 0 | 10.5 (23/220) |
| 1 | 26.8 (59/220) |
| 2 | 33.6 (74/220) |
| 3 | 17.7 (39/220) |
| 4 | 6.8 (15/220) |
| 5 | 4.5 (10/220) |
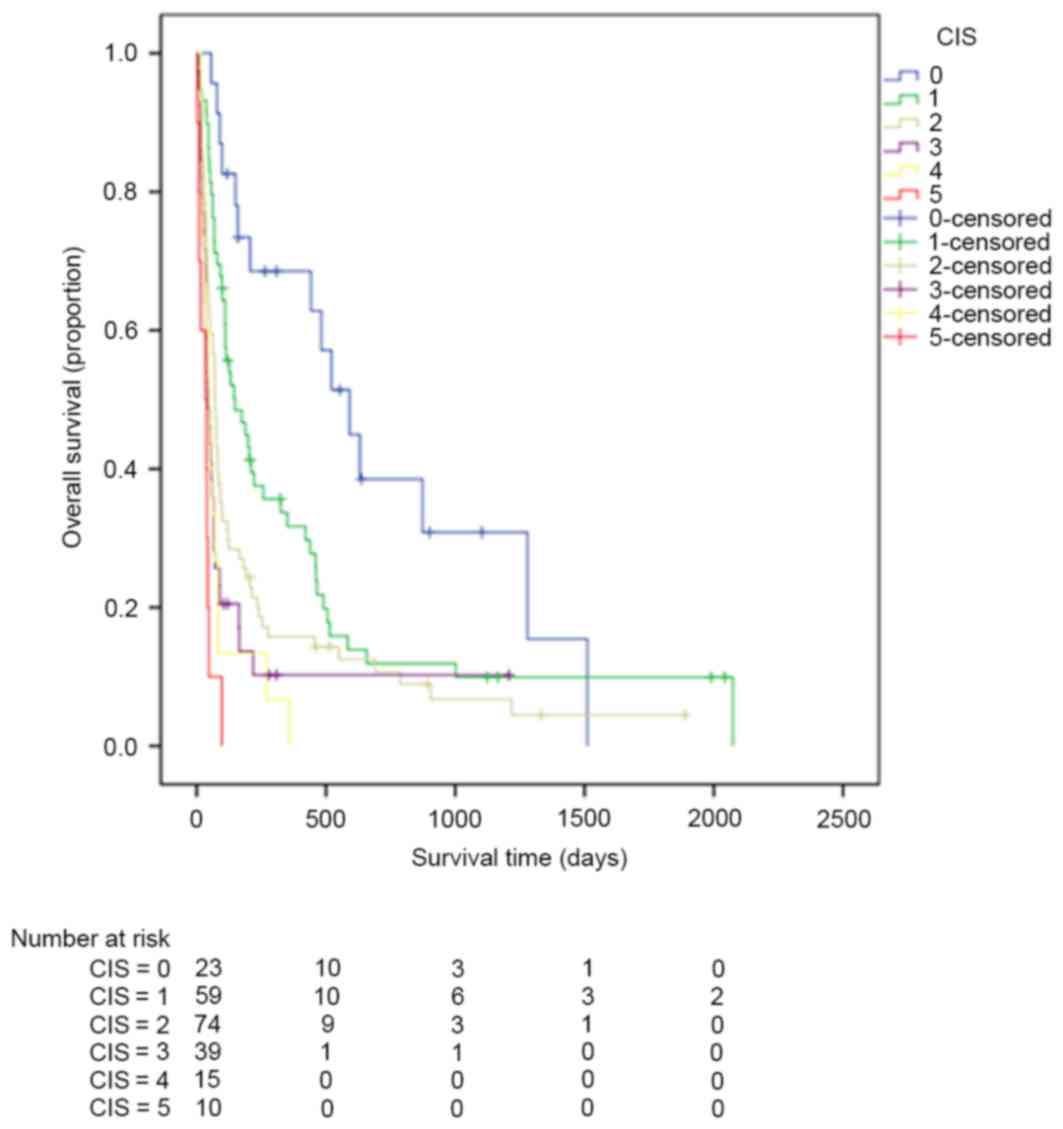
Evaluation of staging systems
Kaplan-Meier estimator curves were generated using
SPSS software for CLIP (Fig. 1), CIS
(Fig. 2), CUPI (Fig. 3), Okuda (Fig. 4), TNM (Fig.
