Introduction
Pituitary tumors occur in the anterior and posterior
pituitary of the pituitary gland and in the epithelium of the
craniopharyngeal duct (1).
Clinically, obvious symptoms account for approximately 10% of
intracranial tumors. These tumors occur in males slightly more than
females. Pituitary tumors usually occur in young adults and often
affect growth and development, reproductive function, learning and
the working ability of patients (2–4). Clinical
manifestations include hormone secretion disorders, tumor
compressions of the surrounding tissues of the pituitary gland,
pituitary apoplexy and the decline of other anterior pituitary
functions (5,6). In recent years, with the rise of tumor
markers, the study on pituitary tumors has gradually developed to
the molecular level (7).
EGR-1, is an early growth response 1-encoded protein
(8). It is believed that EGR-1 plays
an important role in regulating proliferation, differentiation,
apoptosis and embryonic development of early pituitary tissues and
in the occurrence and development processes of a variety of benign
and malignant tumors, including genital tumors and tumors of the
digestive system (9). PTEN, is a
phosphatase and tension homolog encoded protein (10). Previous findings showed that PTEN is
one of the many new genes that inhibits the growth of the pituitary
gland (11).
The present study used the immunohistochemical SP
method to detect the protein expression in pituitary adenomas and,
according to pathological staging, to observe different expression
changes and examine the role and possible mechanism involved in the
occurrence and development of pituitary tumors to provide a
preliminary experimental basis for the prevention, early diagnosis
and target gene treatment of the disease.
Materials and methods
Inclusion criteria and exclusion
criteria
From January 2014 to September 2015, we collected 35
cases confirmed by pathological diagnosis as senile pituitary
tumors from the hospital's Dermatology Clinic. These consisted of
25 cases of non-invasive pituitary adenomas and 10 cases of
invasive pituitary adenomas. At the same time, 35 cases of normal
pituitary tissues were taken from the patients. This experiment was
approved by the University Medical Ethics Committee at the Binhai
Development Zone People's Hospital (Weifang, China).
The inclusion criteria of the study were as follows:
i) Senile pituitary tumors by pathological diagnosis; ii) patient
had no other primary or secondary benign or malignant tumors; iii)
patient was first diagnosed; and iv) patient voluntarily
participated and signed an informed consent form.
The exclusion criteria of the study were: i) Patient
and family members could not participate in the experiment; ii)
patient refused to accept pathological examination; iii) patient
refused treatment; iv) patient was treated with chemotherapy,
radiotherapy, targeted therapy or immune regulation 3–4 weeks
before he or she was had pathologic tissue cutting performed and
was enrolled in this study; and v) patient had mental illness or a
consciousness disorder.
Test reagent
The solutions used in the study were: 0.9% sterile
saline (Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan), mouse
anti-human EGR-1 antibody and mouse anti-human PTEN antibody (both
from Wuhan Boster Bio-Engineering Co., Ltd., Wuhan, China),
immunohistochemical SP900 staining kit, diaminobenzidine (DAB)
concentration staining kit and Mayer's hematoxylin (all from
Zhongshan Jinqiao Biotechnology Co., Ltd., Beijing, China), fresh
xylene (Tianjin Fu Chen Chemical Reagents Factory, Tianjin, China),
35% ethanol, NaH2PO42•H2O,
Na2HPO412•H2O, citric acid and
sodium citrate (all from Tianjin Fu Chen Chemical Reagents Factory,
Tianjin, China), and water bath (Beijing Medical Equipment Factory,
Beijing, China).
Experimental instruments
The instruments used in the present study were:
Micropipettes (Eppendorf AG, Hamburg, Germany), refrigerator (set
at 4°C) (Haier Group, Shandong, China), 10 and 5 ml syringe (both
from Tianjin Hanahao Medical Materials Co., Ltd., Tianjin, China),
pathological microtome (Leica Microsystems GmbH, Wetzlar, Germany),
EP tube (Eppendorff AG), micro camera and optical microscope (both
from Olympus, Tokyo, Japan).
