Introduction
Lung cancer is one of the most frequently diagnosed
types of human malignancy and the leading cause of cancer mortality
globally, particularly in developed countries (1,2). In China,
lung cancer morbidity and mortality have increased in recent
decades (1). Pathologically, lung
cancer is classified as non-small cell lung cancer (NSCLC) and
SCLC, and NSCLC accounts for 75–80% of all lung cancer cases
(3). Surgery remains the most
curative treatment option for patients with NSCLC and prolongs
survival rate of such patients; however, a great number of patients
are diagnosed at the late stages of the disease, leading to surgery
not being an option (4). Despite
advances in surgery, chemotherapy, radiotherapy and targeting
therapy, the prognosis of patients with advanced NSCLC remains poor
(5) which leads to substantial
financial and psychological burdens for patients and their families
associated with NSCLC diagnosis and therapy (6–9). In the
early stages, NSCLC rarely exhibits noticeable symptoms (8,9); thus, the
development and identification of biomarkers for early detection
and prediction of prognosis may aid medical oncologists to detect
the disease early or to provide more aggressive treatment to
effectively control the disease.
The dysfunctional regulation of microRNAs (miRNAs or
miRs) has been associated with human disease, including various
types of cancer (10,11). miRNAs are a class of
naturally-occurring small non-coding RNAs of 18–22 nucleotides in
length, which are able to post-transcriptionally inhibit the
expression of their targeting messenger RNAs (mRNAs). A single
miRNA may regulate hundreds of targeting mRNAs by specifically
binding to the 3′-untranslated region of mRNA, while one type of
mRNA may also be regulated by different miRNAs (12). miRNAs are usually localized in the
exosome of cells (13).
Cancer-secreted exosomes/miRNAs can be detected in tissue samples
or other samples such as blood (13–15). Thus,
miRNAs may be ideal markers to foster predictive or early
diagnostic tumor markers or for proficient therapeutic
decisions.
miR-105 has been reported to be altered in human
cancer and lost miR-105 expression was associated with poor patient
survival (16). However, little is
known about the association between miR-105-1 expression and the
survival of patients with NSCLC. The present study performed in
silico analysis of differentially expressed miRNAs in different
peripheral blood samples from patients with various diseases vs.
controls using Gene Expression Omnibus (GEO) database data, and
assessed miR-105-1 expression in 32 normal lung and 142 non-small
cell lung cancer (NSCLC) tissue samples using reverse
transcription-quantitative polymerase chain reaction (RT-qPCR). The
aim of the present study was to evaluate and identify the utility
of miR-105-1 as a prognostic marker for patients with NSCLC.
Materials and methods
Acquisition of GEO database data
The present study downloaded the raw data on
GSE61741 and GSE24709 from the GEO database (17,18). GEO
is the repository database to store all high-throughput gene
expression data of hybridization arrays, chips or microarrays. The
GSE61741 dataset includes 1,049 miRNA expression data in normal
controls, chronic obstructive pulmonary disease (COPD), lung cancer
and other types of cancer, while the GSE24709 dataset includes 47
miRNA expression data from 19 normal control and 28 lung cancer
patients. The present study utilized these two sets of
differentially expressed miRNA data to identify differentially
expressed miRNAs for NSCLC. Hierarchical clustering was performed
using the multiple experiment viewer (MeV) 4.7.1 software programs
(http://www.tm4.org/).
Patients and tissue samples
The present study collected tumor and matched
non-tumorous tissue specimens from patients with NSCLC who
underwent surgery in Shanghai Tenth People's Hospital, Tongji
University School of Medicine (Shanghai, China) between January
2008 and December 2014. Two experienced pathologists confirmed
NSCLC diagnosis independently according to the World Health
Organization criteria (19) and tumor
staging according to the Seventh Edition of the American Joint
Committee on Cancer tumor-node-metastasis (TNM) staging system for
NSCLC (20). Specimens included 32
paired cancer and adjacent non-cancerous tissues, and 110 cases of
NSCLC tumor tissues. The present study was approved by the Ethics
Committee of Shanghai Tenth People's Hospital, Tongji University
School of Medicine (approval no. SHSY-IEC-PAP-15-18). Patients
and/or their legal surrogates provided written informed consent to
the surgical procedures and participation in the present study by
donating the tissue specimens.
The demographic and clinicopathological
characteristics of the patients were documented, including the
clinical information, sex, age, smoking history, tumor
characteristics, lymph-node metastasis, tumor differentiation,
histological subtype, TNM stage, invasion of lung membrane,
vascular invasion diameter, overall survival (OS) and disease-free
survival (DFS). The last follow-up was conducted on July 30, 2015
through direct correspondence or phone interview. Mortality or
tumor relapse was verified by patients or their relatives, or from
medical or social security records. OS was computed in months from
the date of diagnosis to the time of mortality, regardless of the
cause. DFS was defined as the period from the initial date of
diagnosis to the time of tumor progression by computed tomography
scan, or to the time of mortality due to the disease.