5), JIS (Fig. 6) and BCLC
(Fig. 7). Significant statistical
differences were observed between different prognostic strata for
CLIP, CUPI, TNM, JIS, Okuda, CIS and BCLC (P<0.05 in all cases,
log-rank test).
The LRT and AIC results are listed in Table II. The LRT χ2 values for
CLIP, CIS, CUPI, OCUDA, TNM, JIS and BCLC were 75.6, 48.4, 46.7,
36.0, 21.0, 46.8 and 7.24, respectively. The AIC values for CLIP,
CIS, CUPI, OCUDA, TNM, JIS and BCLC were 1601.5, 1632.3, 1629.9,
1641.1, 1654.8, 1627.4 and 1671.1, respectively. CLIP exhibited the
highest χ2 value and lowest AIC value.
| Table II.Homogeneity LRT χ2 test
and AIC of various hepatocellular carcinoma staging systems. |
Table II.
Homogeneity LRT χ2 test
and AIC of various hepatocellular carcinoma staging systems.
| Staging system | Homogeneity LRT
χ2 test | AIC | P-value |
|---|
| Cancer of the Liver
Italian Program | 70.6 | 1601.5 | <0.0001 |
| China Integrated
Score | 48.4 | 1632.3 | <0.0001 |
| Chinese University
Prognostic Index | 46.7 | 1629.9 | <0.0001 |
| Okuda | 36.0 | 1641.1 | <0.0001 |
|
Tumor-node-metastasis | 21.0 | 1654.8 | <0.0001 |
| Japan Integrated
Staging | 46.8 | 1627.4 | <0.0001 |
| Barcelona Clinic
Liver Cancer |
7.24 | 1671.1 | 0.0071 |
Pairwise comparison of the AUC of ROC curves
predicting 3-month survival revealed that CLIP ranked highest,
followed by CIS. There was no significant difference between CLIP
and CIS observed when predicting 3-month survival (Table III). In terms of predicting 6-month
survival, the AUC of CLIP ranked first, followed by JIS. There was
a significant difference between CLIP and JIS (Table IV).
| Table III.Pairwise comparison of relative
operating characteristic curves predicting 3-month survival. |
Table III.
Pairwise comparison of relative
operating characteristic curves predicting 3-month survival.
| System | System | Difference | P-value |
|---|
| CLIP | CIS | 0.0346 | 0.2001 |
| CLIP | JIS | 0.0526 | 0.0320 |
| CLIP | CUPI | 0.0559 | 0.0312 |
| CLIP | Okuda | 0.0757 | 0.0110 |
| CLIP | TNM | 0.164 | <0.0001 |
| CLIP | BCLC | 0.185 | <0.0001 |
| CIS | JIS | 0.0180 | 0.5367 |
| CIS | CUPI | 0.0213 | 0.4983 |
| CIS | Okuda | 0.0410 | 0.2045 |
| CIS | TNM | 0.129 | 0.0001 |
| CIS | BCLC | 0.150 | <0.0001 |
| JIS | CUPI | 0.00333 | 0.9147 |
| JIS | Okuda | 0.0231 | 0.4718 |
| JIS | TNM | 0.111 | 0.0011 |
| JIS | BCLC | 0.132 | 0.0001 |
| CLIP | CIS | 0.0346 | 0.2001 |
| CLIP | JIS | 0.0526 | 0.0320 |
| Table IV.Pairwise comparison of receiver
operating characteristic curves predicting 6-month survival. |
Table IV.
Pairwise comparison of receiver
operating characteristic curves predicting 6-month survival.
