Introduction
Leriche syndrome is a disease of aortoiliac
occlusion, which causes diminished femoral pulses, impotence, and
claudication (1,2). Hypertension, diabetes mellitus,
hyperlipidemia, and smoking are risk factors for the disease
(3). When performing colorectal
cancer surgeries for patients with Leriche syndrome, the following
considerations must be addressed. First, the blood flow to the
rectum is also reduced because of occlusion of the internal iliac
arteries and/or inferior mesenteric artery (IMA), and therefore,
reconstruction with anastomosis may be complicated by ischemia when
performing rectal cancer surgery. Second, the blood flow to the
lower limb is supplied by collateral arteries, such as the inferior
epigastric artery and deep circumflex iliac artery (4), and therefore, attention should be paid
not to injure them during trocar insertion when performing
laparoscopic surgeries.
Here, we report three rare cases of colorectal
cancers complicated by Leriche syndrome, which were successfully
treated with laparoscopic surgery. Informed consent was obtained
from all patients and the publication of the case reports was
approved by institutional ethics committee.
Case report
Case 1
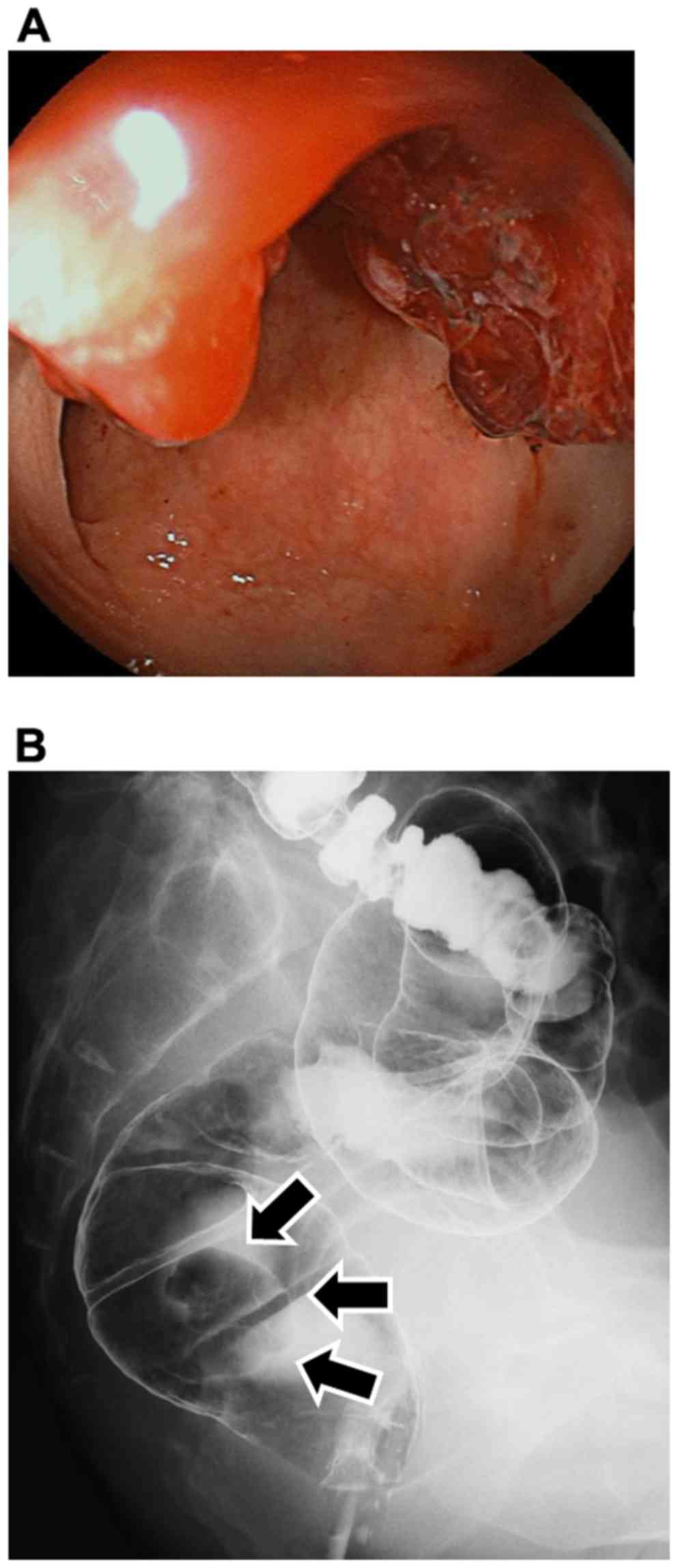
A 71-year-old man underwent total colonoscopy to
evaluate a chief complaint of melena and weight loss. Colonoscopy
revealed rectal cancer (Fig. 1). Risk
factors for arteriosclerosis for the patient included diabetes
mellitus, hypertension, and smoking (30 times per day, from ages 20
to 54 years old). The ankle-brachial index (ABI) was 0.32 on the
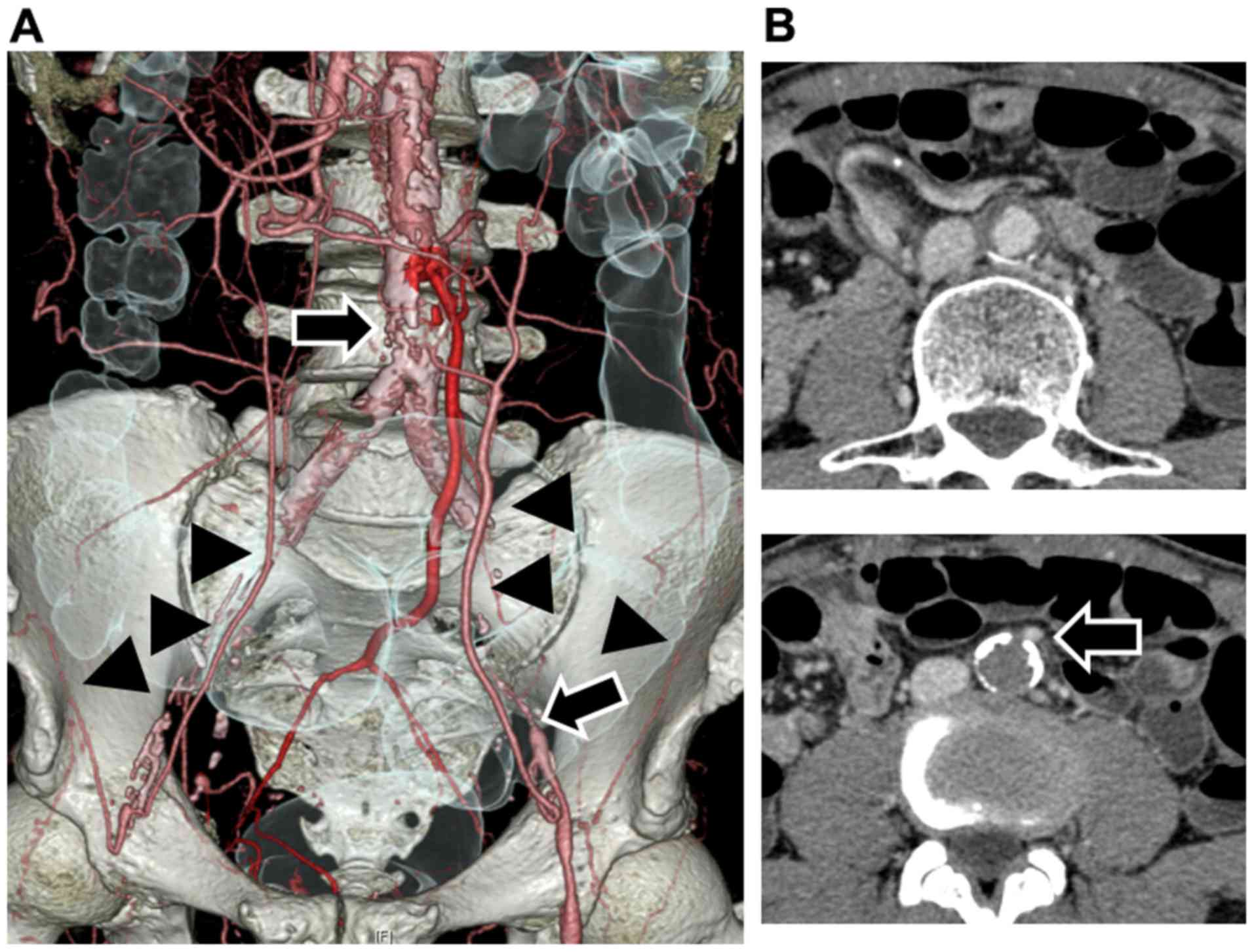
right side and 0.36 on the left side. A preoperative computed
tomography (CT) scan revealed occlusion of the aorta just below the
origin of the IMA (Fig. 2). The blood
flow of the lower limbs was supplied through the inferior
epigastric arteries and deep circumflex iliac arteries. While the
IMA was patent, the internal iliac arteries were occluded
bilaterally. A laparoscopic Hartmann's operation without
anastomosis was performed because the IMA, which was the only blood
supply of the rectum, would be sacrificed via lymph node
dissection, and ischemia of the remnant rectum was anticipated. The
inferior epigastric arteries had developed as collateral arteries.
