Introduction
Colorectal cancer (CRC) constitutes the third most
frequent type of cancer worldwide (1). Approximately 50% of all patients with
CRC develop liver metastases (LMs) (2,3).
Hepatectomy is generally regarded as the most effective and
potentially curative treatment for patients with colorectal liver
metastases (CRLMs), with a 5-year survival rate of 40–50% (4–6). Due to
recent advances in the development of surgical techniques and
peri-operative therapy, an aggressive approach to hepatic
metastases resection has been widely adopted. However, not all
patients with technically resectable liver-limited metastases
benefit from surgery, with >50% of patients developing
recurrence within 2 years after resection (7,8). Many
prognostic factors have emerged for predicting survival in patients
with CRLMs after hepatectomy, the most common criteria for patient
selection and recurrence prediction are based on the clinical risk
score system (CRS) presented by Fong et al (9). Numerous studies have confirmed that
patients in high-risk group (CRS ≥3) would have a significantly
shorter overall survival (OS) than patients in the low-risk (CRS
<3) group (6,10–12).
However, the validity of CRS has recently been debated as it was
based on treatment outcomes of patients in 1990s, prior to the
implementation of current chemotherapy regimens (13,14).
Neo-adjuvant chemotherapy (NACT) has been widely
adopted for the treatment of patients with resectable CRLMs, not
only in prolonging progression-free survival (15), but also in downsizing the tumors to
preserve a larger volume of liver parenchyma, making surgery easier
(16,17). However, tumor progression does occur
in approximately 5–10% of patients after NACT (18,19).
Numerous studies have demonstrated that a tumor's response to
pre-operative chemotherapy (TRC) is an important predictive factor
for evaluating long-term survival in patients with CRLMs (18–20).
However, whether patients could benefit from liver resection after
tumor progression during NACT remains controversial. In addition,
although both the Fong's CRS system (9) and the TRC can predict a patient's
oncological status, it is unknown whether a combination of the CRS
system and the TRC (CRS-TRC classification) could improve the
predictive accuracy of survival in patients with CRLMs. Therefore,
the aim of our study was to evaluate which patients are suitable
for hepatectomy after underwent tumor pregression during
chemotherapy, and the value of CRS-TRC classification in predicting
survival and selecting patients with CRLMs for curative
therapy.
Materials and methods
Patient selection
A total of 425 patients with CRLMs underwent
hepatectomy between January 2005 and December 2015 in the
Hepatopancreatobiliary Surgery Department I at the Beijing Cancer
Hospital and Institute (Beijing, China). Patients were screened on
the following exclusion criteria: Concurrent unresectable
extrahepatic metastases; no R0 resection; repeated hepatectomy due
to liver recurrences; and unavailable TRC data. All study
participants provided informed written consent, and the study was
approved by the Ethical Review Board committee of the Beijing
Cancer Hospital and Institute.
Study design
The tumor response was evaluated after every two
cycles of NACT based on computed tomography (CT) or magnetic
resonance (MR) images, using the Response Evaluation Criteria in
Solid Tumors (v.1.1) (21). The good
TRC group (response to NACT) included patients with a complete or
partial response and those with a response within a stable disease
status (a reduction in the sum of tumor diameters of <30%),
while the bad TRC group comprised of patients with a progressive
disease or progression within a stable disease status (an increase
in the sum of the diameters of the target lesion of <20%). In
patients who received multiple lines of chemotherapy, the tumor
response to the last regimen was considered. According to the CRS
system patients were classified into a either a high-risk (CRS ≥3)
or a low-risk (CRS <3) group (9).
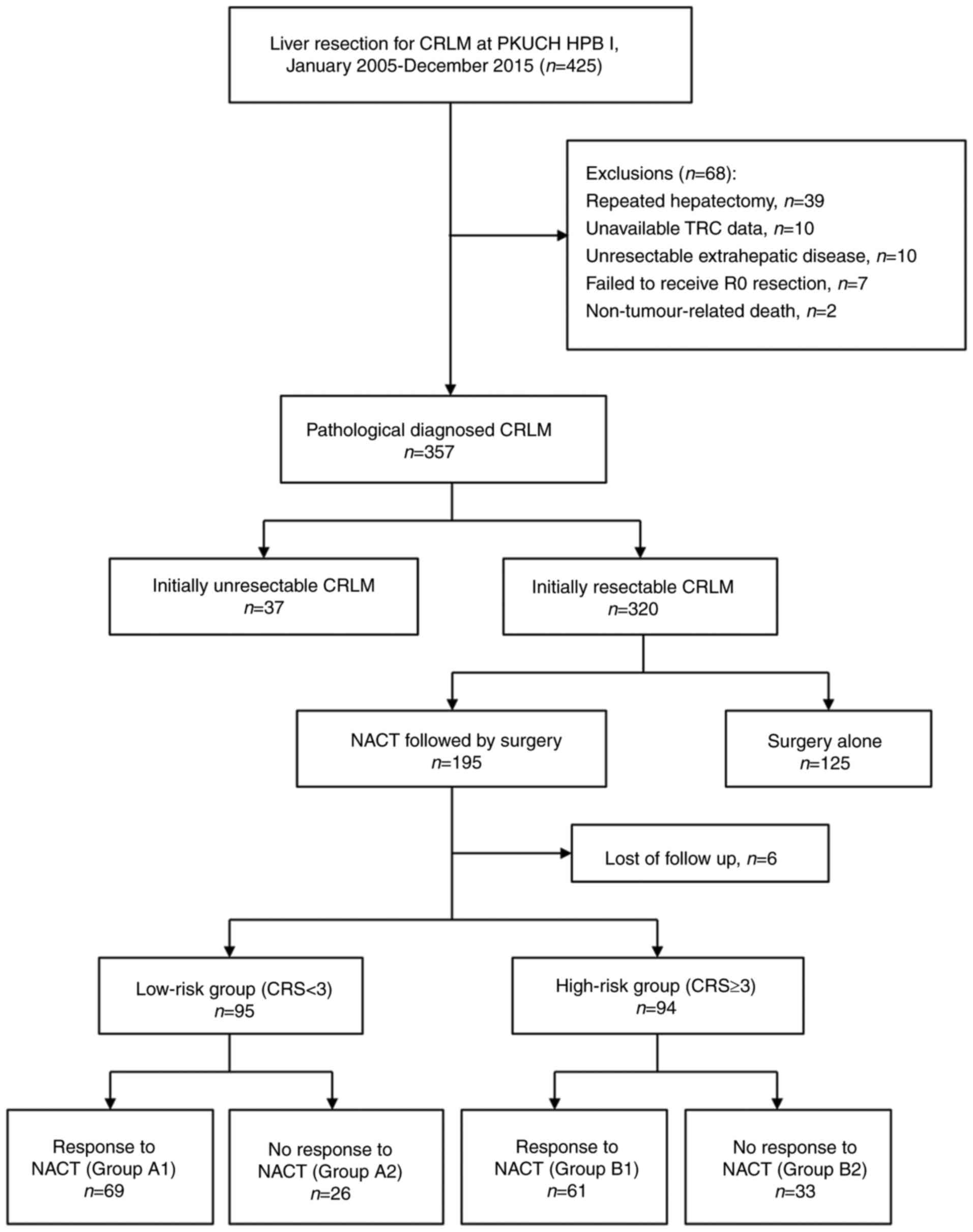
We further subclassified patients using our new combined CRS-TRC
classification, shown in Fig. 1, into
the following subgroups: Group A1, low CRS and good TRC; group A2,
low CRS and bad TRC; group B1, high CRS and good TRC; and group B2,
high CRS and bad TRC. Clinical outcomes and survival were evaluated
between these subgroups.