| System | System | Difference | P-value |
|---|
| CLIP | CIS | 0.0996 | 0.0007 |
| CLIP | JIS | 0.0826 | 0.0010 |
| CLIP | CUPI | 0.111 | <0.0001 |
| CLIP | Okuda | 0.136 | <0.0001 |
| CLIP | TNM | 0.164 | <0.0001 |
| CLIP | BCLC | 0.254 | <0.0001 |
| CIS | JIS | 0.0170 | 0.6087 |
| CIS | CUPI | 0.0115 | 0.7274 |
| CIS | Okuda | 0.0368 | 0.2942 |
| CIS | TNM | 0.0646 | 0.0837 |
| CIS | BCLC | 0.154 | <0.0001 |
| JIS | CUPI | 0.0285 | 0.3518 |
| JIS | Okuda | 0.0538 | 0.1320 |
| JIS | TNM | 0.0816 | 0.0294 |
| JIS | BCLC | 0.171 | <0.0001 |
| CLIP | CIS | 0.0996 | 0.0007 |
| CLIP | JIS | 0.0826 | 0.0010 |
Comparison of the predictive ability of the seven
staging systems for 3- and 6-month survival was calculated by ROC
analysis. The AUC curves of the seven staging systems for
predicting 3- and 6-month survival are demonstrated in Figs. 8 and 9.
 | Figure 8.ROC curves of CLIP, CIS, CUPI, Okuda,
TNM, JIS and BCLC when predicting 3-month survival. ROC, relative
operating characteristics; CLIP, the Cancer of the Liver Italian
Program; CIS, China Integrated Score; CUPI, Chinese University
Prognostic Index; TNM, tumor-node-metastasis; JIS, Japan Integrated
Staging; BCLC, Barcelona Clinic Liver Cancer. |
 | Figure 9.ROC curves of CLIP, CIS, CUPI, Okuda,
TNM, JIS and BCLC when predicting 6-month survival. ROC, relative
operating characteristics; CLIP, the Cancer of the Liver Italian
Program; CIS, China Integrated Score; CUPI, Chinese University
Prognostic Index; TNM, tumor-node-metastasis; JIS, Japan Integrated
Staging; BCLC, Barcelona Clinic Liver Cancer. |
When predicting 3-month survival, the AUCs of CLIP,
CIS, CUPI, Okuda, TNM, JIS and BCLC were 0.806, 0.772, 0.751,
0.731, 0.643, 0.754 and 0.622, respectively. When predicting
6-month survival, the AUCs of CLIP, CIS, CUPI, Okuda, TNM, JIS and
BCLC were 0.828, 0.729, 0.717, 0.692, 0.664, 0.746 and 0.575,
respectively.
Prognostic factors of survival
Independent prognostic factors for overall survival
were identified using univariate and multivariate analyses. These
factors are summarized in Table V.
Univariate analyses identified age, metastasis, PS, tumor size,
weight loss, ALP, AFP, albumin, BUN, creatinine, α-L-fucosidase,
platelet count, GGT, WBC, neutrophil count, fibrinogen, portal vein
thrombus and Child-Pugh class as independent predictors of overall
survival. Multivariate analyses identified tumor size, AFP, BUN,
portal vein thrombus, Child-Pugh class and neutrophil count as
independent prognostic factors.
| Table V.Independent prognostic factors for
overall survival in patients with advanced hepatocellular
carcinoma. |
Table V.
Independent prognostic factors for
overall survival in patients with advanced hepatocellular
carcinoma.
| Covariate | Hazard ratio for
mortality | 95% confidence
interval of Exp(b) | P-value |
|---|
| α-fetoprotein | 0.56 | 0.37–0.87 | 0.01 |
| Blood urea
nitrogen | 3.23 | 2.02–5.17 | <0.01 |
| Child-Pugh class of
original Child-Pugh system | 1.36 | 1.07–1.732 | 0.01 |
| Neutrophil
count | 1.29 | 1.03–1.62 | 0.03 |
| Portal vein
thrombosis | 0.62 | 0.38–0.99 | 0.05 |
| Tumor size | 0.57 | 0.37–0.87 | 0.01 |
Discussion
The majority of patients are diagnosed with advanced
HCC at their initial diagnosis and a number of them are
unresectable (17). In these
patients, the therapeutic option is systemic therapy (20). In the Sorafenib Hepatocellular
Carcinoma Assessment Randomized Protocol study (4), sorafenib was demonstrated to
significantly prolong median overall survival of patients with
advanced HCC (sorafenib arm, 10.7 months vs. placebo arm, 7.9
months; P<0.001) and the Asia-Pacific study (5) (sorafenib arm, 6.5 months vs. placebo
arm, 4.2 months; P<0.01). Kaplan-Meier estimator survival curves
of HCC begin to deviate from the third month subsequent to patients
receiving sorafenib (4,5). Life expectancy >3 months is an
essential inclusion criterion of clinical trials. A previous study
had assessed several staging systems for HCC (21), including CLIP, CUPI, JIS, BCLC, CIS,
TNM and Okuda. There is currently no consensus on which staging
system ranks first for predicting 3- and 6-month and overall
survival rates in patients with advanced HBV-associated HCC.