Pathological drawing method
Licensed physicians removed skin tissue from
suspected lesions. Prior to the incision, lidocaine was used for
local anesthesia. Skin tissue samples were immediately placed in a
container with 4% paraformaldehyde solution. The section was
embedded by the Department of Pathology of the Binhai Development
Zone People's Hospital. Using the method of serial section, the
physicians set the thickness at 5 µm, and recorded the patient's
name, medical record number, sampling time and sampling tissue
types. The samples were placed into an oven at 60°C for 1 h, to
enable the tissue to closely attach to the slide. Samples were
removed from the oven and cooled to room temperature.
Immunohistochemical SP method
Prior to immunohistochemical staining, the paraffin
section of the pathological tissue was initially tested (12). The steps of paraffin section testing
included fixation, dehydration, transparency, tissue embedding,
slicing and using a baking sheet. After generating the paraffin
section, the immunohistochemical SP method was used to perform
histochemical staining.
The staining steps were as follows: i) Dewaxing: at
20°C and standing for 60 min, soaked with xylene for 25 min; ii)
hydration: Soaked in anhydrous alcohol for 2 min before being
placed in a solution of 95, 80 and 70% alcohol, respectively, each
for 2 min; phosphate-buffered saline (PBS) rinse performed 2–3
times, each rinse for 5 min. iii) Blocking: Use of 3%
H2O2 deionized water and incubation for 10
min followed by PBS rinsing 2–3 times, with each rinse for 5 min.
iv) Antigen repair: in 95°C citric acid buffer solution (pH 6.0)
and heating for 15–20 min, followed by cooling at room temperature
for 20 min; placed in cold water and then into a cylinder at room
temperature; PBS rinse performed 2–3 times, each rinse for 5 min.
v) Enclosed: Use of normal goat serum blocking at room temperature
and incubation for 20 min, removal of excess liquid; use of primary
antibody (50 µl), incubating at 20°C for 1 h. PBS rinse was then
peformed 2–3 times, with each rinse for 5 min followed by addition
of 40–50 µl horseradish peroxidase secondary monoclonal goat
anti-rabbit IgG antibody (dilution, 1:2,000; cat. no. ab6721;
Abcam, Cambridge, MA, USA), incubating at room temperature for 1 h.
PBS rinsing was then performed 2–3 times, with each rinse for 5
min, followed by the addition of streptavidin peroxidase and
incubation at room temperature for 30 min prior to PBS rinse 2–3
times, with each rinse for 5 min. vi) Color: Samples were immersed
into DAB color development solution for 5–10 min and viewed under
the microscope to note the degree of staining. A brown cytoplasm
was determined as the positive pituitary (PP) gland, and a tap
water rinse was performed for 10 min to terminate the reaction.
vii) Complex: Performed hematoxylin staining for 2 min, followed by
the addition of hydrochloric acid alcohol for differentiation prior
to a tap water rinse of 10–15 min. viii) Dehydrate, clean and
mount: Neutral gum was used under the tissue, and this was covered
with the coverslip for microscopic examination.
Interpretation method of
immunohistochemical staining results of senile pituitary tumor
The results of the staining were interpreted and
scored as follows: i) Positive detection: Product protein was found
to be positive for EGR-1 and PTEN gene expression in
the pituitary gland. After staining and under optical microscope,
pituitary nuclear particles were viewed as brown or tan, indicating
positive designation; ii) pituitary count: The pituitary count was
expressed as PP/mm2, this factor was scored according to
the observed EGR-1 and PTEN PP ratio and staining intensity (SI);
iii) scoring criteria: Total score = SI × PP. A total score of ≤6
and >6 were defined as negative and positive, respectively. In
accordance with the pituitary staining intensity, testing was
divided into 4 levels: i) No pituitary staining was negative, 0
points; ii) weakly positive (+), 1 point; iii) moderately positive
(++), 2 points; and iv) strongly positive (+++), 3 points.