Pre-operative management and
neo-adjuvant chemotherapy
A multidisciplinary team meeting is routinely
conducted each week at our centre. Gadoxetic acid/contrast-enhanced
MR imaging was routinely performed in every CRLMs patients.
Positron emission tomography-CT scans performed for patients with
suspected extrahepatic metastases. In general, patients received
2–6 cycles of NACT (22). A modern
chemotherapy regime for all cases, using oxaliplatin- or
irinotecan-based chemotherapy, in combination with targeted therapy
using cetuximab or bevacizumab determined on a per-patient basis
using the RAS mutation status. The time interval between the date
of the last chemotherapy session and hepatic surgery was usually 4
weeks, extending to 6–8 weeks for patients who received
bevacizumab.
Patient selection for liver resection
and operative technique
LMs were considered resectable provided the
following criteria were met: i) The possibility of R0 resection
with a liver remnant of ≥30% and sufficient hepatic blood inflow
and outflow, and ii) no evidence of unresectable extrahepatic
metastases (23,24). Hepatic resections were performed using
the parenchymal sparing method (9)
with a resection margin of >1 mm. An ablation technique
(25,26) was performed, in combination with
resection surgery, for tumors that were deep and technically
difficult to resect.
Post-operative outcomes and
follow-up
Contrast-enhanced CT scans or MR imaging, liver
function and carcinoembryonic antigen levels were performed every 3
months within the first 2 years, and then every 6 months after
operation.
Statistical analysis
Continuous variables were presented as the mean and
standard deviation or the median and interquartile range. Discreet
variables were presented as the number and percentage.
Between-group differences were evaluated using a chi-squared test
for categorical variables, and Student's t-test or non-parametric
test for continuous variables, as appropriate. Disease-free
survival (DFS) and OS were calculated from the date of hepatectomy.
Patients were followed until death or the end-point of the study
(April 1, 2016), whichever occurred first. Survival curves were
plotted using the Kaplan-Meier method and compared using the
log-rank test. Variables that were statistically significant in the
univariate analysis (P<0.10) were included in the multivariate
analysis using a Cox proportional hazards model. All statistical
analyses were conducted using Statistical Package for the Social
Sciences for Windows v.21.0 (IBM SPSS, Armonk, NY, USA). P<0.05
was considered to indicate a statistically significant
difference.
Results
A total of 195 patients with resectable CRLMs
underwent pre-operative chemotherapy followed by surgery. Six
patients were lost to follow-up (Fig.
1). Therefore, our analysis was based on the data of 189
patients. The following data from these patients was retrieved for
analysis: Age, sex, primary tumor status, LM status, disease-free
interval, carcinoembryonic antigen levels, and chemotherapy regimen
used.
Patient characteristics and treatment
regimens
The clinical variables and treatment regimens of the
189 patients included in our analysis are summarised in Table I. In summary, our group include 121
males and 68 females, with a mean age was 56 years. In 82 patients
(43.4%), the primary tumor was located in the rectum. Fifty-seven
patients (30.2%) were treated with targeted therapy and 36 patients
(19.0%) received multiple lines of chemotherapy. When categorised
according to the proposed CRS-TRC classification, 68 patients with
a low CRS (group A1) responded to chemotherapy, whereas 26 patients
also with a low CRS (group A2) did not. Variables between patients
in groups A1 and A2 were comparable, with the exception of the
proportion who received adjuvant chemotherapy (P=0.011) and the use
of multiple lines of chemotherapy (P<0.01). Sixty-one patients
with a high CRS (Group B1) responded to chemotherapy, whereas 33
patients with a high CRS (Group B2) did not. Multiple lines of
chemotherapy (P<0.001) were the only variable that was
statistically significant between patients in Group B1 and Group
B2. Chemotherapy regimens were comparable between the two
sub-groups in both the low- and the high-risk groups.
 | Table I.Patients' characteristics and
treatment features. |
Table I.
Patients' characteristics and
treatment features.
|
| Low risk group
(n=95) | High risk group
(n=94) |
|---|
|
|
|
|
|---|
| Variables | Response, Group A1
N=69 | No response, Group A2
N=26 | P-value, A vs.
B1 | Response, Group B1
N=61 | No response, Group B2
N=33 | P-value, B2 vs.