In the present study, the seven current staging
systems were evaluated in order to identify out the most suitable
staging system. In the selected patient population of the present
study, the CLIP staging system was the most capable of predicting
3- and 6-month mortality and overall survival rates in patients
with advanced HBV-associated HCC. The TNM staging system included
only anatomical factors, and did not perform well in overall
survival prediction. Only patients with BCLC C or D HCC were
recruited in the present study, as all patients with BCLC A and
BCLC B HCC received specific antitumor therapies and were excluded.
For this reason, BCLC did not perform well and demonstrated poor
discriminatory ability: It exhibited the lowest likelihood ratio
value and the highest AIC value.
CLIP was the most accurate staging system in
predicting survival rates in the present study. CLIP is a
frequently used staging system in stratifying patients with HCC
whose main etiology is hepatitis C (10). The CLIP system scores patients from 0
to 6 on the basis of four factors: Portal vein thrombosis, tumor
morphology, AFP level and Child-Pugh class (10): Higher scores predict poorer outcomes.
Anatomical factors and liver function were assessed in CLIP. A
previous retrospective study demonstrated that CLIP exhibited a
good ability to predict recurrence following curative resection in
174 patients with HCC with hepatitis B as the main etiology
(22). In the present study of
patients with HBV-associated HCC exclusively, CLIP also exhibited
the best predictive ability with regard to survival outcomes. The
results of the present study also suggested that CLIP is capable of
stratifying patients with HCC with HBV. The utility of CLIP may be
additionally improved: A previous study suggested that CLIP may
have an improved discriminatory ability by adding abdominal pain,
presence of esophageal varices, PS and AST into the staging system
(23). This requires prospective
validation.
In the present study, when predicting 3-month
mortality, the prognostic values of CIS ranks the second following
CLIP. In 2010, Zhang et al proposed a HCC staging system
termed the CIS (14). CIS included
three factors: adjusted TNM stage, Child-Pugh class and AFP. The
score of adjusted TNM stage was defined as follows: 0, TNM stage
I–III comprising uninodular tumor or multinodular tumors, in a
single lobe; 1, TNM stage IVa, multinodular tumors within multiple
lobes, peritoneum invasion or involves veins; 2, stage IVb HCC that
exhibits distant metastases. The score of the Child-Pugh class was
defined as follows: 0, Child-Pugh class A; 1, Child-Pugh class B;
2, Child-Pugh class C. The score of AFP was defined as follows: 0,
≤400 mg/l; 1, >400 mg/l. The score of each factor was summed and
a CIS score was calculated. CIS is easy to use (14). In the study by Zhang et al a
number of staging systems were compared by analyzing 196 patients
with HCC who received non-surgical treatment, and it was concluded
that CIS was not good in predicting survival in this specific
cohort of patients (13). Additional
studies are required to confirm whether CIS will perform well in
predicting 3-month mortality of patients with HCC who did not
receive any standard anticancer treatment.
In the present study, when predicting 6-month
mortality, the prognostic values of JIS ranks second to CLIP. JIS
score was proposed based on analysis of 722 Japanese patients with
HCC (11). Child-Pugh class defined
by original Child-Pugh system and TNM stage by the Liver Cancer
Study Group of Japan criteria were incorporated into the JIS score
in a previous study (11). Kudo et
al (24) demonstrated that in
patients with early-stage HCC, JIS demonstrated a higher predictive
value for survival compared with CLIP. In the present study, in
patients with advanced HCC, the predictive value of JIS was lower
compared with that of CLIP. In the present study, one patient
scored JIS 0 and 13 patients scored JIS 1. The PS of the patients
with JIS 0 and 1 scores was 1, and they were classified as BCLC C.