According to the percentage of PP, testing was
divided into four levels: i) Negative: No pituitary staining, 0
points; ii) positive: Pituitary ≤10%, 1 point; iii) PP 11–50%, 2
points; iv) PP 51–80%, 3 points; and v) PP >80%, 4 points. The
positive rate of samples was calculated by the percentage of
positive samples in the total number of samples. Ten randomly
selected fields were viewed by high magnification, ×400, calculated
as a percentage of PP samples. Mean ± SD was the average value of
the PP and its standard deviation was the expression intensity.
Statistical analysis
SPSS 19.0 software (IBM SPSS, Armonk, NY, USA) was
used for statistical analysis, and the qualitative data were
analyzed and tested by analysis of variance (ANOVA) test, t-test
and χ2 test. The Fisher's precise probability method was
used for the 4 grid data of who did not meet the conditions.
Quantitative data were compared and tested by ANOVA. P<0.05 was
considered to indicate a statistically significant difference.
Results
Positive rate of EGR-1 and PTEN in
tissues of patients and healthy non-pituitary tumors
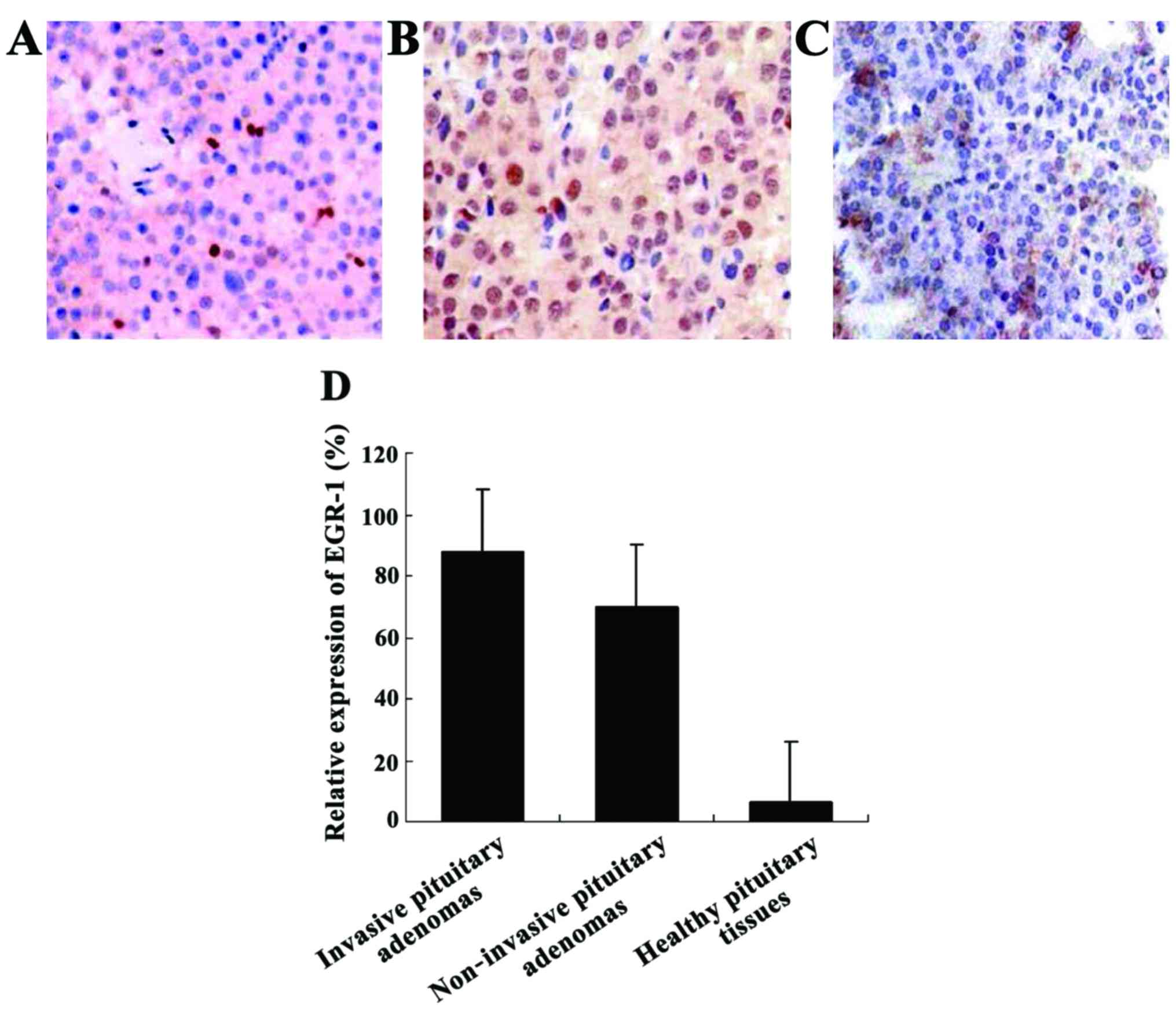
We detected the positive rates of EGR-1 and
PTEN genes in the tissue samples (Table I). Compared with the EGR-1 positive
rate of skin tissue samples of the healthy non-pituitary tumor
cases, in elderly patients with pituitary tumor, the EGR-1
and PTEN positive rates had no significant changes. Compared
with the healthy pituitary tissue, the PTEN positive rates
increased significantly in patients with pituitary tumors. The
difference was statistically significant (χ2=56.7,
p<0.05) (Fig. 1).
 | Table I.Comparison of the positive rates of
EGR-1 and PTEN genes in tissue samples. |
Table I.
Comparison of the positive rates of
EGR-1 and PTEN genes in tissue samples.