RNA isolation and RT-qPCR
Total RNA from NSCLC and normal tissues was isolated
using TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA) according to the protocol of the manufacturer.
RNA concentration was measured using NanoDrop ND-1000 (Thermo
Fisher Scientific, Inc., Wilmington, DE, USA) and the quality was
assessed using electrophoresis in 1.5% denaturing agarose gels and
viewed on a Kodak Gel Logic 2200 imaging system (Kodak, Rochester,
NY, USA). TaqMan probe-based qPCR was carried out using a
commercial kit (Applied Biosystems; Thermo Fisher Scientific, Inc.)
according to the protocol of the manufacturer (21). RT reactions were performed using AMV
Reverse Transcriptase (Takara Biotechnology Co., Ltd., Dalian,
China) and qPCR was performed using a standard TaqMan PCR kit
protocol on the Applied Biosystems 7900HT Sequence Detection system
(Thermo Fisher Scientific, Inc.). A specific primer (sequence,
5′-AGGACUCAAAUGCUCAG-3′) and TaqMan probe (sequence,
5′-UCAAAUGCUCAGACUCCUGU-3′) were used to quantify the expression of
hsa-miR-105-1 (PN: 000441). Thermocycling conditions were as
follows: Initial denaturation at 94°C for 10 min, followed by 35
cycles of 94°C for 30 sec, 60°C for 30 sec and 72°C for 30 sec,
with a final extension at 72°C for 10 min. Each reaction was
independently tested in duplicate a minimum of three times. U6 was
used as the internal control and miR-105-1 levels were quantified
using the 2−ΔΔCq method (22). miR-105-1 level was summarized and
recorded as high vs. low levels of expression based on the median
value.
Statistical analysis
Levels of miR-105-1 were summarized and recorded as
the mean ± standard deviation. The independent t-test was used to
calculate the difference between two groups of data. The
χ2 test was used to evaluate the difference between the
groups. Kaplan-Meier curves and log-rank tests were used to analyze
the OS or DFS of patients with NSCLC. Multivariate Cox proportional
hazards regression models were performed to explore the character
of multiple characteristics in the prognosis of patients with
NSCLC. All statistical analyses were performed using the SPSS 20.0
software program (IBM SPSS, Armonk, NY, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
Reduced miR-105-1 expression using
miRNA microarray profiling data
The present study first performed an in
silico analysis using GEO database data. GSE61741 included