JIS did not incorporate PS into the system. Previously, Nishikawa
et al (25) proposed a system
in which performance status was combined with the Japan Integrated
Staging system (PS-JIS), and PS-JIS was compared with four other
prognostic systems, including the original JIS system, BCLC, TNM
and CLIP scoring systems. It was demonstrated that for all
patients, at each time point (1-, 3- and 5-year time points), the
c-index of the PS-JIS system was the highest among five staging
systems, indicating that the PS-JIS system possessed the best
predictability among these staging systems (25). Another study suggested that
incorporating AFP into JIS improved its prognostic ability
(26). However, the modification of
JIS was not widely accepted due to lack of validation.
Different studies have revealed differential ranking
of the various staging systems, and the best staging system for HCC
remains unknown. To the best of our knowledge, the present study is
the first to focus only on patients with HBV-associated advanced
HCC who did not receive any standard antitumor therapy. The present
study indicated that Child-Pugh class defined by original
Child-Pugh system BUN, AFP, portal vein thrombosis, tumor size and
neutrophil count were predictors of survival in the cohort of
patients with HCC. The results of the present study revealed again
that the ranking of staging system may vary, and prognostic factors
may vary for different systems of HCC patients (27).
Patients with advanced HCC are a heterogeneous
group. It is difficult to construct a standard staging system that
is able to precisely predict survival. A number of confounding
factors should be taken into account, including anatomic factors,
liver function, serum tumor markers, symptoms and comorbidities.
The construction of a universally accepted HCC staging system
appears to be unachievable. A large number of Asian and Caucasian
patients with HCC should be recruited to perform careful
statistical analyses and prospective validation. The present study
was a retrospective study, and all patients were from a single
hospital. The next step is to evaluate the hypothesis of the
present study prospectively in patients with HCC from different
institutes and different countries, and in patients with HCC with
HBV, HCV and alcohol-associated risk factors.
Staging classifications continue to be refined by
ongoing studies. In the future, tumor markers may be incorporated
into staging systems to improve prognostic ability. A number of
tumor markers prognostic of survival have been identified. The
BALAD score is a novel scoring system based on five serum markers:
Bilirubin; albumin; lens culinaris agglutinin-reactive AFP, AFP and
des-γ-carboxy prothrombin, and thus, it is termed the BALAD score
(28). The BALAD score is easy to use
and stage can be evaluated with the use of only one serum sample
(28). Molecular markers including
Wiskott-Aldrich syndrome protein family member 3, hepatocellular
carcinoma-associated protein JCL-1, DEP domain-containing protein
1A, prolyl hydroxylase domain-containing protein 2, microRNA
(miR)-9, miR-24-3p, miR-148a and keratin 19 (KRT19) have an implied
association with survival outcome (29–36). Kaseb
et al (37) integrated plasma
vascular endothelial growth factor into CLIP and constructed V-CLIP
to stratify patients. They concluded that V-CLIP exhibited improved
discriminatory ability compared with CLIP (P=0.05). A previous
study identified five genes (TATA box-binding protein-associated
factor F9, receptor activity-modifying protein 3, hematological and
neurological expressed 1, KRT19 and Ras-related nuclear protein)
with prognostic value: Patients were stratified with HCC to be good
risk group and poor risk group by using a gene expression score
(38). Integrating these tumor
markers into current staging systems may assist in additionally
improving the sensitivity and specificity of these staging
classifications. In the selected group of patients with advanced
HBV-associated HCC in the present study, CLIP was identified to be
the best staging system for predicting 3- and 6-month and
cumulative survival rates. CIS was adequate for predicting 3-month
mortality and JIS was adequate for predicting 6-month mortality.
Prospective and multicenter validations are required to determine
which staging system is best.
Acknowledgements
The statistical methods used in the present study
were reviewed by FanSong Zeng from the School of Public Health, Sun
Yat-sen University (Guangzhou, China). The present study was
supported by grants from the National Natural Science Foundation of
China (grant nos. 31600710 and 81372374), the Combination Project
of Production, the scientific research project for University
belong to Guangzhou Municipal (grant no. 1201630019), and Natural
Science Foundation of Guangdong (grant nos. 2014A030313146 and
2016A030313302).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lai CL, Ratziu V, Yuen MF and Poynard T:
Viral hepatitis B. Lancet. 362:2089–2094. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, De Oliveira AC, Sanoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S,
Kim JS, Luo R, Feng J, Ye S, Yang TS, et al: Efficacy and safety of
sorafenib in patients in the Asia-Pacific region with advanced
hepatocellular carcinoma: A phase III randomised, double-blind,
placebo controlled trial. Lancet Oncol. 10:25–34. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bruix J, Gores GJ and Mazzaferro V:
Hepatocellular carcinoma: Clinical frontiers and perspectives. Gut.