| Genes for
detection | Groups | No. of cases | Positive | Negative | Positive rate
(%) |
χ2-value | P-value |
|---|
| EGR-1 | Invasive pituitary
tumor | 25 | 19 | 6 | 76.0 (19/25) | 8.9 | 0.007 |
|
| Noninvasive pituitary
tumor | 10 | 6 | 4 | 60.0 (6/10) |
|
|
|
| Healthy pituitary
tissue | 35 | 2 | 33 | 6.06 (2/35) |
|
|
| PTEN | Invasive pituitary
tumor | 25 | 22 | 3 | 88.0
(22/25) | 56.7 | <0.0001 |
|
| Noninvasive pituitary
tumor | 10 | 7 | 3 | 70.0 (7/10) |
|
|
|
| Healthy pituitary
tumor tissue | 35 | 2 | 33 | 6.06 (2/35) |
|
|
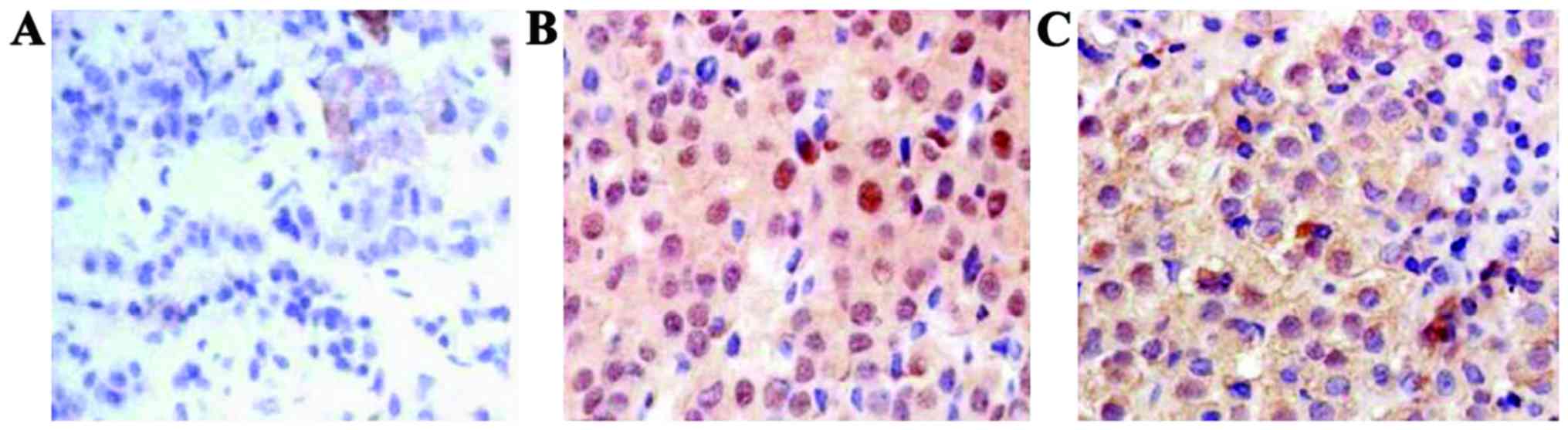
EWxpression intensity of EGR-1 and
PTEN in patients and healthy non-pituitary tumors (mean ± SD)
The average expression intensity of EGR-1 and PTEN
protein in pituitary tumors of patients were 7.21±2.3 and 4.62±1.4,
respectively. The expression intensity in normal skin tissues was
8.52±1.7 and 0.27±0.8, respectively, compared with the healthy
non-pituitary tumors. The difference of the expression intensity of
EGR-1 and PTEN had statistical significance (t=8.44, 5.31,
p<0.05) (Fig. 2 and Table II).
| Table II.The expression intensity of
EGR-1 and PTEN in each group. |
Table II.
The expression intensity of
EGR-1 and PTEN in each group.
| Groups | No. of cases | EGR-1 expression
intensity | PTEN expression
intensity | T-value | P-value |
|---|
| Invasive pituitary
tumor | 25 | 7.21±2.3 | 8.52±1.7 | 8.44 | 0.012 |
| Non-invasive
pituitary tumor | 10 | 4.62±1.4 | 0.27±0.8 |
|
|
| Healthy pituitary
tumor tissue | 35 |
0.01±0.005 |
0.02±0.01 |
|
|
Discussion
A pituitary tumor is a common intracranial tumor,
whose incidence rate is approximately 1 of 10 million, second only
to nerve epidermal tumors and meningiomas. With the development of
imaging and endocrine detection technology, the detection rate is
