Introduction
Breast cancer is established as a global public
health concern and it is predicted to account for 29% of newly
diagnosed cancer cases in women (1).
Although there has been a gradual improvement in treatment for
patients with breast cancer, a number of these patients may develop
distant metastases. Breast cancer frequently metastasizes to the
local and distant nodes, lungs, bones, liver or brain (1). However, it is rare for breast cancer to
metastasize to the gastrointestinal system, particularly to the
stomach (2). The estimated rate of
breast to stomach metastasis varies from 0.3% in retrospective
series to 8–18% in autopsy series (3). Due to the low incidence, only sporadic
cases or small series of gastric metastases from breast cancer have
currently been identified. Therefore, little is established on the
clinicopathological characteristics, clinical outcomes, endoscopic
features and, particularly, the prognostic factors and appropriate
treatments for these patients.
Therefore, the current study investigated a primary
breast cancer metastasized to the stomach, which was diagnosed
using gastroscopy and immunohistochemistry analysis. Additionally,
the present study reviewed 77 similar cases that have been reported
in previously published studies. The aim of the current study was
to perform a retrospective analysis of a cohort of patients with
breast cancer and gastric metastases to examine the
clinicopathological and endoscopic features, the treatment
modalities and the factors associated with prolonged survival. In
the present study, it was revealed that gastric metastasis from
breast cancer is more common in invasive lobular breast cancer
compared with infiltrative ductal breast cancer. In addition,
abdominal pain was revealed to be the most common symptom.
Therefore, when a stomach mass is detected in a patient with
lobular breast cancer, it may be either a primary stomach cancer or
the metastasis of the breast cancer, although the gastric
metastasis from breast cancer is quite rare. Additionally,
histological and immunopathological analysis may aid the
differential diagnoses. For the gastric metastasis from breast
cancer with hormone receptor overexpression (such as estrogen
receptor and progesterone receptor), systemic treatment strategy,
including hormonal therapy, is also recommended.
Materials and methods
Case report
A 73-year-old female was admitted to the Department
of Oncology, Renji Hospital, Shanghai Jiaotong University School of
Medicine (Shanghai, China), who presented with anorexia, fatigue,
abdominal distention and a history of multiple skin nodules in the
chest wall for the prior two months. On physical examination, the
chest wall nodules appeared as solid, irregular and fixed,
measuring 0.5–1.2 cm in diameter. A core needle biopsy was
performed and histopathological studies identified the infiltration
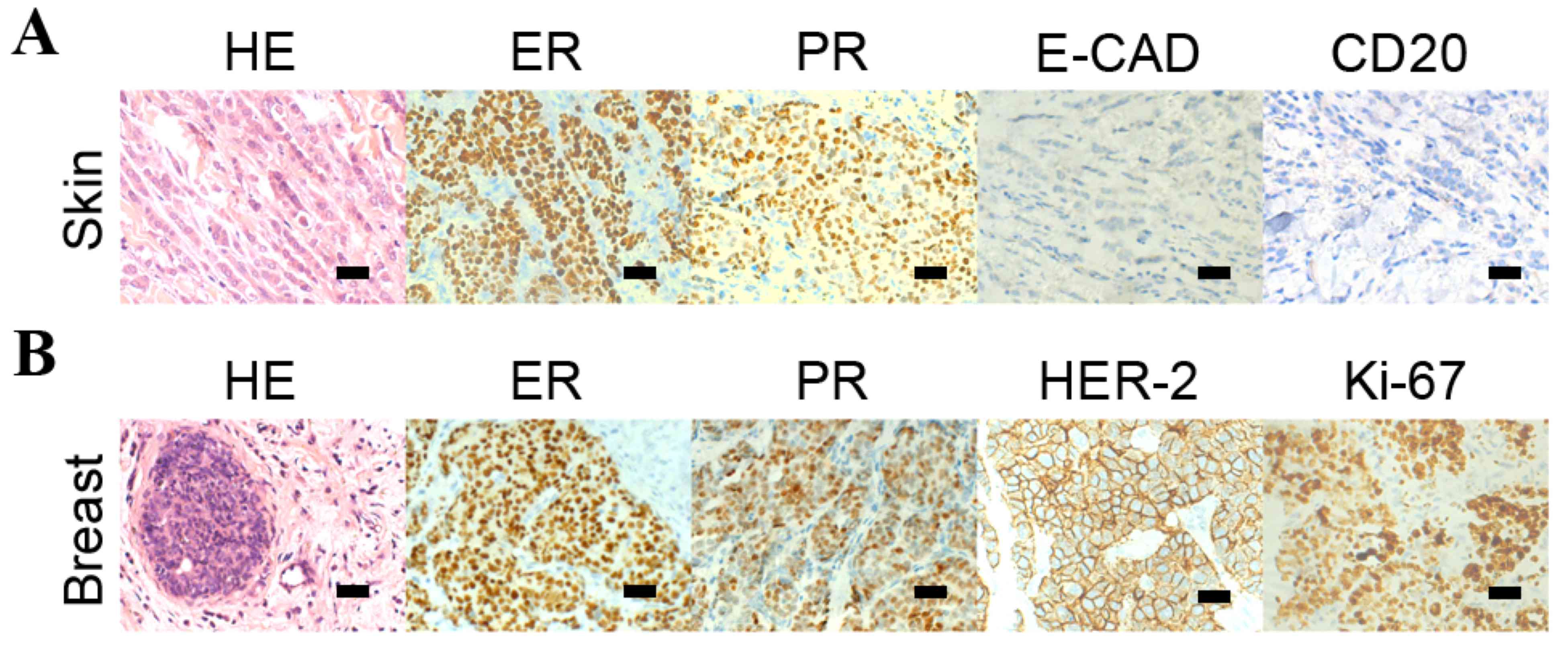
of malignant tumor cells into the dermis. Additionally
immunohistochemistry analysis identified that the tumor cells were
positive for the estrogen receptor (ER) and the progesterone
receptor (PR), but negative for epithelial-cadherin (E-CAD) and
cluster of differentiation (CD) 20 (Fig.
1A) indicating the immunophenotype was consistent with lobular
carcinoma of the breast.
The patient also identified that ~1 year prior to
the onset of gastrointestinal symptoms, they identified the
painless bilateral breast masses but did not present to a
clinician. Subsequently, the patient underwent a bilateral breast
magnetic resonance imaging examination, which identified bilateral
mammary gland hyperplasia and diffuse patchy shadows with nodular
enhancement determined to be category 3 on the Breast Imaging
Reporting and Data System mammographic assessment scale (4). Bilateral breast core biopsies were
performed and the histopathology examination identified invasive
lobular carcinoma (ILC) with positive ER and PR staining (Fig. 1B). In addition, immunohistochemical
stains also exhibited negative HER-2 and weakly positive ki-67
(5%).