63:844–855. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bertino G, Demma S, Ardiri A, Proiti M,
Gruttadauria S, Toro A, Malaguarnera G, Bertino N, Malaguarnera M,
Malaguarnera M and Di Carlo I: Hepatocellular carcinoma: Novel
molecular targets in carcinogenesis for future therapies. Biomed
Res Int. 2014:2036932014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Abou-Alfa GK: Selection of patients with
hepatocellular carcinoma for sorafenib. J Natl Compr Canc Netw.
7:397–403. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abou-Alfa GK: Hepatocellular carcinoma:
Molecular biology and therapy. Semin Oncol. 33 6 Suppl 11:S79–S83.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Llovet JM and Bruix J: Prospective
validation of the cancer of the liver Italian program (CLIP) score:
A new prognostic system for patients with cirrhosis and
hepatocellular carcinoma. Hepatology. 32:679–680. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kubo S, Tanaka H, Shuto T, Takemura S,
Yamamoto T, Uenishi T, Tanaka S, Hai S, Yamamoto S, Ichikawa T, et
al: Prognostic effects of causative virus in hepatocellular
carcinoma according to the Japan integrated staging (JIS) score. J
Gastroenterol. 40:972–979. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
DeLong ER, DeLong DM and Clarke-Pearson
DL: Comparing the areas under two or more correlated reciever
operating characteristic curves: A nonparamentric approach.
Biometrics. 44:837–845. 1988. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang JF, Shu ZJ, Xie CY, Li Q, Jin XH, Gu
W, Jiang FJ and Ling CQ: Prognosis of unresectable hepatocellular
carcinoma: Comparison of seven staging systems (TNM, Okuda, BCLC,
CLIP, CUPI, JIS, CIS) in a Chinese cohort. PLoS One. 9:e881822014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang BH, Wang XH, Yue HY and Ling CQ: A
new staging system is more discriminant than conventional staging
systems for unresectable hepatocellular carcinoma. J Cancer Res
Clin Oncol. 136:821–827. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Adhoute X, Penaranda G, Raoul JL, Le Treut
P, Bollon E, Hardwigsen J, Castellani P, Perrier H and Bourlière M:
Usefulness of staging systems and prognostic scores for
hepatocellular carcinoma treatments. World J Hepatol. 8:703–715.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yau T, Yao TJ, Chan P, Ng K, Fan ST and
Poon RT: A new prognostic score system in patients with advanced
hepatocellular carcinoma not amendable to locoregional therapy:
Implication for patient selection in systemic therapy trials.
Cancer. 113:2742–2751. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bruix J and Sherman M; Practice Guidelines
Committee, American Association for the Study of Liver Diseases, :
Management of hepatocellular carcinoma. Hepatology. 42:1208–1236.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
[Guideline] National Comprehensive Cancer
Network, . NCCN Hepatobiliary Cancers Clinical Practice Guidelines
in Oncology. http://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdfVersion
2. 2016
|
|
20
|
Tabrizian P, Roayaie S and Schwartz ME:
Current management of hepatocellular carcinoma. World J
Gastroenterol. 20:10223–10237. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Maida M, Orlando E, Cammà C and Cabibbo G:
Staging systems of hepatocellular carcinoma: A review of
literature. World J Gastroenterol. 20:4141–4150. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang YH, Chen CH, Chang TT, Chen SC, Wang
SY, Lee HS, Lin PW, Huang GT, Sheu JC, Tsai HM, et al: Evaluation
of predictive value of CLIP Okuda, TNM and JIS staging systems for
hepatocellular carcinoma patients undergoing surgery. J
Gastroenterol Hepatol. 20:765–771. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Huitzil-Melendez FD, Capanu M, O'Reilly
EM, Duffy A, Gansukh B, Saltz LL and Abou-Alfa GK: Advanced
hepatocellular carcinoma: Which staging systems best predict
prognosis? J Clin Oncol. 28:2889–2895. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kudo M, Chung H, Haji S, Osaki Y, Oka H,
Seki T, Kasugai H, Sasaki Y and Matsunaga T: Validation of a new
prognostic staging system for hepatocellular carcinoma: The JIS
score compared with the CLIP score. Hepatology. 40:1396–1405. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nishikawa H, Kita R, Kimura T, Endo M,
Ohara Y, Sakamoto A, Saito S, Nishijima N, Nasu A, Komekado H and
Osaki Y: Proposal of the performance status combined Japan
Integrated Staging system in hepatocellular carcinoma complicated
with cirrhosis. Int J Oncol. 46:2371–2379. 2015.PubMed/NCBI
|
|
26
|
Yen YH, Changchien CS, Wang JH, Kee KM,
Hung CH, Hu TH, Lee CM, Lin CY, Wang CC, Chen TY, et al: A modified
TNM-based Japan Integrated Score combined with AFP level may serve
as a better staging system for early-stage predominant
hepatocellular carcinoma patients. Dig Liver Dis. 41:431–441. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Qin LX and Tang ZY: The prognostic
significance of clinical and pathological features in
hepatocellular carcinoma. World J Gastroenterol. 8:193–199.