C |
|---|
| Age, years, (Mean ±
SD) | 56.84±9.73 | 56.23±10.16 | 0.788 | 54.69±10.13 | 57.39±10.29 | 0.222 |
| Gender, Male/Female,
n (%) | 45 (65.2)/24
(34.8) | 15 (57.7)/11
(42.3) | 0.634 | 39 (63.9)/22
(36.1) | 22 (66.7)/11
(33.3) | 0.791 |
| DFI<12 months,
Yes/No, n (%) | 50 (72.5)/19
(27.5) | 22 (84.6)/4
(15.4) | 0.287 | 61 (100.0)/0
(0.0) | 32 (97.0)/1
(3.0) | 0.351 |
| CEA at
diagnosis≥200ng/ml, Yes/No, n (%) | 1 (1.4)/68
(98.6) | 3 (10.3)/26
(89.7) | 0.061 | 50 (82.0)/11
(18.0) | 29 (87.9)/4
(12.1) | 0.563 |
| Adjuvant
chemotherapy, Yes/No, n (%) | 57 (82.6)/12
(17.4) | 15 (57.7)/11
(42.3) | 0.011a | 47 (77.0)/14
(23.0) | 26 (78.8)/7
(21.2) | 0.847 |
| Primary tumor |
|
|
|
|
|
|
| Tumor
location, Rectal/Colon, n (%) | 30 (43.5)/39
(56.5) | 14 (53.8)/12
(46.2) | 0.489 | 23 (37.7)/38
(62.3) | 15 (45.5)/18
(54.4) | 0.513 |
| N
stage, N0/N+, n (%) | 43 (62.3)/26
(37.7) | 15 (57.7)/11
(42.3) | 0.814 | 10 (16.4)/51
(83.6) | 4 (12.1)/29
(87.9) | 0.764 |
| Liver
metastasis |
|
|
|
|
|
|
| Tumor
number, Single/Multiple, n (%) | 40 (58.0)/29
(42.0) | 18 (69.2)/8
(30.8) | 0.354 | 8 (13.1)/53
(86.9) | 1 (3.0)/32
(97.0) | 0.153 |
| Tumor
size≥50 mm, Yes/No, n (%) | 6 (8.7)/63
(91.3) | 5 (19.2)/21
(80.8) | 0.166 | 12 (19.7)/49
(80.3) | 12 (36.4)/21
(63.6) | 0.088 |
| Tumor
distribution, Bilobar/Unilateral, n (%) | 29 (42.0)/40
(58.0) | 9 (34.6)/17
(65.4) | 0.640 | 33 (54.1)/28
(45.9) | 22 (66.7)/11
(33.3) | 0.278 |
| NACT details |
|
|
|
|
|
|
| More
than 1 line, Yes/No, n (%) | 9 (13.0)/60
(87.0) | 10 (38.5)/16
(61.5) | 0.006a | 4 (6.6)/57
(93.4) | 13 (39.4)/20
(60.6) | 0.000 |
| NACT
total cycles, ≤2/>2, n (%) | 22 (31.9)/47
(68.1) | 9 (34.6)/17
(65.4) | 0.810 | 18 (29.5)/43
(70.5) | 9 (27.3)/24
(72.7) | 1.000 |
| NACT
regimenb, n (%) |
|
| 0.659 |
|
| 0.366 |
|
Oxa/Iri-based
chemotherapy | 49 (71.0) | 19 (73.1) |
| 31 (50.8) | 20 (60.6) |
|
|
FOLFOXIRI | 1 (1.4) | 0 (0) |
| 1 (1.6) | 1 (3.0) |
|
|
Chemotherapy + targeted
drugs | 12 (17.4) | 6 (23.1) |
| 28 (45.9) | 10 (30.3) |
|
|
HAI | 7 (10.1) | 1 (3.8) |
| 1 (1.6) | 2 (6.1) |
|
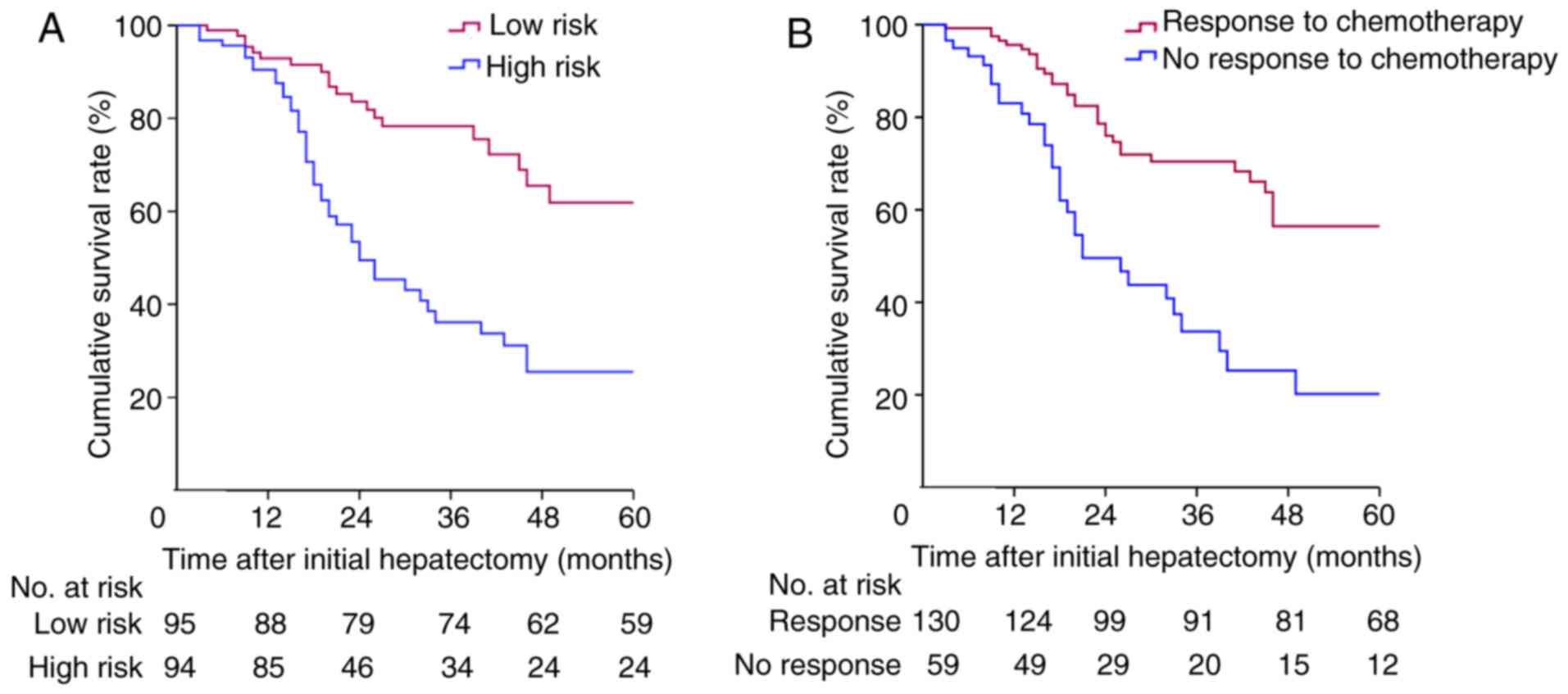
Survival analysis
The median follow-up duration was 46 (95% confidence
interval [CI]: 37.7–54.3) months. The Kaplan-Meier survival curve
is shown in Fig. 2. Sixty-seven
patients (35.4%) were still alive after follow-up. The median OS
time was 46 (95% CI: 37.7–54.3) months. When categorised according
to the CRS system, the 1-, 3-, and 5-year OS rates were 93.0, 78.7,
and 62.3% for patients in the low-risk group (CRS <3) and 90.5,
36.2, and 25.5% for patients in the high-risk group (CRS ≥3),
respectively (P<0.001; Fig. 2A).