The following staging examinations, including chest
and whole brain computed tomography (CT), abdominal ultrasound scan
and bone emission CT identified synchronous metastases in bones,
lungs, pleura and the stomach. The CT scan of the chest of the
patient identified multiple pulmonary nodules and pleural effusion
of the two sides of thorax with a possible lymphangitic metastasis.
Multiple hyperdense lesions in the thoracic vertebrae were
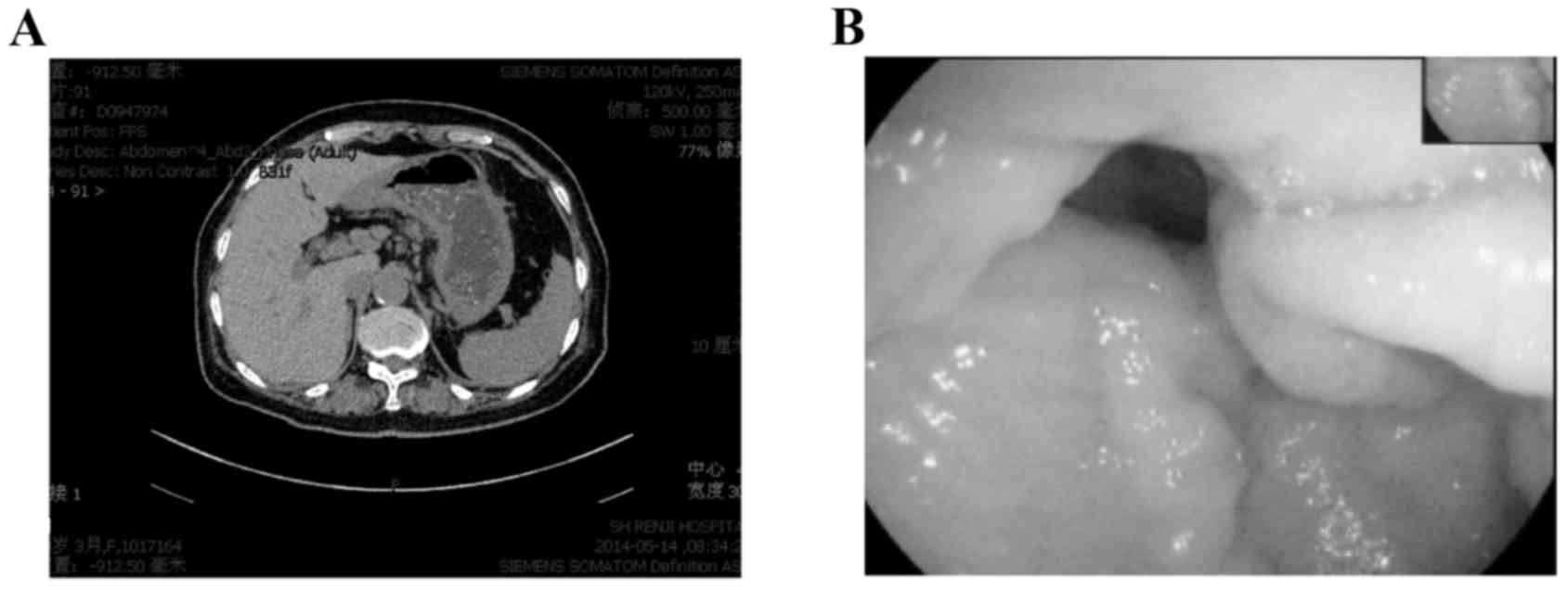
identified. An abdominal CT scan revealed a gastric wall thickening
with characteristics of linitis plastic; however, there was no
evidence of intra-abdominal spread (Fig.
2A). Similarly, gastroscopy evaluation identified rigid gastric
folds with poor distensibility due to the presence of diffuse
infiltrative lesions that involved the entire stomach (Fig. 2B). No evidence of Helicobacter
pylori infection was noted. Pathological analysis of the
endoscopic biopsy samples demonstrated diffuse infiltration with
poorly differentiated adenocarcinoma. Immunohistochemistry analysis
identified that the tumor cells were positive for ER, PR, gross
cystic disease fluid protein (GCDFP) −15 and cytokeratin (CK) 7 but
not for CK20 (Fig. 3) supporting the
diagnosis of a metastatic gastric cancer from the breast carcinoma.
A tumor-marker panel was analysed using a radioimmunoassay as
previously described before (5), and
the results indicated increased levels of cancer antigen (CA)153
(212.90 U/ml), CA125 (502.90 U/ml), CA199 (45.70 U/ml) and
carcinoembryonic antigen (CEA; 21.62 ng/ml). Therefore, the
diagnosis was of the development of lung, bone and stomach
metastases originating from lobular breast cancer.
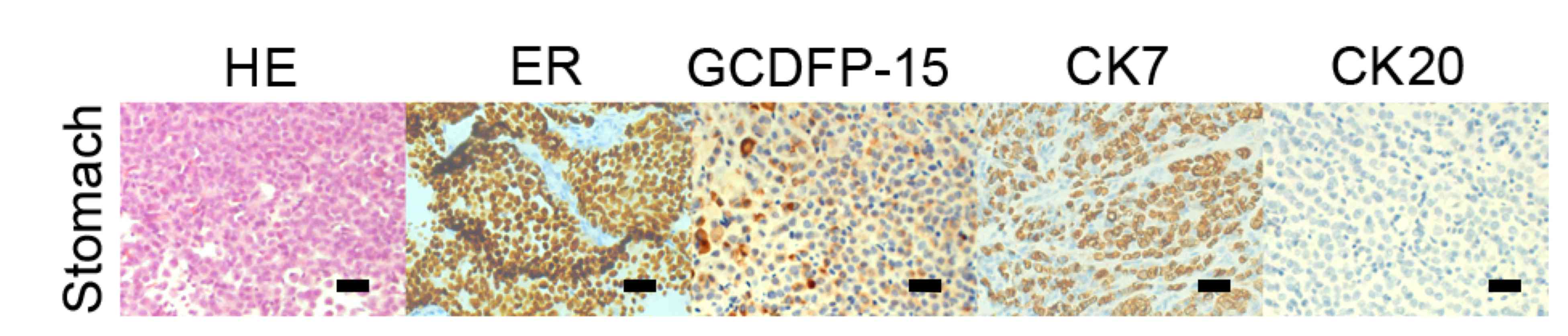 | Figure 3.HE staining and immunohistochemistry
analysis of the gastric metastases HE staining revealed the
malignant cells in the gastric wall, and immunohistochemistry
indicated that cells from the gastric tumor were positive for CK7,
ER and GCDFP-15 and negative for CK20. Scale bar, 50 µm. HE,
hematoxylin and eosin; ER, estrogen receptor, PR, progesterone
receptor; E-CAD, epithelial cadherin; HER-2, human epidermal growth
factor receptor 2; GCDFP-15, gross cystic disease fluid protein 15;
CK7, cytokeratin 7; CK20, cytokeratin 20; CD20, cluster of
differentiation 20. |
Subsequently, zoledronic acid (4 mg every 4 weeks)
was administrated to the patient for the treatment of metastatic
bone disease and to prevent skeletal-related events.