peripheral blood profiles of patients with various diseases and
controls. There were 93 differentially expressed miRNAs between
normal controls and lung cancer, with the cut-off point of ≥2-fold
changes for upregulated miRNAs and ≤0.5-fold changes for
downregulated miRNAs (Fig. 1A). This
included certain upregulated miRNAs such as miR-130b-3p, miR-135b
and miR-92 (23,24), and certain downregulated miRNAs such
as miR-144-3p, miR-30 and miR-486 (25–27), which
were reported previously in lung cancer.
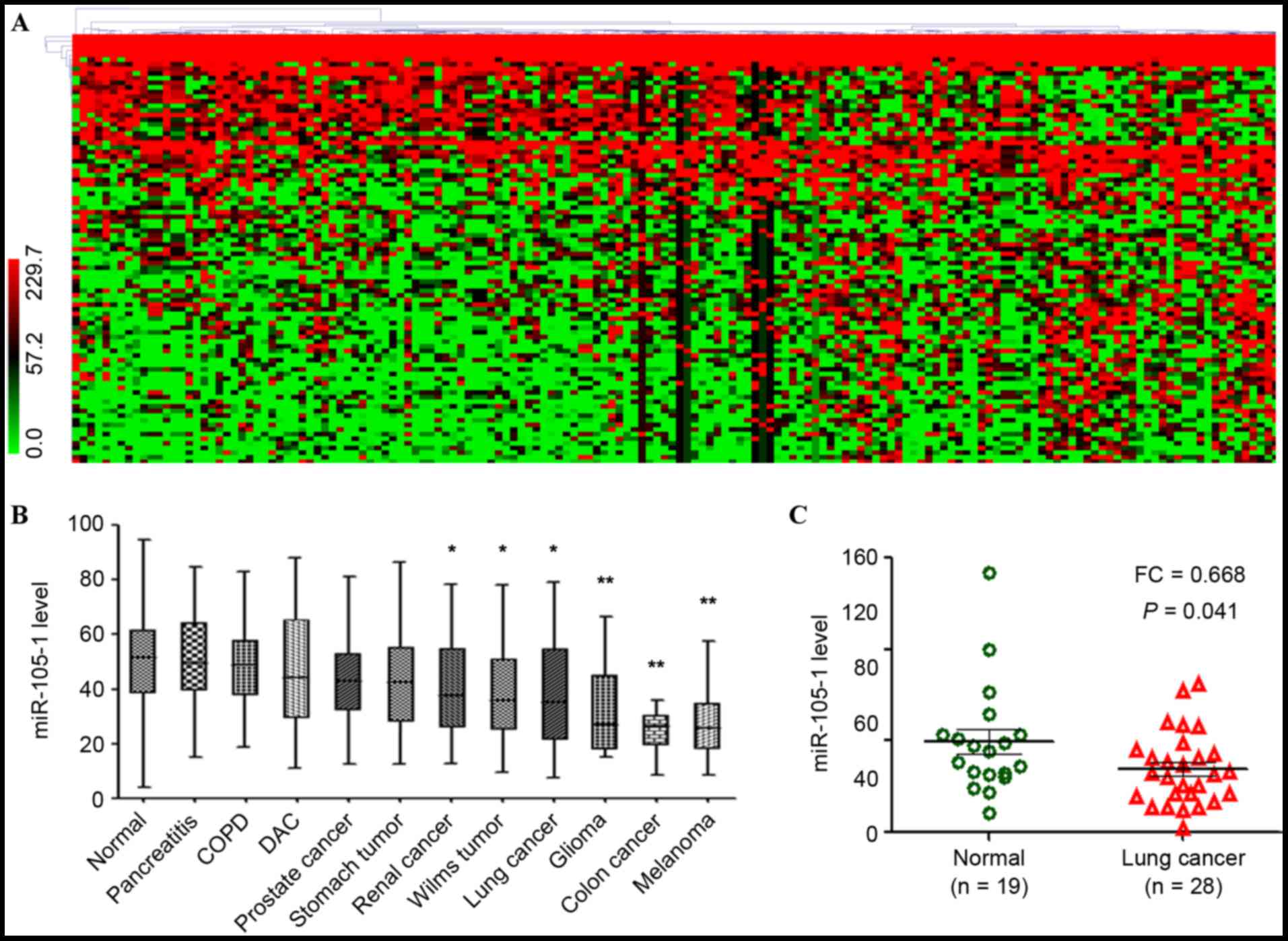 | Figure 1.Reduced expression of miR-105-1 in
lung cancer using the GEO datasets. (A) Data on GEO GSE61741
dataset, including 1,049 miR expression data in normal controls,
COPD, lung cancer and other types of cancer, were clustered using
MeV 4.7.1 software. The color ratio bar (range, 0–299.7) indicates
intensity of gene upregulation (red), downregulation (green) and no
change (black). (B) Relative expression levels of miR-105-1 in
different types of cancer vs. normal controls (GSE61741). (C)
Relative expression levels of miR-105-1 in non-small cell lung
cancer, adjacent normal tissues and non-cancerous lung diseases
from GEO GSE24709 datasets. *P<0.05 and **P<0.01 vs. normal.
GEO, Gene Expression Omnibus; COPD, chronic obstructive pulmonary
disease; DAC, ductal adenocarcinoma; FC, fold change; miR,
microRNA. |
The usefulness of other newfound miRNAs as
prognostic markers for NSCLC patients was then analyzed, including
miR-105-1 [fold change (FC)=0.43, P=0.044; Fig. 1A]. The different expression levels of
the dysregulated miRNAs in a control, lung cancer, COPD and
pancreatitis with different types of tumor were investigated, and
the results revealed that miR-105-1 was significantly downregulated
in the majority of tumor types, particularly in lung cancer
(P<0.05; Fig. 1B).
The present study then validated the aforementioned
findings in another set of NSCLC vs. non-cancerous tissue samples.
GSE24709 data also demonstrated that the miR-105-1 level was
significantly reduced in lung cancer compared with that in normal
controls (FC=0.668, P=0.041; Fig.
1C).
Validation of the reduced miR-105-1
level in NSCLC tissue samples
The present study next performed RT-qPCR to quantify
the miR-105-1 level in 142 (90 I–II and 52 III–IV grades) NSCLC
specimens and 32 non-cancerous tissues from patients with NSCLC.