When categorised according to TRC, the 1-, 3-, and 5-year OS rates
were 95.6, 70.4, and 56.4% for patients in the TRC group and 91.2,
33.7, and 20.2% for patients in the no TRC group, respectively
(P<0.001; Fig. 2B). Multivariate
analysis identified both CRS and TRC as independent prognostic
factors for OS in patients with CRLMs (Table II).
| Table II.Univariate and multivariate Cox
proportional hazards regression analyses of factors associated with
overall survival. |
Table II.
Univariate and multivariate Cox
proportional hazards regression analyses of factors associated with
overall survival.
|
|
| Multivariate
analysis |
|---|
|
|
|
|
|---|
| Whole group
(N=189) | Univariate
P-value | HR (95% CI) | P-value |
|---|
| Primary tumor
location (rectal/colon) | 0.910 |
|
|
| Primary N stage
(N0/N+) | 0.215 |
|
|
| Tumor number
(single/multiple) | 0.043a | 0.867
(0.419–1.792) | 0.699 |
| Tumor size (<50
mm/≥50 mm) | 0.005a | 1.429
(0.777–2.629) | 0.250 |
| Tumor distribution
(unilateral/bilobar) | 0.185 |
|
|
| DFI (<12
months/≥12 months) | 0.230 |
|
|
| CEA at diagnosis
(<200 ng/ml/≥200 ng/ml) | 0.035a | 1.405
(0.641–3.078) | 0.39 |
| CRS (low risk/high
risk) | 0.000a | 3.000
(1.501–5.995) | 0.002a |
| Tumor
responseb (no/yes) | 0.000a | 2.522
(1.521–4.181) | 0.000a |
| More than 1 line
NACT (no/yes) | 0.208 |
|
|
| No-response to
1st-line chemotherapy group (N=71) |
|
|
|
| CRS (low risk/high
risk) | 0.006a | 2.259
(1.257–4.747) | 0.032a |
| Tumor response in
2nd line (no/yes) | 0.012a | 1.837
(1.184–3.265) | 0.045a |
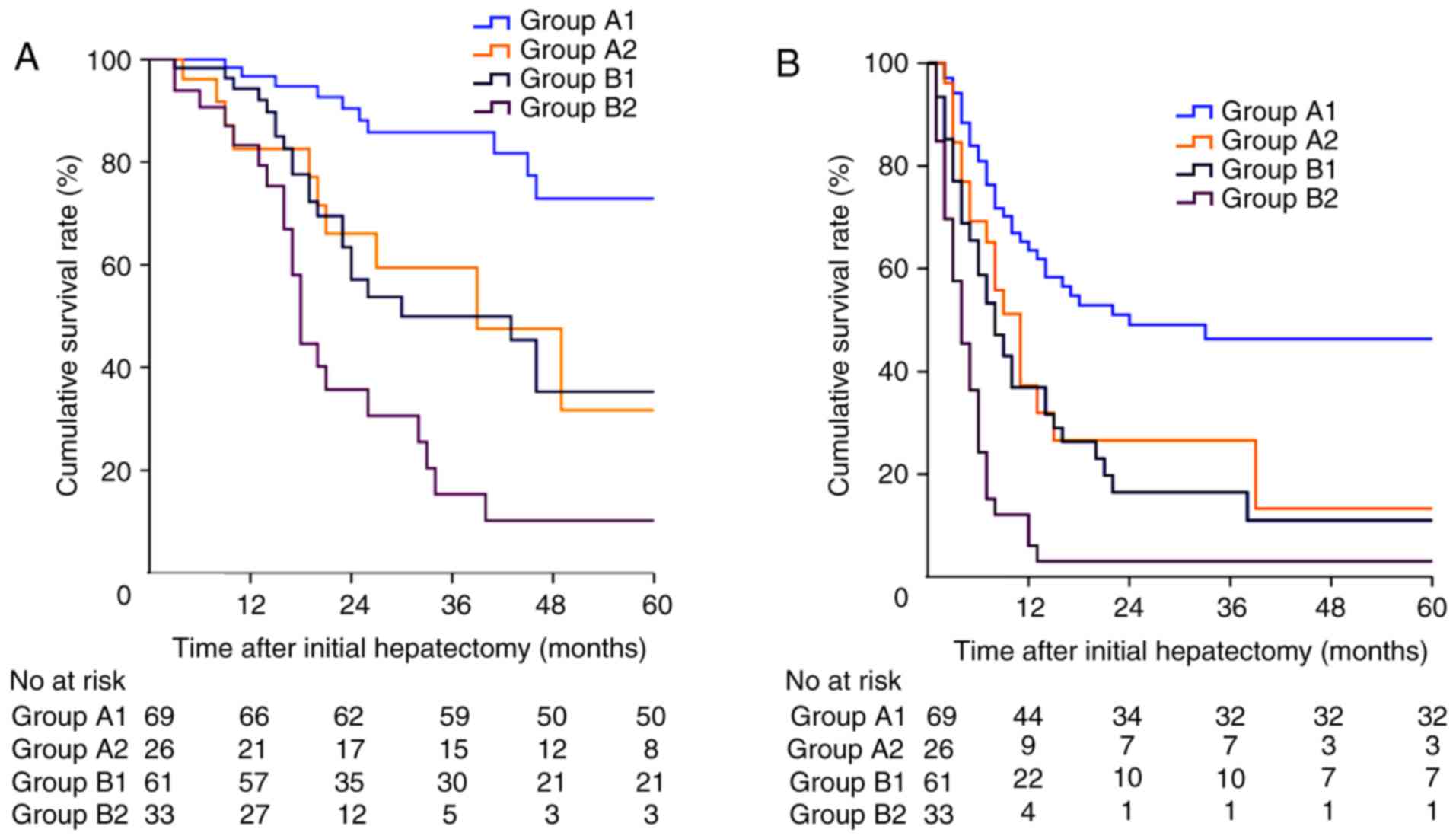
We subsequently categorised patients into four
sub-groups according to the proposed CRS-TRC classification
outlined in Fig. 1. Patients in Group
A1-2 had a low CRS with/without a TRC and patients in Group B1-2
had a high CRS with/without a TRC. The Kaplan-Meier survival curve
of the patients is shown in Fig. 3.