Simultaneously, hormonal therapy (letrozole, 2.5 mg/day) was also
administered. After nine months, the bilateral breast masses and
the chest wall nodules had reduced in volume significantly. The
tumor lesions in the stomach and lungs were stable. Laboratory
examinations indicated a decreased CA125 level to 107.4 U/ml and
CA153 level to 60.57 U/ml. The serum CEA returned to a normal
level. At the 13-month follow-up, the patient's condition remained
asymptomatic in March 2015 and the described treatment was
continued.
Literature search for gastric
metastases from breast cancer
A search of literature using the PubMed website of
data published in English between January 1960 and October 2015 was
performed with the key words ‘stomach OR gastric’, ‘breast cancer’
and ‘metastasis OR metastases’. The reference lists of the original
articles were also searched for relevant studies. The titles,
abstracts and associated citations of the studies that were
identified were reviewed. Only articles with available information
were included in the analysis. The collected data included the
epidemiological information, symptomatology, indications of
endoscopic investigation, macroscopic presentation, time between
primary breast tumor diagnosis and the detection of gastric
metastasis, tumor treatment and prognosis.
Statistical analysis
Survival data was defined as the time from gastric
metastasis until date of mortality or final follow-up and the
median survival and overall survival rates were calculated.
Univariate analyses were performed using the Kaplan-Meier method
and groups were compared using a log-rank test. Multivariate
analysis using the Cox proportional hazards model, including all
factors with P<0.05 from the univariate analysis, was performed
to determine the impact of associated factors. All P-values were
two-sided. All statistical analyses were performed using SPSS
version 21.0 (IBM SPSS, Armonk, NY, USA). P<0.05 was considered
to indicate a statistically significant difference.
Results
Clinicopathological characteristics of
primary breast cancer
A total of 78 cases of primary breast cancer with
gastric involvement were identified in studies obtained via PubMed.
The characteristics of the primary breast cancer cases identified
from the literature search are summarized in Table I. The median age of primary breast
cancer diagnosis was 53 years (range, 33–86; mean, 54.8) and all
patients were female.
 | Table I.Clinicopathological information of
primary breast tumor. |
Table I.
Clinicopathological information of
primary breast tumor.
| Variables | Number of
patients | % |
|---|
| Age, years |
|
<40 | 8 | 10.3 |
|
40–59 | 47 | 60.3 |
|
≥60 | 23 | 29.5 |
|
Median | 53 |
|
| Tumor position |
|
Left | 34 | 43.6 |
|
Right | 25 | 32.1 |
|
Bilateral | 14 | 17.9 |
|
Unknown | 5 | 6.4 |
| Tumor size |
| T0 | 2 | 2.6 |
| T1 | 22 | 28.2 |
| T2 | 29 | 37.2 |
| T3 | 12 | 15.4 |
| T4 | 1 | 1.3 |
|
Unknown | 12 | 15.4 |
| Lymph node
involvement |
|
Positive | 44 | 56.4 |
|
Negative | 20 | 25.6 |
|
Unknown | 14 | 17.9 |
| Stagea |
| 1 | 6 | 7.7 |
| 2 | 28 | 35.9 |
| 3 | 8 | 10.3 |
| 4 | 23 | 29.5 |
|
Unknown | 13 | 16.7 |
| Histology |
|
ILC | 51 | 65.4 |
|
IDC | 19 | 24.4 |
|
Other | 2 | 2.6 |
|
Unknown | 6 | 7.7 |
| ER status |
|
Positive | 49 | 62.8 |
|
Negative | 8 | 10.3 |
|
Unknown | 21 | 26.9 |
| PR status |
|
Positive | 36 | 46.1 |
|
Negative | 17 | 21.8 |
|
Unknown | 25 | 32.1 |
| HER-2 status |
|
Positive | 5 | 6.4 |
|
Negative | 40 | 51.3 |
|
Unknown | 33 | 42.3 |
Tumor size was available in 66/78 cases, and the
majority were identified as T1-stage (28.2%) and T2-stage (37.2%)
breast cancer, according to the 2003 American Joint Committee on
Cancer staging system (6). Two
patients (2.6%) presented with occult breast cancer. The majority
of the patients initially presented with stage II cancer (35.9%)
and the remaining tumours were classified as follows: Stage I,
7.7%; stage III, 10.3%; stage IV, 29.5% (Table I). Stage information was unavailable
in 13 patients (16.7%) due to unknown tumor size or lymph node
status. A total of 51 patients (65.4%) had a history of breast ILC,
whereas only 19 patients (24.4%) were identified with a history of
breast invasive ductal carcinoma (IDC). Additionally, lymph node
involvement was detected in 44 patients (56.4%), whereas 22
patients (25.9%) had no nodal involvement. In the present study, ER
and PR expression levels were positive in 49 cases (62.8%) and 45
(46.1%) cases, respectively. Human epidermal growth factor
receptor-2 (HER-2) status was available in 67 cases and only 7
cases (6.4%) were positive (Table
I).
Clinicopathological characteristics of
gastric metastasis
The clinicopathological characteristics of patients
with gastric metastasis are presented in Table II. The median age at the gastric
metastasis diagnosis was 59 years (range, 38–86; mean, 60.9). The
median interval between the primary diagnosis and metastatic
presentation was 60 months (range, 0–252; mean, 70.7). Gastric
metastasis was identified at the same time as the breast cancer
diagnosis in 18 patients (23.1%). A total of 14 patients sought the
initial consultation for gastrointestinal symptoms prior to the
breast cancer being diagnosed (17.9%).
| Table II.Log-rank analysis of clinical
characteristics of gastric metastases with overall survival
rate. |
Table II.