Therefore, these arteries were preoperatively marked using
ultrasonography to avoid injury of the arteries during trocar
insertion (Fig. 3). The ABI did not
decrease (0.36 on the right side and 0.50 on the left side) and the
patient was discharged from the hospital on postoperative day 14
without complications.
The CT scan performed 6 months after the surgery
revealed that the enhancement of the remnant rectum was remained.
However, the blood flow was supplied from the small collateral
artery (Fig. 4).
Case 2
A 70-year-old man was admitted to our hospital
because of bowel occlusion due to the cancer of the transverse
colon. Colonoscopy revealed three colorectal cancers, located in
the transverse colon, sigmoid colon, and rectum. The risk factor
for arteriosclerosis for this patient was smoking (30 times per
day, from ages 40 to 70 years old). ABI was 0.41 on the right side
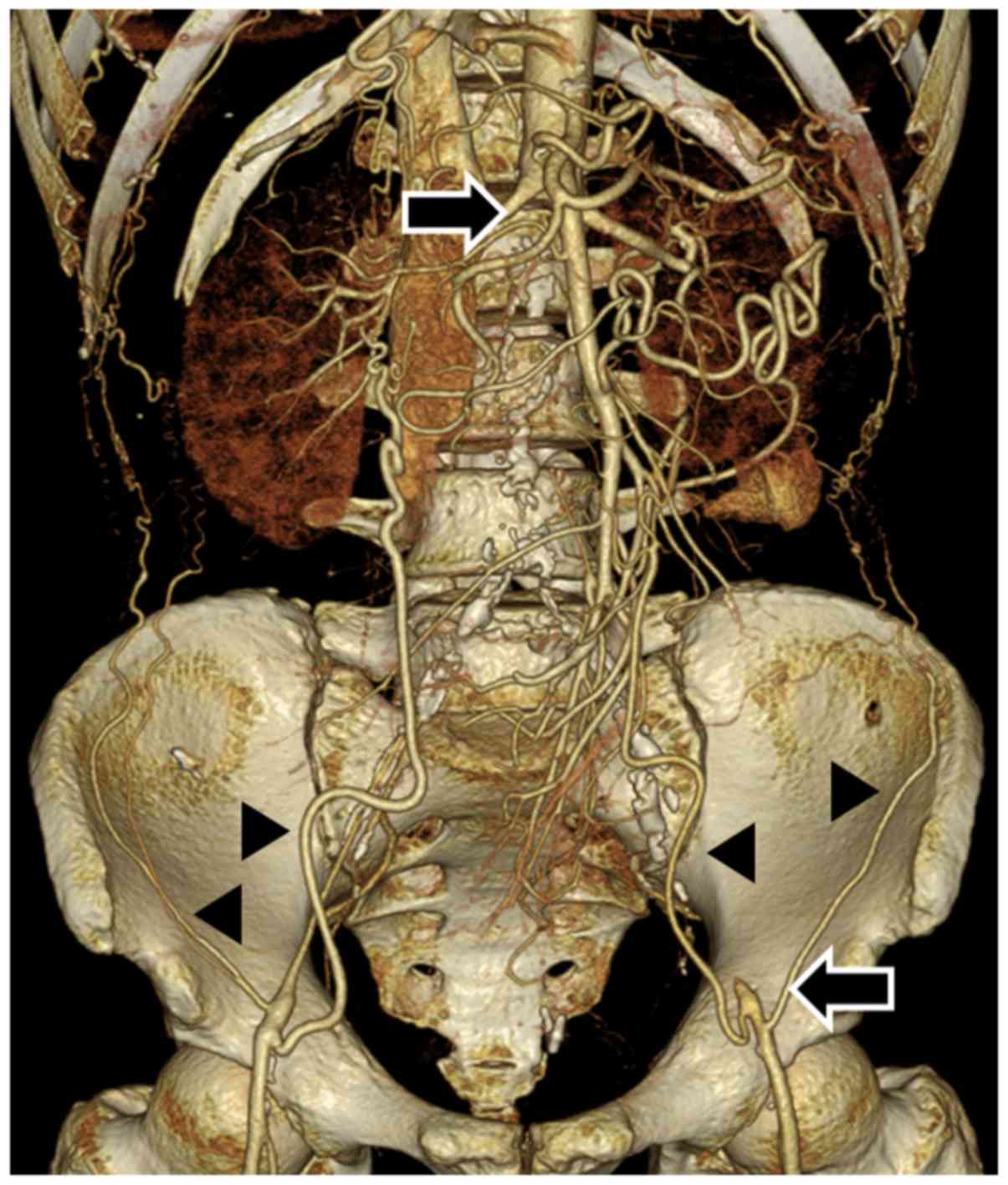
and 0.45 on the left side. A preoperative CT scan revealed
occlusion of the aorta just below the origin of the renal arteries
(Fig. 5). The blood flow of the lower
limbs was supplied through the inferior epigastric arteries and
deep circumflex iliac artery. Because the IMA and both internal
iliac arteries were occluded, laparoscopic left hemicolectomy and
rectal resection with colostomy were performed. The inferior