The 1-, 3-, and 5-year OS rates were 96.7, 85.8, and 72.9%,
respectively, for patients in Group A1; 82.6, 59.5, and 31.7%,
respectively, for patients in Group A2, 94.3, 49.4, and 35.3%,
respectively, for patients in Group B1, and 83.3, 15.3, and 10.2%,
respectively, for patients in Group B2 (P<0.001; Fig. 3A). The median DFS was 24.0 (95% CI:
20.8–27.9) months, 11.0 (95% CI: 7.8–14.2) months, 8.0 (95% CI:
5.5–10.5) months, and 4.0 (95% CI: 2.4–5.6) months for patients in
Group A1-2 and Group B1-2, respectively (P<0.001; Fig. 3B).
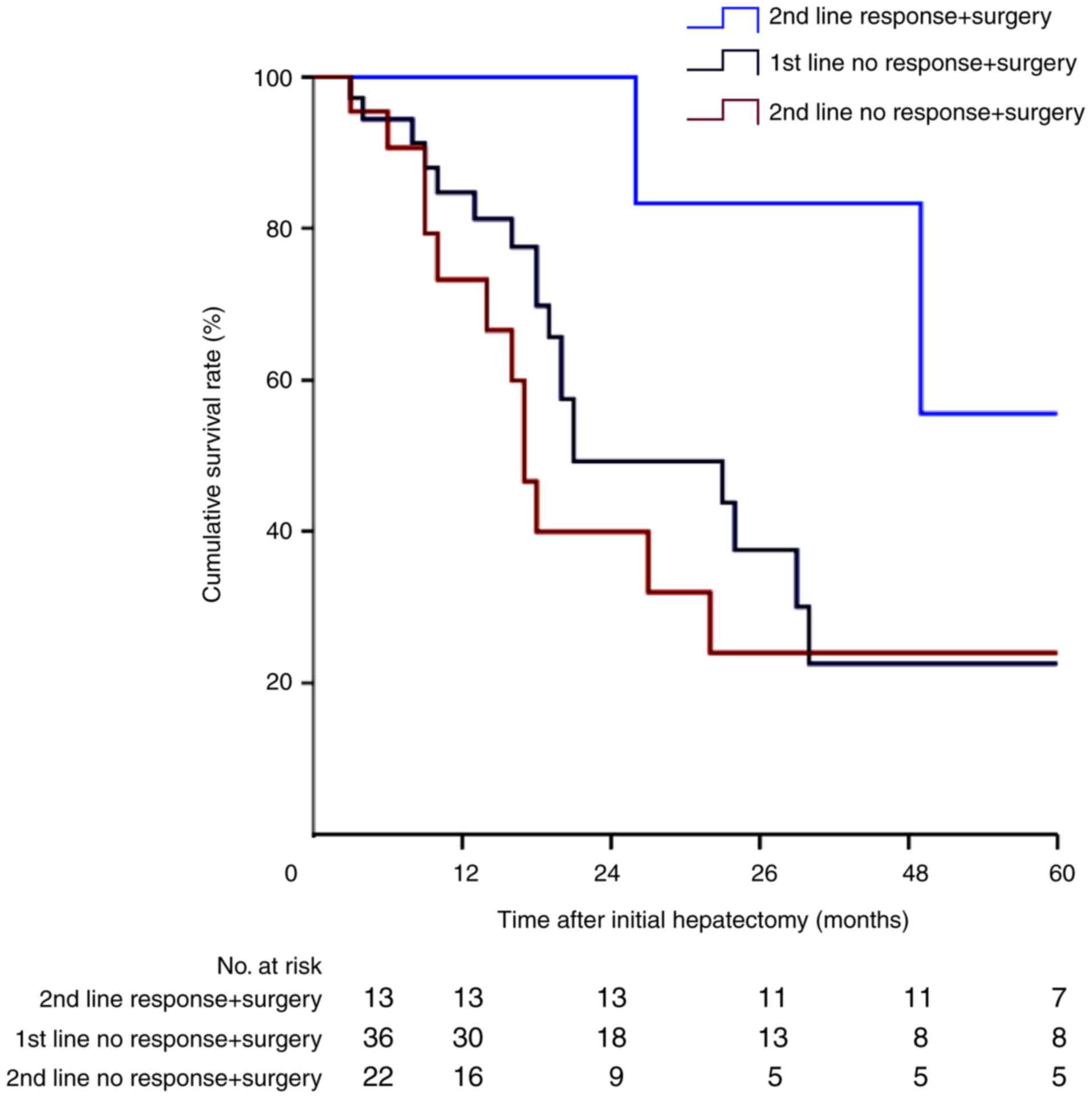
Survival analysis of patients who
progressed on first-line chemotherapy
Among the 71 patients underwent tumor progression
during first-line chemotherapy, 36 were treated surgically
immediately after first-line progression. The remaining 35 patients
received second-line chemotherapy, with only 13 patients (37.1%)
showing a good tumor response, a proportion that is considerably
lower than the 130 patients (68.8%) who had a tumor response to
first-line chemotherapy. The Kaplan-Meier survival curve of these
patients is shown in Fig. 4. Patients
who responded well to second-line chemotherapy had a significantly
better prognosis than patients who progressed on either first- or
second-line chemotherapy (P<0.05). Multivariate analysis
identified TRC to second-line chemotherapy as an independent
prognostic factor for OS in patients who did not respond to
first-line chemotherapy (Table
II).
To further investigate the effects of second-line
chemotherapy on TRC, the treatment details of these patients were
analysed (Table III). Of the 13
patients with a tumor response to second-line chemotherapy followed
by surgery, six patients (46.2%) received targeted therapy, four
patients (30.8%) underwent HAI therapy, and only three patients
(23.0%) were still treated with a doublet regimen. Conversely, of
the remaining 22 patients who progressed on second-line
chemotherapy, 11 patients (50.0%) were still treated with a doublet
regimen, a ratio that is considerably higher than for the TRC
group.
| Table III.Treatment details of patients who
received second line chemotherapy. |
Table III.