Log-rank analysis of clinical
characteristics of gastric metastases with overall survival
rate.
|
Characteristics | Number of patients
(%) | P-value |
|---|
| Age at diagnosis of
gastric metastases, years |
| 0.166 |
|
0–49 | 12 (15.4) |
|
|
≥50 | 66 (84.6) |
|
| Time between
primary and secondary cancers, years |
| 0.998 |
|
0–2 | 28 (35.9) |
|
| ≥2 | 48 (60.3) |
|
|
Unknown | 2 (2.6) |
|
| Location of
lesion |
| 0.160 |
| Upper
3rd | 16 (20.5) |
|
| Middle
3rd | 14 (17.9) |
|
| Lower
3rd | 23 (29.5) |
|
| Whole
stomach | 18 (23.1) |
|
|
Unknown | 5 (6.4) |
|
| Solitary lesion in
stomach |
| 0.025 |
|
Yes | 36 (46.2) |
|
| No | 40 (51.3) |
|
|
Unknown | 2 (2.6) |
|
| Any other
metastases prior to stomach involved |
| 0.006 |
|
Yes | 27 (34.6) |
|
| No | 43 (55.1%) |
|
|
Unknown | 8 (10.3) |
|
| Any other
metastases when stomach involved |
| 0.048 |
|
Yes | 49 (62.8) |
|
| No | 29 (37.2) |
|
| Peritoneal
carcinomatosis |
| 0.005 |
|
Yes | 36 (46.2) |
|
| No | 41 (52.7) |
|
|
Unknown | 1 (1.3) |
|
| Main symptom |
| 0.765 |
|
Abdominal pain | 59 (75.6) |
|
|
Anorexia | 45 (57.7) |
|
|
Bleeding | 6 (7.7) |
|
|
Dysphagia | 4 (5.1) |
|
|
Vomiting | 15 (19.2) |
|
|
Asymptomatic | 5 (6.4) |
|
A total of 27 patients were identified as having
other organs that had already been affected when the diagnosis of
gastric metastases was established (34.6%). Furthermore,
co-existing metastases in other tissues were present in <62.8%
of cases at the time of diagnosis of the stomach metastasis
(Table II). The majority of
additional metastases were located in the bone (50.0%), colon
(24.4%), liver (20.4%) and lung (12.2%) (data not shown).
The majority of gastric metastases of breast cancer
manifested as nonspecific symptoms, including dyspepsia, anorexia,
bloating, melena, nausea, vomiting, early satiety and epigastric
pain. Abdominal pain was the most frequent symptom in the current
study (75.6%). Endoscopy evaluation is essential in the diagnosis
of gastric metastatic disease due to the diversity of clinical
manifestations in the patients with gastric metastases. The
evaluation of endoscopic information identified 16 patients that
had lesions in the upper third of the stomach (20.5%), 14 patients
(17.9%) that had lesions in the middle third of the stomach and 23
patients that had lesions in the lower third of the stomach (29.5%;
Table II). Solitary lesions in the
stomach were identified in 36 cases (46.2%) and 40 patients were
identified to have multiple gastric metastatic lesions (51.3%;
Table II). Additionally, ER and PR
status were able to be assessed in 50 and 41 cases, respectively,
and the majority of gastric metastases were hormonal receptor
positive (ER for 94.0% and PR for 68.3%). However, in the 34 cases
with HER-2 information, only 2/34 cases were HER-2 positive (5.9%;
Table II).
Following the discovery of gastric metastatic
disease, the majority of patients received salvage chemotherapy
(56.4%) or salvage hormonal therapy (51.3%). Surgeries that were
performed included total gastrectomy, subtotal gastrectomy and
wedge resection, which were performed in a total of 32 patients
(41.0%). A small number of patients were treated with radiotherapy
(7.7%; Table III).
| Table III.Treatment modalities and their
association with overall survival rate in patients with breast
cancer with stomach metastases. |
Table III.
Treatment modalities and their
association with overall survival rate in patients with breast
cancer with stomach metastases.
|
Characteristics | Number of patients
(%) | P-value |
|---|
| Surgery |
| 0.134 |
|
Yes | 32 (41.0) |
|
| No | 42 (53.8) |
|
|
Unknown | 4 (5.1) |
|
| Chemotherapy |
| 0.182 |
|
Yes | 44 (56.4) |
|
| No | 28 (35.9) |
|
|
Unknown | 6 (7.7) |
|
| Radiotherapy |
| 0.951 |
|
Yes | 6 (7.7) |
|
| No | 68 (87.2) |
|
|
Unknown | 4 (5.1) |
|
| Hormonal
therapy |
| 0.032 |
|
Yes | 40 (51.3) |
|
| No | 31 (39.7) |
|
|
Unknown | 5 (6.4) |
|
Patient survival
The follow-up data was available for 74 patients.
The median survival was 10.5 months (range, 0.25–116). The
univariate analysis for the association between overall survival
(OS) rate and clinicopathological and biological characteristics of
the primary breast tumor and gastric metastasis was performed.