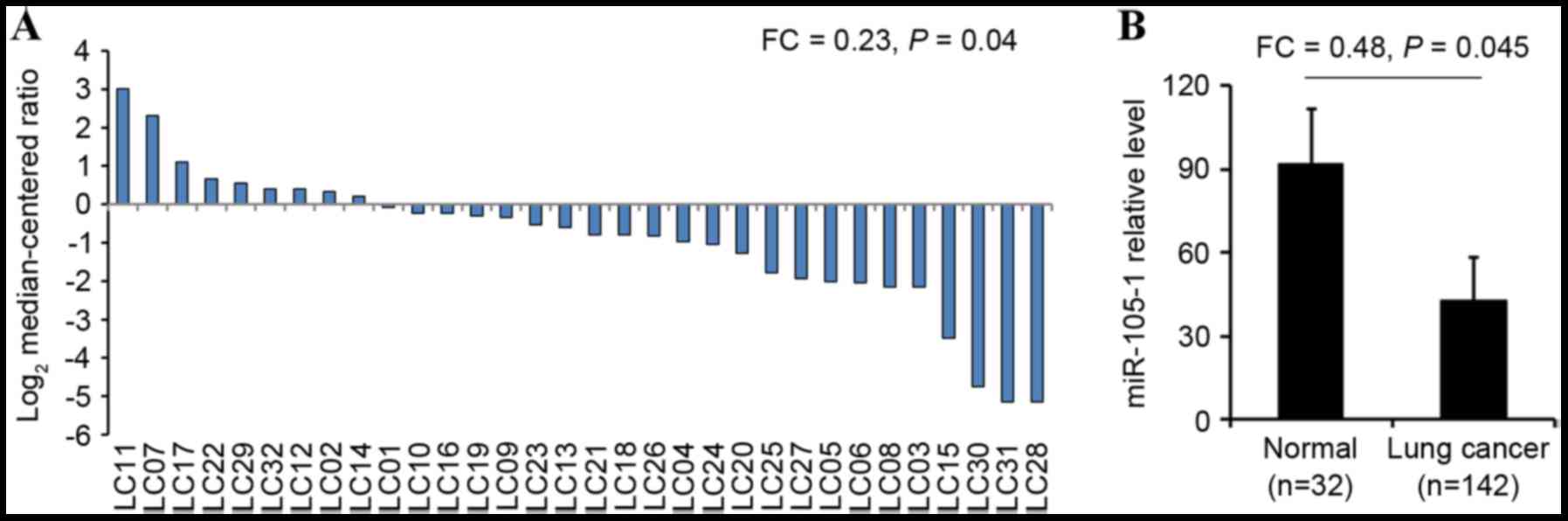
miR-105-1 levels were observed to be significantly lower in NSCLC
tissues (21.36±3.89) compared with those in paired adjacent
non-cancerous tissues (92.89±10.75). The difference between tumor
and normal tissues was statistically significant (FC=0.23, P=0.04;
Fig. 2A). In addition, the level of
miR-105-1 expression was also lower in all NSCLC tumor biopsies
(44.59±5.93) compared with the expression in normal lung tissues
(92.89±10.75) and the differences were statistically significant
(FC=0.48, P=0.045; Fig. 2B).
Association of miR-105-1 expression
with clinicopathological data from patients with NSCLC
The present study next associated miR-105-1
expression with clinicopathological data from patients with NSCLC
and observed that miR-105-1 expression levels were inversely
associated with tumor size (P=0.013; Table I), but there was no association of
miR-105-1 expression with other clinicopathological data from NSCLC
patients, including sex, age, smoking history, tumor
differentiation, histology, vascular invasion, lymph-node
metastasis, TNM stage or invasion of the lung membrane (P>0.05;
Table I).
 | Table I.Univariate analysis of overall
survival based on patients with non-small cell lung cancer
stratified by clinical characteristics. |
Table I.
Univariate analysis of overall
survival based on patients with non-small cell lung cancer
stratified by clinical characteristics.
|
|
|
|
| Overall survival |
|
|---|
|
|
|
|
|
|
|
|---|
| Variable | N | miR-105-1 expression,
mean ± SD | P-value | Mean months | 95% CI (mean) | P-value (log-rank
test) |
|---|
| Age, years |
|
| 0.39 |
|
| 0.74 |
|
≥60 | 90 | 39.76±3.83 |
| 31.46 | 29.38–32.14 |
|
|
<60 | 52 | 46.35±4.38 |
| 33.52 | 30.51–35.69 |
|
| Sex |
|
| 0.89 |
|
| 0.90 |
|
Male | 86 | 45.39±3.47 |
| 31.97 | 28.36–32.34 |
|
|
Female | 56 | 44.38±6.54 |
| 32.42 | 29.38–33.13 |
|
| Tobacco
smoking |
|
| 0.74 |
|
| 0.32 |
|
Never | 35 | 41.35±2.85 |
| 32.33 | 28.74–29.16 |
|
|
Ever | 41 | 40.29±6.58 |
| 30.26 | 27.43–35.06 |
|
|
Unknown | 66 | 42.36±6.89 |
| 31.29 | 27.04–33.65 |
|
| Lymph node