Treatment details of patients who
received second line chemotherapy.
|
| Response in 2nd
line chemotherapy followed by surgery (Group 1, N=13) | No response in 2nd
line chemotherapy followed by surgery (Group 2, N=22) |
|---|
|
|
|
|
|---|
| Group | Patients | CRS | Regime | Cycle | Patients | CRS | Regime | Cycle |
|---|
| Targeted drugs |
|
|
|
|
|
|
|
| Group
1, n=6 (46.2%); | P1 | High | FOLFIRI+BEV | 2 | P1 | Low | FOLFIRI+BEV | 2 |
| Group
2, n=9 (40.9%) | P2 | Low | FOLFIRI+BEV | 5 | P2 | Low | FOLFIRI+BEV | 2 |
|
| P3 | Low | FOLFIRI+CET | 3 | P3 | Low | FOLFIRI+BEV | 3 |
|
| P4 | High | FOLFOX+CET | 2 | P4 | High | XELIRI+BEV | 4 |
|
| P5 | High | XELOX+CET | 2 | P5 | High | XELOX+BEV | 3 |
|
| P6 | Low | FOLFOX+CET | 3 | P6 | Low | FOLFIRI+CET | 3 |
|
|
|
|
|
| P7 | High | FOLFIRI+CET | 4 |
|
|
|
|
|
| P8 | High | FOLFIRI+CET | 4 |
|
|
|
|
|
| P9 | High | FOLFOX+CET | 2 |
| HAI |
|
|
|
|
|
|
|
|
| Group
1, n=4 (30.8%); | P7 | Low | Oxa+5-Fu | 2 | P10 | Low | Oxa+5-Fu | 4 |
| Group
2, n=2 (9.1%) | P8 | Low | Oxa+5-Fu | 2 | P11 | High | Oxa+5-Fu | 2 |
|
| P9 | High | Oxa+5-Fu | 2 |
|
|
|
|
|
| P10 | Low | Oxa+5-Fu | 3 |
|
|
|
|
| Doublet
regimes |
|
|
|
|
|
|
|
|
| Group
1, n=3 (23.0%); | P11 | High | FOLFIRI | 2 | P12 | Low | FOLFIRI | 2 |
| Group
2, n=11 (50%) | P12 | Low | FOLFIRI | 3 | P13 | Low | FOLFIRI | 3 |
|
| P13 | High | XELOX | 4 | P14 | Low | FOLFIRI | 3 |
|
|
|
|
|
| P15 | High | FOLFIRI | 6 |
|
|
|
|
|
| P16 | High | XELIRI | 2 |
|
|
|
|
|
| P17 | High | XELOX | 2 |
|
|
|
|
|
| P18 | High | XELOX | 2 |
|
|
|
|
|
| P19 | Low | XELOX | 2 |
|
|
|
|
|
| P20 | High | XELOX | 2 |
|
|
|
|
|
| P21 | Low | FOLFOX | 2 |
|
|
|
|
|
| P22 | High | FOLFOX | 2 |
Discussion
With respect to tumor oncological status, the CRS
system of Fong has been validated by numerous studies for its
efficiency in predicting survival (6,10–12). Meanwhile, with recent advances in the
development of more effective chemotherapeutic and targeted agents,
some authors questioned the impact of Fong's CRS system on
survival, arguing that the real value of the tumor response in
predicting survival may be underestimated in the modern era of
chemotherapy (13,14). Allen et al (19) initially found that patients with
synchronous CRLMs who responded well to chemotherapy had a
prolonged survival compared to patients who underwent surgery
alone. Similarly, Adam et al (27) reported that survival times were
significantly shorter in patients with multiple metastases (≥4
tumors) who experienced tumor progression during NACT after
hepatectomy. However, whether surgery should be performed in
patients who have experienced progression during NACT has long been
debated (28,29). Neumann et al (28) reported that there was no association
between TRC and long-term survival in patients with synchronous
CRLMs, indicating that liver resection may not be contraindicated
in these patients. It should be noted that patients' clinical risk
factors differed substantially between the above-mentioned studies.
Moreover, the choice of chemotherapy regimen can play a pivotal
role in tumor response, with a high proportion of patients in the
above-mentioned studies treated with 5-fluorouracil
monotherapy.
To investigate the outcome of patients who underwent
hepatectomy under different clinical and chemotherapy response
conditions, we proposed a CRS-TRC classification in which patients
were stratified into four sub-groups according to both clinical
risk factors and tumor response factors. Our findings demonstrate
that patients with a low CRS and a TRC (Group A1) derived the most
benefits of hepatectomy, with a 5-year OS rate of 72.9%.
Conversely, patients with a high CRS and no TRC (Group B2)
exhibited the poorest prognosis, with only 10.2% of patients alive
after 5 years. The long-term survival of the remaining patients
with only one risk factor in either the high CRS (A2) or no TRC
(B1) groups was poorer than the survival among patients in Group
A1, but was significantly longer than survival among patients in
Group B2. These findings suggest that patients with CRLMs who have
a low CRS but underwent tumor progression during NACT should not be
precluded from surgical resection since the 5-year OS rate can be
as high as 31.7% after hepatectomy, although no TRC is a poor
prognostic factor. On the other hand, the prognosis of patients in
Group B2 with both a high CRS and progressed during NACT was very
poor, these patients might not be suitable for surgery, although
they were initially deemed to have resectable tumors. Similarly,
Vigano et al (20) found that
hepatectomy should not be considered as an absolute
contraindication to liver resection since a proportion of low-risk
patients with disease progression would benefit from surgery. Our
findings support this conclusion. In fact, in a multidisciplinary
international consensus of the Expert Group on OncoSurgery
management of Liver Metastases (30),
oncological criteria for contraindication to hepatic resection in
patients with CRLMs included a greater number of tumor and tumor
progression during chemotherapy. These criteria are consistent with
the CRS-TRC classification, which includes ‘inner’ clinical risk
factors, reflected by Fong's CRS system, and ‘external’ oncological
factors, reflected by the TRC. Therefore, we can better understand
that both clinical risk factors and a TRC play significant roles in
patient selection for surgical resection. It may be unwise to
select patients or predict survival considering only one of these
factors since both are important in predicting oncological
behaviour.