increasing annually (12–14). In addition to prolactin, which can be
taken in the first trial of the drug sensitivity test for
bromocriptine, surgical resection is the first choice for other
types of pituitary tumors.
In the diagnosis of pituitary tumors, a pathological
diagnosis remains the gold standard, sometimes by means of B-mode
ultrasound, computed tomography and other imaging examinations, as
well as nasal endoscopic and other methods used to judge the
distance of the invasion (15,16).
However, these methods are difficult as a substitute for
pathological examination. In addition, cancer cells can be present
in patients with potential invasive foci. Local invasion foci
cannot be detected through general imaging, which brings great
challenges to a surgical operation and postoperative treatment.
Previous findings have shown EGR-1 or PTEN can be
used as markers for the diagnosis of senile pituitary tumors
(17,18). Of note in evaluating the invasion and
prognosis of malignant tumors, in previous studies of PTEN levels
in cervical cancer, PTEN was significantly increased in the early
stages, but the levels significantly decreased with the increase in
the degree of malignancy (19). PTEN
competes for substrates with tyrosine kinase as a tumor suppressor.
It can play a regulatory role by blocking pituitary growth, mitosis
and other factors, but the underlying mechanism is not clear
(20). In human solid tumors, the
blocking mechanism remains to be confirmed. Based on this, we
designed the present study to detect the expression of PTEN in
human pituitary adenomas and to determine some of the influencing
factors. However, we found that PTEN expression was not high in
some patients with pathologically diagnosed pituitary tumors.
Therefore, we selected EGR-1 as a common reference detection
index.