metastasis |
|
| 0.07 |
|
| 0.03 |
|
Negative | 48 | 46.75±8.95 |
| 33.69 | 32.05–34.73 |
|
|
Positive | 82 | 39.87±15.74 |
| 30.83 | 28.95–32.22 |
|
|
Unknown | 12 | 40.39±10.88 |
| 30.26 | 28.34–33.16 |
|
| Tumor
differentiation |
|
| 0.10 |
|
| 0.12 |
|
Poorly | 51 | 40.23±5.96 |
| 28.74 | 26.47–30.96 |
|
|
Moderately | 85 | 41.05±6.25 |
| 30.51 | 28.48–32.52 |
|
|
Well | 6 | 43.47±4.89 |
| 31.26 | 29.56–33.03 |
|
| Histology |
|
| 0.89 |
|
| 0.22 |
|
Adenocarcinoma | 90 | 42.68±9.87 |
| 28.99 | 27.06–31.13 |
|
|
Squamous cell carcinoma | 52 | 43.15±6.63 |
| 32.04 | 29.37–34.59 |
|
| TNM stage |
|
| 0.06 |
|
| 0.011 |
|
I–II | 92 | 42.67±5.24 |
| 32.48 | 30.56–34.33 |
|
|
III–IV | 50 | 40.38±6.69 |
| 27.59 | 24.69–29.38 |
|
| Invasion of lung
membrane |
|
| 0.08 |
|
| 0.08 |
|
Negative | 28 | 40.56±2.04 |
| 31.69 | 28.47–32.64 |
|
|
Positive | 102 | 41.36±6.67 |
| 29.08 | 27.95–31.02 |
|
|
Unknown | 12 | 43.25±5.26 |
| 29.31 | 27.65–35.43 |
|
| Vascular
invasion |
|
| 0.87 |
|
| 0.67 |
|
Negative | 130 | 41.26±5.03 |
| 30.59 | 28.74–32.69 |
|
|
Positive | 8 | 42.65±3.38 |
| 31.26 | 29.38–33.15 |
|
|
Unknown | 4 | 41.96±5.74 |
| 29.63 | 27.31–31.31 |
|
| Tumor size, cm |
|
| 0.01 |
|
| 0.00 |
| ≥5 | 35 | 35.26±6.67 |
| 26.15 | 24.18–29.34 |
|
|
<5 | 107 | 42.37±5.89 |
| 33.06 | 31.25–34.31 |
|
Association of miR-105-1 levels and
clinicopathological data with survival of NSCLC patients
The present study additionally associated miR-105-1
levels and clinicopathological data with the survival of patients
with NSCLC. miR-105-1 levels were recorded as high vs. low using
the median value as the cut-off point. Kaplan-Meier survival curves
were plotted to estimate the prognostic value of the
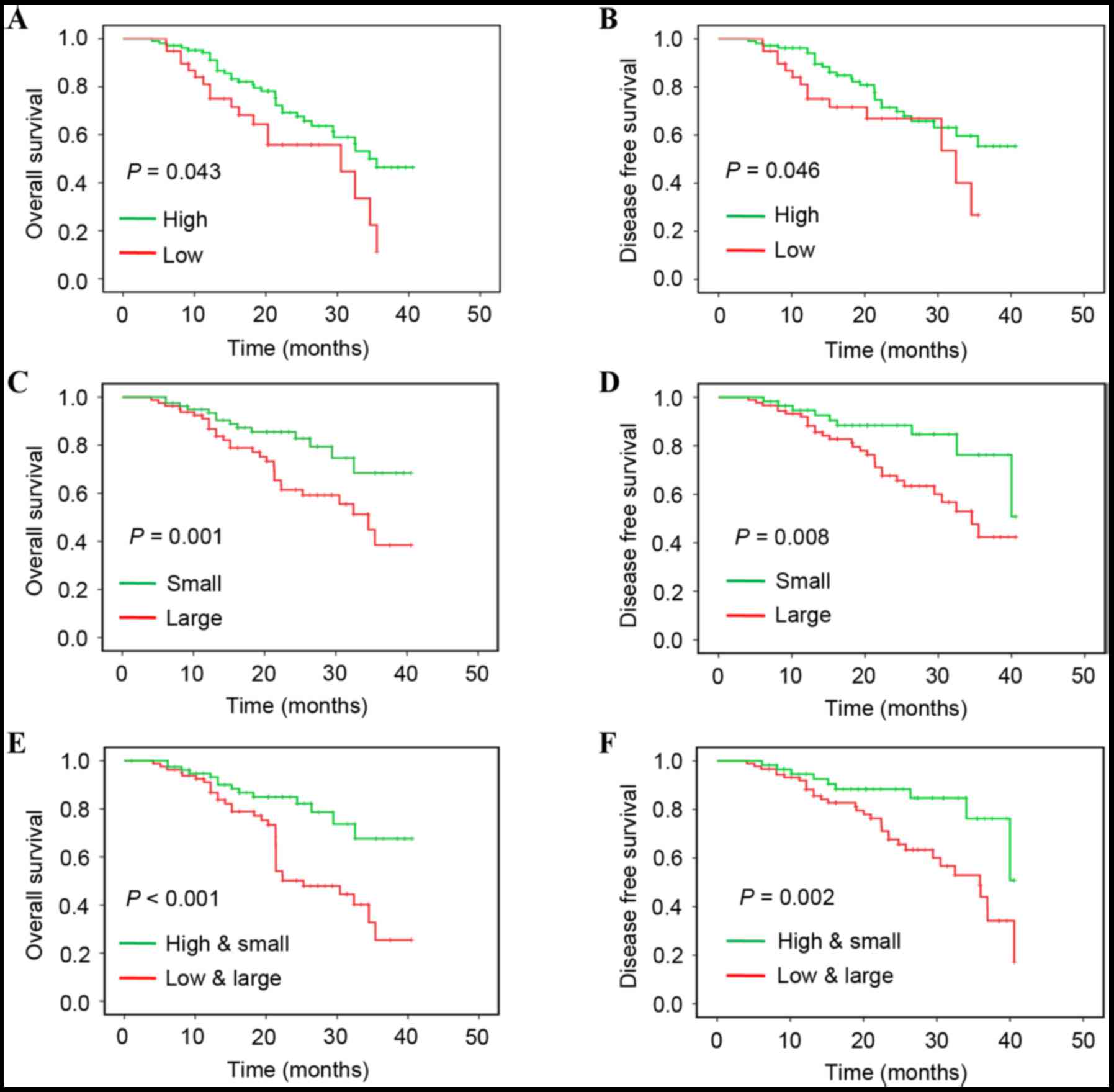
clinicopathological characteristics for OS. The data of the present
study revealed that a reduced miR-105-1 level was associated with a
shorter OS (P=0.043; Fig. 3A) and DFS
(P=0.046; Fig. 3B), while lymph-node
metastasis (P=0.031), TNM stage (P=0.011) and tumor size (≥5 cm;
P=0.001) were all associated with shorter OS of patients with NSCLC
(Fig. 3 and Table II).