In the present study, the survival time of patients
who underwent resection after effective second-line chemotherapy
was considerably longer than that of patients who underwent
resection directly or patients who still underwent resection even
though second-line chemotherapy was ineffective. These findings
emphasize the importance of achieving ‘good’ tumor control to
maximise the benefit of surgical resection, especially in high-risk
patients. Moreover, among patients who received second-line
chemotherapy, the proportion of HAI therapy or targeted drugs used
in the effective second-line chemotherapy group was considerably
higher than among patients with a poor tumor response to
second-line chemotherapy group. A randomised controlled trial
conducted by Ye et al (31)
has highlighted the efficiency of cetuximab in increasing the
objective response rate. Additionally, HAI therapy has also been
shown to be effective in increasing the response rate in patients
who progressed on first-line systematic chemotherapy (32). Therefore, we hypothesised that the
increasing use of HAI therapy and targeted drugs will assist more
patients in achieving a better TRC, therefore reducing disease
progression and prolonging survival. Unfortunately, although the
most powerful drugs were used in our second-line chemotherapy
regimens, the response rate was poor overall, with only 13 patients
(37.1%) achieving a TRC. This rate of TRC was considerably lower
than the 130 patients (68.8%) who achieved a TRC with first-line
chemotherapy.
To the best of our knowledge, this is the first
study to have considered both clinical and chemotherapy factors in
predicting outcomes for patients with CRLMs after hepatic
resection. However, there are still several limitations that need
to be acknowledged in the interpretation of our results for
clinical practice. Firstly, this is a retrospective analysis with a
limited number of patients, although no fewer than in the majority
of previous studies. Therefore, the clinical effectiveness of the
proposed CRS-TRC classification will need to be verified further in
prospective studies with larger cohorts. Secondly, recent studies
have identified other prognostic factors to predict clinical
outcomes of treatment for patients with CRLMs, including the
detection of RAS/BRAF mutations (33–35).
However, since we only began routinely detecting RAS/BRAF
mutations in 2012, this factor was not considered in our study. In
the future, a far more complete system may be developed, combining
tumor clinical factors, gene status, and chemotherapy and
pathological responses, just like the CRS system presented by Fong
(9).
In conclusion, the proposed CRS-TRC classification
may be beneficial in the modern chemotherapy era for selecting
suitable candidates for potentially curative treatment approaches.
Patients with a low CRS benefit from surgical resection even if
they develop tumor progression during chemotherapy. Conversely, it
may be less beneficial to perform surgery in patients with a high
CRS who develop tumor progression during first-line NACT. The best
approach for these patients would be to select a more powerful
second-line chemotherapy regime, such as targeted drugs or HAI, to
maximise tumor control.
In this 10-year retrospective cohort study, we
proposed a new classification considering both Clinical Risk Scores
(CRS) and tumor response to pre-operative chemotherapy (TRC), which
will be assistant in predicting survival and selecting suitable
patients with resectable colorectal liver metastases for curative
therapy.
Acknowledgements
The present study was supported by a grant (no.
81371868) from the National Nature Science Foundation of China and
Beijing Municipal Administration of Hospitals Incubating Program
(code: PX2016002).
References
|
1
|
Smith JJ and D'Angelica MI: Surgical
management of hepatic metastases of colorectal cancer. Hematol
Oncol Clin North Am. 29:61–84. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Leporrier J, Maurel J, Chiche L, Bara S,
Segol P and Launoy G: A population-based study of the incidence,
management and prognosis of hepatic metastases from colorectal
cancer. Br J Surg. 93:465–474. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rees M, Tekkis PP, Welsh FK, O'Rourke T
and John TG: Evaluation of long-term survival after hepatic
resection for metastatic colorectal cancer: A multifactorial model
of 929 patients. Ann Surg. 247:125–135. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Aloia TA, Vauthey JN, Loyer EM, Ribero D,
Pawlik TM, Wei SH, Curley SA, Zorzi D and Abdalla EK: Solitary
colorectal liver metastasis: Resection determines outcome. Arch
Surg. 141:460–467. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Simmonds PC, Primrose JN, Colquitt JL,
Garden OJ, Poston GJ and Rees M: Surgical resection of hepatic
metastases from colorectal cancer: A systematic review of published
studies. Br J Cancer. 94:982–999. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nakai T, Ishikawa H, Tokoro T and Okuno K:
The clinical risk score predicts the effectiveness of adjuvant
chemotherapy for colorectal liver metastasis. World J Surg.
39:1527–1536. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kanas GP, Taylor A, Primrose JN, Langeberg
WJ, Kelsh MA, Mowat FS, Alexander DD, Choti MA and Poston G:
Survival after liver resection in metastatic colorectal cancer:
Review and meta-analysis of prognostic factors. Clin Epidemiol.
4:283–301. 2012.PubMed/NCBI
|
|
8
|
Petrelli NJ: Perioperative or adjuvant
therapy for resectable colorectal hepatic metastases. J Clin Oncol.
26:4862–4863. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fong Y, Fortner J, Sun RL, Brennan MF and
Blumgart LH: Clinical score for predicting recurrence after hepatic
resection for metastatic colorectal cancer: Analysis of 1001
consecutive cases. Ann Surg. 230:309–321. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rahbari NN, Reissfelder C,
Schulze-Bergkamen H, Jäger D, Büchler MW, Weitz J and Koch M:
Adjuvant therapy after resection of colorectal liver metastases:
The predictive value of the MSKCC clinical risk score in the era of
modern chemotherapy. BMC Cancer. 14:1742014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mann CD, Metcalfe MS, Leopardi LN and
Maddern GJ: The clinical risk score: Emerging as a reliable
preoperative prognostic index in hepatectomy for colorectal
metastases. Arch Surg. 139:1168–1172. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ayez N, van der Stok EP, Grunhagen DJ,
Rothbarth J, van Meerten E, Eggermont AM and Verhoef C: The use of
neo-adjuvant chemotherapy in patients with resectable colorectal
liver metastases: Clinical risk score as possible discriminator.