In previous studies, the EGR-1-encoded protein
structure has three repeated zinc finger domains and plays an
important role in the interaction between the external signal and
the target gene (21). There was a
significant increase in many types of malignant tumors, including
senile pituitary tumors, but the degree of the increase was not
significantly associated with the occurrence and development of
tumors and the degree of tumor differentiation (22,23).
Through experiments, we found that in patients with non-invasive
pituitary tumors, EGR-1 and PTEN levels increased significantly.
Conversely, in patients with invasive pituitary tumors, EGR-1
levels increased significantly, albeit the level of PTEN was normal
or even low. Taking the possible reasons for our results into
account, we believe that in the early stages of pituitary tumor
development, due to the impact of various physical and chemical
factors, the EGR-1 gene was activated in vivo,
further promoting the occurrence of cancer. Concurrently, as the
balance lever, the tumor suppressor gene PTEN, is also
activated. Through the inhibition of tumor pituitary mitosis and in
other ways, PTEN inhibits the proliferation of tumor pituitary and
distant invasive cells. However, with the progress of the disease,
due to the various signaling pathways and the release of
inflammatory factors, it results in the activation of the
proto-oncogene, which may contain some genes that suppress PTEN
signal pathways. This results in the anti-oncogene PTEN weakening
the protective effect and promoting tumor invasion. Nevertheless,
this hypothesis requires additional theoretical experimentation for
possible confirmation.
In conclusion, the present findings have shown that
in senile pituitary tumor patients, EGR-1 and PTEN
levels were significantly higher than those of healthy individuals,
but in patients with distant invasive pituitary tumors, PTEN levels
decreased while EGR-1 levels increased. PTEN and EGR-1 can play an
important role in the potential invasiveness of pituitary tumors in
patients, and this is an area of great significance in guiding
clinical surgery and chemotherapy.
References
|
1
|
Beckers A, Aaltonen LA, Daly AF and Karhu
A: Familial isolated pituitary adenomas (FIPA) and the pituitary
adenoma predisposition due to mutations in the aryl hydrocarbon
receptor interacting protein (AIP) gene. Endocr Rev. 34:239–277.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Donangelo I, Ren SG, Eigler T, Svendsen C
and Melmed S: Sca1+ murine pituitary adenoma cells show
tumor-growth advantage. Endocr Relat Cancer. 21:203–216. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zhu X, Wang Y, Zhao X, Jiang C, Zhang Q,
Jiang W, Wang Y, Chen H, Shou X, Zhao Y, et al: Incidence of
pituitary apoplexy and its risk factors in Chinese people: a
database study of patients with pituitary adenoma. PLoS One.
10:e01390882015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhou Y, Zhang X and Klibanski A: Genetic
and epigenetic mutations of tumor suppressive genes in sporadic
pituitary adenoma. Mol Cell Endocrinol. 386:16–33. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Xiao JQ, Liu XH, Hou B, Yao Y, Deng K,
Feng M, Xing B, Lian W, Wang RZ and Feng F: Correlations of
pituitary tumor transforming gene expression with human pituitary
adenomas: a meta-analysis. PLoS One. 9:e903962014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cristina C, Luque GM, Demarchi G,
Lopez-Vicchi F, Zubeldia-Brenner L, Perez-Millan MI, Perrone S,
Ornstein AM, Lacau-Mengido IM, Berner SI, et al: Angiogenesis in
pituitary adenomas: human studies and new mutant mouse models. Int
J Endocrinol. 2014:6084972014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Waligórska-Stachura J, Andrusiewicz M,
Sawicka-Gutaj N, Kubiczak M, Jankowska A, Liebert W, Czarnywojtek
A, Waśko R, Blanco-Gangoo AR and Ruchała M: Evaluation of survivin
splice variants in pituitary tumors. Pituitary. 18:410–416. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yang L, Tang J, Chen H, Ge D, Sui T, Que
J, Cao X and Ge Y: Taurine reduced epidural fibrosis in rat models
after laminectomy via downregulating EGR1. Cell Physiol Biochem.