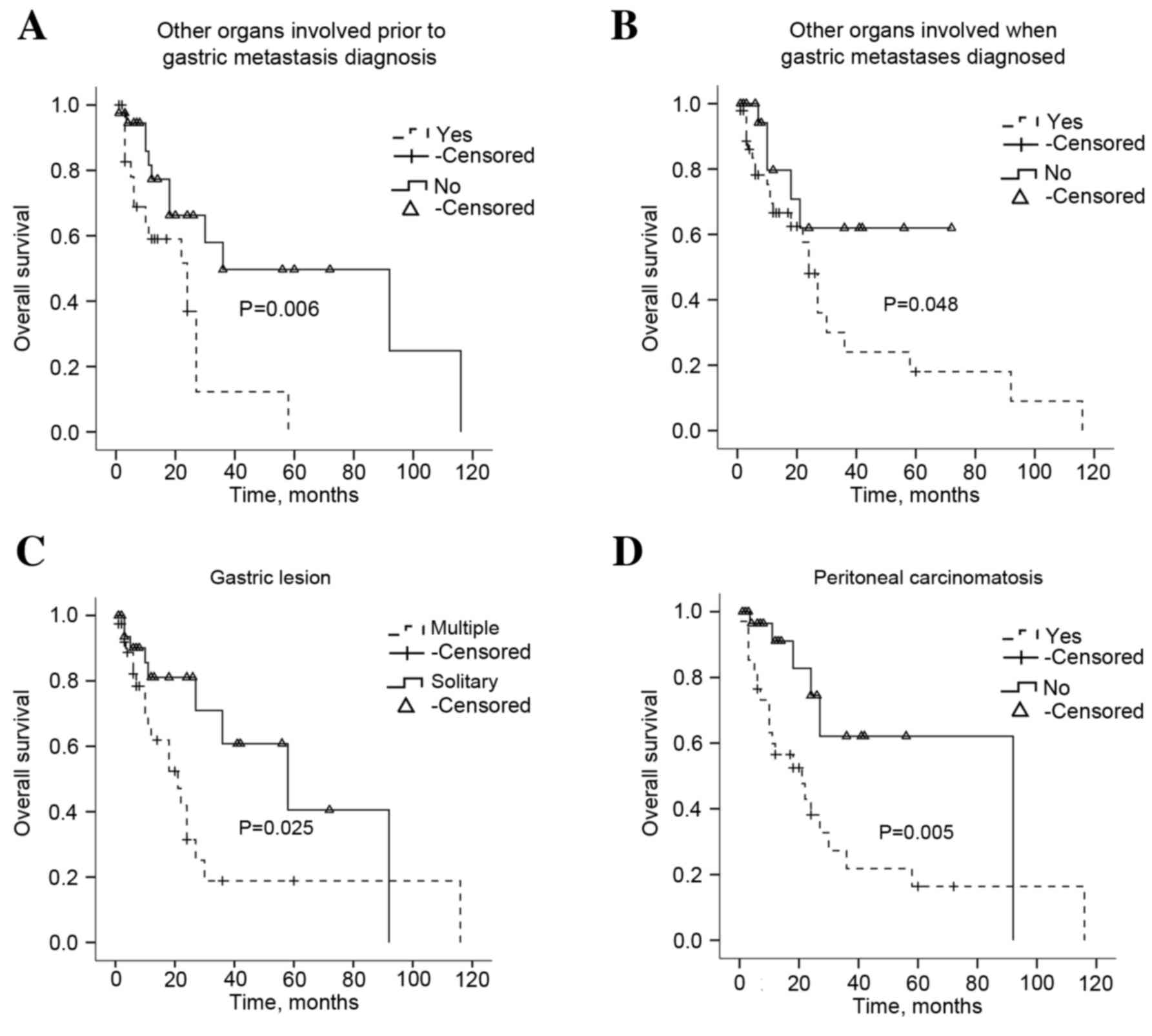
According to the univariate analysis, multiple organ involvement
prior to or at the time of gastric metastatic disease diagnosis and
the presence of multiple gastric lesions, or peritoneal
carcinomatosis were significantly correlated with OS (P=0.006,
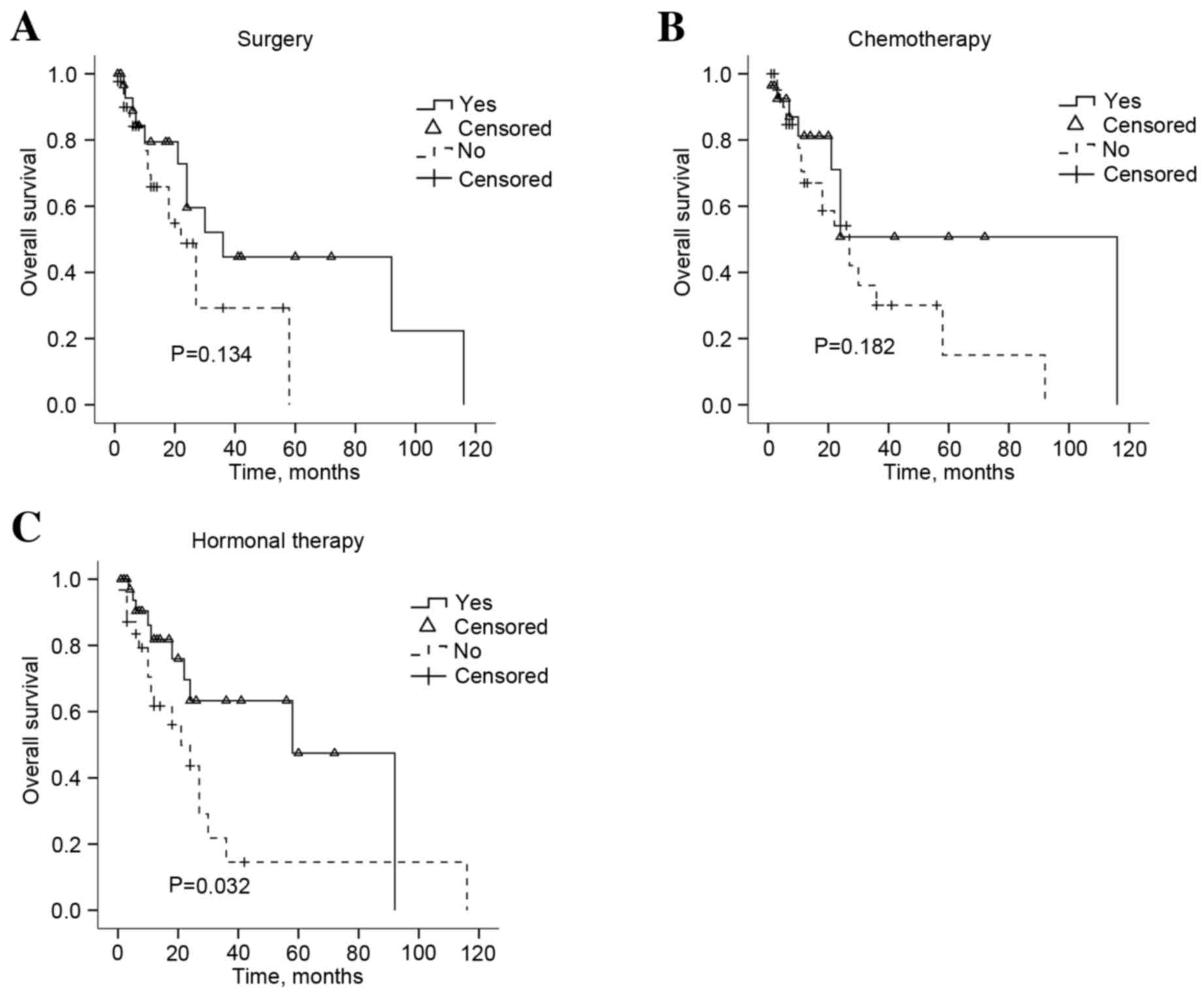
P=0.048, P=0.025 and P=0.005, respectively; Fig. 4). Treatment modalities were also
investigated and salvage hormonal therapy (P=0.0320), but not
surgery or chemotherapy (P=0.134, P=0.182, respectively),
significantly extended the OS (Fig.