| Table II.Univariate and multivariate analyses
of overall survival of patients with non-small cell lung
cancer. |
Table II.
Univariate and multivariate analyses
of overall survival of patients with non-small cell lung
cancer.
|
|
|
|
| miR-105-1
multivariate analysis |
|---|
|
|
|
|
|
|
|---|
| Factor | HR | 95% CI
(univariate) | P-value | HR | 95% CI
(multivariate) | P-value |
|---|
| Age | 1.24 | 1.11–1.35 | 0.68 | 1.31 | 1.15–1.38 | 0.55 |
| Sex | 0.89 | 0.74–1.02 | 0.66 | 0.85 | 0.77–0.89 | 0.61 |
| Smoking
history | 1.31 | 1.24–1.65 | 0.23 | 1.48 | 1.35–1.74 | 0.09 |
| Lymph-node
metastasis | 1.89 | 1.56–2.21 | 0.04 | 1.95 | 1.66–2.32 | 0.04 |
| Tumor
differentiation | 1.33 | 0.94–1.52 | 0.12 | 1.31 | 0.92–1.46 | 0.14 |
| Histology | 1.06 | 0.84–1.52 | 0.32 | 1.08 | 0.89–1.63 | 0.31 |
| TNM stage | 2.31 | 2.04–2.66 | 0.01 | 2.47 | 2.25–2.89 | 0.01 |
| Invasion of lung
membrane | 1.62 | 1.44–1.81 | 0.09 | 1.68 | 1.49–1.84 | 0.07 |
| Vascular
invasion | 0.92 | 0.74–1.02 | 0.77 | 0.93 | 0.75–1.08 | 0.75 |
| Tumor size | 2.26 | 2.08–2.69 | <0.01 | 3.01 | 2.65–3.33 | <0.01 |
| miR-105-1
expression | 0.66 | 0.55–0.71 | 0.03 | 0.64 | 0.51–0.70 | 0.02 |
Univariate and multivariate analyses with Cox
proportional hazards regression model revealed that lymph node
metastasis [P=0.04; hazard ratio (HR)=1.89; 95% confidence interval
(CI), 1.56, 2.21], advanced TNM stage [P=0.01; HR=2.31 (95% CI,
2.04, 2.66)], larger tumor size [P=0.001; HR=2.26 (95% CI, 2.08,
2.69)] and reduced miR-105-1 levels [P=0.034; HR=0.66 (95% CI,
0.55, 0.71)] were all predictors for poorer NSCLC prognosis
(Table II). When combining the
reduced miR-105-1 level with tumor size, multivariate analysis
demonstrated that the aforementioned variables were independent
predictors for poor OS (P<0.001; Fig.
3E) and DFS (P=0.002; Fig.
3F).
Discussion
Sensitive and specific tumor-markers for early NSCLC
detection may be useful to decrease lung cancer morbidity and
mortality (28,29). In the present study, we evaluated and
identified miR-105-1 as a prognostic marker able to predict OS and
DFS of patients with NSCLC. An in silico analysis of
miR-105-1 was performed, together with other differentially
expressed miRNAs in lung cancer vs. other conditions using GEO
database data. The present study then validated the aforementioned
findings in another set of NSCLC vs. non-cancerous tissue samples.
The data of the present study revealed that a downregulated
miR-105-1 level was associated with tumor size and poor OS and DFS
of patients with NSCLC.
The findings of the present study are consistent
with those from previous studies on various types of tumor. For
example, Guan et al (16)
revealed that the miR-105 level was markedly decreased in gliomas
compared with that in non-neoplastic brain tissues and that the
reduced miR-105 expression was statistically associated with
advanced tumor grades, such as grade IV glioma. The authors
speculated that downregulation of miR-105 expression was associated
with poor clinical outcome, and was involved in glioma
tumorigenesis and progression; thus, the detection of miR-105
levels may be a novel biomarker in the prediction of glioma
prognosis. Shen et al (30)
reported that miR-105 expression was prominently low in
hepatocellular carcinoma (HCC) cell lines and tissues compared with
that in normal human hepatocyte and adjacent non-cancerous tissues,
respectively. The authors also observed that miR-105 functioned as
a potential tumor suppressor to inhibit expression of the
phosphoinositide 3-kinase (PI3K)/Akt signaling pathway genes and
may represent a potential therapeutic target for patients with HCC.