2002.PubMed/NCBI
|
|
28
|
Toyoda H, Kumada T, Osaki Y, Oka H, Urano
F, Kudo M and Matsunaga T: Staging hepatocellular carcinoma by a
novel scoring system (BALAD score) based on serum markers. Clin
Gastroenterol Hepatol. 4:1528–1536. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ji Y, Li B, Zhu Z, Guo X, He W, Fan Z and
Zhang W: Overexpression of WAVE3 promotes tumor invasiveness and
confers an unfavorable prognosis in human hepatocellular carcinoma.
Biomed Pharmacother. 69:409–415. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hashimoto R, Kanda M, Takami H, Shimizu D,
Oya H, Hibino S, Okamura Y, Yamada S, Fujii T, Nakayama G, et al:
Aberrant expression of melanoma-associated antigen-D2 serves as a
prognostic indicator of hepatocellular carcinoma outcome following
curative hepatectomy. Oncol Lett. 9:1201–1206. 2015.PubMed/NCBI
|
|
31
|
Yuan SG, Liao WJ, Yang JJ, Huang GJ and
Huang ZQ: DEP domain containing 1 is a novel diagnostic marker and
prognostic predictor for hepatocellular carcinoma. Asian Pac J
Cancer Prev. 15:10917–10922. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhen L, Shijie N and Shuijun Z: Tumor PHD2
expression is correlated with clinical features and prognosis of
patients with HCC receiving liver resection. Medicine (Baltimore).
93:e1792014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Cai L and Cai X: Up-regulation of miR-9
expression predicate advanced clinicopathological features and poor
prognosis in patients with hepatocellular carcinoma. Diagn Pathol.
9:10002014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Meng FL, Wang W and Jia WD: Diagnostic and
prognostic significance of serum miR-24-3p in HBV-related
hepatocellular carcinoma. Med Oncol. 31:1772014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Heo MJ, Kim YM, Koo JH, Yang YM, An J, Lee
SK, Lee SJ, Kim KM, Park JW and Kim SG: microRNA-148a dysregulation
discriminates poor prognosis of hepatocellular carcinoma in
association with USP4 overexpression. Oncotarget. 5:2792–2806.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Govaere O, Komuta M, Berkers J, Spee B,
Janssen C, De Luca F, Katoonizadeh A, Wouters J, van Kempen LC,
Durnez A, et al: Keratin 19: A key role player in the invasion of
human hepatocellular carcinomas. Gut. 63:674–685. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kaseb AO, Hassan MM, Lin E, Xiao L, Kumar
V, Pathak P, Lozano R, Rashid A, Abbruzzese JL and Morris JS:
V-CLIP: Integrating plasma vascular endothelial growth factor into
a new scoring system to stratify patients with advanced
hepatocellular carcinoma for clinical trials. Cancer.
117:2478–2488. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Nault JC, De Reyniès A, Villanueva A,
Calderaro J, Rebouissou S, Couchy G, Decaens T, Franco D, Imbeaud
S, Rousseau F, et al: A hepatocellular carcinoma 5-gene score
associated with survival of patients after liver resection.
Gastroenterology. 145:176–187. 2013. View Article : Google Scholar : PubMed/NCBI
|