5). The survival analysis also identified that the patient age
and the time interval between primary disease and gastric
metastasis did not prolong the survival of patients with gastric
metastases (Table II; P=0.166 and
P=0.998, respectively). Multivariate analysis indicated that any
other metastasis exist prior to stomach was an independent
indicator of poor OS (P=0.011; Table
IV).
| Table IV.Multivariate analysis of prognostic
factors for OS in patients with gastric metastases. |
Table IV.
Multivariate analysis of prognostic
factors for OS in patients with gastric metastases.
| Variables | B | SE | Wald | P-value | OR | 95% CI |
|---|
| Other metastases
prior to stomach involvement | −1.127 | 0.445 | 6.414 | 0.011 | 0.324 | 0.135–0.775 |
| Other metastases
when stomach involved | −0.317 | 0.642 | 0.243 | 0.622 | 0.729 | 0.207–2.564 |
| Salvage hormonal
therapy | 0.749 | 0.442 | 2.864 | 0.091 | 2.114 | 0.888–5.030 |
| Solitary lesion in
stomach | 0.25 | 0.436 | 0.33 | 0.566 | 1.285 | 0.547–3.019 |
| Peritoneal
carcinomatosis | −0.717 | 0.484 | 2.192 | 0.139 | 0.488 | 0.189–1.261 |
Discussion
Metastatic involvement of the stomach secondary to
breast cancer is rare and its management varies significantly from
that of a primary gastric cancer (7).
A previous study reported a retrospective series of breast cancer
metastases with an incidence of metastasis to the stomach of 0.1%
(8). However, another study
investigating the autopsies of 1,010 patients with cancer
identified that gastric metastases were detected in 17 patients,
yielding an incidence rate of <1.7% (9). It was previously hypothesized that
gastric metastases of breast cancer have been underestimated in the
history of breast cancer diagnosis (10). This may occur primarily as a result of
the diverse and nonspecific symptoms at clinical presentation,
indistinguishable radiological and endoscopic features and the
potentially lengthy disease-free survival period of patients with
gastric metastases from breast cancer (11–13).
Therefore, novel studies investigating the diagnosis and treatment
received by patients with gastric metastasis from breast cancer are
required to improve the therapeutic outcomes for this group.
Of the patients with gastric metastases, the
prevalent primary sites were breast cancer (27.9%), followed by
lung cancer (23.8%), esophageal cancer (19.1%), renal cell
carcinoma (7.6%) and malignant melanoma (7.0%) (14). This may reflect the high incidence of
breast cancer and lung cancer in the general population (11). Concordant with previous studies
(8,15,16),
gastric metastases from breast cancer developed more frequently
from ILC (65.4%) compared with IDC (24.4%; Table I). ILC comprises ~15% of breast cancer
cases and has clinical, biological and molecular distinctions
compared with IDC (15). Borst et
al (16) reported the metastatic
patterns of ILC and IDC differ considerably. ILC has a greater
propensity towards metastasizing to the gastrointestinal tract,
gynaecological organs, peritoneum, retroperitoneum, adrenal glands
and bone marrow (17,18) and IDC frequently metastasizes to the
lung, bones and liver (19). The
factors that account for this variation in metastatic patterns are
yet to be elucidated. A previous study hypothesized that the
distinct ILC transcriptomic signature may be associated with
metastatic behaviour (20). Fernandes
et al (21) also reported that
the absence of the cell-cell adhesion molecule E-CAD decreased the
adhesiveness of tumor cells and may be responsible for the
metastatic patterns of ILC. The incidence of ILC has been
increasing over the previous two decades and this may occur as a
result of the use of replacement hormonal therapy and improvements
in diagnostic practice (22,23). Therefore, the number of patients with
gastric metastases that develop from breast cancer may also
increase.
Due to nonspecific symptoms including dysphagia,
dyspepsia, anorexia, abdominal pain, early satiety, nausea and
vomiting and bleeding, the clinical presentation of gastric
metastases from breast cancer mimics a primary gastric tumor
(24). Concordant with previous
studies, abdominal pain was the most common symptom in the current
study (75.6%; Table II). The pain
associated with gastric metastasis is typically mild and localized
to the epigastric region, which may mimic peptic ulcer disease and
be relieved by eating. Furthermore, gastric metastases may develop
several years following the initial diagnosis in patients with
breast cancer (25). The median time
between the diagnosis of primary breast cancer and gastric
involvement was 60 months in the present study (Table II). Therefore, a patient with ILC
that has been disease-free for several years may still be at risk
of gastric metastases and exhibit gastrointestinal symptoms.
Notably, gastric metastasis frequently occurs with synchronously
with other sites of metastases (11,24). In
the current study, systemic metastases to other locations were
detected in 27 patients prior to the diagnosis of gastric
metastases (34.6%). At the time of gastric metastasis diagnosis, 49
patients had concurrent metastases, which typically occurred in the
bone (50%), lung (12.2%) and liver (20.4%). Taken together, the
present study emphasizes the importance of a comprehensive
examination at the time of diagnosis of a patient's gastric
metastasis, which may aid clinicians in providing an accurate
diagnosis and an earlier initiation of effective treatment.