Another previous study demonstrated that miR-105 inhibited prostate
tumor growth via the inhibition of cyclin-dependent kinase 6
(31). However, not all published
data supported this association or the tumor-suppressive activity
of miR-105-1. For example, Honeywell et al (32) reported that the levels of miR-105-1
were upregulated in cancerous tissue analyzed by RT-qPCR. This
inconsistent finding may be due to the tumor type or contamination
of normal tissue in the tumor samples. However, another in
vitro study revealed that cancer-secreted miR-105 destroyed
vascular endothelial barriers and promoted cancer metastasis
(14). Thus, additional studies are
required to clarify the role of miR-105 in NSCLC.
To date, the precise role and potential
patho-physiological mechanism responsible for or involving the
antitumor activity of miR-105-1 require additional investigation,
including NSCLC. The next step will be to predict and identify the
targeting genes of miR-105-1 in NSCLC and, based on that data, the
role of miR-105-1 in lung tissue may be speculated. Thus, targeting
miR-105-1 may be used as a therapeutic strategy for NSCLC
patients.
Although the present study revealed reduced
miR-105-1 levels in NSCLC tissue, which was associated with poor OS
and DFS of patients with NSCLC, there are several limitations.
Primarily, the miR-105-1 levels in tissues were detected using
RT-qPCR, which was not microdissected and included a mixture of
normal and tumor tissues. Furthermore, the data of the present
study are from an association study, and little is known about the
molecular and patho-physiological mechanisms of miR-105-1 in
NSCLC.
In conclusion, the data of the present revealed that
a reduced level of miR-105-1 in NSCLC tissues was associated with a
shorter OS and DFS of patients with NSCLC, and that miR-105-1 was a
predictor for shorter OS of patients with NSCLC.
Acknowledgements
We appreciate the experimental support of Central
Laboratory for Medical Research, Shanghai Tenth People's Hospital
(Shanghai, China). The present study was supported by grants from
the National Natural Science Foundation of China (Beijing, China;
grant nos. 81472501, 81201535, 81301993, 81372175, 81472202 and
81302065) and Health and Family Planning Commission projects
(Shanghai, China; grant nos. 201540228 and 201440398).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hill A, Fisher P and Yeomanson D:
Non-small cell lung cancer. BMJ. 345:e64432012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cykert S, Dilworth-Anderson P, Monroe MH,
Walker P, McGuire FR, Corbie-Smith G, Edwards LJ and Bunton AJ:
Factors associated with decisions to undergo surgery among patients
with newly diagnosed early-stage lung cancer. JAMA. 303:2368–2376.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fervers B: Chemotherapy in elderly
patients with resected stage II–IIIA lung cancer. BMJ.
343:d41042011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sullivan R, Alatise OI, Anderson BO,
Audisio R, Autier P, Aggarwal A, Balch C, Brennan MF, Dare A,
D'Cruz A, et al: Global cancer surgery: Delivering safe,
affordable, and timely cancer surgery. Lancet Oncol. 16:1193–1224.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Global Burden of Disease Cancer
Collaboration, Fitzmaurice C, . Dicker D, Pain A, Hamavid H,
Moradi-Lakeh M, MacIntyre MF, Allen C, Hansen G, Woodbrook R, et
al: The Global burden of cancer 2013. JAMA Oncol. 1:505–527. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
National Lung Screening Trial Research
Team, . Church TR, Black WC, Aberle DR, Berg CD, Clingan KL, Duan
F, Fagerstrom RM, Gareen IF, Gierada DS, et al: Results of initial
low-dose computed tomographic screening for lung cancer. N Engl J
Med. 368:1980–1991. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gasparini P, Cascione L, Landi L, Carasi
S, Lovat F, Tibaldi C, Alì G, D'Incecco A, Minuti G, Chella A, et
al: microRNA classifiers are powerful diagnostic/prognostic tools
in ALK-, EGFR-, and KRAS-driven lung cancers. Proc Natl Acad Sci
USA. 112:pp. 14924–14929. 2015, View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cheng CJ, Bahal R, Babar IA, Pincus Z,
Barrera F, Liu C, Svoronos A, Braddock DT, Glazer PM, Engelman DM,
et al: MicroRNA silencing for cancer therapy targeted to the tumour
microenvironment. Nature. 518:107–110. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Martello G, Rosato A, Ferrari F, Manfrin
A, Cordenonsi M, Dupont S, Enzo E, Guzzardo V, Rondina M, Spruce T,
et al: A MicroRNA targeting dicer for metastasis control. Cell.