38:2261–2271. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fekete C and Lechan RM: Central regulation
of hypothalamic- pituitary-thyroid axis under physiological and
pathophysiological conditions. Endocr Rev. 35:159–194. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gaston-Massuet C, Andoniadou CL, Signore
M, Jayakody SA, Charolidi N, Kyeyune R, Vernay B, Jacques TS,
Taketo MM, Le Tissier P, et al: Increased Wingless (Wnt) signaling
in pituitary progenitor/stem cells gives rise to pituitary tumors
in mice and humans. Proc Natl Acad Sci USA. 108:pp. 11482–11487.
2011; View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Miermeister CP, Petersenn S, Buchfelder M,
Fahlbusch R, Lüdecke DK, Hölsken A, Bergmann M, Knappe HU, Hans VH,
Flitsch J, et al: Histological criteria for atypical pituitary
adenomas - data from the German pituitary adenoma registry suggests
modifications. Acta Neuropathol Commun. 3:502015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Heaney AP: Clinical review: pituitary
carcinoma: difficult diagnosis and treatment. J Clin Endocrinol
Metab. 96:3649–3660. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mathioudakis N, Sundaresh R, Larsen A,
Ruff W, Schiller J, Guerrero-Cázares H, Burger P, Salvatori R and
Quiñones-Hinojosa A: Expression of the pituitary stem/progenitor
marker GFRα2 in human pituitary adenomas and normal pituitary.
Pituitary. 18:31–41. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lines KE, Stevenson M and Thakker RV:
Animal models of pituitary neoplasia. Mol Cell Endocrinol.
421:68–81. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Antoine V, Moret C, Schmitt E, Klein M and
Bracard S: MRI imaging of the neural pituitary. Ann Endocrinol
(Paris). 69:181–192. 2008.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Komotar RJ, Starke RM, Raper DM, Anand VK
and Schwartz TH: Endoscopic endonasal compared with microscopic
transsphenoidal and open transcranial resection of giant pituitary
adenomas. Pituitary. 15:150–159. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Birt JA, Nabli H, Stilley JA, Windham EA,
Frazier SR and Sharpe-Timms KL: Elevated peritoneal fluid TNF-α
incites ovarian early growth response factor 1 expression and
downstream protease mediators: a correlation with ovulatory
dysfunction in endometriosis. Reprod Sci. 20:514–523. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Palumbo T, Faucz FR, Azevedo M, Xekouki P,
Iliopoulos D and Stratakis CA: Functional screen analysis reveals
miR-26b and miR-128 as central regulators of pituitary
somatomammotrophic tumor growth through activation of the PTEN-AKT
pathway. Oncogene. 32:1651–1659. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tornesello ML, Annunziata C, Buonaguro L,
Losito S, Greggi S and Buonaguro FM: TP53 and PIK3CA gene mutations
in adenocarcinoma, squamous cell carcinoma and high-grade
intraepithelial neoplasia of the cervix. J Transl Med. 12:2552014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Burgucu D, Guney K, Sahinturk D, Ozbudak
IH, Ozel D, Ozbilim G and Yavuzer U: Tbx3 represses PTEN and is
over- expressed in head and neck squamous cell carcinoma. BMC
Cancer. 12:4812012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ozen E, Gozukizil A, Erdal E, Uren A,
Bottaro DP and Atabey N: Heparin inhibits hepatocyte growth factor
induced motility and invasion of hepatocellular carcinoma cells
through early growth response protein 1. PLoS One. 7:e427172012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mellotte G, Maher V, Devitt PG, Shin VY
and Leung CP: Minimally invasive surgical oncology: state of the
art. Asian Pac J Surg Oncol. 1:101–112. 2015.
|
|
23
|
He J, Yu JJ, Xu Q, Wang L, Zheng JZ, Liu
LZ and Jiang BH: Downregulation of ATG14 by EGR1-MIR152 sensitizes
ovarian cancer cells to cisplatin-induced apoptosis by inhibiting
cyto-protective autophagy. Autophagy. 11:373–384. 2015. View Article : Google Scholar : PubMed/NCBI
|