Breast cancer with stomach involvement presents a
diagnostic challenge. Endoscopic investigation followed by a biopsy
is the required procedure to provide a definitive diagnosis and
histological comparisons between biopsy samples and the prior
breast carcinoma specimens is recommended (12,14). Kim
et al (11) had identified
three main morphological features of gastric metastases in
endoscopic examination as follows: Submucosal tumor masses with
elevation and tip ulceration; non-ulcerative masses; multiple
nodules of varying sizes. In the current study, gastric lesions
were described as polypoid masses or volcano-like ulcers and mostly
involved the lower third of the stomach, including the antrum and
pylorus. However, gastric metastases that have spread throughout
the mucosa and gastric wall may resemble primary gastric cancer,
making clinical management problematic. Primary gastric diffuse
signet-ring cell carcinoma and lobular breast carcinoma exhibit
similar morphological features and these two neoplasms may be
indistinguishable without further investigation (26). Furthermore, primary stomach cancer is
also able to metastasize to the breast, which may complicate the
diagnosis (27,28). The use of a variety of methods,
including immunochemistry, may be helpful to differentiate gastric
metastasis with morphologically similar tumors and tumors of
unknown origin. In the present study, the majority of the
metastatic breast carcinomas were ER-, PR-, GCDFP-15 and CEA-
positive and CK20-negative (Fig. 1)
(29), whereas a primary stomach
cancer is typically CK7- and CK20-positive and ER- and
mammaglobin-negative (30). However,
as an established mediator of the carcinogenic process, HER-2 is
dysregulated in a number of types of solid tumor, including breast
and stomach cancer (31) and
therefore it may not be a suitable diagnostic marker for gastric
metastasis from breast cancer. Taken together, it may be important
for clinicians to not solely rely on the tumor biomarkers for the
accurate diagnosis and treatment of gastric metastasis, due to the
lack of a specific immunohistochemistry marker for breast cancer
(32) and that the tumor phenotype
may be unstable throughout the disease progression (33). Therefore, the diagnosis and
appropriate treatment of gastric metastases of breast cancer may be
improved using a diverse approach from the clinician along with the
use of numerous diagnostic methods that aid pathological
diagnosis.
To the best of our knowledge, a small number of
studies have been reported to investigate the prognostic factors
and standard treatment strategies for gastric metastases of breast
cancer due to the low incidence rate. Certain previous studies
advocated systemic therapy for the cases of breast cancer that have
metastasized to the stomach, rather than using surgery as a primary
treatment option (12,34). Surgery may only be considered in cases
of acute complications, including stomach bleeding, obstruction and
perforation, to improve quality of life (10,14).
However, other studies also hypothesized that surgery may be the
optimal first-line treatment for operable solitary breast cancer
metastasis to the stomach (29,35). As
presented in Fig. 4A and B, survival
analysis identified that surgical intervention and chemotherapy did
not significantly extend OS (P=0.134 and P=0.182, respectively),
whereas hormonal therapy was demonstrated to be an effective
strategy (P=0.032; Fig. 4). This was
partly as the hormonal receptors are typically positive in patients
with gastric metastases. As aforementioned, gastric metastases from
breast cancer are more typical in ILC (Table I) and ILC tissues were significantly
more likely to be ER and PR-positive (18,36).
Therefore, the present study hypothesizes that the biological
features of the primary breast tumors may partly contribute to the
sensitivity to hormonal therapy of gastric metastases. Concordant
with previous studies (24,37), the present study demonstrated that low
HER-2 expression was identified in gastric lesions (6.4%). Although
trastuzumab (Herceptin) has been approved for the treatment of
advanced metastatic gastric cancer with a positive HER-2 status, as
defined by an immunohistochemistry 3+ result (38), this group of patients were rarely
treated with anti-HER2-targeted therapy. Further studies are
important to evaluate the role of targeted therapy for this rare
disease phenotype.
In conclusion, the present study indicated that
systemic treatment strategies, including hormonal therapy, may be
the optimal choice for gastric metastasis from breast cancer. The
described case demonstrated that hormonal therapy was able to
control the disease and provided a lengthy duration of relapse-free
survival. Several limitations should be considered when
interpreting the results of the present study. Firstly, the present
study is retrospective and had a long duration and thus, the
patients were heterogenous. In addition, the treatment modalities
and the primary breast carcinoma features were heterogenous among
distinct medical centres. In addition, the specific information
concerning the primary tumor and follow-up was unavailable. The
current study focuses on the contributing factors of survival and
appropriate treatments for patients with breast cancer with gastric
metastases. Prospective studies with a longer follow-up time and
higher patient numbers may allow an improved understanding of the
biological, pathological and clinicopathological characteristics,
the clinical outcomes and the endoscopic features associated with
gastric metastases from breast cancer.
Acknowledgements
This study was supported by The National Natural
Science Foundation of China (grant nos. 81172522 and 81301858).
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015: CA Cancer J Clin. 65:5–29. 2015.
|
|
2
|
Wang H, Zhang C, Zhang J, Kong L, Zhu H
and Yu J: The prognosis analysis of different metastasis pattern in
patients with different breast cancer subtypes: A SEER based study.
Oncotarget. Dec 27–2016.(Epub ahead of print). View Article : Google Scholar
|
|
3
|
Koike K, Kitahara K, Higaki M, Urata M,
Yamazaki F and Noshiro H: Clinicopathological features of gastric
metastasis from breast cancer in three cases. Breast Cancer.
21:629–634. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cheng L and Li X: Breast imaging reporting
and datasystem (BI-RADS) of magnetics resonance imaging: Breast
mass. Gland Surg. 1:62–74. 2012.PubMed/NCBI
|
|
5
|
Bast RC Jr, Klug TL, St John E, Jenison E,
Niloff JM, Lazarus H, Berkowitz RS, Leavitt T, Griffiths CT, Parker
L, et al: A radioimmunoassay using a monoclonal antibody to monitor
the course of epithelial ovarian cancer. N Engl J Med. 309:883–887.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Singletary SE, Allred C, Ashley P, Bassett
LW, Berry D, Bland KI, Borgen PI, Clark GM, Edge SB, Hayes DF, et
al: Staging system for breast cancer: Revisions for the 6th edition
of the AJCC cancer staging manual. Surg Clin North Am. 83:803–819.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Almubarak MM, Laé M, Cacheux W, de Cremoux
P, Pierga JY, Reyal F, Bennett SP, Falcou MC, Salmon RJ, Baranger B
and Mariani P: Gastric metastasis of breast cancer: A single centre
retrospective study. Dig Liver Dis. 43:823–827. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Abid A, Moffa C and Monga DK: Breast
cancer metastasis to the GI tract may mimic primary gastric cancer.
J Clin Oncol. 31:e106–e107. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Taal BG, Boot H, van Heerde P, de Jong D,
Hart AA and Burgers JM: Primary non-Hodgkin lymphoma of the
stomach: Endoscopic pattern and prognosis in low versus high grade
malignancy in relation to the MALT concept. Gut. 39:556–561. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zelek L, Cottu PH, Mignot L, de
Roquancourt A, Fizazi K, Cojean-Zelek I, Espie M and Marty M:
Gastric metastases from breast cancer: A retrospective series of 12
patients. Am J Clin Oncol. 24:363–365. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Takeuchi H, Hiroshige S, Yoshikawa Y,
Kusumoto T and Muto Y: A case of synchronous metastasis of breast
cancer to stomach and colon. Anticancer Res. 32:4051–4055.