141:1195–1207. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yanaihara N, Caplen N, Bowman E, Seike M,
Kumamoto K, Yi M, Stephens RM, Okamoto A, Yokota J, Tanaka T, et
al: Unique microRNA molecular profiles in lung cancer diagnosis and
prognosis. Cancer Cell. 9:189–198. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Peinado H, Alečković M, Lavotshkin S,
Matei I, Costa-Silva B, Moreno-Bueno G, Hergueta-Redondo M,
Williams C, García-Santos G, Ghajar C, et al: Melanoma exosomes
educate bone marrow progenitor cells toward a pro-metastatic
phenotype through MET. Nat Med. 18:883–891. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhou W, Fong MY, Min Y, Somlo G, Liu L,
Palomares MR, Yu Y, Chow A, O'Connor ST, Chin AR, et al:
Cancer-secreted miR-105 destroys vascular endothelial barriers to
promote metastasis. Cancer Cell. 25:501–515. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hood JL, San RS and Wickline SA: Exosomes
released by melanoma cells prepare sentinel lymph nodes for tumor
metastasis. Cancer Res. 71:3792–3801. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Guan Y, Chen L, Bao Y, Li Z, Cui R, Li G
and Wang Y: Identification of low miR-105 expression as a novel
poor prognostic predictor for human glioma. Int J Clin Exp Med.
8:10855–10864. 2015.PubMed/NCBI
|
|
17
|
NCBI Resource Coordinators: Database
resources of the national center for biotechnology information.
Nucleic Acids Res. 44:D7–D19. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Barrett T, Wilhite SE, Ledoux P,
Evangelista C, Kim IF, Tomashevsky M, Marshall KA, Phillippy KH,
Sherman PM, Holko M, et al: NCBI GEO: Archive for functional
genomics data sets-update. Nucleic Acids Res. 41:(Database Issue).
D991–D995. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lantuejoul S, Rouquette I, Brambilla E and
Travis WD: New WHO classification of lung adenocarcinoma and
preneoplasia. Ann Pathol. 36:5–14. 2016.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Edge SB and Compton CC: The American Joint
Committee on cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen C, Ridzon DA, Broomer AJ, Zhou Z, Lee
DH, Nguyen JT, Barbisin M, Xu NL, Mahuvakar VR, Andersen MR, et al:
Real-time quantification of microRNAs by stem-loop RT-PCR. Nucleic
Acids Res. 33:e1792005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schaap-Oziemlak AM, Raymakers RA,
Bergevoet SM, Gilissen C, Jansen BJ, Adema GJ, Kögler G, le Sage C,
Agami R, van der Reijden BA and Jansen JH: MicroRNA hsa-miR-135b
regulates mineralization in osteogenic differentiation of human
unrestricted somatic stem cells. Stem Cells Dev. 19:877–885. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhao B, Zhu Y, Cui K, Gao J, Yu F, Chen L
and Li S: Expression and significance of PTEN and miR-92 in
hepatocellular carcinoma. Mol Med Rep. 7:1413–1416. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gao F, Wang T, Zhang Z, Wang R, Guo Y and
Liu J: Regulation of activating protein-4-associated metastases of
non-small cell lung cancer cells by miR-144. Tumour Biol. Aug
8–2015.(Epub ahead of print).
|
|
26
|
Qi F, He T, Jia L, Song N, Guo L, Ma X,
Wang C, Xu M, Fu Y, Li L and Luo Y: The miR-30 family inhibits
pulmonary vascular hyperpermeability in the premetastatic phase by
direct targeting of Skp2. Clin Cancer Res. 21:3071–3080. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hu Z, Chen X, Zhao Y, Tian T, Jin G, Shu
Y, Chen Y, Xu L, Zen K, Zhang C and Shen H: Serum microRNA
signatures identified in a genome-wide serum microRNA expression
profiling predict survival of non-small-cell lung cancer. J Clin
Oncol. 28:1721–1726. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liu D, Hu X, Zhou H, Shi G and Wu J:
Identification of aberrantly expressed miRNAs in gastric cancer.
Gastroenterol Res Pract. 2014:4738172014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zen K and Zhang CY: Circulating microRNAs:
A novel class of biomarkers to diagnose and monitor human cancers.
Med Res Rev. 32:326–348. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shen G, Rong X, Zhao J, Yang X, Li H,
Jiang H, Zhou Q, Ji T, Huang S, Zhang J and Jia H: MicroRNA-105
suppresses cell proliferation and inhibits PI3K/AKT signaling in
human hepatocellular carcinoma. Carcinogenesis. 35:2748–2755. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Han Y, Jia C, Cong X, Yu F, Cai H, Fang S,
Cai L, Yang H, Sun Y, Li D, et al: Increased expression of TGFβR2
is associated with the clinical outcome of non-small cell lung
cancer patients treated with chemotherapy. PLoS One.
10:e01346822015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Honeywell DR, Cabrita MA, Zhao H,
Dimitroulakos J and Addison CL: miR-105 inhibits prostate tumour
growth by suppressing CDK6 levels. PLoS One. 8:e705152013.
View Article : Google Scholar : PubMed/NCBI
|