epigastric arteries were important as collateral arteries, and were
preoperatively marked using ultrasonography to avoid injury. The
ABI did not change, and the patient was discharged from the
hospital on postoperative day 18, without complications.
Colonoscopy performed postoperatively revealed no
ischemic changes or stenosis in the remnant rectum.
Case 3
A 61-year-old man underwent total colonoscopy to
evaluate a chief complaint of melena, revealing rectal cancer. Risk
factors for arteriosclerosis for this patient included diabetes
mellitus, hypertension, hyperlipidemia, and smoking (40 times per
day, from age 25 years to age 57 years). The ABI was 0.77 on the
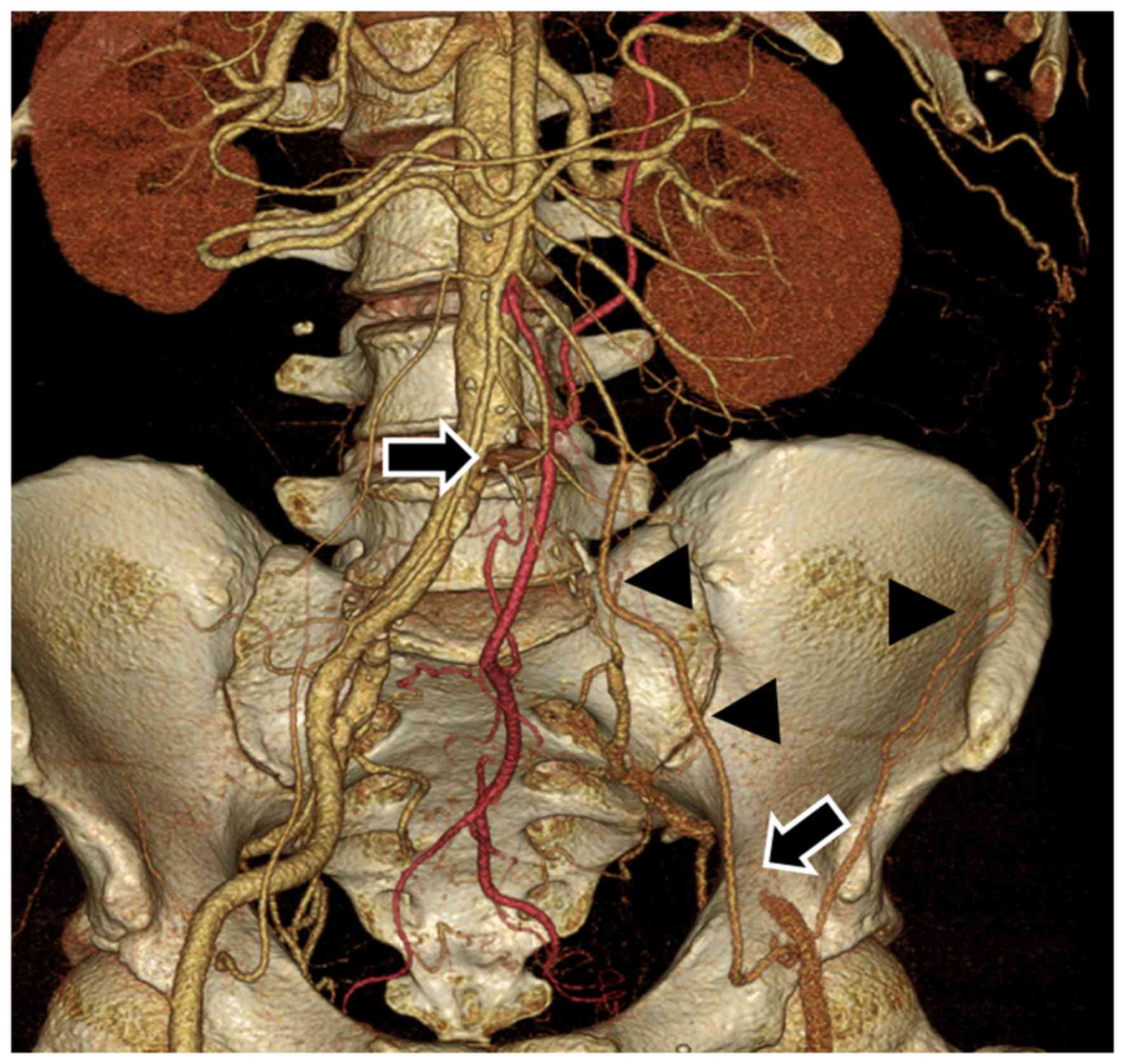
right side and 0.50 on the left side. A preoperative CT scan
revealed occlusion of the left common iliac artery (Fig. 6). The blood flow to the left lower
limb was supplied through the inferior epigastric artery and deep
circumflex iliac artery. Because the right internal iliac artery
was patent, he underwent laparoscopic low anterior resection with
anastomosis. The left inferior epigastric artery was very important
as a collateral artery. Therefore, the artery was preoperatively
marked using ultrasonography to avoid injury. The patient had an
uncomplicated postoperative course and was discharged from the
hospital on postoperative day 18.
Postoperative colonoscopy revealed no stenosis or
ischemic change in anastomosis.
Discussion
The blood flow to the rectum is mainly supplied from
the IMA and bilateral internal iliac arteries, and the main blood
supply was interrupted in cases 1 and 2. Impaired blood supply is
considered one of the causes of anastomotic leakage (5). Although some institutions use
fluorescence imaging with indocyanine green to evaluate intestinal
perfusion (6–8), it remains difficult to evaluate the risk
of anastomotic leakage accurately. Therefore, Hartmann's operations
were performed in two cases. Although impaired blood supply from
the IMA and bilateral internal iliac arteries sometimes result in
intestinal ischemia (9), no necrosis
or stenosis of the remaining rectum was observed, either
intraoperatively or postoperatively. Leriche syndrome is a chronic
disease, associated with the development of collateral arteries,
and additional artery bypass was unnecessary in all cases. Because
there is no report about the surgery of pelvic viscera for the
patients with Leriche syndrome, the blood flow of the remnant
rectum and the risk of the anastomotic leakage are unknown. The
blood flow was supplied from only small arteries in case 1 and the
risk of anastomotic leakage seemed to be high. The evaluation of
the risk of leakage is an issue in the future.