2012.PubMed/NCBI
|
|
12
|
Taal BG, Peterse H and Boot H: Clinical
presentation, endoscopic features and treatment of gastric
metastases from breast carcinoma. Cancer. 89:2214–2221. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim GH, Ahn JY, Jung HY, Park YS, Kim MJ,
Choi KD, Lee JH, Choi KS, do Kim H, Lim H, et al: Clinical and
endoscopic features of metastatic tumors in the stomach. Gut Liver.
9:615–622. 2015.PubMed/NCBI
|
|
14
|
Namikawa T and Hanazaki K:
Clinicopathological features and treatment outcomes of metastatic
tumors in the stomach. Surg Today. 44:1392–1399. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Van Trappen P, Serreyn R, Elewaut AE,
Cocquyt V and Van Belle S: Abdominal pain with anorexia in patients
with breast carcinoma. Ann Oncol. 9:1243–1245. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Schwarz RE, Klimstra DS and Turnbull AD:
Metastatic breast cancer masquerading as gastrointestinal primary.
Am J Gastroenterol. 93:111–114. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Borst MJ and Ingold JA: Metastatic
patterns of invasive lobular versus invasive ductal carcinoma of
the breast. Surgery. 114:637–642. 1993.PubMed/NCBI
|
|
18
|
Arpino G, Bardou VJ, Clark GM and Elledge
RM: Infiltrating lobular carcinoma of the breast: Tumor
characteristics and clinical outcome. Breast Cancer Res.
6:R149–R156. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sobinsky JD, Willson TD, Podbielski FJ and
Connolly MM: Unusual metastatic patterns of invasive lobular
carcinoma of the breast. Case Rep Oncol Med.
2013:9865172013.PubMed/NCBI
|
|
20
|
Gruel N, Lucchesi C, Raynal V, Rodrigues
MJ, Pierron G, Goudefroye R, Cottu P, Reyal F, Sastre-Garau X,
Fourquet A, et al: Lobular invasive carcinoma of the breast is a
molecular entity distinct from luminal invasive ductal carcinoma.
Eur J Cancer. 46:2399–2407. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fernandes GS, Corrêa TS, Carvalho EP, Katz
A and Hoff PM: Gastric and endobronchial metastases in a case of
lobular breast cancer. Case Rep Oncol. 6:555–560. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Arrangoiz R, Papavasiliou P, Dushkin H and
Farma JM: Case report and literature review: Metastatic lobular
carcinoma of the breast an unusual presentation. Int J Surg Case
Rep. 2:301–305. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bharat A, Gao F and Margenthaler JA: Tumor
characteristics and patient outcomes are similar between invasive
lobular and mixed invasive ductal/lobular breast cancers but differ
from pure invasive ductal breast cancers. Am J Surg. 198:516–519.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pectasides D, Psyrri A, Pliarchopoulou K,
Floros T, Papaxoinis G, Skondra M, Papatsibas G, Macheras A,
Athanasas G, Arapantoni-Datioti P and Economopoulos T: Gastric
metastases originating from breast cancer: Report of 8 cases and
review of the literature. Anticancer Res. 29:4759–4763.
2009.PubMed/NCBI
|
|
25
|
Ricciuti B, Leonardi GC, Ravaioli N, De
Giglio A, Brambilla M, Prosperi E, Ribacchi F, Meacci M, Crinò L,
Maiettini D, et al: Ductal breast carcinoma metastatic to the
stomach resembling primary linitis plastica in a male patient. J
Breast Cancer. 19:324–329. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yoshida Y: Metastases and primary
neoplasms of the stomach in patients with breast cancer. Am J Surg.
125:738–743. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sataloff DM, Dentchev D, Henry DH and
Weese JL: Isolated breast metastases from primary gastric
adenocarcinoma. Breast J. 6:622000. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sato T, Muto I, Fushiki M, Hasegawa M,
Hasegawa M, Sakai T and Sekiya M: Metastatic breast cancer from
gastric and ovarian cancer, mimicking inflammatory breast cancer:
Report of two cases. Breast Cancer. 15:315–320. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sarkut P, Ozer A, Gulcu B, Ozturk E,
Gokgoz S and Ugras N: An extremely rare cause of gastric outlet:
Breast lobular carcinoma metastases to stomach. Breast J.
20:312–313. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tot T: The role of cytokeratins 20 and 7
and estrogen receptor analysis in separation of metastatic lobular
carcinoma of the breast and metastatic signet ring cell carcinoma
of the gastrointestinal tract. APMIS. 108:467–472. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Martin V, Cappuzzo F, Mazzucchelli L and
Frattini M: HER2 in solid tumors: More than 10 years under the
microscope; where are we now? Future Oncol. 10:1469–1486. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Brown RW, Campagna LB, Dunn JK and Cagle
PT: Immunohistochemical identification of tumor markers in
metastatic adenocarcinoma. A diagnostic adjunct in the
determination of primary site. Am J Clin Pathol. 107:12–19. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Guarneri V, Giovannelli S, Ficarra G,
Bettelli S, Maiorana A, Piacentini F, Barbieri E, Dieci MV, D'Amico
R, Jovic G and Conte P: Comparison of HER-2 and hormone receptor
expression in primary breast cancers and asynchronous paired
metastases: Impact on patient management. Oncologist. 13:838–844.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Dassen AE, Lips DJ, Hoekstra CJ, Pruijt JF
and Bosscha K: FDG-PET has no definite role in preoperative imaging
in gastric cancer. Eur J Surg Oncol. 35:449–455. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Gadde R, Tamariz L, Hanna M, Avisar E,
Livingstone A, Franceschi D and Yakoub D: Metastatic gastric cancer
(MGC) patients: Can we improve survival by metastasectomy? A
systematic review and meta-analysis. J Surg Oncol. 112:38–45. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wasif N, Maggard MA, Ko CY and Giuliano
AE: Invasive lobular vs. ductal breast cancer: A stage-matched
comparison of outcomes. Ann Surg Oncol. 17:1862–1869. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ambroggi M, Stroppa EM, Mordenti P,
Biasini C, Zangrandi A, Michieletti E, Belloni E and Cavanna L:
Metastatic breast cancer to the gastrointestinal tract: Report of
five cases and review of the literature. Int J Breast Cancer.
2012:4390232012. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Spackman E, Rice S, Norman G, Suh DC,
Eastwood A and Palmer S: Trastuzumab for the treatment of
HER2-positive metastatic gastric cancer: A NICE single technology
appraisal. Pharmacoeconomics. 31:185–194. 2013. View Article : Google Scholar : PubMed/NCBI
|