Eur J Surg Oncol. 41:859–867. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Reddy SK, Kattan MW, Yu C, Ceppa EP, de la
Fuente SG, Fong Y, Clary BM and White RR: Evaluation of
peri-operative chemotherapy using a prognostic nomogram for
survival after resection of colorectal liver metastases. HPB
(Oxford). 11:592–599. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kumar R, Dennison AR, Robertson V, Jones
MJ, Neal CP and Garcea G: Clinical risk scores in the current era
of neoadjuvant chemotherapy for colorectal liver metastases. ANZ J
Surg. Sep 12–2016.(Epub ahead of print). View Article : Google Scholar
|
|
15
|
Nordlinger B, Sorbye H, Glimelius B,
Poston GJ, Schlag PM, Rougier P, Bechstein WO, Primrose JN, Walpole
ET, Finch-Jones M, et al: Perioperative FOLFOX4 chemotherapy and
surgery versus surgery alone for resectable liver metastases from
colorectal cancer (EORTC 40983): Long-term results of a randomised,
controlled, phase 3 trial. Lancet Oncol. 14:1208–1215. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Baize N, Gerard B, Bleiberg H, Caroli-Bosc
F, Berthier F, Legendre H, Pector JC and Hendlisz A: Long-term
survival of patients downstaged by oxaliplatin and 5-fluorouracil
combination followed by rescue surgery for unresectable colorectal
liver metastases. Gastroenterol Clin Biol. 30:1349–1353. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Adam R, Delvart V, Pascal G, Valeanu A,
Castaing D, Azoulay D, Giacchetti S, Paule B, Kunstlinger F,
Ghémard O, et al: Rescue surgery for unresectable colorectal liver
metastases downstaged by chemotherapy: A model to predict long-term
survival. Ann Surg. 240:644–658. 2004.PubMed/NCBI
|
|
18
|
Vessie EL, Liu DM, Forster B, Kos S,
Baxter K, Gagnon J and Klass D: A practical guide to magnetic
resonance vascular imaging: Techniques and applications. Ann Vasc
Surg. 28:1052–1061. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Allen PJ, Kemeny N, Jarnagin W, DeMatteo
R, Blumgart L and Fong Y: Importance of response to neoadjuvant
chemotherapy in patients undergoing resection of synchronous
colorectal liver metastases. J Gastrointest Surg. 7:109–117. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vigano L, Capussotti L, Barroso E, Nuzzo
G, Laurent C, Ijzermans JN, Gigot JF, Figueras J, Gruenberger T,
Mirza DF, et al: Progression while receiving preoperative
chemotherapy should not be an absolute contraindication to liver
resection for colorectal metastases. Ann Surg Oncol. 19:2786–2796.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumors:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zendel A, Lahat E, Dreznik Y, Zakai BB,
Eshkenazy R and Ariche A: ‘Vanishing liver metastases’-A real
challenge for liver surgeons. Hepatobiliary Surg Nutr. 3:295–302.
2014.PubMed/NCBI
|
|
23
|
Jones RP, Stattner S, Sutton P, Dunne DF,
McWhirter D, Fenwick SW, Malik HZ and Poston GJ: Controversies in
the oncosurgical management of liver limited stage IV colorectal
cancer. Surg Oncol. 23:53–60. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Clavien PA, Petrowsky H, DeOliveira ML and
Graf R: Strategies for safer liver surgery and partial liver
transplantation. N Engl J Med. 356:1545–1559. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ruers T, Punt C, Van Coevorden F, Pierie
JP, Borel-Rinkes I, Ledermann JA, Poston G, Bechstein W, Lentz MA,
Mauer M, et al: Radiofrequency ablation combined with systemic
treatment versus systemic treatment alone in patients with
non-resectable colorectal liver metastases: A randomized EORTC
Intergroup phase II study (EORTC 40004). Ann Oncol. 23:2619–2626.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tanis E, Nordlinger B, Mauer M, Sorbye H,
van Coevorden F, Gruenberger T, Schlag PM, Punt CJ, Ledermann J and
Ruers TJ: Local recurrence rates after radiofrequency ablation or
resection of colorectal liver metastases. Analysis of the European
Organisation for Research and Treatment of Cancer #40004 and
#40983. Eur J Cancer. 50:912–919. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Adam R, Pascal G, Castaing D, Azoulay D,
Delvart V, Paule B, Levi F and Bismuth H: Tumor progression while
on chemotherapy: A contraindication to liver resection for multiple
colorectal metastases? Ann Surg. 240:1052–1064. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Neumann UP, Thelen A, Röcken C, Seehofer
D, Bahra M, Riess H, Jonas S, Schmeding M, Pratschke J, Bova R and
Neuhaus P: Nonresponse to pre-operative chemotherapy does not
preclude long-term survival after liver resection in patients with
colorectal liver metastases. Surgery. 146:52–59. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gallagher DJ, Zheng J, Capanu M, Haviland
D, Paty P, Dematteo RP, D'Angelica M, Fong Y, Jarnagin WR, Allen PJ
and Kemeny N: Response to neoadjuvant chemotherapy does not predict
overall survival for patients with synchronous colorectal hepatic
metastases. Ann Surg Oncol. 16:1844–1851. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Adam R, De Gramont A, Figueras J, Guthrie
A, Kokudo N, Kunstlinger F, Loyer E, Poston G, Rougier P,
Rubbia-Brandt L, et al: The oncosurgery approach to managing liver
metastases from colorectal cancer: A multidisciplinary
international consensus. Oncologist. 17:1225–1239. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ye LC, Liu TS, Ren L, Wei Y, Zhu DX, Zai
SY, Ye QH, Yu Y, Xu B, Qin XY and Xu J: Randomized controlled trial
of cetuximab plus chemotherapy for patients with KRAS wild-type
unresectable colorectal liver-limited metastases. J Clin Oncol.
31:1931–1938. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Levi FA, Boige V, Hebbar M, Smith D,
Lepère C, Focan C, Karaboué A, Guimbaud R, Carvalho C, Tumolo S, et
al: Conversion to resection of liver metastases from colorectal
cancer with hepatic artery infusion of combined chemotherapy and
systemic cetuximab in multicenter trial OPTILIV. Ann Oncol.
27:267–274. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
De Roock W, Piessevaux H, De Schutter J,
Janssens M, De Hertogh G, Personeni N, Biesmans B, Van Laethem JL,
Peeters M, Humblet Y, et al: KRAS wild-type state predicts survival
and is associated to early radiological response in metastatic
colorectal cancer treated with cetuximab. Ann Oncol. 19:508–515.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Roth AD, Tejpar S, Delorenzi M, Yan P,
Fiocca R, Klingbiel D, Dietrich D, Biesmans B, Bodoky G, Barone C,
et al: Prognostic role of KRAS and BRAF in stage II and III
resected colon cancer: Results of the translational study on the
PETACC-3, EORTC 40993, SAKK 60–00 trial. J Clin Oncol. 28:466–474.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Van Cutsem E, Köhne CH, Láng I, Folprecht
G, Nowacki MP, Cascinu S, Shchepotin I, Maurel J, Cunningham D,
Tejpar S, et al: Cetuximab plus irinotecan, fluorouracil, and
leucovorin as first-line treatment for metastatic colorectal
cancer: Updated analysis of overall survival according to tumor
KRAS and BRAF mutation status. J Clin Oncol. 29:2011–2019. 2011.
View Article : Google Scholar : PubMed/NCBI
|