For patients with Leriche syndrome, the following
two pathways are important as collateral arteries to the lower
limbs; i) subclavian artery-internal thoracic artery-superior
epigastric artery-inferior epigastric artery pathway and ii)
subclavian artery-internal thoracic artery-lower intercostals or
subcostals arteries-deep circumflex iliac artery pathway (4). CT angiography can aid surgeons in
identifying anatomical vascular variations preoperatively (10,11). In
all three cases, it was easy to obtain anatomical imaging of these
collateral arteries via CT angiography. As trocar insertion has a
risk of injuring the inferior epigastric arteries in laparoscopic
surgery, the arteries were marked using ultrasonography. While
marking was easy because the arteries had enlarged as collateral
arteries in the middle and lower abdominal area, there was some
difficulty in the upper abdominal area because of some branches.
These branches were also confirmed via CT angiography (Figs. 2, 5, and
6). Therefore, the trocar was
inserted in the middle or lower abdominal area according to the
preoperative marking. The ABI did not worsen in any case, and
axillary-femoral artery bypass was unnecessary. Because the
inferior epigastric arteries were sometimes meandering, such as in
case 2, it is important to obtain images via CT angiography and to
mark these arteries using ultrasonography.
The incidence of arteriosclerosis is increasing. It
is important to visualize the image the blood flow via CT
angiography and to mark collateral arteries using ultrasonography
preoperatively in patients with Leriche syndrome for whom
laparoscopic surgery was planned for colorectal cancer.
Acknowledgements
We would like to thank Editage for English language
editing.
References
|
1
|
Leriche R and Morel A: The syndrome of
thrombotic obliteration of the aortic bifurcation. Ann Surg.
127:193–206. 1948. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Friedman SA, Holling HE and Roberts B:
Etiologic factors in aortoiliac and femoropopliteal vascular
disease. The leriche syndrome. N Engl J Med. 271:1382–1385. 1964.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Frederick M, Newman J and Kohlwes J:
Leriche syndrome. J Gen Intern Med. 25:1102–1104. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wooten C, Hayat M, du Plessis M, Cesmebasi
A, Koesterer M, Daly KP, Matusz P, Tubbs RS and Loukas M:
Anatomical significance in aortoiliac occlusive disease. Clin Anat.
27:1264–1274. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kingham TP and Pachter HL: Colonic
anastomotic leak: Risk factors, diagnosis, and treatment. J Am Coll
Surg. 208:269–278. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
James DR, Ris F, Yeung TM, Kraus R, Buchs
NC, Mortensen NJ and Hompes RJ: Fluorescence angiography in
laparoscopic low rectal and anorectal anastomoses with pinpoint
perfusion imaging-a critical appraisal with specific focus on leak
risk reduction. Colorectal Dis. 17 Suppl 3:S16–S21. 2015.
View Article : Google Scholar
|
|
7
|
Kawada K, Hasegawa S, Wada T, Takahashi R,
Hisamori S, Hida K and Sakai Y: Evaluation of intestinal perfusion
by ICG fluorescence imaging in laparoscopic colorectal surgery with
DST anastomosis. Surg Endosc. 31:1061–1069. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Koh FH and Tan KK: Fluorescent angiography
used to evaluate the perfusion status of anastomosis in
laparoscopic anterior resection. Ann Surg Oncol. 23 Suppl
5:6922016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Järvinen O, Laurikka J, Sisto T and Tarkka
MR: Intestinal ischemia following surgery for aorto-iliac disease.
A review of 502 consecutive aortic reconstructions. Vasa.
25:148–155. 1996.PubMed/NCBI
|
|
10
|
Murono K, Kawai K, Kazama S, Ishihara S,
Yamaguchi H, Sunami E, Kitayama J and Watanabe T: Anatomy of the
inferior mesenteric artery evaluated using 3-dimensional CT
angiography. Dis Colon Rectum. 58:214–219. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Murono K, Kawai K, Ishihara S, Otani K,
Yasuda K, Nishikawa T, Tanaka T, Kiyomatsu T, Hata K, Nozawa H, et
al: Evaluation of the vascular anatomy of the right-sided colon
using three-dimensional computed tomography angiography: A
single-center study of 536 patients and a review of the literature.
Int J Colorectal Dis. 31:1633–1638. 2016. View Article : Google Scholar : PubMed/NCBI
|